
Abstract
Objective:
To evaluate the incidence rate of nephrotoxicity in Tripterygium wilfordii Hook. f (TwHF) preparations approved by the China Food and Drug Administration and the potential risk factors.
Methods:
CENTRAL, PubMed, SinoMed, Chinese National Knowledge Infrastructure, VIP, China Important Conference Papers Database, China Dissertation Database, and online clinical trial registry websites were searched for articles that reported on nephrotoxicity of TwHF preparations until November 23, 2017. There was no limitation for study design.
Results:
A total of 36 articles involving 2,017 participants were included. Results showed that the incidence of nephrotoxicity associated with TwHF preparations was 5.81% (95% confidence interval: 4.43–7.57). Subgroup analysis showed that the disease type, combined medication, duration, and study design were not correlated with the incidence of nephrotoxicity.
Conclusion:
The incidence rate of nephrotoxicity in TwHF preparations was 5.81%. The possible risk factors, such as disease type, the combination with other drugs, medication time, and study design, were not found to be correlated with the incidence of nephrotoxicity. However, due to the limited number of included articles, the limited sample size, and the poor methodology quality, the incidence rate of nephrotoxicity of TwHF preparations might be overestimated, and more prospective articles are needed to explore the potential influence factor.
Introduction
Tripterygium wilfordii Hook. f (TwHF) is a commonly used herbal medicine in Traditional Chinese Medicine (TCM). A number of proprietary Chinese medicines contain the herb TwHF, which has been approved by the China Food and Drug Administration (CFDA). In China, TwHF preparations are widely used as an immunosuppressant for diseases such as rheumatoid arthritis and nephrotic syndrome. Previous studies showed that TwHF might lead to reproductive toxicity, and endocrine system and digestive system damage. 1,2 In addition, nephrotoxicity is also reported to be associated with TwHF preparations in animal and clinical studies. 3 In the 1990s, Chou et al. reported a case suggesting that people who had taken TwHF preparation might have a risk of nephrotoxicity. 4 Until April 2012, about 839 cases of adverse events were reported to be associated with TwHF preparations, and renal insufficiency and failure were the most severe adverse events. 5
The incidence of nephrotoxicity associated with TwHF preparations is inconsistent between different studies and for a variety of TwHF preparations. A systematic review of all available clinical studies on nephrotoxicity of TwHF preparations can present a more reliable and comprehensive picture of the available evidence.
This systematic review aimed to explore the incidence of nephrotoxicity of TwHF preparations and the related risk factors. Results of this review may provide the evidence for the prevention and reduction of nephrotoxicity of TwHF preparations.
Materials and Methods
The protocol was registered (CRD42018082340) and conducted following PRISMA harms checklist.
Definition of TwHF preparations
In this review, TwHF preparations were defined as proprietary Chinese medicines that contain the herb TwHF and have been approved by CFDA. We searched the CFDA domestic drug database and screened the instructions of all available 58,908 proprietary Chinese medicines for TwHF preparations. A total of 26 TwHF preparations were identified and the selection process is presented in Figure 1. The names and compositions of these 26 TwHF preparations are shown in Appendix Table A1.
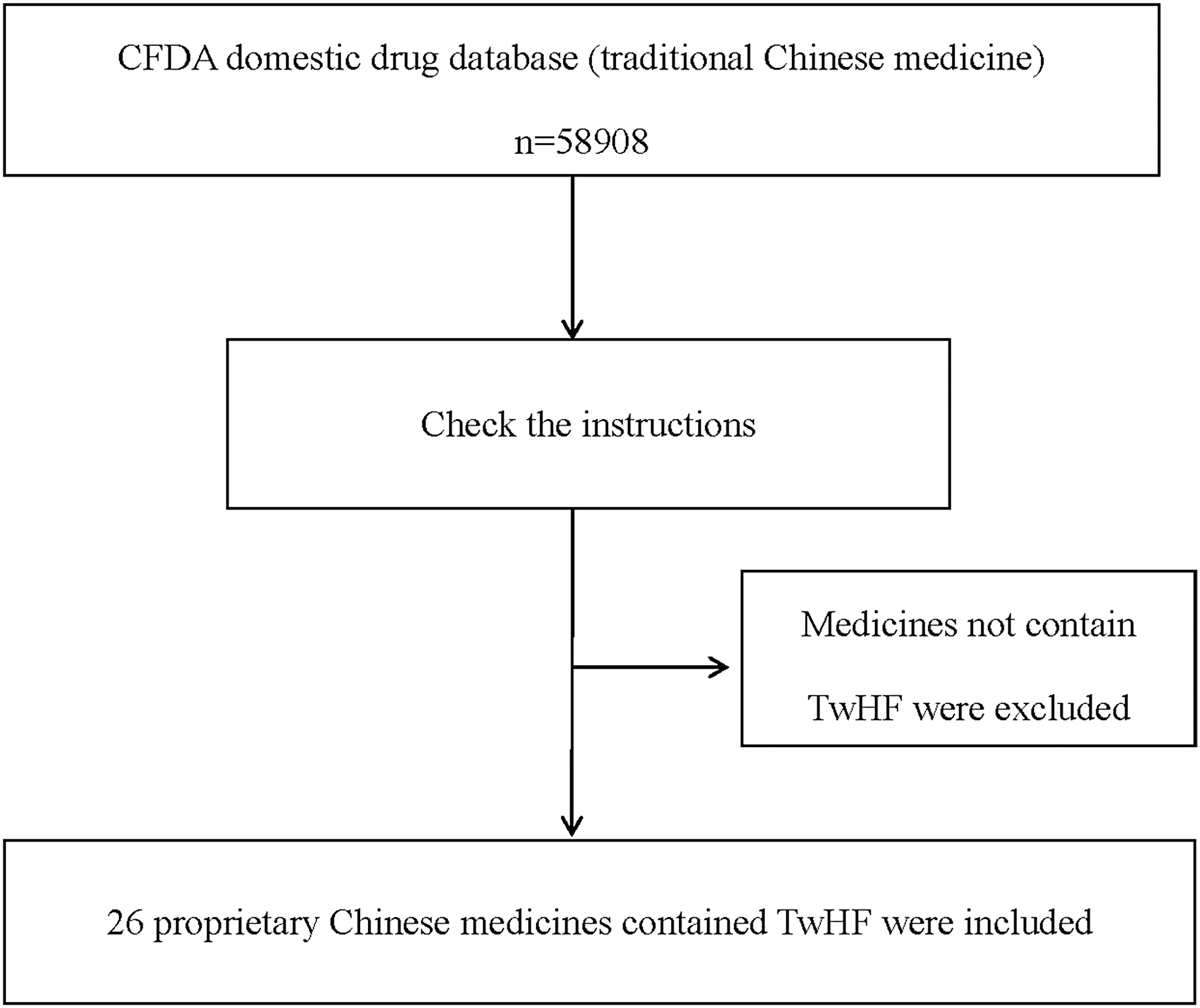
Flow chart of TwHF preparation selection process. CFDA, China Food and Drug Administration; TwHF, Tripterygium wilfordii Hook f.
Definition of nephrotoxicity
Nephrotoxicity is a kidney-specific feature, in which excretion does not go smoothly owing to toxic chemicals or drugs. 6 In this review, nephrotoxicity refers to nephrotoxicity caused by TwHF preparations.
Inclusion criteria
Articles that explored the 26 TwHF preparations in any kind of patients and reported nephrotoxic outcomes were included. There was no limitation on study design. Systematic reviews, randomized controlled trials (RCTs), quasi-randomized controlled trials, nonrandomized controlled trials (NRCTs), controlled before-and-after studies, prospective cohort studies, retrospective cohort studies, historically controlled trials, nested case–control studies, case–control studies, cross-sectional studies, before-and-after comparisons, case reports (CR), and case series were all included.
Searching strategy
We searched six Chinese and English databases, including Chinese BioMedical CD-ROM (SinoMed), Chinese National Knowledge Infrastructure, Chinese VIP information (VIP), Wanfang database, PubMed, and Cochrane Central Register of Controlled Trials (CENTRAL), from the inception date until November 23, 2017. The publication types and languages were not limited. Detailed search strategy of PubMed is shown in Appendix A1. Reference lists of all relevant articles were also hand-searched for potential relative articles.
Article selection and data extraction
Two authors (X.F. and S.-N.F.), independent of each other, selected the articles and extracted the data. We resolved disagreements through discussion, and asked W.C. to arbitrate when disagreements still existed.
The extracted data included the following information: publication data (year and authors), study characteristics and design, characteristics of participants (age, gender, and diagnosis of the diseases), interventions (drug name, forms, dosage, and duration), the number of participants with adverse events related to nephrotoxicity, and the quality of the literature. Special cases were handled according to Cochrane handbook, 7 such as (1) three-armed trials of two TwHF preparations groups compared to a non-TwHF preparation group were separately analyzed as a controlled trial and a case series (CS). (2) RCTs of TwHF preparations in both groups were downgraded to two CS for data extraction.
Methodological quality assessment
Methodological quality of RCTs was assessed by the Cochrane risk of bias tool. 8 We made judgments on each of these criteria relating to the risk of bias: low, high, or unclear (indicating unclear or unknown risk of bias).
NRCTs were assessed by the MINORS scale. 9 A total of 12 items were assessed, each item 0–2 points. 0 point indicates no information was reported, 1 point indicates insufficient information reporting, and 2 points indicate sufficient information reporting. The first eight items were for noncomparative studies, with a maximum of 16 points. The last four and the first eight items together were for comparative studies, with a maximum of 24 points.
Cohort study and case–control study were assessed by the Newcastle-Ottawa Scale on selection of study participants (four stars), comparability of studies based on design or analysis (two stars), and evaluation of ascertained outcomes (three stars). 10 Out of nine stars, a total of five stars or more was rated as high-quality research.
CS were assessed by the Quality Appraisal Tool for Case Series conducted by Canada Institute of Health Economics. 11 The 20-criterion quality appraisal checklist examines the main domains of a case series. including study design, population, intervention and co-interventions, outcome measures, statistical analysis, results and conclusions, and competing interest and sources of financial support. Each criterion was judged as “yes,” “no,” or “unclear.” A case series of 14 or more yes responses (≥70%) was considered to be of acceptable quality.
Because there were no well-established methodological criteria for case report, currently, we assessed these items of included CR according to the Cochrane Handbook 12 : (1) whether the reports had good predictive value; (2) whether the reports determined causality; (3) whether there was a plausible biological mechanism linking the intervention to the adverse event; (4) whether the reports provide enough information to allow detailed appraisal of the evidence; and (5) whether there were any potential problems from using data from the reports, which might outweigh the perceived benefit of being comprehensive.
Two authors (X.F. and S.-N.F.) independently assessed the quality of the included articles. Disagreement was resolved by discussion, and consensus was reached through discussion with a third party (W.C.).
Data synthesis
R 3.3.2 software was used to conduct the meta-analysis of nephrotoxicity incidence. Odds ratio with its 95% confidence interval (CI) was measured. We tested heterogeneity using the I 2 statistic with significance set at 50% and the chi-square statistic significance set at p < 0.10. If we identified significant heterogeneity, the random-effects model would be used. In addition, subgroup analysis would be conducted according to the type of disease treated, drug delivery way, medication time, study design, and age of the participants (children and adults).
Results
Literature search results and articles selection
A total of 5,097 articles were identified through primary retrieval; 5,094 articles were got from electronic database, and 3 articles were got from hand-search (reference lists of 36 included articles). We excluded 2,297 duplicates and 1,347 obviously irrelevant citations by screening titles and abstracts. After reading 1,453 full text articles, 36 articles were included. The flow chart of selection process is presented in Figure 2.

Flow chart of Literature selection process. TwHF, Tripterygium wilfordii Hook f.
Description of included articles
This review included 16 randomized controlled trials, 13 –28 1 nonrandomized controlled trial, 29 6 CS, 30 –35 and 13 CR. 36 –48 Two RCTs, 18,27 which included TwHF preparations in both arms, were separated and analyzed as four CS. One RCT 22 compared TwHF preparation with another hospital preparation containing TwHF. We only extracted the information of TwHF preparation group and analyzed as a CS. One RCT, 26 which included TwHF preparations in three arms, was separated and analyzed as three CS. One three-armed RCT 29 included TwHF preparations in two arms. We split it into one nonrandomized controlled trial and one CS. The interventions of another three-armed RCT 16 were TwHF preparations plus basic treatment, Zhengqing Fengtong Ning plus basic treatment, and basic treatment. We chose two arms (TwHF preparations plus basic treatment vs. basic treatment) for analysis to avoid the reuse of data. Thus, 41 “new” articles from 36 publications were included in our final analyses, including 12 RCTs, 1 NRCT, 15 CSS, and 13 CR. The distribution of articles published time is presented in Figure 3. Study-type distribution is presented in Figure 4. Disease distribution is presented in Figure 5.
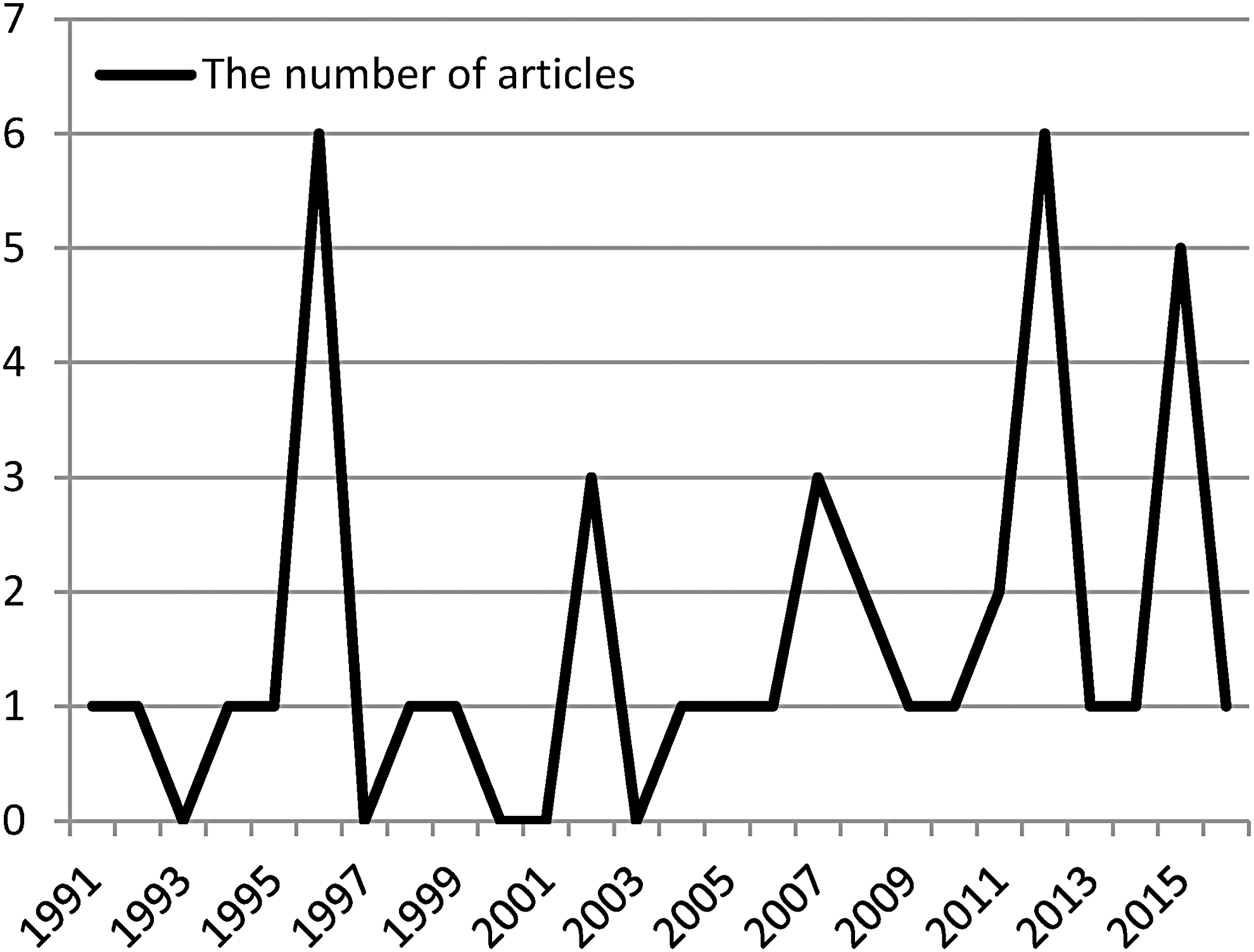
Article published time.

Study-type distribution. RCT, randomized controlled trial.
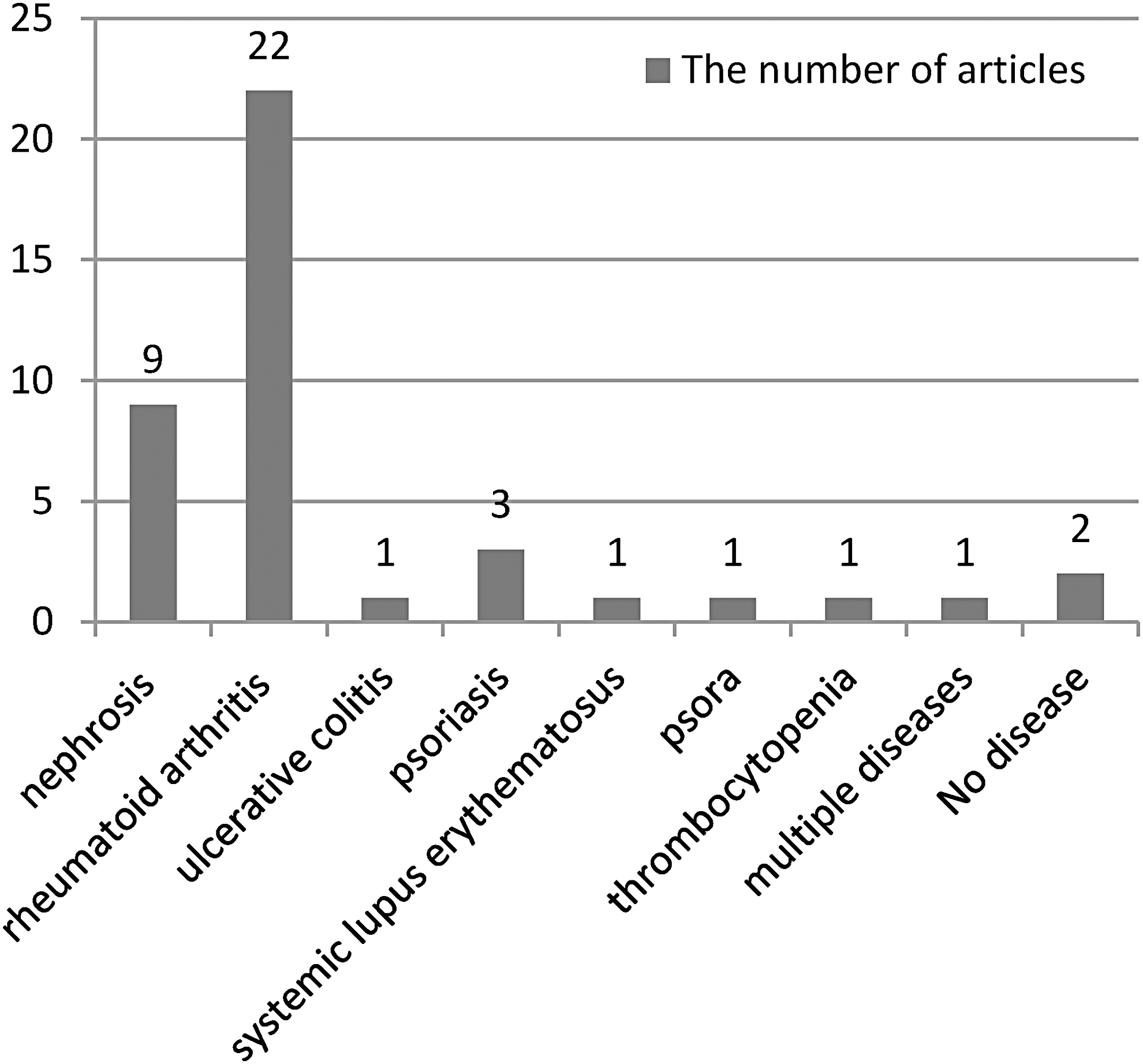
Disease distribution.
A total of 28 RCTs, NRCT, and CSS were included in the meta-analysis involving 1,999 participants. Among them, 1,555 participants were treated with TwHF preparations. The smallest sample size was 23 13 and the largest was 226. 32 The participants were between 1 33 and 78 years 19 of age. Of these, only 5 articles 18,27,31 (split from 3 articles) included both children and adults, and the remaining 23 articles 13 –17,19 –26,28 –32,34–35 (split from 20 articles) only included adults. TwHF preparations were used in 6 articles 13 –17,34 for the treatment of nephropathy and in 22 articles 18 –33,35 (split from 17 articles) for other diseases, including rheumatoid arthritis, ulcers colitis, psoriasis, and systemic lupus erythematosus. The trial interventions of 7 articles 13,22,24,32 –34 were TwHF preparations alone and the other 21 articles 14 –21,23,25 –31,35 (split from 16 articles) were TwHF preparations in combination with other medications. TwHF preparations were administered orally with a daily cumulative dose of 10–60 mg in 25 articles (split from 20 articles). The doses of another two articles were 3 mg/kg 17 and 4.5 mg/kg 25 per day, respectively, and the other one article 33 did not report the doses. Medication time ranged from 40 days to 18 months. The basic characteristics of the articles are shown in Appendix Table A2.
The 13 CR 36 –48 included a total of 18 participants. The age ranged from 10 to 77. One article 47 included children, one 38 included both adults and children, and the other 11 articles 36–37,39 –46,48 included only adults. Three articles used TwHF preparations for the treatment of nephropathy. 38,44,46 The participants of eight articles and one participant of one article used TwHF preparations for the treatment of other diseases 36,39 –45,48 : rheumatoid arthritis (seven articles), psoriasis (one article), and low platelet count (one article). The remaining two articles were for participants who had wrongly taken TwHF preparations. 37,38 The daily dose of TwHF preparations was 30–1,000 mg. Five articles did not explicitly report the dose of TwHF preparations, but only the number of tablets. 37,40,43,46,47 Nephrotoxicity appeared from 1 h to 6 months after taking TwHF preparations. The basic characteristics of CR are shown in Appendix Table A4.
Quality assessment
Randomized controlled trials
The methodological quality of 12 RCTs was generally low. Random number table was used in 5 RCTs 13–14,20,23,25 for random sequence generation. All 12 RCTs did not mention allocation concealment or blinding. Only four RCTs 14,17,20,28 reported the number of people lost to follow-up, but did not conduct an intention-to-treat analysis. Selective reporting was generally unclear in the RCTs due to inaccessibility to the trial protocol. The risk of bias for RCTs is presented in Figure 6.
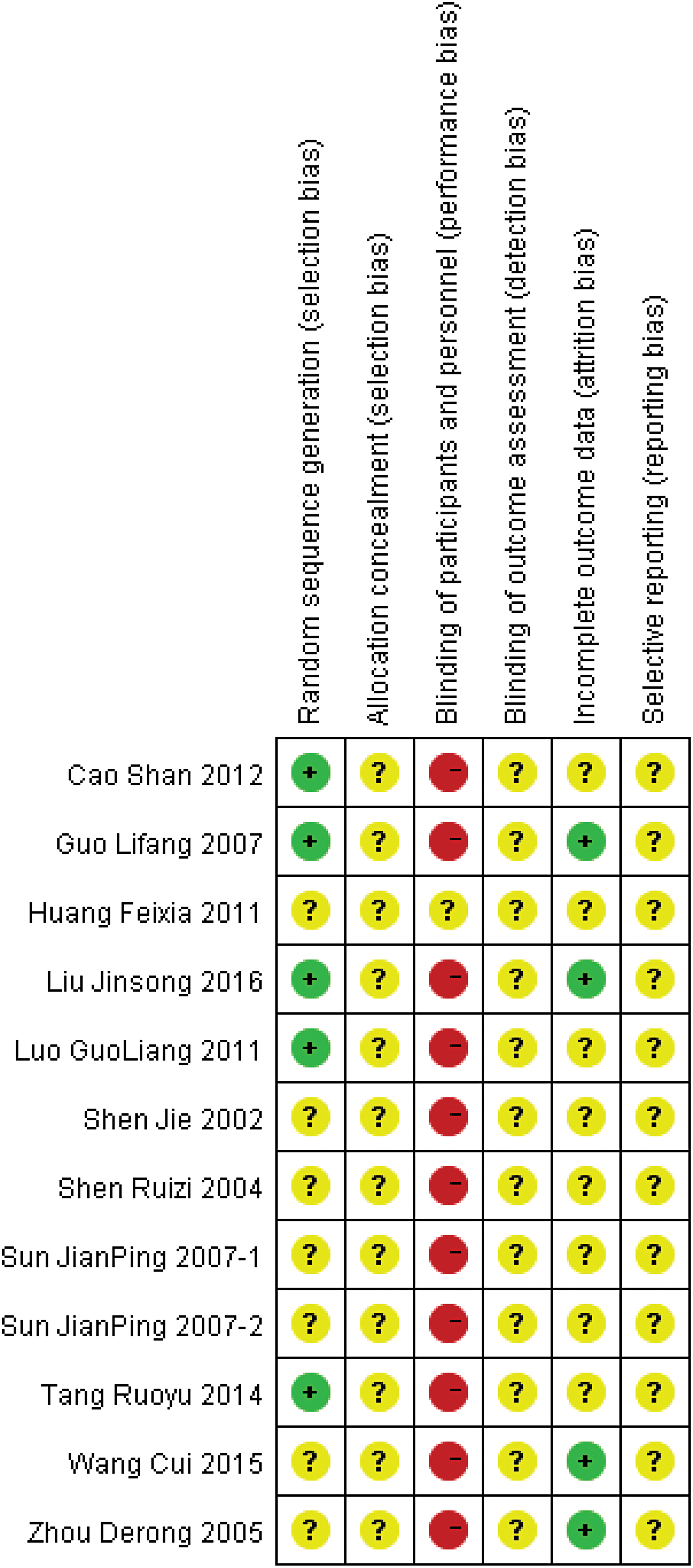
Risks of bias graph. Color images available online at
Nonrandomized controlled trials
The methodological quality of the NRCT was low, with a score of 10 (as shown in Table 1).
Methodological Quality Evaluation Table of Non-Randomized Clinical Controlled Trial
Case series
The methodological quality of 15 CS was generally low as the yes responses to 20-criterion checklist of each article was <12 (as shown in Fig. 7).

Methodological quality evaluation of case series.
Case reports
The methodological quality of 13 CR was generally low. Only six CR had good predictive value, which determined the adverse reactions were caused by interventions. These six CR reported that the drug's adverse reaction was not related to the purpose of the medication under normal usage and dosage, and the adverse reaction could not be explained by the prognosis and progress of the original disease. None of the 13 CR reported how nephrotoxicity was attributed to TwHP preparations. There was plausible biological mechanism linking the intervention to the nephrotoxicity in 13 CR. The information reported by the 13 CR was not informative. These CR did not report the dose, course of treatment, original disease, and the characteristics of participants. Only six CR reported relatively sufficient information. Insufficient information made it difficult to judge the relationship between intervention and nephrotoxicity, so there was a potential bias in using the data in the report (as shown in Fig. 8).

Methodological quality evaluation of case report.
Meta-analysis of nephrotoxicity in TwHF preparations
A meta-analysis of 28 articles (split from 23 articles) involving 1,999 participants was conducted, including RCT, NRCT, and CS. Among the 1,999 participants, 93 people's renal function was damaged. Of these, 1,555 cases were treated with TwHF preparations, and 78 cases had nephrotoxicity. The result showed that the nephrotoxicity incidence of TwHF preparations was 5.81% (95% CI: 4.43–7.57). See Figure 9 for details.
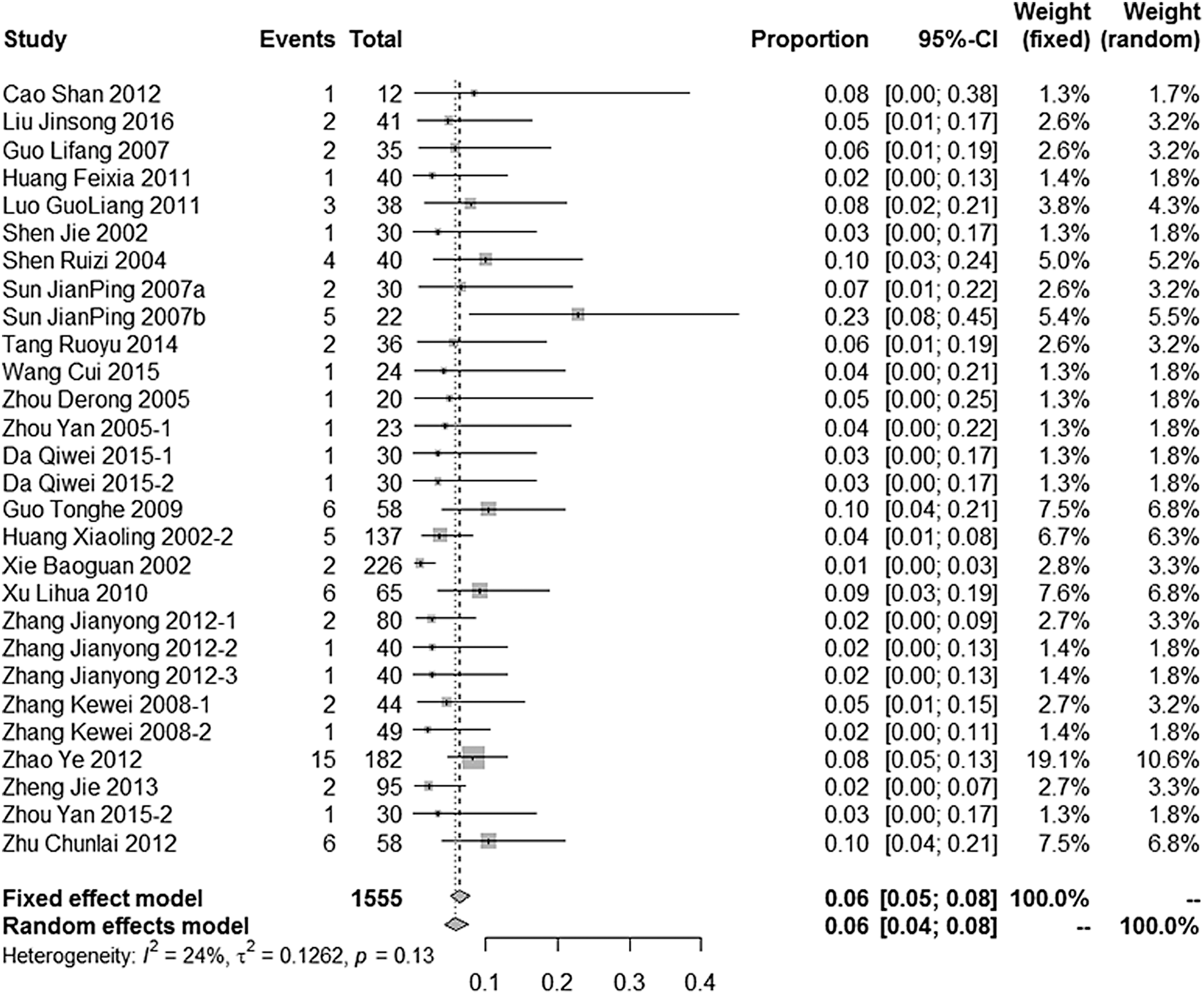
Meta-analysis of nephrotoxicity in TwHF preparations. CI, confidence interval; TwHF, Tripterygium wilfordii Hook f.
Subgroup analysis
Type of disease
The results of subgroup analysis showed that there was no statistical significance of nephrotoxicity incidence rate between kidney diseases and non-kidney diseases.
Drug delivery way
The results of subgroup analysis showed that there was no statistical significance of nephrotoxicity incidence rate between TwHF preparations used alone and in combination with other drugs.
Medication time
The results of subgroup analysis showed that there was no statistical significance of nephrotoxicity incidence rate between medication time within 3 months, 3–12 months, and over 12 months by TwHF preparations.
Study design
Subgroup analysis showed no significant difference between the different study design and the incidence of nephrotoxicity.
Age of the participants (children and adults)
Of the 28 articles (included in the meta-analysis), 5 articles included both children and adults, and the remaining 23 articles only included adults. Therefore, subgroup analysis on children and adults cannot be conducted.
Subgroup analysis results are presented in Table 2.
Subgroup Analysis
CI, confidence interval; CS, case series; NRCT, nonrandomized controlled trials; RCT, randomized controlled trials.
Discussion
Meta-analysis showed that the incidence of nephrotoxicity associated with TwHF preparations was 5.81%. However, due to the limited number of articles and the small sample size, the incidence rate might be overestimated. In addition, the types of included articles were also one of the important factors that had an impact on the results. Most articles included in meta-analysis were CS, so the effect of selection bias and confounding factors on the outcome could not be ignored, and might have influence for the results of the meta-analysis.
The reasons for the overestimation of the incidence of nephrotoxicity
We thought that there were four reasons for the overestimation of the incidence of nephrotoxicity: (1) we did not include articles that did not report adverse reactions, and these articles accounted for more than one-third of the total number of articles on TwHF preparations; (2) results from limited number of articles included in our review and the small sample size of the included articles may be caused by chances; (3) as only one or a few rare adverse reactions was reported in the case report and we could not get the information of denominator, case report cannot be included in meta-analysis. (4) There is a possibility that participants in the included studies were concomitant with renal function impairment. For instance, rheumatoid arthritis-related kidney damage accounted for 0.79% of secondary kidney disease 49 ; kidney involvement accounts for ∼90% of patients with systemic lupus erythematosus according to pathological examination 50 ; and psoriasis can also cause kidney damage. 51 It is difficult to distinguish whether kidney damage was caused by the disease itself or by TwHF preparations. For these reasons, there might be a false-positive risk due to the chance.
Result of subgroup analysis
Subgroup analysis showed no difference when comparing trials about nephropathy to trials about other diseases in the outcome incidence of nephrotoxicity. We thought that the poor reported quality made some clinical heterogeneity difficult to identify, which was one of the reasons for this phenomenon. The small number of included articles, especially the small number of articles related to renal diseases, might impact the authenticity of the result. The dosage of TwHF preparations, medication time, and other factors in the meta-analysis were not well controlled, which also had some impacts on the results.
Subgroup analysis showed that the incidence of nephrotoxicity was not significantly different between single pharmacy and combined pharmacy by TwHF preparations. However, the combined drugs, such as metacortandracin 52 and methotrexate, 53 also had a potential risk of causing nephrotoxicity, and no article had described how to determine adverse reactions attributable to TwHF preparations or other drugs. Therefore, we could not conclude that there was no difference in the incidence of nephrotoxicity between TwHF preparations used alone and in combination with other drugs.
Subgroup analysis of medication time showed no significant difference between the length of time of TwHF preparations and the incidence of nephrotoxicity, which was different from the result of a previous study 54 showing that longer use of TwHF medication was associated with higher incidence of adverse events. The small number of articles included in this review, mostly of CS design, and the discrepancy between dosage and medication time might explain the difference.
Subgroup analysis showed no significant difference between the different study design and the incidence of nephrotoxicity. The poor reported quality and methodological quality may impact the authenticity of the result.
The impact of methodological quality of included articles on the results
The poor methodology of included articles had a significant impact on the authenticity of the research results. In addition to some common methodological problems in articles that focus on efficacy, the articles included in this review also have the following problems: (1) the risks of bias of many trials that were “unclear” may have an unclear impact on an accurate assessment of the intervention effect; (2) it was not possible to determine whether there was reporting bias of the outcomes in a study with no prior registration; (3) inadequate control of confounding factors, such as disease severity, type of disease, and treatment criteria was also the reason for the baseline imbalance between the two groups, which may threat the validity of findings; (4) the outcome measurement of security was not clearly defined. All articles did not define security indicators; (5) few articles had stratified analysis of the results. The patient's basic characteristics or disease stages can be used as stratification factors to further analyze the correlation of these factors with adverse reactions; and (6) few articles reported how to determine nephrotoxicity due to TwHF preparations rather than other diseases.
Implications for clinical practice
Our review showed that the incidence of nephrotoxicity in TwHF preparations was 5.81%. Although this might be overestimated, TwHF preparations should still be used with caution in clinical practice.
In previous studies, it was also found that, although TwHF preparations had the risk of causing severe nephrotoxicity, its therapeutic advantages could not be ignored. In the studies 25 of TwHF preparations compared with metacortandracin for nephrosis, studies 19 of TwHF preparations compared with methotrexate for rheumatoid arthritis, and studies 21 of TwHF preparations compared with sulfasalazine for ulcerative colitis, TwHF preparations showed a better effect on global symptom improvement and there was no significant difference in the incidence of nephrotoxicity compared with these western medicines. Moreover, some severe nephrotoxicity cases were reported to occur most due to overdose of TwHF preparations. Therefore, the development of a “Guideline for the rational use of TwHF preparations” is in need.
Implications for clinical research
We recommend future studies should follow the items of the CONSORT-HARM statement when reporting on nephrotoxicity. The definition and evaluation method of nephrotoxicity should be described. Investigators should report how to collect information on nephrotoxicity, collection time, and collectors. Nephrotoxicity should be analyzed using well-established attribution methods and rational statistical methods. More importantly, it should be clearly stated whether they count recurrent events (events that occur more than once in the same participant) as separate events or as one event.
In addition, considering the characteristics of TCM, the following aspects should be reported in detail: (1) manufacturer, production batch number, dose, usage, and medication time of Chinese patent medicine; (2) the name, dose, usage, and medication time of the combination medication; and (3) the syndrome differentiation of participants and its basis.
Limitations
This review has some limitations. The analysis was still based on the reported data as we could not get the individual data from each single article. Also, some important confounding factors (gender, age, dose of TwHF preparations, disease index, etc.) were not well controlled, which may lead to false conclusions.
Conclusions
The incidence of nephrotoxicity in TwHF preparations was 5.81%. However, as only a limited number of small articles were included, there may be a false-positive conclusion due to chance. Articles that did not report the adverse events were not included in this review; therefore, the incidence of nephrotoxicity in TwHF preparations may be overestimated. Subgroup analysis showed that there was no significant correlation between incidence rate of nephrotoxicity and the disease type, medication way, medication time, and study design. However, due to the small number of included articles, the research type most on CS, and poor quality of methodology, the affirmative conclusion cannot be acquired and prospective researches are needed.
Footnotes
Acknowledgment
W.C. is supported by the National Natural Science Foundation of China Youth Fund Project (Grant No. 81603451).
Author Disclosure Statement
No competing financial interests exist.