
Abstract
Objectives:
It is unclear whether osteopathic manipulative treatment (OMT) affects gastric myoelectric activity (GMA), an index of gastric motility. We hypothesized that OMT significantly alters power spectral density (PSD) analyses of electrogastrography (EGG) recordings, an index of GMA, compared with time control OMT.
Design:
GMA data were obtained from nine subjects before and after OMT and time control on separate days in a cross-over design. Fifteen-minute EGG recordings were obtained before and after each intervention and after a water challenge (WC). Percent power in the normogastric range (PPN) was estimated from PSD analyses. Absolute percent change of PPN and dominant frequency (DF) from baseline to postintervention and baseline to post-WC was computed and compared using two-way repeated-measures ANOVA.
Results:
OMT altered PPN versus time control (time control: 5.3% ± 1.2%; OMT: 24.5% ± 4.5%; p = 0.015). WC altered PPN compared with time control (post-time control ΔPPN: 5.3% ± 1.2%; post-drink ΔPPN: 30.3% ± 7.2%; p < 0.01). However, WC did not alter PPN with prior OMT treatment (post-OMT ΔPPN: 24.5% ± 4.5%; post-WC ΔPPN: 19.4% ± 5.6%; p = 0.47). Nevertheless, OMT reduced the rate of change for DF compared with time control (WC post-time control: 37.9% ± 7.4%; WC post-OMT: 20.0% ± 5.9%; p = 0.02).
Conclusions:
We conclude that (1) OMT significantly alters GMA compared with time control and that (2) OMT reduces the rate of change in the frequency response to WC within the normal frequency range of 2–4 cycles per minute, indicating a physiological effect.
Introduction
C
The gastrointestinal system and its modes of regulation present the opportunity for the application of principles of OMT through the modulation of autonomic function, enteric neural feedback, and/or direct mechanical effects on abdominal viscera. The stomach is richly innervated by intrinsic and extrinsic nerves. 7 Intrinsically, the myenteric (or Auerbach's) plexus lies between the longitudinal and circular muscular layers of the stomach, while the submucosal (or Meissner's) plexus lies within the submucosa. Extrinsically, the branches of the autonomic nervous system modulate the enteric nervous system's (ENS) activity and thus can affect gastric function. 7 Furthermore, mechanical forces (e.g., passage of a food bolus, gravitational forces with standing, and direct palpation) stimulate gastrointestinal smooth muscles to increase the amplitude and frequency of contraction. The summated activity of these mechanical forces with intrinsic and extrinsic neural firing contributes to the rhythmic contractions of the stomach and can be detected using electrogastrography (EGG), which is a noninvasive measure of gastric myoelectric activity (GMA). 8 A complete peristaltic contraction through the gastrointestinal tract is known as 1 cycle, and normal human GMA slow waves have been quantified at ∼2–4 cycles/minute (CPM). 9 Consequently, EGG is usually expressed as percent power in the normal frequency range (2–4 CPM) using power spectral density (PSD) analyses. Hence, the purpose of this study was to test the hypotheses that (1) OMT significantly alters EGG dominant frequency (DF), power (DP), and percent power in the normal range (PPN) in healthy subjects, and (2) OMT modulates the EGG response to water ingestion, a classic stimulus of GMA.
Materials and Methods
Subjects
Prior approval was given by the University of North Texas Health Science Center's Institutional Review Board (IRB # 2014-063). Informed consent was obtained for each subject according to the Declaration of Helsinki. Subjects had no history of gastrointestinal, cardiovascular, or metabolic disease, were not taking any medication, and were instructed to fast for at least 8 h and abstain from caffeine, alcohol, and tobacco for 12 h before the session. Subjects were tested between 6 and 8 AM, before their first meal. A total of 17 subjects were recruited. During the preintervention baseline (see Experimental Design section), the EGG waveform was scrutinized for motion artifacts, which were easily identifiable and removed. 8 If a subject's data included >50% of power outside of 18 cpm, which is the upper limit of what can be reasonably derived from a gastrointestinal source, that subject was excluded. A total of seven subjects were excluded before OMT intervention, due to artifact (usually respiration-related) that would have altered EGG results and consequently were excluded according to prior criteria. 10 One additional subject was excluded due to a persistent coughing fit after the post-OMT water challenge (WC), which made data unusable. A total of nine subjects completed the study and provided usable data.
Experimental design
Subjects participated in a subject-blinded cross-over design composed of two study visits—time control and OMT, separated by at least 24 h. The time control treatment was always performed on the first visit to effectively screen for EGG motion artifacts that would preclude further participation in the study. Furthermore, the time control visit was also performed first to preclude potential lasting effects of OMT on subsequent control visits that may occur. Each subject lay supine on an examination table, the height of which was adjusted by the physician to optimize treatment position. Table 1 describes the OMT procedures that were utilized during the OMT visit, with point of contact, vector, and time for each treatment in seconds. OMT was performed by neuromusculoskeletal medicine/osteopathic manipulative medicine residents. For the time control visit, the physician stood in the same position as they would on the OMT day for the same amount of time, without touching or speaking with the subject. Subjects were positioned comfortably, reclining on a hospital bed, and advised to remain as still as possible.
OMT, osteopathic manipulative treatments.
Data collection
GMA (EGG100C; BIOPAC, Santa Barbara, CA) was measured as described previously. 8 Briefly, the positive electrode was placed at 1–3 cm to the right of the midline from the xiphoid process to the umbilicus, which was on or near the gastric antrum as confirmed by ultrasound (Fig. 1). 11 The negative electrode was placed 45 degrees from the positive electrode and 5 cm above it, while a ground electrode was placed on the flank. 11 The data were sampled at 15 Hz to measure the normal frequency of gastric slow waves, which occurs at 2–4 CPM, or 0.030–0.067 Hz. 8 Vital signs, including arterial pressure, heart rate, and respiratory rate, were taken before and after each experiment.
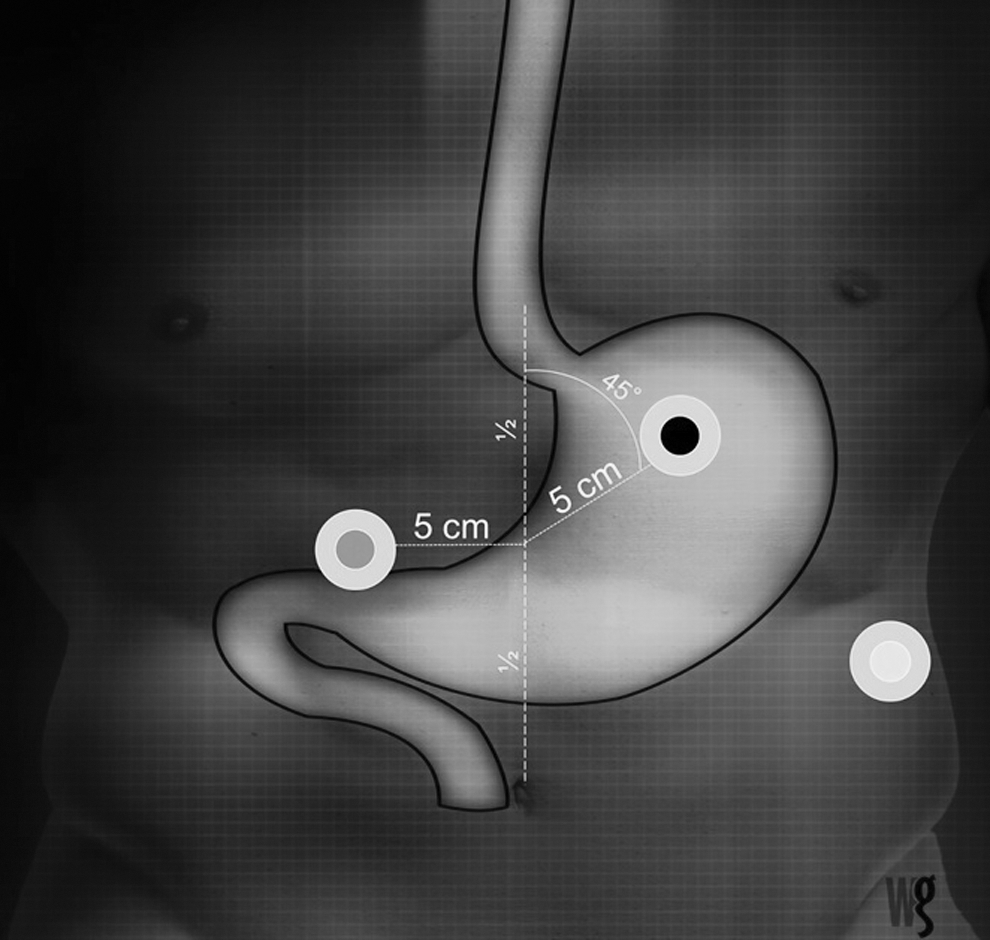
The gray electrode corresponds to the positive electrode of the EGG, the black electrode to the negative, and white to the ground. EGG, electrogastrography. Credit: William V. Grammar.
Protocol
After instrumentation and vital signs were taken, data collection began for 15 min pre-OMT and pre-time control to establish a baseline (preintervention). Then, either OMT (see Table 1 for techniques) or time control was performed for 8 min as described in detail below. After the intervention was completed, data were collected for an additional 15 min to document changes in measured variables immediately after OMT or time control. Subjects then initiated a WC, in which they drank ∼500 mL of purified water chilled to 16°C over 5 min. 12 To ensure an equal rate of gastric distention between visits, subjects drank 50 mL aliquots in 2–3 sec every half-minute for 5 min during each visit. Fifteen minutes of data were collected immediately after the WC to measure the effect of rapid gastric distention for OMT and time control visits.
Data analyses
Electrogastrography
The last 10 min of each recording period was analyzed, allowing each subject to have 5 min to reach a steady state. We have found in previous studies that this was normally adequate to achieve a stable baseline. EGG waveforms were bandpass-filtered at 0.0083–0.167 Hz to remove excessive noise and interference in the signal as well as to remove the effect of respiration. The EGG waveform was then scrutinized for motion artifacts, which were easily identifiable and removed. 8 PSD was then calculated for the EGG waveform as described previously. 8 Briefly, Hanning windows of software-determined size and overlap were applied to the EGG waveform and a PSD plot was generated using Fast-Fourier Transform using an EGG analysis software (Acqknowledge 4.3.0; BIOPAC Systems, Santa Barbara, CA). Power was then calculated for normogastric frequencies (2–4 CPM), bradygastric frequencies (0.5–2 CPM), tachygastric frequencies (4–9 CPM), and arrhythmic frequencies (9–18 CPM). Percent of normogastric, bradygastric, tachygastric, and arrhythmic frequencies was calculated by dividing the power of respective frequency range by the total power (1–18 CPM) in the signal according to the previously established standard. 8 DF was the frequency within 2–4 CPM that had the highest power, while dominant power was the power of the DF. 8
Analysis/statistics
Power analysis using preliminary data generated an effect size of 0.56. With an α of 0.05 and a power of 80%, preliminary power analysis suggested a sample size of eight subjects to achieve the targeted power. The absolute value of percent change in 2%–4% CPM (PPN), ΔDP, and ΔDF were calculated from baseline to postintervention and from baseline to post-WC. A two-(OMT vs. time control)-by-two (postintervention, post-WC) analysis of variance (ANOVA) with repeated measures was performed on the PPN, ΔDP, and ΔDF values. A Student–Newman–Keuls post hoc test was performed when an interaction effect became significant (p < 0.05) to evaluate differences within and between factors. A significance level (α) was set at 0.05. Data are reported as mean ± standard error of the mean (SEM) unless otherwise indicated.
Results
Effects of OMT on EGG percent power in the normal range, DF, and dominant power
For PPN values, repeated-measures ANOVA demonstrated no main effect of treatment (OMT vs. time control; p = 0.45) or time point (postintervention vs. post-WC; p = 0.08), but uncovered a significant interaction for treatment and time point (p = 0.01). Subsequent post hoc testing showed that OMT significantly altered the absolute percent change of PPN versus time control (time control: 5.3% ± 1.2%; OMT: 24.5% ± 4.5%; p = 0.015; Fig. 2). Furthermore, WC also significantly altered PPN compared with time control (post-time control: 5.3% ± 1.2%; WC post-time control: 30.3% ± 7.2%; p < 0.01; Fig. 3). However, WC did not alter PPN with prior OMT treatment (post-OMT: 24.5% ± 4.5%; WC post-OMT: 19.4% ± 5.6%; p = 0.47; Fig. 3).
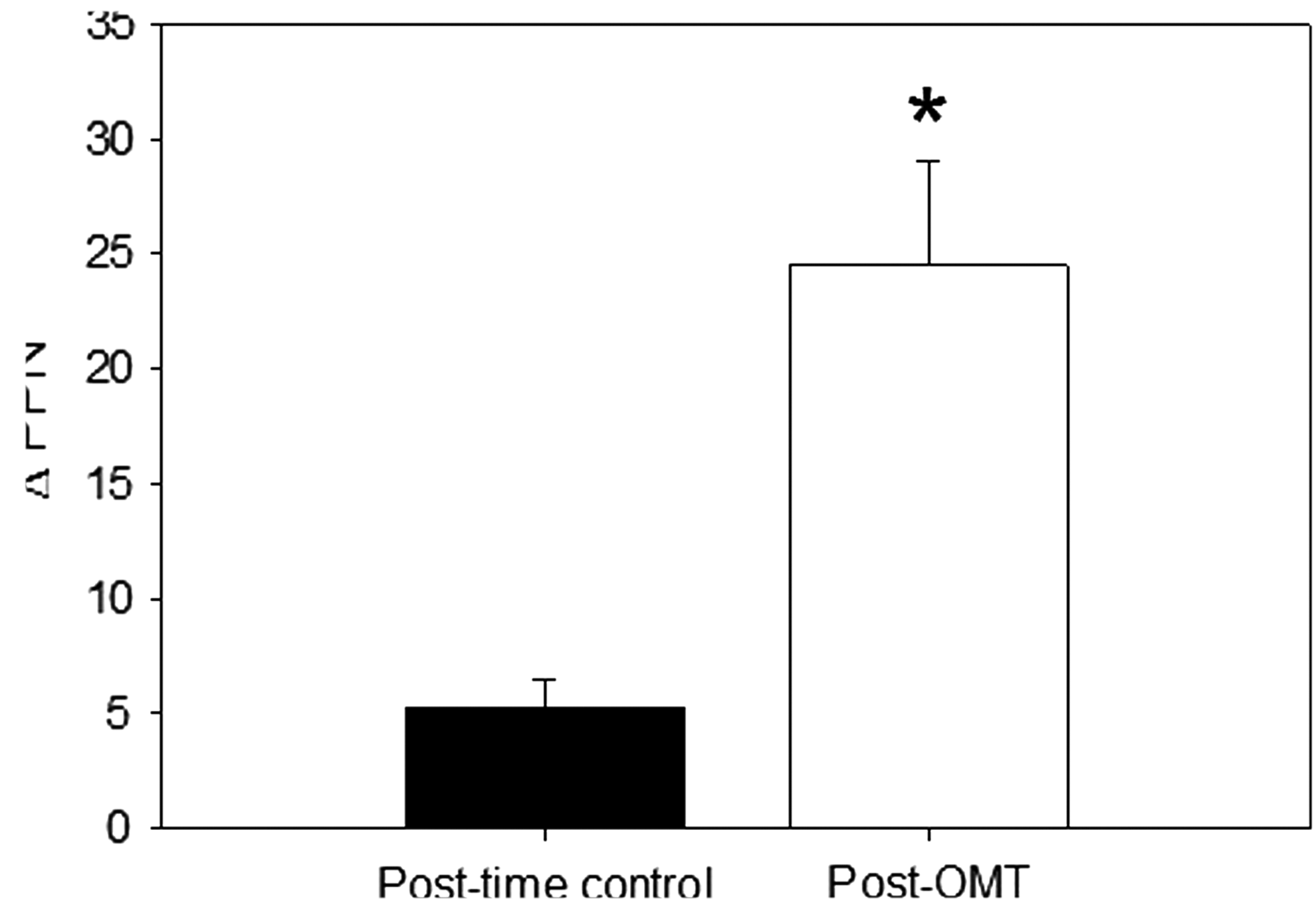
Postintervention comparisons of OMT and time control on GMA expressed as the absolute percent change of power in the normogastric range (PPN) postintervention, as measured by EGG. *p < 0.05. GMA, gastric myoelectric activity; EGG, electrogastrography; OMT, osteopathic manipulative treatment.
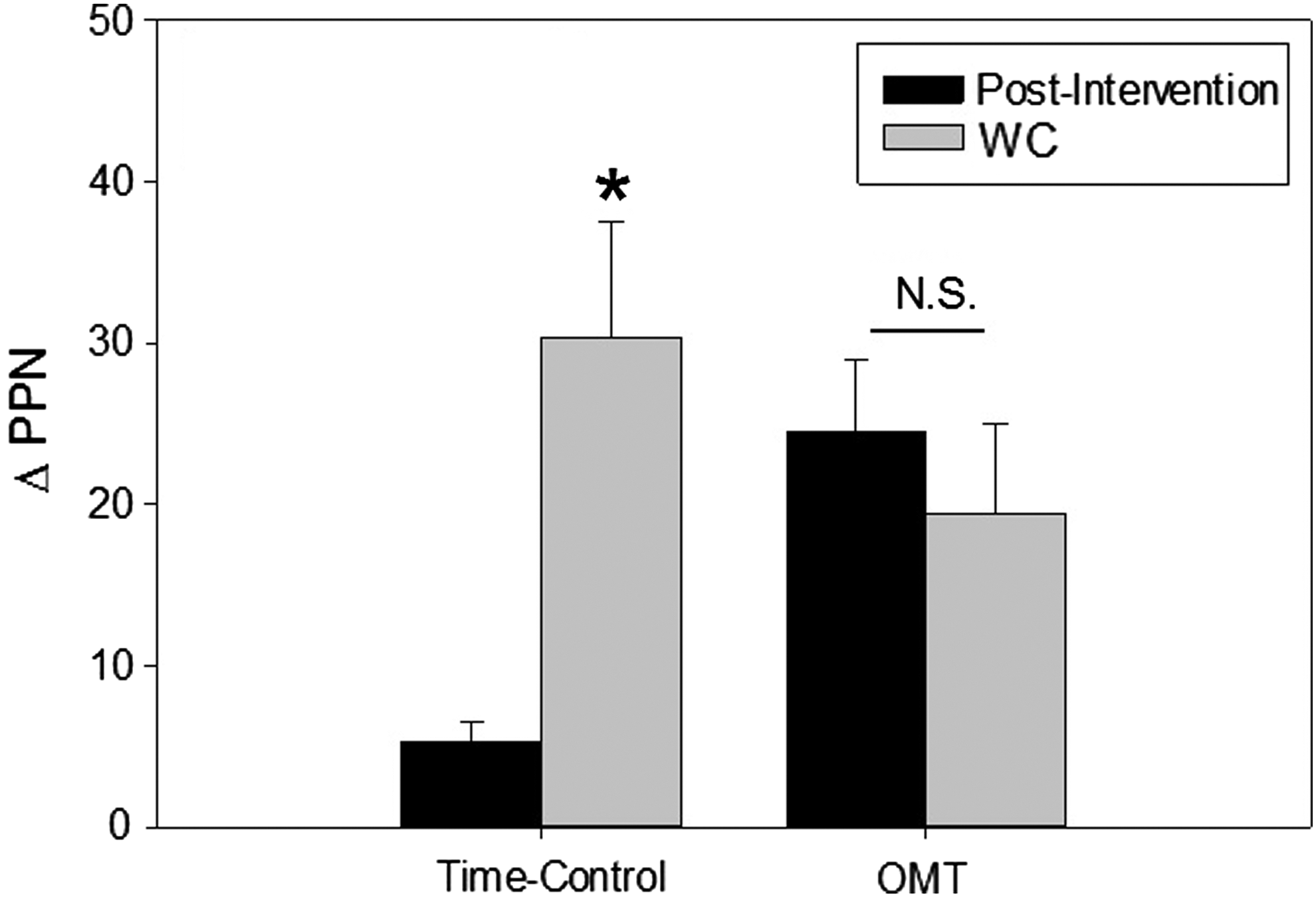
Effect of a 5-min WC with OMT as compared with time control expressed as the absolute percent change of power in the normogastric range (PPN). *p < 0.05 for time point. WC, water challenge; N.S., not significant; OMT, osteopathic manipulative treatment.
Similarly, for the percent change in ΔDF, repeated-measures ANOVA demonstrated no main effect of treatment (OMT vs. time control; p = 0.31), but showed a significant main effect of time point (postintervention vs. post-WC; p = 0.02) and a significant interaction between treatment and time point (p = 0.04). Post hoc tests demonstrated no significant effect of OMT itself on ΔDF (time control: 6.5% ± 1.8%; OMT: 12.9% ± 7.8%; p = 0.39, Fig. 4); however, OMT significantly modulated the response in DF to WC (WC post-time control: 37.9% ± 7.4%; WC post-OMT: 20.0% ± 5.9%; p = 0.02, Fig. 4). Furthermore, similar to the changes observed with PPN, the ΔDF response to WC was not significantly different from post-OMT (post-OMT: 12.9% ± 7.8%; WC post-OMT: 20.0% ± 5.9%; p = 0.40; Fig. 4), while the ΔDF response to WC was significantly greater than post-time control (time control: 6.5% ± 1.8%; WC post-time control: 37.9% ± 7.4%; p = 0.002; Fig. 4).

Postintervention and WC effects of OMT vs. time control on the absolute percent change in ΔDF. *p < 0.05 for time point, † p < 0.05 for time control vs. OMT. WC, water challenge; ΔDF, dominant frequency; N.S., not significant; OMT, osteopathic manipulative treatment.
With respect to dominant power, repeated-measures ANOVA uncovered no effects of treatment (p = 0.20), time point (p = 0.094), or interaction (p = 0.51).
Discussion
Our study demonstrated that (1) OMT significantly altered GMA compared with time control, and that (2) OMT reduced the rate of change in the frequency of gastric contraction (as expressed by DF) in response to WC and not the PPN response. To our knowledge, this is the first investigation documenting this physiologic alteration of GMA by OMT. Our study supports the notion that OMT increases gastric motility in healthy subjects and, in response to WC, alters the rate of gastric contraction without altering the power in normal frequency range. This preclinical evidence lends support to prior clinical findings that OMT can affect gastric function in patients with postoperative ileus and diabetic gastroparesis. 6,5 Whether this alteration is due to OMT modulating the autonomic nervous system (ANS) or through its direct mechanical effects remains to be determined.
The effects of OMT on GMA in this study have three possible sources, including modulation of (1) the ENS, (2) the ANS (sympathetic withdrawal or parasympathetic activation), and/or (3) direct mechanical effects. As the EGG measures the summated myoelectric potentials of sources intrinsic and extrinsic to the stomach, it is unclear whether the OMT performed altered GMA by altering ANS modulation of the ENS or by altering the ENS itself. Furthermore, it is well known that gastrointestinal smooth muscle increases contraction and peristalsis in response to mechanical stretch or distention, such as during passage of a food bolus. The WC provokes such a stimulus and demonstrates a clear change in GMA as measured. OMT, although not affecting the PPN response to WC, reduced the change in frequency of gastric contractions in response to rapid gastric distention (Fig. 4). This indicates that OMT modulates the response to gastric distention by altering contraction frequency within the normal frequency range. Hence, since OMT did not shift gastric contractions into brady- or tachykinesia, we speculate that OMT exerts a primarily physiological effect.
It is acknowledged that this study is limited by a relatively small sample size. Further, this study utilized a time control intervention and not a sham control, which does not rule out the possibility of a “placebo effect” of touch on the measured variables reported. The study design was not randomized, and the possibility of an order effect cannot be excluded. The exclusion of several subjects before the OMT intervention (secondary to artifact in their baseline recordings) could represent a form of selection bias. Additionally, our study made use of several OMT techniques that are thought to affect both sympathetic and parasympathetic branches of the ANS, and additional research is needed to determine which techniques alter which branch and what the extent of that alteration is. In addition, our study used one OMT technique (ganglion release) in which substantial pressure was applied to the area above the stomach and could provoke a mechanical effect on the GMA.
Conclusions
We conclude from our findings that OMT significantly alters GMA and that OMT alters the gastric contraction frequency within the normal range in response to gastric distention. Alteration of sympatho-vagal balance, direct mechanical stimulation to the stomach, as well as other effects of the ENS could be responsible, and future studies are warranted to investigate these potential independent effects. Nevertheless, this study provides preclinical evidence that there is a change in gastric motility as measured by EGG with OMT. We contend that this study will form the foundation for future investigations into the physiological effects of OMT on gastrointestinal function and its potential clinical use in conditions such as diabetic gastroparesis and postoperative ileus.
Footnotes
Acknowledgments
Authors' Contributions
M.L.S., N.P.J., and K.H. were involved in experimental design, while E.S., N.P.J., A.R., R.L., and J.W. performed data collection. N.P.J. completed data analysis. E.S. and N.P.J. prepared the article. Each author reviewed the article critically and contributed intellectually to the work.
Author Disclosure Statement
No competing financial interests exist.