
Abstract
Background:
Rheumatoid arthritis (RA) is characterized by pain, functional disability, poor quality of life (QoL), high socioeconomic impact, and annual costs of over $56 billion in the United States. Acupuncture (AC) is widely in use; however, studies show severe methodological shortcomings, did not consider the functional diagnosis for the allocation of acupoints and their results showed no differences between verum and control groups.
Objective:
The authors aimed to objectively assess the safety and efficacy of AC treatments for RA.
Methods:
105 RA patients with a functional diagnosis of a “Pivot syndrome” or “Turning Point syndrome” were randomly assigned to (1) verum-AC (verum acupoints), (2) control-AC (sham acupoints—points outside of the conduits/meridians and of the extra-conduits), or (3) waiting list (each group n = 35). AC groups experienced the exact same number, depth, and stimulation of needles. Assessments took place before and 5 min after AC with follow-ups over 4 weeks.
Results:
(1) Verum-AC significantly improved self-reported pain (Z = −5.099, p < 0.001) and pressure algometry (Z = −5.086, p < 0.001); hand grip strength (Z = −5.086, p < 0.001) and arm strength (Z = −5.086, p < 0.001); health status improved significantly (p < 0.001, Z = −4.895); QoL improved significantly in 7/8 survey domains; and number of swollen joints (Z = −2.862, p = 0.004) and tender joints (Z = −3.986, p < 0.001) significantly decreased. (2) Control-AC showed no significant changes, except in self-reported pain improvement. (3) Waiting list group showed an overall worsening.
Conclusion:
This is the first double-blind controlled study on AC in RA of the hand that objectively and specifically assesses positive effects supporting its integration in rheumatology. Acupoint allocation according to Chinese Medicine functional diagnoses is extremely relevant to assess AC effectiveness in a patient group primarily defined by a “western” medicine diagnosis. Based on clear allocation criteria for acupoints, the authors minimized the possible bias of unspecific and suggestive effects on the control group, showed the specific effects of the points chosen, improved efficacy, and identified an evidence base for AC.
Introduction
Rheumatoid arthritis (RA) is a chronic inflammatory autoimmune disease, characterized by pain, loss of physical function, and a reduced health-related quality of life (HRQoL). 1,2 The worldwide prevalence is estimated at 1% with at least twice as many women affected as men. 2,3 Over 90% of patients with RA have involvement of the wrist and small joints of the hand, including the knuckles and the middle joints of the fingers involving destructive polyarthritis of the synovium. 2,4 RA annual costs have been estimated at over $56 billion in the United States in 2016. 5 Thus, the socioeconomic impact is high on the individuals, on work-related problems like absenteeism, or on inability to work, as well as additional impacts on the health care system. 1,5
In recent decades, the treatment of RA has largely improved. However, patients frequently require therapy with analgesics, nonsteroidal anti-inflammatory drugs (NSAIDs), or glucocorticoids over a long time. These are not free of adverse drug reactions (ADRs) and show a high variability in treatment responses. 6 ADRs include NSAID-induced enteropathy with gastrointestinal ulcers, renal failure, and cardiovascular events. 7,8 Glucocorticoid use is limited for the development of serious ADRs such as loss of bone mass, infections, diabetes, hypertension, and others. 9 So-called disease-modifying antirheumatic drugs (DMARD) like methotrexate (MTX) may even limit family planning, 10 as women with RA are often of childbearing age.
Recently, efforts have been focused on using the class of drugs called biologics. 11,12 Although these agents reduce inflammation and joint destruction, their use is limited by their higher costs and severe side effects such as life-threatening infections and increased risk of malignancies. 11 –13
It seems understandable that an estimated 30% to 60% of RA patients use some form of complementary medicine, such as Chinese Medicine (CM) and its most widespread methodology acupuncture (AC). 14
AC effects on RA are contradictory; the studies show methodological shortcomings or are inconclusive. For example, standardized AC protocol results have not shown any differences between verum and control groups. 15,16 The type of intervention and stimulation, the number of sessions, unsuitability of the protocol for treating RA, and small sample sizes might have influenced the lack of efficacy of AC. Individualized AC protocols showed better results, but have methodological limitations due to inappropriate controls, inadequate quantification of AC effects, or lack of double blinding. 17 –20
A contemporary understanding of CM explains AC as a reflex therapy with both peripheral and central nervous system effects, thereby causing the release of neurochemical messenger molecules and biochemical, affective, and cognitive changes that influence the body's homeostatic mechanisms. 21 –23 It may promote the release of vascular and immunomodulatory factors, improve biomechanic functions, and can positively affect areas of the brain that reduce sensitivity to pain, stress, and inflammation. 24,25 These complex patterns of effects must match with the patient and his/her complaints.
One of the central problems of AC studies is how to systematically and effectively allocate acupoints to an individual. A set of acupoints may be effective in one individual with a certain pattern of symptoms, whereas others with the same Western diagnosis but other subsets of symptoms may not profit. These symptomatic distinctions are part of the CM diagnosis and may be due to the individual vegetative functional state of the patient that this functional diagnosis of CM may be defined, as described in detail previously. 23 To overcome this allocation problem, the authors decided to functionally homogenize the groups of their study by adding the underlying functional diagnosis of CM to the inclusion criteria. By this the authors tried to avoid mixing potential responders and nonresponders by not considering the functional basis for the allocation of acupoints, which may have resulted in showing no differences between verum and control groups and potentially impaired outcomes of previous AC studies. 15,16,26 By setting this inclusion criterion, the authors avoided individualizing to AC protocols which had shown better results but may have intensified patient's relation to the therapist, thereby possibly inducing more suggestive effects, and have limited proper blinding and double blinding. 17 –20 The diagnostic process was described in detail previously, 23,26,27 as well as the principle of targeting subgroups of patients most likely to respond. 26
The authors have observed in their department that RA patients with affection of the hand and pain worsened by grip in the fingers worse than in the knuckles or in the thumb, changeable temperature sensations and wandering complaints, present a clinical picture defined as Pivot syndrome (shaoyang pivot and shaoyin pivot, first described by Huang Di Nei Jing, the earliest existent canon of CM), also called turning point syndrome (TPS) in the Heidelberg Model to CM. 23,26,27
Basically, the pathogen agent algor/“cold” is fighting against the remaining levels of qi and xue in the extima/“exterior” alternated with exhaustion of the body mechanisms and, consequently, algor/“cold” proceeds to the intima/“interior.” However, sometimes it is repelled again. This imbalance elicits a set of autonomic signs that alternate continuously and are an underlying mechanism of shared symptoms or intermingled patterns, resulting in Pivot dysfunction or TPS symptoms to arise. Concomitantly, an increase of microcirculation signs related to the shaoyang (Felleal/“Gallbladder” and Tricaloric/“Sanjiao” conduits and respective body islands), and lack of microcirculation signs related to the shaoyin (Cardial/“Heart” and Renal/“Kidney” conduits and respective body islands) are present. 23,26,27
The neuroimmunologic pathways involved in RA, especially inflammation and pain, may be understood by the Shang Han Lun (theory on cold damage) or algor leadens theory, and it can only briefly be mentioned in this study. 23,27,28
To truly objectify the outcome of the treatment, the authors assessed both patient reported outcomes (PROs) and objectively measurable physical parameters in a double-blind, prospective randomized clinical trial. The authors were aiming to objectify specific AC effects based on clear allocation criteria for acupoints by objectively assessing outcomes utilizing valid scientifically recognized benchmarks for assessing the safety and efficacy of RA treatments, which by nature cannot fully be captured by clinical laboratory markers.
Methods
Patient's selection
The study was conducted at the Experimental Pathology and Acupuncture Department of the Faculty of Medicine, University of Coimbra, Portugal. Patients were enrolled from September 2015 to December 2017, after approval of the respective committee according to the Helsinki declaration, using media resources distributed to rheumatology departments in Coimbra and RA national associations.
The authors included patients with RA of the hands if they had (1) previously signed an informed consent, (2) active RA fulfilling the American College of Rheumatology criteria as assessed by an independent rheumatologist not involved in the study, (3) chronic pain over a minimum period of 3 months before recruitment, (4) had current pain greater than 30/100 mm on a Visual Analog Scale (VAS) despite medication and stable dose treatment for at least 3 weeks, (5) impairment of hand strength, (6) pain worsened by grip in the fingers worse than in the knuckles or in the thumb, and (7) showed the clinical picture of a pivotal or TPS according to the criteria defined previously 23,26,27,29 and diagnosed by a CM practitioner with a master degree in CM.
Patients were excluded from this study if they (1) were under the age of 18 years, (2) were pregnant, (3) previously had AC, (4) suffered from local skin infections, (5) had severe chronic or uncontrolled comorbidities, (6) hand pain worsened by grip in the knuckles or in the thumb, (7) or seemed to be seeking for economic benefits, that is, by applying for a pension during the study.
All patients were under stable doses of biomedical combination therapies, including NSAIDs, DMARD, biologics, and analgesic drugs, and were instructed not to change their usual therapies during the study.
Design of the study and double blinding
After checking the inclusion and exclusion criteria during a first visit by the “diagnosing acupuncturist” (referred to in this article as S.S.), patients were randomly assigned in a 1:1:1 ratio by a computer-generated randomization program to verum, control, or waiting list group during a second visit. Outcome measures were assessed for the first time (baseline) after randomization. Patients randomized to the verum and control AC (CAC) groups received three treatment sessions in the first week. After the first week, they were treated twice per week over a period of 3 weeks, with a minimum interval of 72 h in between treatments and continued conventional treatment as before. Waiting list patients did not receive AC treatments but continued their usual treatments.
Double blinding was achieved as described previously by their group.
30,31
In brief, this four-step procedure included: assessment of baseline values and acupoint allocation by a physician unaware of the allocation of the groups. all the patients received the same approach: measurement and marking the verum acupoints and sham acupoints by dots in different colors by a physician unaware of the allocation of groups or acupoints and their colors, leaving the patients unaware of the meaning of the colors (blinding of the patient). The allocation of colors and patients was randomly changed by a randomization computer program. The “therapists” were western medical doctors and at the same time novices to AC, unaware of the meaning of the points or the symptoms of the patients. These “therapists” were informed by the randomization computer program about the color of the points that were supposed to be needled and instructed to maintain a standardized method as to needle insertion or needle stimulation throughout all the sessions (blinding of the “therapist”). After each AC session, the patients were dressed with a light garment to cover any potential marks from needling, to hide the treatment received, and post-treatment assessments were performed by a person unaware of the allocation of groups or acupoints and their colors (blinding of the observer).
Weeks after the final assessment, the participants treated with AC were contacted and specifically asked to state their group by selecting one option: “real acupuncture” or “false acupuncture.”
Outcome measures
Primary clinical outcomes
Pain in general was measured with a VAS ranging from 0 (no pain) to 10 (maximum pain). Pain pressure threshold in the hand of RA patients was measured with a pressure algometer (PA) device, specifically designed by us to objectively assess the hand pressure tolerated by RA patients. 32 Measures of arm strength (AS) and hand grip strength (HGS) were assessed with a Jamar® Hydraulic Hand Dynamometer (Patterson Medical®).
All the primary outcomes were assessed before the AC treatments at specific times (T): T0, T2, T4, T6, T8, T10, T12, T14, and T16, and 5 min after the AC treatments at: T1, T3, T5, T7, T9, T11, T13, T15, and T17. Primary clinical outcomes were assessed at baseline (T0) and 4 weeks after the first visit (T17) in the waiting list group.
Secondary clinical outcomes
Functional ability and health status were assessed with the Disability Index of the Health Assessment Questionnaire (HAQ), a PRO that assesses eight subscales: arising, common daily activities, dressing and grooming, eating, grip, hygiene, reach, and walking. The HAQ subscales ranged from 0 (no difficulty) to 3 (unable to do).
HRQoL was assessed using the Medical Outcome Short Form-36 Health Survey (SF-36). SF-36 consists of a self-assessment tool that measures personal and individual functional health and well-being parameters. The scores ranged from 0 (worst) to 100 (best) for each of the eight domains (bodily pain, general health, physical functioning, role-physical, mental health, role-emotional, social functioning, and vitality). The authors established the minimum clinically important difference for assessing improvement or deterioration as a 2.5 to 5 point difference from baseline.
Other secondary outcomes included disease activity score-28 for RA, which includes the number of tender and swollen joints, and the grade of inflammation by the erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) blood levels.
Secondary clinical outcome assessments were assessed at baseline (T0) and 4 weeks after the first visit (T17).
Intervention
The patients allocated to the verum AC (VAC) group were treated with a specific choice of points of the affected conduits/“meridians”: San Jiao 5 (tricaloric 5, TC5/triple burner, TB5), (clusa externa/Waiguan); Felleal 39 (F39)/Gallbladder 39 (GB39), (campana suspensa, Xuanzhong); Cardial 3 (C3)/Heart 3 (HT3), (mare minus, Shaohai); and Renal 7 (R7)/Kidney 7 (KI7), (amnis recurrens, Fuliu). 23
The patients allocated to the CAC group were treated with the exact same number, depth, and stimulation of needles, but not according to the CM diagnosis, and on points allocated in areas close to the real acupoints but at nonacupoints.
The acupoints and the nonacupoints were stimulated using sterile subcutaneous needles (0.30 mm × 8 mm) (BD Micro-Fine®) 29 using the Leopard Spot technique (bloodletting or fang xue acupuncture), a way of dispelling “blood” (xue) stasis described in the third century. 33
The “therapists” were trained to execute the Leopard Spot technique by pricking quickly the points (five times per point, three to five blood drops per point) with the color indicated by the randomization computer program.
Statistical analysis
Each categorical variable was described by its absolute and relative frequencies, while each quantitative variable was described by its median, 25th percentile, and 75th percentile. Chi-square and Fisher tests were used to assess the association between categorical variables. Shapiro–Wilk tests were performed to assess the normality of quantitative variables. When they were normally distributed, analysis of variance was used to verify whether statistically significant differences exist among the verum, control, and waiting list groups. When the normality requirements did not hold, Kruskal–Wallis tests were used instead. When the comparisons were performed between only two of the groups, Student's t tests or Mann–Whitney tests were used, as applicable. Within each of the three groups, Wilcoxon tests were used to assess whether quantitative outcomes were altered with statistical significant differences between the baseline and after the last treatment. The analyses were performed on IBM SPSS Statistics 24 and on R 3.3.2. The significance level adopted was 0.05.
Results
Recruitment rate and baseline characteristics
Of the 284 RA patients enrolled, 151 (79.5%) RA participants showed pain worsen by grip in the fingers more than in the knuckles or thumb, and 147 of these patients were diagnosed, according to the CM diagnose process, with the TPS (Fig. 1).
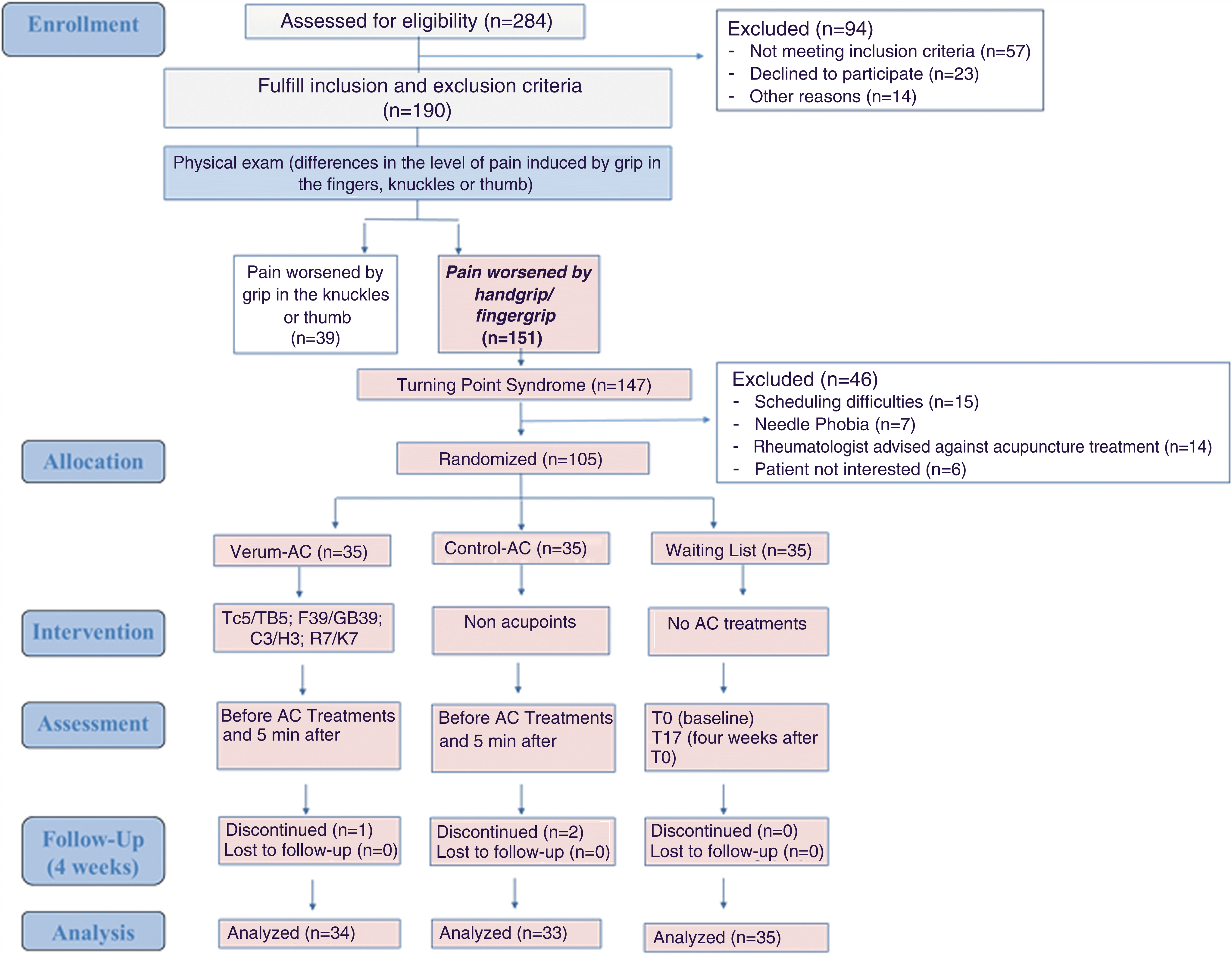
CONSORT 2010—Flow Diagram. Study flow diagram and patients' progress through the trial. AC, acupuncture. Color images available online at
Of those 147 eligible patients, 105 patients were randomized. The study flow chart and the reasons for discontinuation are shown in Figure 1.
Demographic, clinical features, and CM functional vegetative state assessments, according to the symptoms and signs manifested by RA patients, with hand pain worsening by handgrip (n = 105), at baseline are described in Table 1. There were no significant differences in baseline characteristics between the three groups.
Demographic and Clinical Characteristics (Baseline)
Data are presented as number (frequency); mean ± standard deviation or median (first quartile, third quartile). There was no significant difference in any of the characteristics between the three groups.
AC, acupuncture; BMI, body mass index; DMARD, disease-modifying antirheumatic drugs; F, female; M, male; NSAID, nonsteroidal anti-inflammatory drug.
Clinical efficacy
At baseline, there were no significant differences in the primary outcomes between the three groups. At the end of the treatment, all VAC patients significantly improved in HGS (p ≤ 0.001), AS (p ≤ 0.001), VAS (p ≤ 0.001), and PA (p ≤ 0.001). The CAC patients showed only self-reported pain improvement, VAS (p ≤ 0.001). In the waiting list group, there was no change from baseline in AS and VAS, while there was a significant worsening in HGS (p ≤ 0.029) and PA (p ≤ 0.001) (Table 2) (Fig. 2). At the last assessment, the differences in all the primary outcomes between groups were significant (p < 0.001) (Table 2).
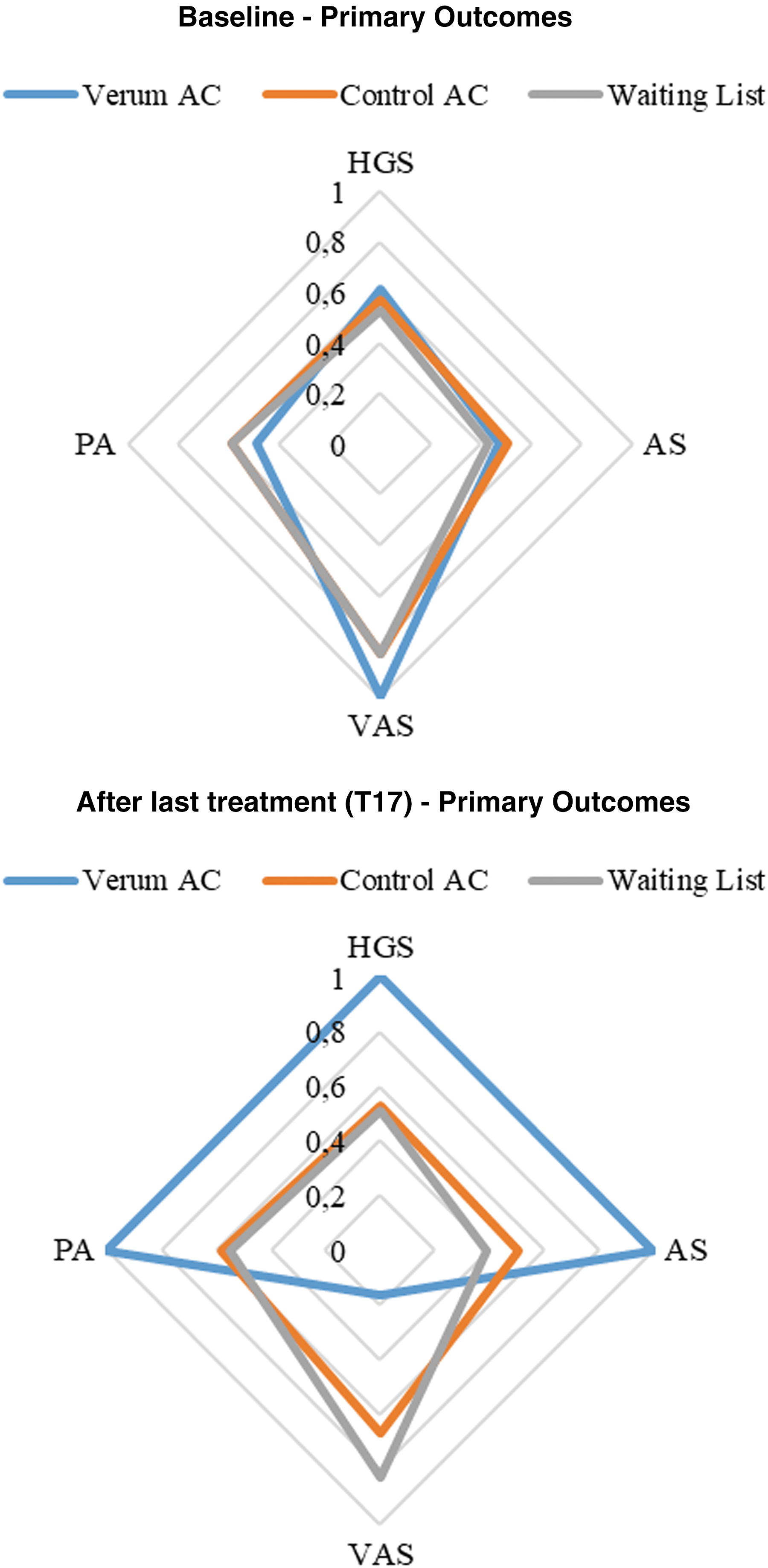
Primary outcome changes for the three groups of patients. A radar plot is displayed for each group (verum AC, control AC, waiting list), in which the different SF components are shown. To enable an easy visualization, the normalized medians are shown for each group and for each variable. The normalization procedure consisted of dividing, for each group and each variable, the corresponding median with the maximum of the six medians obtained, over all the groups, for that variable. AC, acupuncture; AS, arm strength; HGS, hand grip strength; PA, pressure algometer; VAS, Visual Analog Scale. Color images available online at
Clinical Outcome Changes for the Three Groups of Patients
Data are presented as median (1st quartile; 3rd quartile). p-Value adopted was 0.05, * p < 0.05 comparing before and after treatment.
AC, acupuncture; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; HAQ, Health Assessment Questionnaire; kgf, kilogram force; p-value, probability value; SF-36, Short Form-36 health survey; VAS, visual analog scale.
Patients in the VAC group showed significantly better outcomes compared to CAC group for all outcome measures, in particular after T3 for VAS, after T5 for PA, after T7 for AS, and after T11 for HGS. Figure 3 summarizes strength (AS and HGS) and pain (VAS and PA) changes during AC treatment in VAC and CAC groups (Fig. 3) (Table 2).
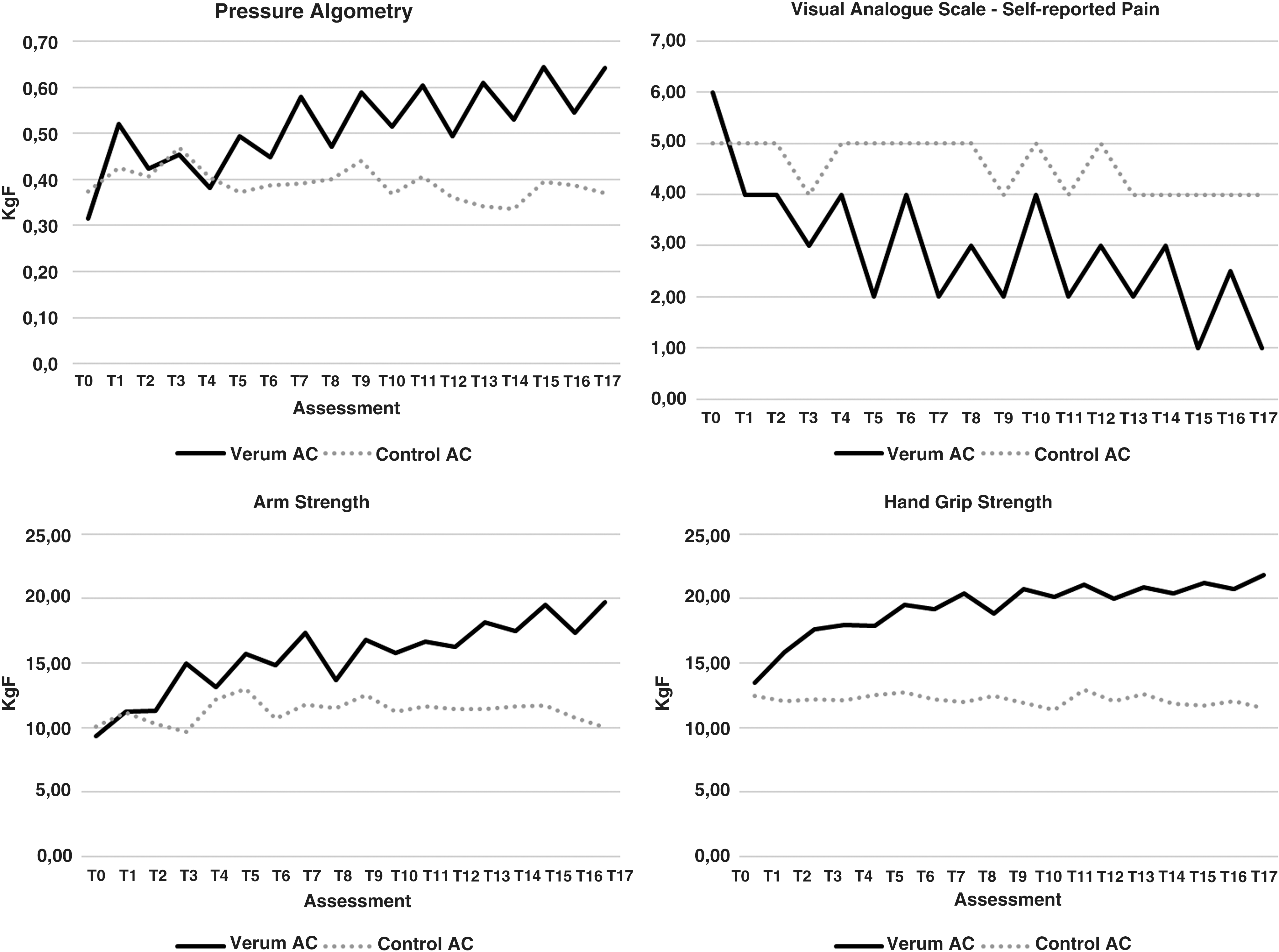
Primary outcome changes for the groups treated with AC. AC, acupuncture.
With respect to secondary outcomes, at baseline, the SF-36 bodily pain domain was significantly worse in the VAC group, and the number of tender joints was significantly higher in the CAC group compared to the other groups (Table 2). Also at baseline, the median scores of the SF-36 assessments showed that physical function was the most compromised domain and mental health the least.
Secondary outcomes analyzed after 4 weeks showed that HAQ scores significantly decreased in the VAC group, while there was no change in the CAC group and an increase in the waiting list group; verum AC improved significantly 7/8 SF-36 domains, while sham AC improved significantly only 5/8 SF-36 domains, and the waiting list group showed a statistically significant worsening of 5/8 SF-36 domains (Table 2) (Fig. 4). The number of swollen and tender joints significantly decreased in the VAC group, while there was no change in the CAC and waiting list groups (Table 2) (Fig. 4). There were no changes within groups and between groups for ESR and CRP (Table 2) (Fig. 4).

Secondary outcome changes for the three groups of patients. A radar plot is displayed for each group (verum AC, control AC, waiting list), in which the different SF components are shown. To enable an easy visualization, the normalized medians are shown for each group and for each variable. The normalization procedure consisted of dividing, for each group and each variable, the corresponding median with the maximum of the six medians obtained, over all groups, for that variable. AC, acupuncture; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; HAQ, Health Assessment Questionnaire; HRQoL, health-related quality of life; SF-36, Short Form-36 health survey. Color images available online at
All the participants remained on stable doses of existing medications. Therefore, medications are unlikely to represent a confounding factor in the analyses presented.
Throughout the period in which the study took place, AC treatments were well tolerated. No side effects were reported except for minor bleeding at the site of needle insertion.
The patients treated with AC gave an opinion of their treatment group after the study had been completed. Eighty-one percent of the AC group and 82% of the sham group replied. Of the replies 14 of the VAC (41%) and 15 of the CAC (44%) correctly named their treatment allocation. These were not significantly different (Chi-square test, p = 0.39). Twenty-three percent of those that had AC and 15% of the CAC group wrongly guessed their treatment allocation.
Discussion
Their results clearly indicate a relevant clinical effect of AC on RA of the hand in patients suffering from TPS. The authors used the exact same number, depth, and stimulation of needles in the VAC and CAC groups so that the authors could identify if one group of points works better than the other. It is not like the usual “explanatory” placebo trial where the verum AC technique is compared to one placebo strategy. As the effects were shown in a double-blind manner, a mere placebo or suggestive AC effects can be excluded, and the differences between the AC groups can therefore be considered to be specifically induced by the acupoints used.
The rigorous design of this randomized controlled clinical trial also avoids other major problems of AC studies such as nonspecific effects, weak allocation of acupoints, or lack of objective assessment of effects.
Nonspecific AC effects may depend on the depth of penetration, which has consequences for study designs or control interventions to be chosen. The authors decided not to use streitberger placebos, shallow 2 mm needlings, or pyonex controls, because the depth of penetration is zero or low. Therefore, the authors would compare high depth of needling in the verum versus low depth of penetration in controls. This is the reason why the authors chose the same number of needlings and mode of stimulation techniques in verum and control interventions to minimize the influence of unspecific effects. Specific effects of acupoints can only be shown if the verum intervention is maximally effective in comparison to unspecific and suggestive effects of the control intervention. Therefore, the authors included the CM diagnosis according the Heidelberg Model of CM.
It is interesting to note that in their study sham AC only improved significantly the self-reported pain (VAS scores), a subjective outcome and tendentially (but not significantly) improved 5/8 SF-36 domains, but in objectively measurable parameters (AS and HGS), as well as the functional status assessed by the HAQ, no change or even worsening was observed. This shows how important double blinding, randomization, and objective assessment of AC effects are, as they help to discriminate and quantify suggestive and placebo effects of sham and verum acupoints. In their case, sham points showed no significant changes, indicating that acupoints truly make a difference over unspecific skin points in clinical efficacy, which was frequently doubted in the past. 34 The authors could repeatedly show this in a double-blind manner and by objective assessment methods for indications like gait disorders in the elderly 30 or pain in the knee. 31
To carry out this study, the authors needed to develop a specific PA to assess the pain tolerance threshold of RA patients with hand pain whose features are related to the TPS. 32 The device was tested in a small group of 14 RA patients with the TPS before the authors performed this double-blind randomized controlled trial. 32 The authors acknowledge that such a device may have certain limitations such as the nonapplicability to other syndromes, a noncomparability with devices already created, and that the authors may not have enough data to validate this specific device for other studies, and finally, the fact that it doesn't have a patient controlled “stop” button. Thus, the authors recognize that caution is required in the interpretation of clinical findings when using such a device. 32
Although the authors can clearly state the objectivity and specificity of the effects shown, the study also raises a couple of questions like the mechanisms behind, sustainability of effects, and the options of combinations with given conventional therapies. In addition, the blinding of “therapist” novices to AC can be regarded as a weakness.
Bloodletting AC is considered a technique that removes “blood” (xue) stasis. It has been shown that the bleeding of acupoints induces cell proliferation and migration, particularly of fibroblasts, modulates cytokines, growth factors, and inflammatory mediators, as well as improves tissue oxygenation and decreases oxidative stress and edema. 35,36 In addition, it can also relieve pain, stimulate the medullary hematopoiesis through neuro-humoral regulation, and promote tissue regeneration. 37 Given the benefit seen in the VAC group, the bloodletting of the verum acupoints must have activated sensory receptors in the conduits affected by the TPS and helped to rebuild homeostasis regarding edema. 35,38 This potential mechanism would also be supported by the lack of changes in serum ESR and CRP, which point to an effect of AC on the microcirculation rather than on inflammation.
However, the fact that bloodletting AC changed pain, function, strength, and HRQoL but not inflammatory parameters like CRP in their study suggests that vegetative and nervous mechanisms may be more involved in their setting than anti-inflammatory effects.
In addition, the authors saw a quick onset of symptomatic relief within 5 min that continued to improve throughout the period of 4 weeks, as shown by the VAC. The authors speculate that the velocity of the effects can hardly be explained by primary induction of complicated anti-inflammatory biochemical pathways, which is also compatible with the reflex and central nervous system mechanisms behind the effects seen. One of the potential changes of vegetative functions may include an increase of microcirculation as shown earlier, 39 which may contribute to pain relief and reduction of functional disability. 35,36,38
After 4 weeks treatment, patients treated with verum AC improved across all clinical symptoms except inflammation measured by CRP, which resulted in less pain, better functional ability, and improved HRQoL. AC, a nonpharmacologic and nontoxic technique, was an effective and well-tolerated treatment. Further research is needed to explore whether long-term effects can be obtained and if treatment variations may be necessary to achieve this.
The treatment underlying their study was developed in the Heidelberg School of CM, where treatments of RA have frequently been performed for two decades in a similar manner as standard intervention. After the intensive treatment of 4 weeks, frequency is gradually reduced to one session every 3 weeks and symptoms remain on a comparable level. However, this should be examined and objectified by follow-up studies.
Based on the observations of this study, the authors can now estimate that a sample size of 37 patients in each group, to an expected effect size of 0.2 (f = 0.2), with an alpha value of 0.05 (α = 0.05), would be required for a 95% power.
Combination of this therapy with conventional treatments is not only an option but also will remain a necessity according to their clinical experience. There is no cure for RA, and the goals of treatment are considered to minimize symptoms, to prevent deformity of joints and control inflammation, and to maintain day-to-day function. 40 Clinical experience and common sense may support the thesis that some reduction of RA medication may in the future be achieved by follow-up studies, but this remains speculation until data on that are systematically acquired.
In this context, the role of AC in rheumatology should be reconsidered as complementation but not replacement of conventional therapies, with the allocation of individual acupoints following the scientific rules quoted. 23,26,29
Follow-ups concerning sustainability and potential reduction of RA-associated medications are necessary, as well as toward the question of extending these positive results to other joints and possible extra-articular manifestations of RA.
Footnotes
Acknowledgments
The authors gratefully acknowledge the support of Nikki Wird, a native English speaker who reviewed the language. The authors thank Andréa Marques, Ricardo Ferreira, Elsa Santos, and Juliana Paciência for help by the recruitment process and Professor Jorge Machado for the pressure algometer acquisition.
Authors' Contributions
Study conception and design S.S. and H.J.G. Acquisition of data S.S., A.S.C., and S.K. Analysis and interpretation of data S.S., M.P., and H.J.G. Quality control of the clinical study S.S., A.S.C., S.K., and H.J.G. Article drafting and critical revision S.S., G.F., and H.J.G. All authors give final approval of the version to be submitted and any revised version.
Additional Information
Trial registration: clinicaltrials.gov Identifier: NCT02553005.
Ethical approval: This trial ethics review boards of the Faculty of Medicine–University of Coimbra (ref. CE-048/2015). All patients were asked to provide written informed consent before participating.
Transparency: The authors affirm that the article is an honest, accurate, and transparent account of the study being reported; that no important aspects of the study have been omitted; and that any discrepancies from the study as planned have been explained.
Author Disclosure Statement
No competing financial interests exist.