
Abstract
Objectives:
Physical therapy (PT) modalities are used in the treatment of fibromyalgia syndrome (FMS). Acupuncture is a treatment option often sought after by FMS patients. The aim of this study was to compare the effects of PT modalities with those of acupuncture on pain, daily function, and quality of life in FMS patients.
Design:
A comparative effectiveness study.
Setting and Subjects:
Forty-four female patients between the ages of 18–70 years presenting to Baskent University Faculty of Medicine Department of Physical and Rehabilitation Medicine with a new diagnosis of FMS according to the American College of Rheumatology, with manifestations of chronic widespread musculoskeletal pain symptoms, normal routine blood tests, and a desire to receive PT or acupuncture were included in the study. Exclusion criteria included the presence of neurologic, inflammatory, endocrinologic, and other chronic diseases, psychiatric illness, use of antidepressants or analgesics, and contraindication to treatment with PT modalities.
Interventions:
One group (n = 22) received 15 sessions of hotpack, transcutaneous electrical nerve stimulation (TENS), and ultrasound to the tender points of the cervical and upper back regions. The other group (n = 22) received 10 sessions of formulated acupuncture aimed at treating pain of the neck, upper, and lower back regions.
Outcome measures:
Pain, functionality, and quality of life measured using the Short Form McGill Pain Questionnaire (SF-MPQ) and Fibromyalgia Impact Questionnaire (FIQ) before and after treatment.
Results:
There was a reduction in all SF-MPQ domains and FIQ scores after treatment in both the PT and acupuncture groups. There was no difference in pre- and post-treatment scores between the two groups.
Conclusions:
PT modalities and acupuncture can be effectively used in the treatment of FMS. Even though one treatment option was not found to be more beneficial than the other, longer post-treatment follow-up may help determine the superior treatment option.
Introduction
Fibromyalgia syndrome (FMS) is associated with widespread pain, symmetrically distributed tender points, and accompanying systemic symptoms and pathologies such as fatigue, sleep disturbance, depression, and anxiety. 1,2 FMS is seen in ∼1%–11% of the general population, showing a preponderance for women between the ages of 40 and 60 years. 3
Traditionally, the treatment options for FMS are multimodal and multidisciplinary and include patient education, psychotherapy, cognitive behavioral therapy, physical therapy (PT) and exercise, hydrotherapy, and pharmacologic intervention. 4,5
The positive effects of exercise on reducing pain and improving physical function in FMS are well established. 6 The most recent European League Against Rheumatism guidance on the treatment of FMS emphasized that based on review of the meta-analyses to date, exercise is the only therapy-based intervention that comes strongly recommended. 7 The same report recommends that initial management should include patient education and nonpharmacologic interventions.
Transcutaneous electrical nerve stimulation (TENS), hotpacks, ultrasound, massage, and manipulation have also proven to be beneficial in reducing pain and are frequently the PT modalities of choice. 8 –10
More recently, traditional and complementary medicine (TCM) such as acupuncture, t'ai chi, and hypnosis have been recommended in certain guidelines. 11,12 Acupuncture is a Traditional Chinese Medicine that has been used in the treatment of chronic pain for >2000 years. Acupuncture is one of the most frequently used TCM interventions in FMS; it has been reported that one in five FMS patients seeks acupuncture treatment within 2 years of diagnosis. 4 Recent human and animal studies have shown that insertion of an acupuncture needle into acupuncture points activates the pain control pathway that increases plasma and central nervous system endogenous opioid and serotonin release. This has an analgesic, anti-inflammatory, and sedative effect on the patient. 13 –15
A number of studies have been done on the use of acupuncture in the treatment of FMS. 16 The recommendations of the American Pain Society and German Association of Scientific Medical Societies include treatment with acupuncture with a level of evidence of II and Ia, respectively. 17 However, recent meta-analyses concluded that there is not enough evidence to prove the efficacy of acupuncture therapy in the treatment of FMS. 11,18,19 Furthermore, there is an emphasis on the need for further studies comparing acupuncture with more traditional Western treatment modalities, including PT modalities.
Therefore, the aim of this study was to compare the effects of treatment with conventional PT modalities used in Western medicine with those of acupuncture on pain, daily function, and quality of life in FMS patients, thereby determining the superiority of one treatment option over the other.
Materials and Methods
Design and participants
Forty-four consecutive female patients presenting to the Baskent University Faculty of Medicine, Physical Medicine and Rehabilitation (PMR) Outpatient Clinic, who went onto receive a diagnosis of FMS by a PMR specialist, according to the criteria for the diagnosis of fibromyalgia from the American College of Rheumatology (ACR), 20 were included in the study.
Inclusion criteria were (1) a new diagnosis of FMS; (2) manifestations of chronic widespread musculoskeletal pain symptoms; (3) female sex; (4) age 18–70 years; (5) full blood count, erythrocyte sedimentation rate, C reactive protein, urea and electrolytes, liver function tests, and urine dipstick values within the normal limits; and (6) agreeing to attend PT/acupuncture sessions. Exclusion criteria were (1) presence of neurologic, inflammatory, endocrinologic, and chronic diseases such as chronic renal insufficiency; (2) severe physical disability; (3) psychiatric illness; (4) use of antidepressants or regular use of analgesics; and (5) contraindication to the use of TENS, such as the presence of a cardiac pacemaker.
The selection and recruitment were conducted in accordance with the declaration of Helsinki of 1975, as revised in 1983, and all subjects signed a written informed consent form before their inclusion in the study. This study received ethical approval by the Baskent University Faculty of Medicine and Health Sciences Ethics and Research Committee before commencement.
Group allocation
The patients who received a new diagnosis of FMS and met the inclusion–exclusion criteria of the study were assigned to one of two treatment groups. Patient allocation to treatment groups was conducted by a separate clinician not involved in the study, nor in the initial assessment and diagnosis of the patient, and was based on the patient's folder number.
On initial presentation to the hospital, every patient was allocated a new folder and folder number by the admissions staff. This is a number separate to that of the patients' hospital number seen by the assessing clinician on the hospital computers. Those with a folder number ending in an even number were assigned to the physical modality group, whereas those with a folder number ending in an odd number were assigned to the acupuncture group.
Those in group one (n = 22) received PT, those in the group two (n = 22) received formulated acupuncture. All the patients included in the study were evaluated by a second PMR specialist before and at the end of the course of treatment. This PMR specialist was blind to the treatment received by the patients; the patients were reminded not to disclose information regarding their treatment to the specialist.
Patient evaluation included demographic details, symptom duration, and assessment of the patients' pain and quality of life. Pain and quality of life were assessed using the Fibromyalgia Impact Questionnaire (FIQ) and Short Form McGill Pain Questionnaire (SF-MPQ).
Outcome measures
Outcome measures were assessed before the first treatment session (baseline data) and 24 h after the last treatment session had been completed by the same blinded PMR specialist. Clinical and demographic information included age, weight, height, body mass index, employment status, and symptom duration.
The primary outcome measure of this study was pain, the various different aspects of which were assessed using the SF-MPQ. FIQ scores were the secondary outcome measures.
The SF-MPQ is a multidimensional pain questionnaire designed to measure the sensory, affective, and evaluative aspects of pain and its intensity. 21 The SF-MPQ can be used to evaluate the effectiveness and efficacy of pain interventions 22 and its reliability and validity are well established. 23 The main component of the SF-MPQ consists of 15 descriptors (11 sensory and 4 affective), which are used to identify the sensory and affective dimensions of pain. The 15 descriptors are rated on an intensity scale as 0 = none, 1 = mild, 2 = moderate, or 3 = severe. Three pain scores are derived from the sum of the intensity scale scores using the words chosen for sensory (MPQ1), affective (MPQ2), and total descriptors (MPQ3).
The SF-MPQ also includes determination of a visual analogue scale (VAS) score from 0 to 10 cm for current pain (MPQ4) and a present pain intensity (PPI) index score (MPQ5) rated on an intensity scale of 0 = no pain, 1 = mild pain, 2 = discomforting, 3 = distressing, 5 = horrible, and 6 = excruciating. 22 The final score ranges from 0 to 60 with higher scores indicating greater pain levels.
The FIQ was used to assess the impact of FMS on the patient. 24 The Turkish version of the FIQ, whose validity and reliability have been studied and proven, 25 was used in this study.
The FIQ assesses the patient's physical function, work status and well-being, depression, anxiety, morning tiredness, pain, stiffness, fatigue, and well-being over the past week and is composed of 20 items. 26 The first 11 items assess physical function scored on a Likert scale of 0–3 points. Questions 12 and 13 assess the patient's well-being and work status by assessing how many days the patient felt well over the past week and the number of days they were unable to work (including house work) due to FMS symptoms. The remaining seven items of the questionnaire are assessed using a VAS from 0 to 10 cm marked in 1 cm increments on which the patient rates work difficulty, pain, fatigue, morning tiredness, stiffness, anxiety, and depression.
Once the initial scoring has been completed, the scores are subjected to a normalization procedure so that all scores are expressed in similar units. The final score ranges from 0 to 80. Higher scores indicate greater impact of FMS on the patient.
Interventions
PT modalities
A total of 15 sessions (five consecutive sessions per week lasting 1 h each) of hotpack therapy (heated to 71°C–74°C for 20 min), TENS (at a frequency of 100 Hz, intensity adjusted to the patient's tolerability for a total of 20 min), and ultrasound (1 MHz, 1.5 W/cm2 for a total of 10 min) were applied to the tender points 27 of the neck and upper back seen in FMS patients; bilateral suboccipital muscle insertions, bilateral trapezius at the midpoint of the upper border, above the scapula spine near the medial border bilaterally, and paraspinous 3 cm lateral to the midline at the level of the midscapula bilaterally. 27
The number of treatment sessions was determined based on previous studies that focused on the effects of physical modalities on the treatment of FMS. 28,29 All physical modality sessions took place in the Baskent University Faculty of Medicine Physical Medicine and Rehabilitation Department on an outpatient basis. The treatment was provided by a single physiotherapist with at least 10 years of experience in treating FMS patients. The physiotherapist was blind to the pre- and post-treatment patient evaluation.
Acupuncture
Acupuncture sessions in pain–symptomatic illnesses, such as FMS, can be administered daily or as 10 sessions per cure, taking place ∼3 days per week. In many studies, the duration of one effective session has been documented as 20 min. 30 Moreover, an overall dose effect of treatment with acupuncture in FMS patients has been observed in previous studies in which three treatment sessions per week were given as opposed to a single session per week. 31 Indeed, in a systematic review of five randomized clinical trials on the effect of acupuncture in FMS, the number of treatment sessions varied from 6 to 36 over a 2- to 4-week period. 32
Therefore, in this study, those in the formulated Traditional Chinese Medicine acupuncture group received a total of 10 sessions, each lasting 20 min, once every 2 days over a 3-week period. Seventeen needle insertions took place per subject per session. Steel Kingli Sterile Acupuncture Needles (0.25 × 25 mm) were applied perpendicularly to the Houxi (SI 3), Wangu (SI 4), Tianzhu (UB 11), Fengmen (UB 12), Feishu (UB 13), Jueyinshu (UB 14), Jianjing (GB 21), Shenmai (UB 62), Jinggu (UB 64), Shugu (UB 65), and subcutaneously to the Yingtang point using the reinforcing method for a total of 20 min. On insertion of the acupuncture needle, de qi sensation was elicited in the patients.
In FMS patients, the majority of painful pressure points are found in the neck, back, lumbar region, and lower extremities; therefore, acupuncture points that are specifically effective in the treatment of these areas were chosen. It is known that SI 3 and UB 62 are the eight confluent points and are effective in the treatment of diseases of the neck, shoulder, thoracic, and lumbar regions.
The SI 4 point is used in disorders presenting with symptoms of pain in the Yuan-Primary point of the SI meridian and shoulder–neck region. The UB 64 point is used in disorders presenting with symptoms of pain in the Yuan-Primary point of UB meridian and the neck–lumbar region. The UB 65 point is used in disorders with symptoms of pain in the neck–lumbar region and lower extremities. 33
The majority of FMS patients have signs and symptoms of psychologic disturbance. 34,35 Therefore, the Ying Tang point was used as it treats psychologic alterations such as anxiety and depression. 36,37 Further details of the meridians and positioning of the needles can be found in Appendix Table A1.
Acupuncture was performed by a physiologist with over 20 years experience in acupuncture. The acupuncturist was blind to the pre- and post-treatment patient evaluation. All sessions took place in the Baskent University Faculty of Medicine Physiology Department on an outpatient basis.
Statistical analysis
When this study was commenced, there was no prior similar study on which to base a power analysis. Articles on adequate sample sizes for pilot studies suggest a sample size of between 10 and 30 patients. 38 Hertzog recommended 20 to 25 patients for intervention efficacy pilots, given reasonable effect sizes, but 30 to 40 patients per group for pilot studies comparing groups. 39 Therefore, in this pilot study, a sample size of 25 to 30 patients per group was aimed for.
Statistical analyses were performed using the SPSS software version 21. The Kolmogorov–Smirnov test was used to test the normal distribution of each of the variables. Descriptive analyses were presented using means and standard deviations for normally distributed variables, medians (minimum–maximum) for the non-normally distributed variables, and percentages for ordinal variables. Independent sample t-test was used for intergroup comparison of the normally distributed variables and Mann–Whitney U test was used for intergroup comparison of the non-normally distributed qualitative variables. A paired t-test was used for dependent normally distributed numerical variables, whereas the Wilcoxon test was used for double comparisons of dependent abnormally distributed numerical variables. The chi-square test was used to compare the ratios between the different groups.
The minimal clinically important differences (MCIDs) for SF-MPQ and FIQ were used when interpreting the date. MPQ3 MCID was a mean improvement score greater than 5. 21 The MCID for VAS score for current pain (MPQ4) was a reduction of ≥1.37 cm. 40 The MCID for the FIQ score was a reduction in score of 14%. 41 Effect size was calculated using Cohen's d where the values of d for small, medium, and large effects are 0.2, 0.5, and 0.8, respectively. 42
Results
The mean age of the study participants was 48.1 ± 8.77 (29–68). Baseline characteristics of both groups are given in Table 1. A flowchart of the recruitment and follow-up of participants are depicted in Figure 1. All patients allocated to the treatment groups completed the course of treatment. There was no correlation between symptom duration and SF-MPQ or FIQ in either group. Pre- and post-treatment SF-MPQ and FIQ scores for both groups, mean change in score within each group, and the effect size of treatment between the groups are shown in Table 2.
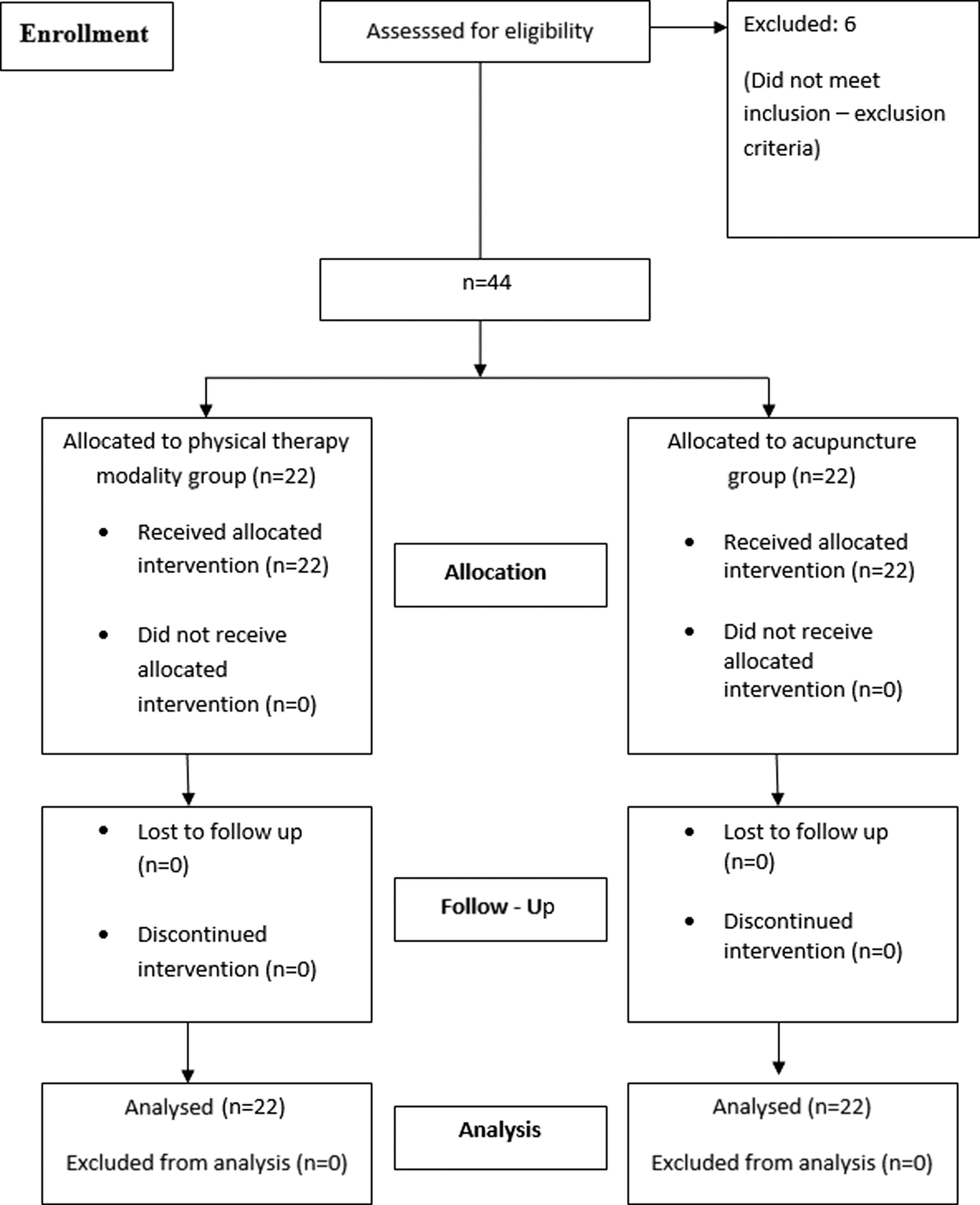
Design and flow of participants through the trial following the CONSORT 2010 guidelines.
Baseline Characteristics of the Patients
Unemployed or retired.
FIQ, Fibromyalgia Impact Questionnaire; MPQ 1, sensory descriptors total score; MPQ2, affective descriptors total score; MPQ3, total descriptors score; MPQ4, VAS score for current pain; MPQ5, PPI index score; PPI, present pain intensity; SF-MPQ, Short Form McGill Pain Questionnaire; VAS, visual analogue scale.
Comparison of Within and Between Group Short Form McGill Pain Questionnaire and Fibromyalgia Impact Questionnaire Scores Before and After Treatment, the Mean Change in Scores, and Effect Size
Cohen's d effect size: 0.2, small; 0.5, medium; 0.8, large.
FIQ, Fibromyalgia Impact Questionnaire; MCIDs, minimal clinically important differences; MPQ1, sensory descriptors total score (range 0–33); MPQ2, affective descriptors total score (range 0–12); MPQ3, total descriptors score (range 0–45, MCID >5); MPQ4, VAS score for current pain (range 0–10, MCID 1.37 cm); MPQ5, PPI index score (range 0–5); FIQ score range 0–80; MCID, 14%; PPI, present pain intensity; SF-MPQ, Short Form McGill Pain Questionnaire; VAS, visual analogue scale.
Based on the MCIDs, there was a clinically important reduction in VAS scores for current pain (mean change in score −4.11 in the PT group and −2.56 in the acupuncture group) and SF-MPQ3 total descriptors score (mean change in score −11.07 in the PT group and −11.16 in the acupuncture group) after treatment with both PT and acupuncture. In addition, there was a clinically important reduction in FIQ total scores after treatment in both the PT and acupuncture groups; the change in the mean FIQ total score was 30% in the PT group and 39% in the acupuncture goup.
There was no difference in pre- and post-treatment SF-MPQ and FIQ scores in any of the domains between the two groups. When comparing the post-treatment scores of the the two groups with one another, there was a small effect size in the MPQ2, 4, and 5 domains with a Cohen's d of 0.458, 0.398, and 0.286, respectively. None of the patients reported any side effects of treatment.
Discussion
Traditionally, in our clinical practice, the basis of FMS treatment includes the use of PT modalities for pain relief in addition to patient education, a supervised exercise program, and pharmacologic treatment. Even so, many patients consider or undergo acupuncture as an alternative treatment option to physical modalities, while continuing their home exercise and drug regimen. Therefore, this comparative effectiveness study aimed to compare the sole effects of treatment with PT modalities with those of acupuncture on pain and quality of life in FMS patients and in doing so determine the superior treatment option of the two.
The results of this study may suggest that, in the short term, neither treatment with physical modalities nor acupuncture is superior to one another when treating pain and improving quality of life in FMS patients. The small effect size of the study supports this finding. However, based on the MCIDs, there was a clinically important improvement in questionnaire scores within each group after treatment.
Even though the traditional treatment options offered to FMS patients include patient education, psychotherapy, PT and exercise, and pharmacologic intervention, 4,5 the first line nonpharmacologic treatment to go alongside exercise remains debatable.
A recent review of Canadian, German, and Israeli guidelines emphasized the importance of a patient-tailored approach according to the patient's key symptoms, with aerobic exercise, cognitive behavioral therapy, and multicomponent therapy as the first choice. 6 Moreover, the German and Israeli guidelines recommended acupuncture as a CAM. However, the latest European League Against Rheumatism guidelines evaluated acupuncture as “weak for” based on the evidence of available meta-analysis. 7
PT modalities aim to reduce symptoms, improve physical function, mood, and general well-being. 43 In addition, hot, cold, and electrotherapies are used to modify pain and improve exercise compliance in FMS patients. 44
In this study, hotpack, TENS, and ultrasound were selected as PT modalities as these are the modalities frequently preferred in the treatment of FMS. Thermotherapy is a useful adjunct in the treatment of painful conditions. Heat decreases pain and muscle spasm and increases tissue metabolism and connective tissue extensibility. 45
TENS is recommended in the treatment of localized pain in FMS patients. 46,47 TENS is thought to reduce localized musculoskeletal pain via supraspinal and spinal mechanisms 36 and to increase muscle microcirculation, thus increasing endogenous opioid activity. A study by Mutlu et al. showed that TENS, alongside exercise, significantly improved myalgia in the short term when compared with exercise alone in FMS patients. 48
Ultrasound increases cell permeability, reduces inflammatory response via mechanical and thermal effects, and results in a slowing of neural transmission and a reduction in pain. Local vasodilatation reduces muscle spasm, which is also of importance in treatment of FMS. 29,36,49 A study by Oltulu et al. comparing the effects of ultrasound with those of laser on pain, stiffness, and tender points in FMS patients found that both treatments were effective. Another study showed an improvement in pain, function, and sleep in FMS patients when combined with a connective tissue manipulation technique. 28
Even though studies to date show that there is no single best PT modality, these modalities seem to reduce symptom severity and so are recommended as part of the treatment program of FMS. 50 In this study, the impact of FMS on the patients' ability to perform activities of daily living, sensation of well-being, and ability to work improved with PT and acupuncture; in both groups, the mean VAS for pain score reduced more than the MCID of 1.3 as determined by Tashjian et al. 40
Equally, in both groups, the improvement in the total descriptors scores (MPQ3) was greater than the MCID. Pain, fatigue, stiffness, anxiety, and depression reduced as shown by the FIQ. Moreover, in both treatment groups, there was a clinical improvement in total FIQ scores; the change in the mean FIQ total score was greater than the MCID for total FIQ score as established by Bennett et al. 41
In 2014, a Cochrane analysis of English and Chinese databases reviewed 124 studies on the role of acupuncture in the treatment of FMS. Nine of these studies, a total of 395 patients, were analyzed in this systematic review and showed that the addition of acupuncture to standard treatments reduced pain by 30%. 51 In the same review, electroacupuncture was found to be superior to placebo in improving general well-being and reducing lethargy and stiffness; however, these positive effects were not found to continue at 6 months follow-up post-treatment. 49
The data on the long-term effects of acupuncture remain insufficient and contradictory. 52 A more recent randomized single blind multicenter study of 153 FMS patients comparing an individualized acupuncture protocol with sham acupuncture found that the reduction of pain was 14% more in acupuncture patients. They also found that the reduction in pain persisted for 1 year with minimal side effects. 53 Equally, a study by Targino et al. based on 58 women in which one group (n = 34) was treated with acupuncture, tricyclic antidepressants (TADs), and exercise, while the other group (n = 24) was treated with exercise and TADs alone, showed that those in the acupuncture group had a significant reduction in tender points and a significant improvement in quality of life after 20 sessions of treatment. These effects were sustained at the 3-month follow-up. 54
This study has some limitations. First, and most importantly, this was a pilot study with a small sample size. Even though this study does provide us with preliminary results regarding study feasibility and treatment effectivity, a type II error may have occurred. The improvement in VAS for pain, SF–MPQ, and total FIQ scores after treatment in both study groups suggests that the results are clinically significant. However, the statistical significance of these findings remains unclear. A future study with a larger sample size, determined using a power analysis based on the MCID for the SF-MPQ and FIQ, would consolidate these findings. The small effect size of the results also indicates that a larger study is required.
In addition to this, this study took place at a time (2006–2007) when the up-to-date ACR criteria for the diagnosis of FMS was not available. Even though the diagnosis of FMS was made by an experienced PMR specialist based on a thorough history, clinical examination (including tender point examination), and investigation findings, the widespread pain index and symptom severity score of the 2010 guidelines could be used as variables or primary outcome measures in future similar studies. 55
Other limitations include the type of therapeutic groups, timing of the post-treatment assessment, and absence of long-term follow-up. Firstly, as mentioned previously, even though physical therapists normally take a multimodal approach to the treatment of the FMS patients, in this study PT modalities or acupuncture was applied independently. A larger similar study could examine the effectiveness of PT modalities or acupuncture as part of a multimodal approach, or include a control group of patients receiving exercise alone. A control group of patients receiving no treatment could also be considered; however, there may be ethical issues and issues with patient compliance to be considered under such circumstances.
The difference in the number of sessions and duration of each session in each group may be seen as a potential limitation; those receiving PT modalities were treated for 1 h for a total of 15 sessions, and those receiving acupuncture were treated for 20 min for a total of 10 sessions. However, these characteristics of the treatment regimens were based upon previous studies and recommended treatment guidance aforementioned, 31,32 and also arose due to the very different nature of the treatments being compared in this study.
The absence of long-term follow-up means that the long-term effects of the two treatment options on pain, functionality, and affect remain unknown. Furthermore, the assessment of the patients so soon after the end of the treatment course may be misleading as the patients may have modified their behavior in response to their awareness of being observed (the Hawthorne effect). However, due to the nature of FMS and its multimodal treatment (including pharmacotherapy), and bearing in mind that the primary outcome was a reduction in pain, the post-treatment evaluation was conducted promptly as FMS patients often seek different treatment options simultaneously, or in quick succession. Therefore, an assessment of the patients was conducted before any other treatment option could be sought.
Conclusions
To the best of the authors' knowledge, this is the first study comparing the effects of conventional PT modalities with acupuncture on the treatment of pain, function, and quality of life in FMS patients. The findings of this pilot study suggest that PT modalities and acupuncture can be used with clinical effectivity in the multimodal treatment of FMS. Even though one treatment method was not found to be superior to the other, it is worth bearing in mind that this pilot study only provides preliminary results.
There is necessity for the clinical effects of PT and acupuncture on pain, daily function, and quality of life to be studied more closely using a sample size based on an adequate power analysis and monitoring of patients over a longer period of time post-therapy.
Future work could also include a comparison of patient-specific acupuncture treatment with PT modalities as well as a comparison between Western modalities and electroacupuncture.
Footnotes
Author Disclosure Statement
All of the authors declare that no competing financial interests exist. No financial support was received for this study. The procedures followed in this study were in accordance with the ethical standards of the Ethics Committee of Baskent University Faculty of Medicine, Turkey, and with the Helsinki Declaration of 1975, as revised in 1983.
Acupuncture Points Used in the Study, Their Meridians, and Needle Location
| Point | Meridian | Needling | Location |
|---|---|---|---|
| SI 3 | Small instestine | Perpendicular insertion 0.5–1.0 inch | When a loose fist is made, the point is on the ulnar aspect of the hand, proximal to the fifth metacarpophalangeal joint, at the end of the transverse crease of the metacarpophalangeal joint, at the junction of the red and white skin. |
| SI 4 | Small instestine | Perpendicular insertion 0.3–0.5 inch | On the ulnar aspect of the palm, in the depression between the proximal end of the fifth metacarpal bone and hamate bone, at the junction of the red and white skin. |
| UB 11 | Urinary bladder | Perpendicular insertion 0.3 inch | On the back, 1.5 cm lateral to the lower border of the spinous process of the first thoracic vertebra |
| UB 12 | Urinary bladder | Perpendicular insertion 0.3 inch | On the back, 1.5 cm lateral to the lower border of the spinous process of the second thoracic vertebra |
| UB 13 | Urinary bladder | Perpendicular insertion 0.3 inch | On the back, 1.5 cm lateral to the lower border of the spinous process of the third thoracic vertebra |
| UB 62 | Urinary bladder | Perpendicular insertion 0.3–0.5 inch | In the depression directly below the lateral malleolus |
| UB 64 | Urinary bladder | Perpendicular insertion 0.3–0.5 inch | On the lateral aspect of the foot, below the tuberosity of the fifth metatarsal bone, at the junction of the red and white skin. |
| UB 65 | Urinary bladder | Perpendicular insertion 0.3–0.5 inch | On the lateral aspect of the foot, posterior to the fifth metatarsophalangeal joint, at the junction of the red and white skin. |
| Ying Tang | Extraordinary point | Subcutaneous insertion 0.3–0.5 inch | Midway between the medial ends of the two eyebrows. |