
Abstract
Objectives:
To evaluate the prevalence of special diet adoption in juvenile idiopathic arthritis (JIA) and parental perceptions of efficacy.
Design:
An online survey was distributed over a year to nearly 20,000 individuals.
Results:
Responses from 261 parents of patients with JIA were received. One of three (n = 79) had tried special diets, including gluten-free (66%), anti-inflammatory (41%), and lactose-free (25%). Overall, >50% of 79 parents reported that patients had improved pain or joint swelling.
Conclusions:
Special diets have been trialed by a third of the patients, with over half reporting symptom improvement. A prospective, controlled trial is warranted to test the efficacy of a dietary approach to JIA.
Introduction
Juvenile idiopathic arthritis (JIA) is the most common rheumatic disease in children. 1,2 Clinical outcomes are variable among different JIA categories and treatment strategies often differ. The etiology of this chronic rheumatic condition remains unclear. Treatment of JIA has benefited greatly from the development of biological treatments, early diagnosis, and aggressive intervention. 3 However, there is still significant interest from families to explore dietary changes in hopes of obtaining better control of this disease with less use of medications. 4,5 In one study (n = 52), 35% of patients with JIA reported removing foods from their diets to control joint symptoms and had reported favorable responses. 5 Although there have been successful dietary interventions in other pediatric inflammatory diseases, such as the use of a specific carbohydrate diet in inflammatory bowel disease (IBD), 6,7 no controlled dietary studies have been performed in JIA.
Our study explored the prevalence of dietary interventions in a cross-sectional group of patients diagnosed with JIA and parental report of the responses of joint symptoms.
Materials and Methods
This research project was approved by the Seattle Children's Hospital Institution Review Board (No. 15963). Consent was waived, because no protected health information was collected. The survey included questions regarding demographics, disease course, use of conventional medications, and/or special diets and perceived outcomes of dietary interventions. Commonly used diet types are listed. The survey was constructed in REDCap, a secure, web-based data capture application. 8 The survey link was posted to the “Juvenile Idiopathic Arthritis” Facebook group (1800 members) in March 2016 and distributed by the Arthritis Foundation through email (16,000 recipients) on April 20, 2016. Reminders were sent periodically during the study period. Letters, including the survey link, were also sent to 1414 patients with JIA followed in Seattle Children's Hospital in March 2017. The targeted study population was parents of children with JIA diagnosed by rheumatologists. Patients with celiac disease or IBD were excluded. The survey was closed on May 4, 2017. Responses were summarized using descriptive statistics. Categorical variables were summarized using frequencies and proportions, while for time after diagnosis, we calculated median and interquartile range. We calculated 95% confidence intervals for symptom response proportions. Independence of categorical variables was evaluated using chi-square tests. Statistical analyses were performed using Stata version 14 (StataCorp, College Station, TX).
Results
A total of 338 responses were received (1.8% response rate) from all sources with 261 responses completed by parents of children with JIA. Other response was from adult patients and excluded. We also excluded 10 patients not diagnosed by a rheumatologist and 13 with IBD or celiac disease. Demographic and JIA patient characteristics are summarized in Table 1. The majority of patients residing in the United States (97%) were female (73%) and had a polyarticular disease (63%). Eighty-three percent of respondents endorsed the use of a disease-modifying antirheumatic drug (DMARD) and/or a biologic drug. A subset of respondents (n = 51) was queried about postdiagnostic duration of JIA as a question was added during the study period. Median time since diagnosis was 2 years (interquartile range 1–5 years).
Demographic and Clinical Characteristics of Children with Juvenile Idiopathic Arthritis (N = 238)
Eight respondents did not indicate whether or not a special diet has been tried.
DMARDs, disease-modifying antirheumatic drugs; JIA, juvenile idiopathic arthritis; NSAIDs, nonsteroidal anti-inflammatory drugs.
Types of special diet and pattern of use in JIA
A total of 79 respondents had tried one or more special diet for their child's arthritis. The diets used are listed in Table 2. The top three special diets included gluten-free (66%), anti-inflammatory (41%), and lactose-free (25%). With regard to when a special diet was tried by each child, a majority of parents reported initiating most diets within a year of diagnosis. Thirty-three (43%) tried a special diet within 6 months of diagnosis, followed by 16 (21%) within 7–12 months postdiagnosis. Forty-five (58%) parents reported trying more than one diet for their child. Elapsed time from the date of diagnosis to the date of initiation of each special diet is detailed in Supplementary Table S1. Over 50% of these respondents maintained these special diets for at least 7 months as detailed in Supplementary Table S2.
Diet Choices in 79 Patients Who Ever Tried a Special Diet
A gluten-free diet excludes the protein gluten found in grains such as wheat, barley, rye. An anti-inflammatory diet is composed of fruits and vegetables, whole grains, plant-based proteins, fatty fish, and fresh herbs and spices. A lactose-free diet excludes food products containing lactose, mainly dairy products. A paleo diet includes lean meats, fish, fruits, vegetables, nuts and seeds and avoids grains, dairy, legumes, potato, refined sugar, and salt. A vegetarian diet excludes meat, fish, poultry, and may allow eggs (Ovo-vegetarian) or dairy products (Lacto-vegetarian) or both (Lacto-ovo vegetarian). A vegan diet excludes meat, poultry, fish, eggs, and dairy products. A specific carbohydrate diet severely limits most carbohydrates (primarily grains, starches, dairy, and sugars) and allows only specific carbohydrates from fresh fruits, honey, and home-made yogurt fermented longer than 24 h.
We considered joint involvement as a marker of disease severity. Patients with four or fewer affected joints were more likely to try a special diet within 6 months of diagnosis compared with those with five or more affected joints (63% vs. 34%, p = 0.06). When looking at reported use by region, those in the Southwest reported the highest percentage of use of a special diet (68%), although the difference between regions did not reach statistical significance.
Parental perception of response to special diet
Among the three most common special diets, the percentage reporting no change in or worsening joint symptoms ranged from 35% for lactose-free to 48% for gluten-free diets and 50% for anti-inflammatory, whereas improved pain or joint swelling was reported by 50% of anti-inflammatory, 52% of gluten-free and 65% of lactose-free respondents (Fig. 1A). Response rates were further divided into joint involvement by diet (Fig. 1B). For each of the three most common diets (gluten-free, anti-inflammatory, lactose-free), the proportion of children experiencing improved symptoms was higher for those children with <5 joints involved (p < 0.05).
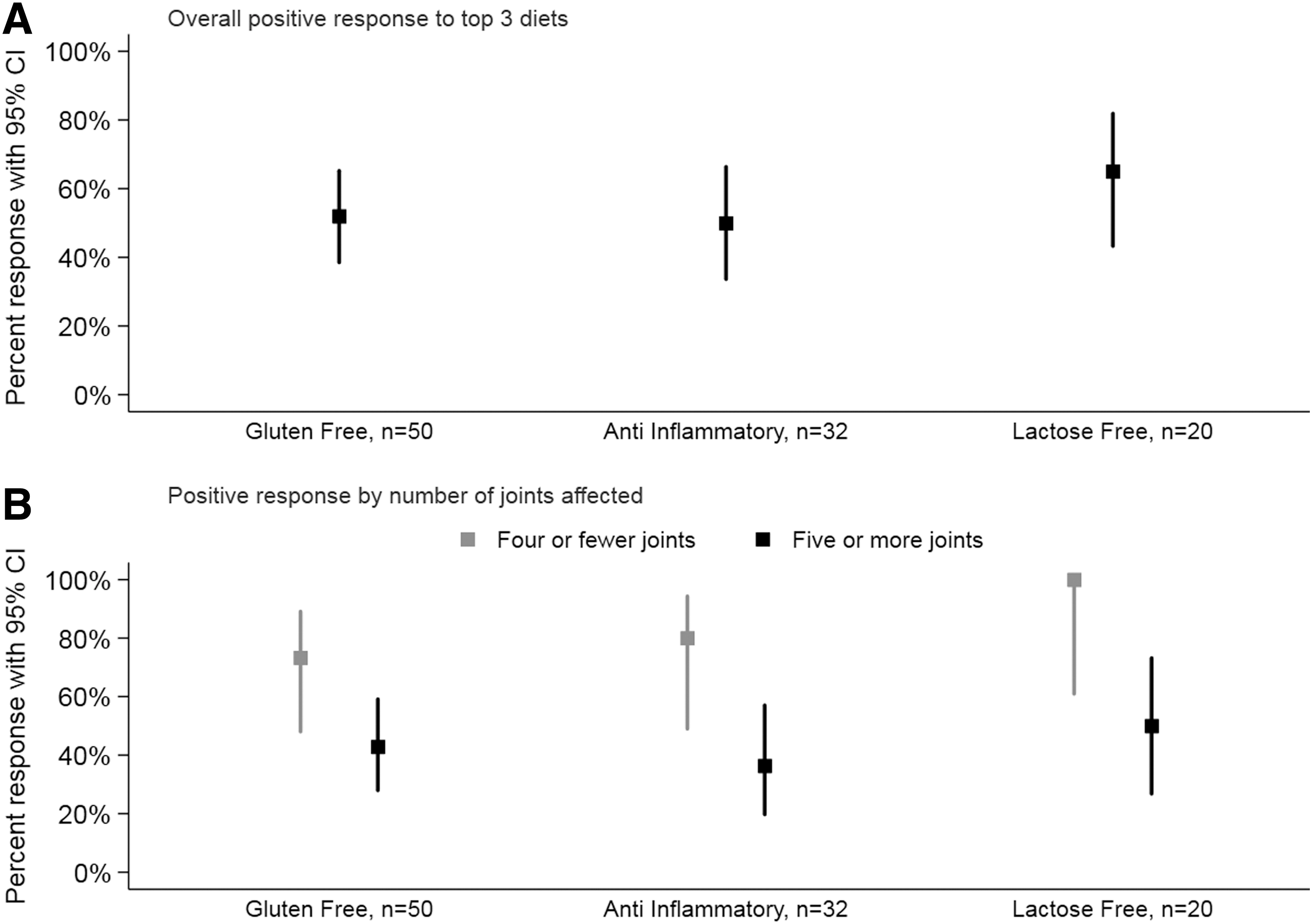
Percentage of children with juvenile idiopathic arthritis who had a favorable response to diet per parental report
As a proxy for disease activity, we specifically asked, “Did your medication change while on a special diet.” Most parents reported no change in medication during a dietary trial. When looking at medication changes while on a special diet, we found that within the patient group that adopted a gluten-free diet, there was a trend toward escalating antirheumatic medication (for example, from nonsteroidal anti-inflammatory drugs to a DMARD or a biologic). In those patients, 19% escalated medication, 8% reduced use of antirheumatic medication, 73% reported no change, and 6% were unable to recall. An opposite trend was seen with the lactose-free diet, where 20% of patients reported a reduced use of antirheumatic medication, 70% reported no change, 10% could not recall, with none reporting an escalation in antirheumatic therapy. The responses from those on the anti-inflammatory diet were missing.
Interest in participating in a special diet research study
In our study population, 26% of respondents stated they would be interested in participating in a dietary study, while 15% would not. Another 33% stated, “It depends” without giving extra details. Of the 15% who would not participate, “inconvenience” was the most common answer, followed by “concern for weight loss,” and “increased stress.” “Cost” and “not enough variety of foods” were the least chosen responses. Compared with those with 4 or fewer joints, those with 5+ joints were more likely to respond “Yes” (32% vs. 19%) and less likely to skip answering the question (16% vs. 36%).
Discussion
We have completed a survey study to capture parental perception of dietary effect on the joint health of their children with JIA. One third of our parents had already tried a special diet to help their child's disease, and 43% of them did so within the first 6 months of diagnosis, despite a paucity of data supporting dietary therapy. These results underscore the desire of families to seek helpful information on the role of diet in JIA management. There is a need for more research on diets and JIA that will allow rheumatologists to help patients and families make informed dietary decisions.
The most popularly adopted diets included a gluten-free diet, an anti-inflammatory diet, and a lactose free diet. Due to the limited number of responses, comparison among these diets did not appear to be statistically significant although there was a trend toward a greater reported reduction in antirheumatic medications in children on a lactose-free diet. The standardized dietary intervention and randomized control study will be necessary to minimize confounding factors and placebo effects. An objective measurement of joint outcomes needs to be used for a future controlled study to confirm these results.
For each of the most common diets, those with fewer joints involved were more likely to experience improvement in symptoms. Several factors may account for this result. First, those with fewer joints involved may respond better to a special diet. Second, when patients had fewer joints involved, they were more likely to report favorable outcome because of a greater tendency to improve or experience a placebo effect.
Based on the reported rates of parent initiation of special diets in our study, a prospective dietary study would be feasible in JIA. However, factors such as growth or picky eating could impact parents' willingness to make changes in their children's diets. Indeed, a review of dietary interventions in rheumatoid arthritis found weight loss to be a common side effect of dietary interventions meant to treat arthritis symptoms. 9 Therefore, close weight and growth monitoring and corresponding corrective measures should be considered in the design of such studies.
There is a paucity of research on how diet impacts the disease status of JIA. While our sample size is limited, our study demonstrates parental interest in diet in JIA. Our respondents had a high prevalence of DMARDs and biologic medication use during the disease course. For that reason, we conclude that the respondents are parents of children with higher disease burden, and thus they are more likely motivated to seek alternative treatment to their children's arthritis. But the parents of children with fewer joint counts were more likely to report improvement with dietary changes.
This study had several limitations making our results exploratory and requiring further validation. First, generalizability is limited because of geographic variations in the response to questions as well as the predominant responses from parents of children with polyarticular disease and a disproportionally overrepresented white population. Second, the response rate was low and families with greater interest in this topic may have been more likely to participate, which may have led to a selection bias. Third, the sample sizes of the entire group and subgroups were small, which reduced the power of statistical analysis. Fourth, questionnaires may lead to recall bias. Lastly, definition of a diet, such as “anti-inflammatory” or “gluten free” may also vary from patient to patient, and the adherence to special diets was not measured, nor was the duration on each diet.
Conclusions
One third of survey respondents from families of children with JIA attempted special diets, and 50% reported improvement in symptoms. Only 26% of survey respondents were willing to participate in a dietary intervention study.
Footnotes
Acknowledgments
The authors would like to thank all the patients and families who have taken the survey. Dr. Eric Allenspach has critically reviewed the article. Arthritis Foundation and Facebook JA groups have helped distribute the survey. REDCap database was supported through grant UL1TR000423 from NCRR/NIH. This work was supported by Center of Clinical and Translational Research and rheumatology research fund within Seattle Children's Hospital and Foundation.
Author Contributions
E.M.L., S.G., and Y.Z. designed study. E.M.L., M.C.B., and Y.Z. analyzed data. E.M.L. and Y.Z. drafted the article and all reviewed critically.
Author Disclosure Statement
Dr. Zhao received research funding from clinical research scholar program in Seattle Children's Hospital, CARRA and Bristol-Myer Squibb Inc. Dr. Stevens has research collaborations with Seattle Genetics, Inc. and Kineta, Inc., patent licensed to Quest Diagnostics. Jennifer Huber is an owner of In Bloom Wellness and is a Certified Nutrition Support Clinician.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.