
Abstract
Objectives:
Among different exercise models proposed for individuals with Parkinson's disease (IwPD), the popularity of traditional forms of dance is increasing. The aim of this study was to evaluate the effects of Sardinian folk dance (Ballu Sardu, BS) on functional performance and motor and nonmotor symptoms in IwPD.
Design:
Single-blind, randomized controlled pilot trial.
Settings:
Outpatient health clinic.
Subjects and interventions:
Twenty IwPD (13M, 7F; 67.4 ± 6.1 years) were randomly assigned to BS (n = 10) or usual care (n = 10). The dance program consisted of two sessions/week, 90-min/class, for 12 weeks.
Outcome measures:
Motor and nonmotor symptoms, as well as functional performance, were evaluated using different questionnaires and tests such as the Unified Parkinson's Disease Rating Scale Part-III (UPDRS-III), 6-min walking test (6MWT), Berg Balance Scale (BBS), Timed Up-and-Go (TUG) test, Five Times Sit-to-Stand Test (FTSST), Back Scratch Test (BST), Sit-and-Reach Test (SRT), instrumented gait analysis, Parkinson's Disease Fatigue Scale (PFS-16), Beck Depression Inventory, Starkstein Apathy Scale (SAS), and Montreal Cognitive Assessment (MOCA) scale.
Results:
Repeated-measures analysis of variance revealed significant Time × Group interactions for UPDRS-III and functional variables such as the 6MWT, BBS, FTSST, TUG (all, p < 0.001), BST (p = 0.04), and gait analysis parameters (stride length, p = 0.031; gait speed, p = 0.049; and gait fatigue index (GFI), p = 0.005). For nonmotor symptoms, significant Time × Group interactions for depression (p < 0.001), apathy (p = 0.016), and MOCA scores (p = 0.012) were observed. Of note, for GFI and SAS, the BS group only showed a trend toward improvement, while the condition of the controls worsened significantly. No between-group differences were observed for SRT and PFS-16.
Conclusions:
BS is an enjoyable activity, which has been proved to be superior to usual care alone in inducing changes in different motor and nonmotor symptoms associated with PD. Results show that BS can be considered a safe tool for contrasting impairments observed in IwPD due to the intrinsic nature of the neurodegenerative disease.
Introduction
Parkinson's disease (PD) is a progressive neurodegenerative condition comprising a spectrum of functional, motor, and nonmotor symptoms. 1,2 Treatment for PD has traditionally been based on the use of dopaminergic medications, even though nonpharmacologic approaches such as exercise-based activities are gaining attention for managing its complex symptomatology. 3,4 In this regard, there is evidence that conventional physical activities such as treadmill training, 5 –7 resistance exercise, 8 –10 and adapted physical activity (APA) programs can have positive effects in improving functional mobility, 11 static and dynamic balance, as well as nonmotor disturbances in individuals with PD (IwPD).
Recently, several nonconventional physical activities have been proposed for IwPD to improve functional mobility and enhance well-being, social inclusion, and quality of life (QoL). 12,13 Among these, t'ai chi, 14,15 boxing, 16 Nordic walking, 17 –19 aquatic-based exercise programs, 20,21 and dance-based approaches have been investigated preliminarily. 22 –26 In particular, the use of different forms of dance as a strategy for managing PD-induced disability is gaining popularity among IwPD, for whom social relations and participation in group activities have been reported to play a key role in the achievement of health goals. 27
Dance is an accessible and appealing form of fitness workout. The supportive, social nature of dance classes and the guidance of a dance teacher are important features that may help IwPD to overcome psychologic barriers, which often prevent them from participating in exercise programs. 28,29 In addition, dance provides a multisensory experience, and is therefore more than a set of isolated movements driven by music, because the activity not only involves physical domains but the emotional, cognitive, cultural, and socio-ethnochoreutics aspects as well. Indeed, traditional folk dance has been described as a form of dance that “may stimulate selective, deep limbic neuronal circuits and cause an emotional involvement, binding the subjective experience of individuals with the dynamic, objective reality of the community, also involving the motor side in the dance rhythm, in what could be construed as a symbolic and therapeutic function.” 30 Previous studies have demonstrated that social and community forms of cultural dance, such as Irish dance or Argentine tango, can improve functional mobility and socialization, which in turn increases adherence to exercise programs in IwPD. 25,26,31 –36
One of the most ancient Mediterranean dances is Sardinian folk dance, commonly referred to as Ballu Sardu (BS). This traditional form of dance is still very popular in Sardinia, embodying not only an enjoyable social moment but also the cultural expression of the community. 37,38 BS is typically danced in a closed or open circle by couples who are holding hands, palm to palm. The movements of the dancers change with the music's rhythms, generally characterized by a first component, which is slow and quiet, and a second more lively and rhythmic component, which includes steps and jumps. Due to its natural characteristics that address both motor and cognitive functions (i.e., coordination, balance, cardiovascular endurance, visual memory, mobility, and posture) and social aspects such as group activities, emotional response to the music, historic re-enactment, and physical contact, 38 BS dance may be a valuable and feasible therapeutic approach for managing several movement disorders, including PD.
Therefore, the purpose of this study was to evaluate the effects of participation in a BS dance program on functional and gait performance, motor symptoms, and on specific cognitive and affective nonmotor symptoms in IwPD with mild-to-moderate disability.
Methods
Study design and participants
The study is a single-blind, randomized controlled pilot trial. Consecutive subjects with a definite diagnosis of PD were recruited from patients attending the outpatient Movement Disorders Clinic of the University of Cagliari. Inclusion criteria for the study included a clinical diagnosis of PD according to Gelb's criteria, 39 a score ≤3 on the Hoehn and Yahr (H&Y) scale, 40 ability to walk without walking aids, stable medication regimen in the 4 weeks before the study, and a score ≥24 on the Mini-Mental State Examination. 41 Exclusion criteria for the study were as follows: H&Y stage >3, diagnosis of dementia according to Diagnostic and Statistical Manual of Mental Disorders 5 (DSM-5) criteria, atypical parkinsonism, pharmacologic treatment with drugs not approved for PD, the presence of any complementary disability or autonomic problems that precluded the training program, or any specific health condition for which exercise was contraindicated. A history of falls in the previous 3-month period, as well as the presence of dyskinesias, freezing, and static–dynamic postural instability, was also verified before enrollment.
Twenty patients meeting eligibility criteria (13M, 7F; mean age 67.4 ± 6.1 years) were randomly allocated into two groups using a random number program generator (Research Randomizer 4.0 software). The exercise group received usual care (medical therapy) plus a 12-week BS dance program, while individuals in the control group did not perform any type of specific exercise program, maintained their habitual activities, and continued their usual care involving medical therapy alone. All participants were informed on the aims of the study and its procedures before enrollment, and written informed consent was obtained from all subjects. The study was approved by the Institutional Review Board at the University of Cagliari (Registration No.: NP/3339) and was performed in accordance with the Declaration of Helsinki. Figure 1 displays the CONSORT flow diagram for the study.
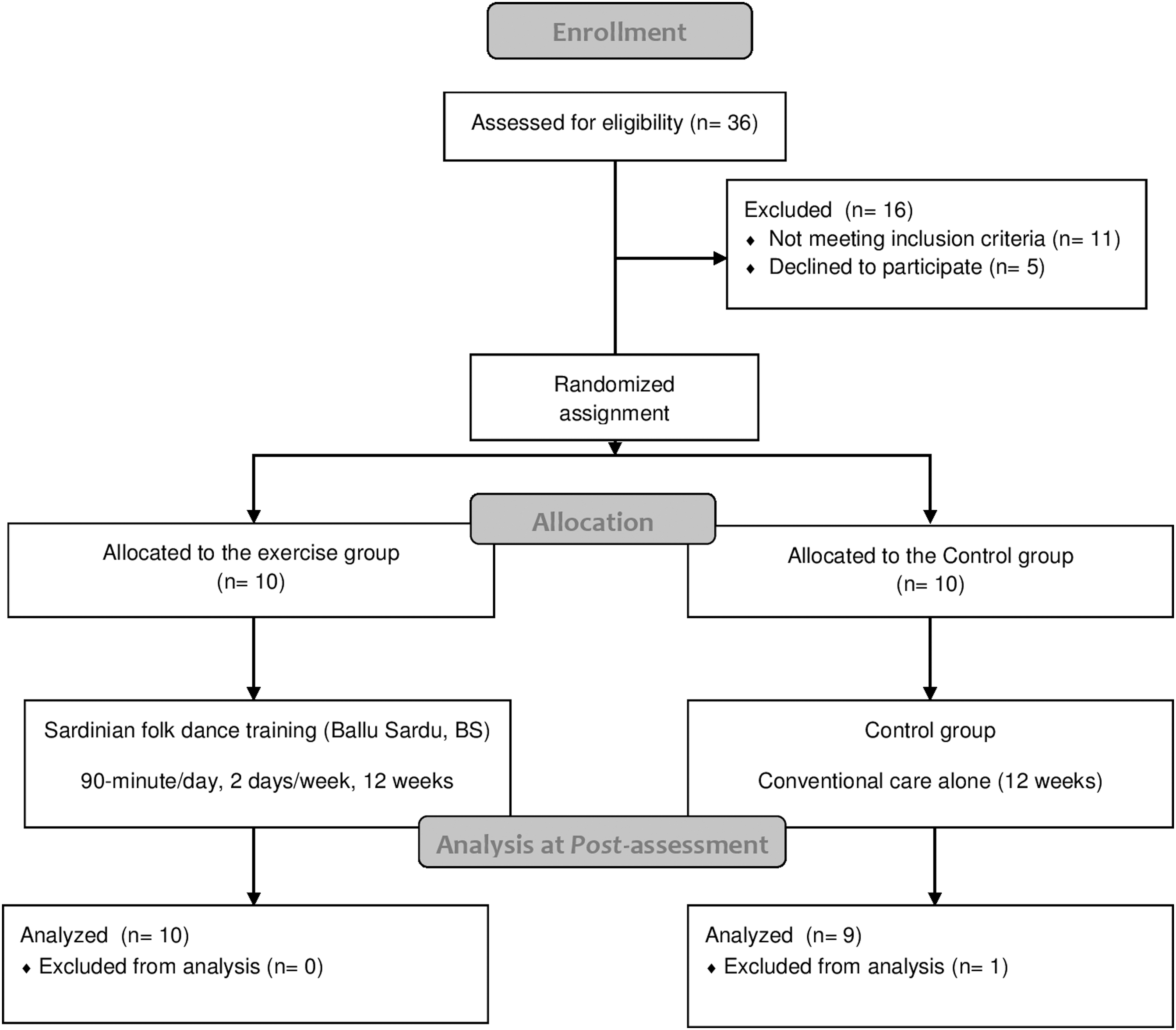
CONSORT flow chart for the study design.
Experimental procedures
Participants in both groups were instructed to continue with their usual care and advised not to change their daily activities during the trial. Assessments were performed by three experienced evaluators (a neurologist for PD motor and nonmotor symptoms, a physiotherapist for functional outcomes, and a bioengineer for gait analysis). Evaluators were blinded to group allocation and not involved in routine clinical follow-up. All outcomes in both groups were assessed at baseline (within 2 weeks before starting the dance program) and after the completion of the 12-week intervention (at week 13). Assessments were carried out when participants were in the “on” phase (i.e., when medications were working and symptoms were controlled). Participants' antiparkinsonian medications were monitored by using a self-report measure.
Motor symptoms and functional outcomes
All participants received a structured clinical evaluation, which included evaluation of their clinical history, the presence and severity of any motor complications related to use of dopaminergic treatment (both motor fluctuations and dyskinesias), and the presence of nonmotor disturbances.
Motor disability was assessed using the motor component of Unified Parkinson's Disease Rating Scale Part-III (UPDRS-III) 42 and the modified H&Y scale. 40 Functional performance was evaluated using a set of standardized tests, including the 6-minute walking test (6MWT) to evaluate cardiovascular fitness 43 and the Five Times Sit-to-Stand Test (FTSST) to estimate dynamic strength in the lower limbs. 44 Neuromotor performance was assessed using the Timed Up-and-Go (TUG) test for functional mobility 45 and using the Berg Balance Scale (BBS) to evaluate static balance. 46 Participant's lower-body joint mobility was assessed by the Sit-and-Reach Test (SRT), 47 and the Back Scratch Test (BST) was used to assess upper-body joint mobility. 48
Gait analysis
During the assessments, each subject was provided with a wearable gait analysis system composed of three magneto-inertial measurement units (MIMUs) (Opal, APDM, sample frequency = 128 Hz). Two MIMUs were attached to the participant's ankles (20 mm above the left and right malleolus) and one on the back approximately at the level of the fifth lumbar vertebrae (L5) (Fig. 2). Participants were instructed to perform a 2-minute walking test (2MWT) at a self-selected speed, walking back and forth in a loop composed of a 7-m straight path and two 180° turns.

Participant with Parkinson's disease wearing the MIMUs and MIMU positions above the ankles and at L5 level. MIMU, magneto-inertial measurement unit.
For each gait cycle, spatiotemporal parameters such as stride length (m), gait speed (m/s), cadence (steps/min), number of straight walks, and straight walking time (s) were estimated.
49,50
In addition, during the 2MWT, a gait fatigue index (GF1) (Eq. 1), based on any decrease in gait speed observed during the test, adapting the equations used previously in repeated-sprint studies,
51
was calculated as follows:
where MGSB is the gait speed over a straight path from the second to the last lap, and MGSAis the gait speed over straight paths of the second lap (negative values indicated the presence of fatigue: −50% indicated a one-third reduction in participant's initial speed, while a value of −100% indicated that participant's initial speed had reduced by half). Data obtained from the gait examination were exported to Statistical Software for the Social Sciences (SPSS), version 18 (SPSS, Inc., Chicago, IL) for further analyses.
Nonmotor symptoms
Parkinson's Disease Fatigue Scale (PFS-16) was used to evaluate fatigue. The PFS is a 16-item scale that asks subjects to assess physical aspects of fatigue and its influence on their daily functioning. Items on the PFS-16 are rated on a scale from 1 to 5. Total PFS-16 scores are the average of item scores across the 16 items, with higher scores representing more fatigue. 52 The Beck Depression Inventory (BDI-II) was used to estimate depressive symptoms. This questionnaire contains 21 items evaluating the presence and severity of depressive symptoms at the time of completion and during the previous 2 weeks, with higher total scores indicating more severe depressive symptoms. 53 Analysis of apathy symptoms was performed using the short version of the Starkstein Apathy Scale (SAS). The scale consists of 14 items, with lower total scores indicating less severe apathy levels. 54 The Montreal Cognitive Assessment (MOCA) 55 scale was used to evaluate cognitive deficits. The MOCA scale allows users to identify cognitive impairments in domains such as attention, concentration, executive functions, memory, visual-spatial skills, calculation, and orientation. Total scores on the MOCA range from 0 to 30, with scores >26 being considered in the normal range.
Sardinian folk dance intervention
The 10 participants assigned to the BS group underwent a Sardinian folk dance program based on an adapted form of BS. The training program consisted of 24, 90-min class sessions, performed twice per week for 12 weeks. Adherence to the training sessions, including attendance at classes, and any adverse effects were recorded. The exercise protocol was performed in close collaboration with the APA Master's Degree Course of the University of Cagliari and with a sports association that promotes exercise therapy (Team Kayak Sardegna).
Each 90-min BS session involved three phases. During the initial 30 min, warmup exercises, balance training, coordination, mobilization, ankle control exercises, proprioception, and breathing exercises were performed. During the following 50 min, a Sardinian folk dance teacher conducted the dance supported by traditional records (based on launeddas rhythms). The BS sessions comprised of different forms of Sardinian folk dance beginning with the monostructured forms and progressing to the bistructured ones. Monostructured forms combine rhythmic and homogeneous movements, which are more suitable to the needs of BS beginners with PD. The monostructured and bistructured BS forms are differentiated by the use of two alternating rhythms, slow and fast (in Sardinian language: seriu and alligru, respectively). During the BS sessions, subjects held hands or arms to form a circle that rotated clockwise. The dynamics of BS include steps and small jumps, with stop on the right foot. In BS dancing, movements of the legs are performed from predominantly the mid-thigh down. During the dance, the knees were kept slightly bent to ensure a uniform springing of the forefoot. The different types of monostructured dances (characterized by slow and gentle rhythms) and bistructured dances (characterized by a slow and a more lively rhythmic music component) employed in this study included the Ballu Seriu (The Slow Dance), the Passu Torrau (The Returned Step), and the Ballu Tundu (The Circle Dance). 37,38 The final 10 min of the 90-min session consisted of deep breathing and static stretching exercises. All 24 training sessions were entirely supervised by a physiotherapist assisted by two APA specialists. Other subjects (relatives, friends, and caregivers) were also allowed to participate in BS sessions not only to support their relatives but also to create an opportunity for them to enjoy the dance with subjects.
Statistical analysis
Data were analyzed using SPSS, version 18 (SPSS, Inc.). Descriptive statistics were calculated for all the variables considered. For sample size calculations of this study, previous studies were considered, which employed other forms of nonconventional exercise-based activities for IwPD who reported large effect sizes (ESs) for UPDRS-III scores ranging from 1.38 19 to 1.46. 20 In addition, during calculations, those studies were considered that specifically focused on the effects of dance-based therapies in this population in which moderate ESs were observed (0.65 in Hackney and Earhart, 56 and 0.68 in Duncan and Earhart 22 ). An a priori power analysis (G × Power 3.1 software, Germany) was then carried out assuming a moderate ES (Cohen's d = 0.7) and an alpha level of 0.05; based on these assumptions, the software indicated that 10 subjects per group would be needed to achieve at least 80% statistical power. Equality of variance was analyzed using Levene's test. Data sphericity was evaluated using Mauchly's test. In the case of nonspherical data, a Greenhouse–Geisser correction was applied. The Kolmogorov–Smirnov and the Shapiro–Wilk tests were used to test the normality of distributions. Main effects (Time, Group) and two-way interactions (Time × Group) were analyzed using repeated-measures analysis of variance (RM-ANOVA). In case of significant differences, Bonferroni-adjusted pairwise comparisons were used to identify differences. Statistical significance for all tests was set at p < 0.05. The clinical relevance of the intervention-induced changes was estimated by calculating ES using Cohen's d (small ES ≤0.5; moderate ES = 0.51–0.79; large ES ≥0.8), 57 according to the formula by Hedges and Olkin, which corrects for bias arising from the use of pooled standard deviations. 58,59
Results
At baseline, no significant differences were identified between the groups for any of the demographic and clinical characteristics reported in Table 1. In addition, the two groups showed no significant differences in any of the variables analyzed. No changes in medication administration or loading doses occurred during the 12 weeks of BS training, and no adverse effects were recorded during the protocol. Participant attendance at the dance classes during the program was 92.9%. Reasons for lack of attendance at dance classes included concomitant illness and individual conditions unrelated to PD. Data from one participant in the control group were discarded after initial review as severe dyskinesia and freezing significantly altered the registration of gait patterns during analyses.
Demographic and Clinical Features of Parkinson's Disease Patients
Note: Values represent mean ± standard deviation and percentage.
BMI, body mass index; BS, Ballu Sardu; H&Y, Hoehn & Yahr; LEDD, Levodopa Equivalent Daily Dose; PD, Parkinson's disease.
Motor symptoms and functional performance
Analysis of UPDRS-III scores revealed that tremor at rest, tremor during action, and postural instability are the most common issues reported by participants. RM-ANOVA showed a significant main effect of Time (F = 11.273; p = 0.004) on UPDRS-III scores, and a significant Time × Group interaction (F = 22.191; p < 0.001, ES 2.19). Post hoc testing with Bonferroni-corrected pairwise comparisons revealed that after the intervention, UPDRS-III scores decreased significantly in the BS group only. Post hoc testing also revealed a statistically significant 72.4% increase in the distance participants in the BS group were able to cover during the 6MWT, with a large between-group ES (F = 41.124; p < 0.001; ES 2.98).
Analysis of static balance scores from the BBS using RM-ANOVA revealed a significant main effect of Time (F = 32.184; p < 0.001) on BBS scores, and a significant Time × Group interaction (F = 49.834; p < 0.001). Pairwise comparisons revealed significant increases in BBS scores in the BS group only, with a large between-group ES (3.51). After the intervention, both groups displayed significant reductions in the amount of time needed to complete the TUG test (BS group: −26.4%; p < 0.001; control group: −6.5%; p = 0.022). Participants in the BS group performed significantly better on the TUG test, with a large between-group ES (F = 26.014; p < 0.001; ES 2.37).
In this analysis of dynamic strength scores for the lower limbs using the FTSST, pairwise comparisons revealed that the amount of time needed by the participants to complete the test reduced only in the BS group (−31.6%), while that needed by the control group increased significantly (+5.6%; p = 0.04), showing a large between-group ES (F = 95.685; p < 0.001; ES 4.54).
RM-ANOVA testing identified a significant main effect for Time (F = 9.130; p = 0.01) and a significant Time × Group interaction (F = 5.152; p = 0.04) for the BST. Improved upper-body flexibility was only observed in individuals in the BS group during the study (BS group: +37.2%; p = 0.005; control group: +5.4%; p = 0.56), resulting in a large ES (1.21). Analysis of SRT test data using RM-ANOVA identified no significant differences within groups and no significant Time × Group interactions (p = 0.42) (Table 2).
PRE to POST Changes in Motor Symptoms and Functional Performance Within- and Between Subjects
Italics indicate confidence interval settled at a 95% confidence level.
Note: Values represent mean ± standard deviation and percentage.
Significant for p < 0.05.
Significant for p < 0.01.
Significant for p < 0.001.
6MWT, 6-Minute Walking Test; BBS, Berg Balance Scale; BS, Ballu Sardu; BST, Back Scratch Test; CI, confidence interval; ES, effect size (calculated by the Hedges g; small <0.5; moderate 0.51–0.79; large >0.8) (58); FTSST, Five Times Sit-to-Stand Test; SRT, Sit-and-Reach Test; TUG, Timed Up-and-Go test; UPDRS-III, Unified Parkinson's Disease Rating Scale Part III.
Gait analysis
Analysis of stride length data from the study using RM-ANOVA found a significant Time × Group interaction (F = 5.608; p = 0.03); post hoc testing using pairwise comparisons identified significant improvements in stride length for participants in the BS group (+4.7%; p = 0.023), with a large between-group ES (1.13). By contrast, in the control group, stride length decreased slightly during the study (−1.5%), although these changes were not statistically significant (p = 0.364).
Analysis of walking speed using pairwise comparisons found that only participants in BS group displayed a statistically significant increase in this variable during the study (BS group: +8.1%; p = 0.002; control group: +0.8%; p = 0.652), with a large between-group ES (F = 4.524; p = 0.049; ES 1.02).
Analysis of walking cadence data from the study showed that walking cadence increased for both groups (BS group: +5.1%; p = 0.01; control group: +4.6%; p = 0.046), but no Time × Group interaction was observed, and the between-group ES was very small (0.16). However, pairwise comparisons revealed a statistically significant increase in the number of straight walks participants in the BS group were able to perform (+10.5%; p < 0.001), while participants in control group showed a nonsignificant, +3.9% increase. A large between-group ES was observed (F = 4.572; p = 0.048; ES 1.02).
Analysis of GFI revealed a significant Time × Group interaction (F = 10.797; p = 0.005). Pairwise comparisons revealed a significant worsening of gait fatigue for the control group, while participants in the BS group showed a trend toward improvement, although the trend failed to reach statistical significance (p = 0.085). A very large ES was calculated between the groups (F = 10.797; p = 0.005; ES 7.72) (Table 3).
PRE to POST Changes in Gait Analysis Parameters Within- and Between Subjects
Italics indicate confidence interval settled at a 95% confidence level.
Note: Values represent mean ± standard deviation and percentage.
Significant for p < 0.05.
Significant for p < 0.01.
Significant for p < 0.001.
BS, Ballu Sardu; CI, confidence interval; ES, effect size (calculated by the Hedges g; small <0.5; moderate 0.51–0.79; large >0.8) (58); GFI, gait fatigue index.
Nonmotor symptoms
After the intervention, no differences were found in perceived fatigue (PFS-16) between the two groups, while a main effect of Time (F = 44.788; p < 0.001) and a Time × Group interaction (F = 47.957; p < 0.001) were detected for the depressive symptoms, as assessed by the BDI-II. BDI-II score improved only in the BS group, displaying a large between-group ES (3.22). A significant Time × Group interaction with a large between-group ES (F = 7.106; p = 0.016; ES 1.24) was detected for apathy symptoms, which remained unchanged in the BS group (p = 0.276), while SAS scores worsened significantly in the control group (p = 0.018). For cognitive impairments (MOCA), a significant Time × Group interaction with a large between-group ES was observed (F = 7.913; p = 0.012; ES 1.31). Pairwise comparisons revealed a significant improvement in cognitive impairment scores for participants in the BS group only, while cognitive impairment scores for the control group showed a slight, nonsignificant worsening (p = 0.363) (Table 4).
PRE to POST Changes in Nonmotor Symptoms Within- and Between Subjects
Italics indicate confidence interval settled at a 95% confidence level.
Note: Values represent mean ± standard deviation and percentage.
Significant for p < 0.05.
Significant for p < 0.01.
Significant for p < 0.001.
BDI-II, Beck Depression Inventory; BS, Ballu Sardu; CI, confidence interval; ES, effect size (calculated by the Hedges g; small <0.5; moderate 0.51–0.79; large >0.8) (58); MOCA, Montreal Cognitive Assessment Scale; PFS-16, Parkinson's Disease Fatigue Scale; SAS, Starkstein Apathy Scale.
Discussion
Previous research has shown that the use of dance-based therapies is associated with improved motor function and balance capacity in IwPD, 26 particularly Argentine tango 34 –36 and Irish set dancing. 25,31 –33 These studies focused on motor performance, with only a limited number of investigations 60 –63 appraising the effects of dance-based activities on nonmotor symptoms such as affective or cognitive impairments.
Results of this study indicate BS as a safe and feasible form of physical exercise that is likely to have positive effects on functioning and nonmotor symptoms in IwPD. Indeed, in line with previous reports that have focused on other types of dance-based activities 25 overall attendance at BS classes in this study was excellent, and no safety issues or adverse effects were reported.
Nevertheless, given the design of this study, which compared participants undergoing dance-based therapy with a nonactive control group, the interpretation of these findings needs to take the neurodegenerative nature of PD into proper consideration. In fact, if left untreated, IwPD tend to display a worsening of motor- and nonmotor symptoms. 64 However, it is generally accepted that a minimum of 12–18 months of observation are required to detect the disease progression in PD trials. 64 In this light, it cannot be claimed with certainty that this was the case for the control group, where a significant decline was observed in 3 variables (FTSST, GFI, and SAS), and a significant improvement in 2 (TUG, cadence) out of 17 outcome measures evaluated. Changes in an outcome measure can be observed not only after an intervention but also as a reflection of the presence of “background noise,” which relates to the amount of error that surrounds a measurement (error zone). Overall, nonactive controls may not prove to be a stable reference for evaluating the long-term effectiveness of exercise-based interventions and may require a comprehensive appraisal of not only between-group but also within-group results to better quantify the net changes obtained at the end of the programs.
Analysis of UPDRS-III scores showed a significant improvement in PD motor symptoms after participation in the BS program. UPDRS-III scores decreased by 5.3 points for participants in the BS group, which is likely to be clinically relevant since it exceeds the threshold for a clinically important difference (CID) for IwPD, which has previously been defined as a change in UPDRS-III scores between 2.5 and 5.2 points. 65 These findings are comparable with those of previous studies on dance-based activities where the dance group exhibited a reduction in the UPDRS-III that exceeded the abovementioned CID. 66
After the intervention, significant improvements in cardiovascular fitness were observed in the BS group. The distance that participants in the BS groups could cover during the 6MWT increased by 239.5 m, greatly exceeding the cutoff for a minimal detectable change (MDC) for this outcome, which has been previously established as a change of at least 82 m. 67 Improved fitness and aerobic capacity are expected findings when reconditioning protocols such as treadmill training 68,69 or Nordic walking programs 70 are employed, but improvements in fitness and aerobic capacity were a novel finding after a dance protocol. Significant improvements in postural stability (+6.9 points on the BBS score), which surpassed the MDC for IwPD (+5.9 points), 67 were also observed in the BS group. This finding is in line with results from a previous study depicting a close relationship between increased walking distance and decreased risk of falls. 71
Spatiotemporal dimensions of gait such as gait speed, stride length, and cadence improved after participation in the BS intervention. In particular, walking speed (which is regarded by many experts as the best predictor of disability severity and functional decline in PD) 72 increased significantly during the dance intervention. Clinically, the degree to which walking speed changed during the intervention (+0.10 m/s) can be interpreted as a small-to-moderate change according to cut points outlined by Hass et al. 73 (small = +0.06 m/s; moderate = +0.14 m/s; large = +0.22 m/s). Analysis of gait in this study also included an assessment of GFI, which is widely recognized as an integral part of the spectrum of motor impairments associated with PD, reflecting both central and peripheral impairments, along with the functional deterioration induced by the disease. 74 Accordingly, while GFI worsened in the control group, GFI showed a trend toward improvement after the BS training. However, given that the differences in GFI were only statistically significant in the control group (who worsened), the role that dance-based activities may have had in countering the neuromuscular fatigue observed in IwPD warrants careful interpretation.
Results of the study found that dynamic strength in the lower limbs increased significantly after participation in the BS dance program, while the control group, which was not given the dance-based intervention, exhibited significant worsening, likely reflecting the neurodegenerative nature of PD, 64 which impacts muscle strength as well. 75 In addition, participants in the BS group showed significant improvements in mobility in the upper body (assessed by BST), displaying a significant Time × Group interaction, while no difference was detected in participant's lower-body flexibility (assessed by SRT). This finding likely suggests the need to integrate additional phases of stretching for the lower body into the BS dance intervention, which are targeted specifically by this form of dance. Walking ability and functional mobility also improved after BS, with potential practical implications in reducing falls, although results of the TUG test did not reach the MDC recognized for this outcome (−1.82 s against a MDC of −4.85 s). 76 Several studies have highlighted how physical activity and structured exercise programs can improve nonmotor symptoms, 77,78 as also previously observed after Nordic walking and APA programs. 17,18 In this line and in addition to previous research, this study revealed a significant reduction of depressive symptoms at large ESs, suggesting a possible clinical relevance. With regard to apathy score (which was assessed using the SAS), a trend toward improvement in participants who took part in the BS program was only observed, while apathy scores in the control group worsened significantly. This, in turn, resulted in significant between-group differences, which likely inflated the study findings and required cautious interpretation.
Finally, findings from this study are in line with previous evidence showing how practicing nonconventional forms of dance-based activity may lead to enhanced cognitive performance. 61,62 Indeed, in the study by De Natale et al. 62 it was found that a 10-week program of Argentine tango had a positive impact on cognitive domains and improved executive function (assessed by the Trail Making Test), while Hashimoto et al. 61 found that after 12 weeks of dance-based exercise, participants displayed significant improvements in task switching and mental flexibility (assessed by the Frontal Assessment Battery and the Mental Rotation Task response time), supporting the concept that nonconventional dance-based activities may influence higher cortical functions as well.
Taken together, all these factors may help explain the global effects that the physical workout of BS exerted on the cohort of IwPD.
Study limitations and future perspectives
Considering the exploratory nature of this pilot trial, the findings presented here should be interpreted carefully, especially in relation to the type of control group that was utilized here. Indeed, the controls did not perform any specific type of exercise program, and maintained their usual medical therapy and habitual activity during the entire intervention protocol.
In future studies, BS dance may be compared with already established exercise training programs and other dance-based activities such as the Argentine tango, for which a considerable body of knowledge is available regarding its effects on disability, independence, and QoL for IwPD. In addition, these results open up the door for new comparisons between different exercise-based programs and innovative social-engagement activities, which would be intriguing to pursue.
Conclusions
Results of this study showed that IwPD who participated in a dance-based BS program displayed significant improvements in a variety of domains, ranging from clinical and functional performance to gait and nonmotor symptoms. Incorporating socially engaging forms of exercise into the clinical management of PD may improve participation and compliance with exercise-based interventions among IwPD, benefiting their overall functioning and, subsequently, QoL. In addition, due to the intrinsic neurodegenerative nature of the disease, the BS intervention may be viewed as an enjoyable and safe tool for contrasting the motor and nonmotor impairments observed in the PD population.
Footnotes
Acknowledgments
The study was supported by Fondazione Banco di Sardegna (Funds 2015). The authors are indebted to Dr. Emanuele Garau for his professional support to the dance classes, and thank Dr. Daniela Picciau, Dr. Matteo Mancino, Dr. Michele Crabolu, and Dr. Serena Nieddu for their determinant contribution to the project.
Author Disclosure Statement
No competing financial interests exist.