
Abstract
Background:
Chinese medicine, when applied as a whole system of care, traditionally incorporates self-care techniques and patient understanding as key aspects of patient recovery and health maintenance.
Objectives:
This review aims to explore the literature to date on Traditional Chinese Medicine (TCM) self-care in settings outside of Asia, beyond the sole application of t'ai chi or qigong, to consider simple self-care techniques as health care interventions that may be generalized to a wider population.
Design:
AMED, CINAHL, EMBASE, PubMed, and MEDLINE databases were searched for articles from inception to July 2018. Studies were included, which were undertaken in settings outside of Asia and/or Asian communities, and were excluded if they solely examined t'ai chi or qigong.
Results:
Findings of the included studies (n = 37) were categorized into four key areas in relation to the TCM self-care component evaluated: self-acupressure, self-acupuncture, self-moxibustion, and the adoption of prescribed lifestyle, diet, and exercise advice based on a TCM diagnosis. The studies included randomized clinical trials, case studies, hospital audits, and qualitative evaluations. The studies assessed TCM self-care in relation to a wide range of health conditions, with the majority of studies concluding positive findings.
Conclusion:
This review draws attention to the potential role of TCM self-care techniques, in settings outside of Asia, beyond the sole practices of t'ai chi and qigong, as an adjunct to health maintenance and recovery. Only tentative conclusions can be drawn from the existing research, however, due to variability across studies in reporting transparency and the overall low number of studies retrieved. Further research is warranted.
Background
Traditional medicine practices from China and East Asia, including acupuncture, moxibustion, cupping, and the prescribing of herbal medicine, are increasingly being practiced outside these regions and are increasingly integrated into contemporary health care. 1 –8 These therapies are most commonly practiced in an integrated model referred to as Traditional Chinese Medicine (TCM), which has its foundation in a medical system designed as a whole system of care that prioritizes assessment of the patient in a holistic context. 9,10
Within this system, patient care has historically focused as much on health maintenance and prevention, through encouraging patients to adhere to simple health and lifestyle practices, as it has on the treatment of illness. 10 Thus, self-care practices, which may be considered activities undertaken by an individual to “prevent disease, evaluate symptoms, and restore health,” 11 are inherent to TCM.
Lifestyle or health-promoting practices from East Asia have become somewhat known in the West via specific manifestations such as t'ai chi and qigong, exercises that typically combine a set form of movements, breathing techniques, and guided imagery, 12 and are increasingly the topic of scientific investigation. 13 –16
A broader concept of lifestyle practices, however, is referred to in the foundational texts of medicine in China, dating back to the classical era c.300–200 BCE. 10 These texts provide guidance on easily adopted preventative health care measures, including minimizing alcohol intake; engaging in exercise routines that include both aerobic and resting practices; having an awareness of the impact of temperature and environmental conditions; and adopting appropriate dietary adjustments specific to the individual. 10 This perspective on health and lifestyle care has been shown to not only be culturally integrated but also to be retained by members of Asian migrant communities, 17 –19 who report including practices on “self-care, use of herbs, lifestyle, hot/cold balance” in daily life, 19 which align with these traditional perspectives.
TCM self-care thus incorporates health behavior practices that draw on these classical perspectives, and could also include self-moxibustion, self-acupressure, or even self-acupuncture, the latter of which is not common to TCM, but is being used in some contemporary Western health care settings.
Self-moxibustion is the self-applied burning of moxa (the dried herb Artemisia vulgaris), prepared in rice grain-sized threads or larger cigar-shaped poles, and either applied to the skin or held above the skin surface, respectively, to instigate a healing response. 20 Self-acupressure involves the patients using their thumb, fingers, or in some cases, a massage tool, to apply therapeutic pressure to selected acupuncture points on their own body. Techniques of acupressure are incorporated into both tuina (TCM massage therapy) and shiatsu (Japanese acupressure therapy). Self-acupuncture involves the patients inserting acupuncture needles to specified therapeutic acupuncture points on their own body.
Noncommunicable chronic and lifestyle illnesses are becoming an increasing part of disease burden globally. In response, the World Health Organization (WHO) has recommended implementation of a number of high-impact measures that are notably similar to TCM lifestyle practices, recommending improvement to individual levels of physical activity; reducing salt/sodium intake, alcohol intake, and tobacco use; as well as providing increased access to medical care and early intervention strategies. The implementation of such measures is perceived to far outweigh the calculated economic and social cost of not applying such interventions. 21 The WHO has also developed a Traditional Medicine Strategy, recommending the integration of traditional medical systems where evidence suggests there may be evidence of health benefit.
For this reason, examination of the practices of TCM self-care may offer insights—including those beyond currently recommended initiatives—into implementing health behavior change in communities globally. However, to date there has been little formal examination of how traditional systems of medicine have been used to promote self-care in integrative settings. This review aims to remedy this information gap, by assessing and analyzing the primary research into TCM self-care techniques, in communities outside of Asia and/or Asian migrant communities, relative to outcomes of health and well-being.
Methodology
Data sources and searches
Electronic searches were conducted in AMED, CINAHL, EMBASE, PubMed, and MEDLINE for articles from inception to July 2018, using terms related to TCM and self-care. Representative search terms are shown in Table 1. Searches were conducted with no date or language restrictions.
Search Terms Applied in PubMed Database Search
Selection criteria
This review included original research reporting on the therapeutic application of TCM in self-care, inclusive of singular therapeutic interventions that have been drawn from TCM. As TCM practices may be culturally embedded in some Asian communities, studies were excluded if the interventions were delivered in a setting within Asia or Asian communities, to consider self-care techniques as health care interventions that may be generalized to a wider population and to gauge their success in naive populations.
Studies were also excluded if they only reported t'ai chi or qigong interventions as both of these practices have been, comparatively, extensively explored in the literature. 13 –16 Furthermore, t'ai chi and qigong practices often involve a set form, involving a combination of specific physical movements, guided imagery, and breathing exercises, 12 which can be more complex, in learning and application, than other TCM lifestyle recommendations.
Results
Study selection
All identified citations (n = 2109) were downloaded into EndNote referencing and management software program. Of the 2109 downloaded citations, 390 were discarded as duplicates and a further 1237 discarded by title (A.H.). The remaining 482 citations were filtered by abstract with a further 331 identified as not fulfilling the inclusion criteria and being discarded. A random sample of articles were screened by title and abstract by the other authors (A.S. and J.W.).
The 151 retained citations were then screened by full text and a further 22 articles discarded due to not directly incorporating a TCM self-care component or merely comprising a report or discussion of the topic area. A further 90 articles examined a t'ai chi or qigong self-care component only and were therefore discarded, leaving 39 articles, of which 12 were discarded based on being set in an Asian country or Asian community. An additional nine articles were located via manually searching through the reference list of included articles. A random sample of articles were screened by a second author (A.S.). Details of this process are summarized in Figure 1.
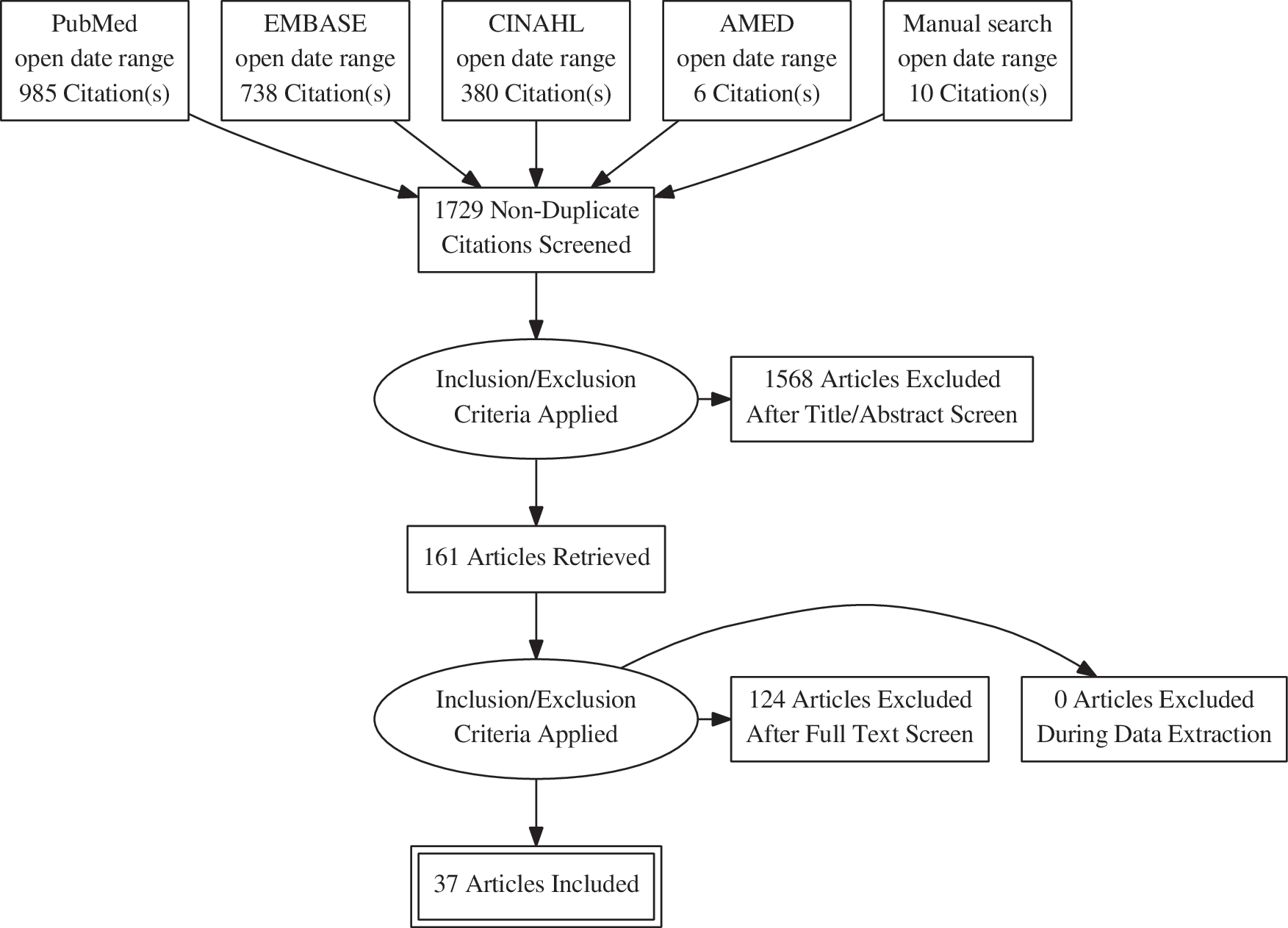
PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Data extraction, risk of bias assessment, and synthesis
Data were extracted from selected articles into a summary table, formatted into domains of study design, nature of the TCM self-care intervention, control, outcome measures, practitioner standard of training, duration of intervention, sample population, condition examined, blinding, summary of findings, and data quality. The summary table was prepared by two reviewers (A.H. and A.S.). Data extraction was completed by one reviewer (A.H.) and periodically checked by a second reviewer (A.S.) with discrepancies resolved through discussion until reaching consensus.
Articles were categorized according to study design for risk of bias and quality assessment, however, also categorized according to the nature of TCM self-care intervention for further analysis and discussion. For the purposes of this review, studies on self-applied tuina, shiatsu, and acupressure were categorized together. Risk of bias and quality of evidence were appraised with the Consolidated Standards of Reporting Trials (CONSORT) 2010 Checklist 22 for the randomized controlled trials (RCTs); Case Report Statement and Checklist (CARE) 23 for the case series and case studies; Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) checklist 24 for the clinical audits, hospital survey, and longitudinal descriptive study; and Consolidated Criteria for Reporting Qualitative Research (COREQ) guidelines 25 for the qualitative studies.
Study characteristics
A total of 37 articles were identified for inclusion in the review. Articles were dated between 2003 and 2018, with the majority of studies (n = 22) being conducted in the past 5 years. Twenty-six of the articles retrieved were randomized clinical trials, 26 –51 of which 11 were undertaken in the United States, 26,32 –34,37 –40,49 –51 3 in Iran, 27,29,47 and 5 in the United Kingdom, 35,41 –43,46 with single RCTs being drawn from Australia, 44 Denmark, 30 Italy, 28 Portugal, 45 Uganda, 36 and Germany 31 and 1 study being conducted in both Australia and China. 48
Studies reviewed that were not RCTs include two case studies 52,53 and a case series 54 undertaken in the United Kingdom, United States, and Canada, respectively; three clinical audits 55 –57 and one hospital survey 58 undertaken in the United Kingdom; and a longitudinal descriptive study undertaken in Germany. 59 The article data are summarized in Table 2.
Traditional Chinese Medicine Self-Care Studies' Summary Table
Standardized/Individualized—Standardized treatment applied according to basic biomedically defined condition/Individualized—Individualization of treatment according to a TCM or similar differential diagnosis.
Data quality: CONSORT: RCTs; CARE: case reports; COREQ: qualitative studies; STROBE: clinical audit, hospital survey, longitudinal descriptive study.
95% CI, 95% confidence interval; AD, atopic dermatitis; BDI, Beck Depression Inventory; BFI, Bowel Function Index; BMAS, British Medical Acupuncture Society; CAM, Complementary and Alternative Medicine; CARE, Case Report Statement and Checklist; CINV, Chemotherapy induced nausea and vomiting; CONSORT, Consolidated Standards of Reporting Trials; COREQ, Consolidated Criteria for Reporting Qualitative Research; CRPS, complex regional pain syndrome; EAP, ear acupressure; EASI, Eczema Area and Severity Index; GP, General Practitioner; HIS, Stimulating/High Dose; IGA, Investigators Global Assessment; IHD, ischemic heart disease; IMEA, Integrative Meditation and Ear Acupressure; INVR, Index of Nausea, Vomiting and Retching; LBP, low back pain; LIS, Stimulating/Low Dose; LTQL, Long-Term Quality of Life Instrument; MDI, major depression inventory; MPQ, McGill Pain Questionnaire; MYCaW, measure yourself concerns and well-being; NPQ, Northwick Pain Questionnaire; NRS, Numeric Rating Scale; NVS, Numeric Verbal Scale; OA, osteoarthritis; PAC-QOL, Patient Assessment of Constipation-Quality of Life Questionnaire; PAR, perennial allergic rhinitis; PPS, pressure pain sensitivity; PRMD, playing-related musculoskeletal disorders; PSOT, practitioner standard of training; PSQI, Pittsburgh Sleep Quality Index; QOL, quality of life; RA, relaxation acupressure; RCT, randomized controlled trial; SD, standard deviation; SDS, Sheehan Disability Scale; SF-12v2, Short Form Health Survey version 2; SF-36, 36-item Short-Form Health Survey; SOD, Sphincter of Oddi dysfunction; SSS, Stanford Sleepiness Scale; STROBE, Strengthening the Reporting of Observational Studies in Epidemiology; TB, tuberculosis; TCM, Traditional Chinese Medicine; TED, treatment-effect difference; VAS, Visual Analog Scale; WHO-5, 5-item World Health Organization Well-Being Index; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Risk of bias assessment
Assessed against CONSORT, 22 the majority of the self-care RCTs adhered closely to the guidelines, with transparent reporting of study methodology (Supplementary Table S1). There was a notable lack of blinding in 12 of the RCTs, however, this was largely reflective of the design of these trials as either pragmatic studies assessing a routine clinical practice 41 –43,46 or as studies directly assessing self-care techniques. 26,28,29,31,32,35,38,47
Other items that scored weakly against the CONSORT include 7 trials failing to detail how sample size was determined, 32 –34,37,38,41,45 a number of studies failing to detail the method used to generate 33,37,41 and type 28,33,37,38,45,47,49 of randomized allocation sequence applied, and 11 of the RCTs failing to define dates of recruitment and follow-up. 27,29,30,32 –34,37 –39,43,45 There was a notable lack of reporting on harms, with nine of the RCTs failing to mention whether there had been any adverse events. 27 –30,32,33,37,41,45 Seven of these were acupressure studies, one comprised both acupressure and acupuncture, 28 and one was a secondary analysis. 41 Clinical trial registration also rated poorly, with 13 RCTs being unregistered, bringing into question positive reporting bias. 28,32 –35,37 –39,41,45,47,49,50
The case studies 52,53 and case series 54 rated well against CARE 23 (Supplementary Table S2), however, all failed to clearly identify study methodology in their report title, as well as failed to comment on adverse events. The clinical audits and hospital survey varied in reporting integrity, when assessed against STROBE 24 (Supplementary Table S3), which was chosen as being the most relevant reporting guidelines published for such studies, however, it may be that STROBE is not adequately reflective of the nuances of clinical audits. The longitudinal descriptive study rated well against STROBE.
There were also three qualitative studies; the first investigating the experience of practitioners and patients 60 in one of the included self-acupuncture RCTs, 43 and the other two studies exploring TCM self-care advice as a component of traditional acupuncture care, from both the practitioner 64 and patient 65 perspective, within a pragmatic RCT. These studies failed to comply with certain items in the COREQ guidelines, 25 with key information missing in all studies, in relation to the research team and any potential pre-existing relationships (Supplementary Table S4).
Categorization of findings
Four key areas emerged in relation to the TCM self-care components evaluated within the included studies: self-acupressure; self-acupuncture; self-moxibustion; and adoption of prescribed lifestyle, diet, and exercise advice based on a TCM diagnosis. One study incorporated both self-care advice and self-acupressure, thus falling into two of the categories. 28
Self-acupressure
The self-care component of TCM most commonly investigated was self-applied acupressure (n = 23), assessed in relation to a biomedically diagnosed condition; 26 –35,37 –40,44,45,47 –51,54,59 this included one study on self-shiatsu (a Japanese variation of TCM acupressure techniques) 54 and one examining self-applied tuina (TCM therapeutic massage). 45 All but two of the acupressure studies 54,59 were RCTs.
Conditions investigated in the acupressure studies varied widely (Table 3). Five studies examined women's health issues, 28,29,31,44,47 four studies assessed acupressure in relation to mental state and/or quality of life (QOL), 30,34,50,51 three studies examined quality of sleep for sample groups with chronic pain, 54 a diagnosis of cancer, 35 and for women going through menopause, 27 with other studies assessing gastrointestinal complaints, 26,33,37,59 skin conditions, 38 allergic rhinitis, 48 and addiction withdrawal. 32 Only four of the 20 acupressure studies evaluated musculoskeletal conditions, 39,40,45,49 with 2 of these being feasibility studies primarily examining recruitment and retention rates. 39,49
Conditions Investigated in Self-Acupressure Studies
MSK, musculoskeletal; QOL, quality of life.
Of the self-acupressure RCTs, three were double blinded 33,39,40 and seven single blinded. 27,30,34,45,48,50,51 Sample size ranged from 735 to 288 participants 51 with average sample size being 110 participants and over half the studies comprising 100 participants or more. 26 –31,33,39,40,47,48,51 Duration of intervention ranged from 3 days 34 to ∼3 months, 30,32,49,50 with the average intervention time being 6 weeks.
Four of the self-acupressure RCTs prescribed an intervention based on an individualized diagnosis. 28,30,35,45 Individualized tuina protocols, based on a differential TCM diagnosis ascertained by an experienced practitioner, were prescribed in a study examining playing related musculoskeletal disorders in musicians, in Portugal. 45 Dietary recommendations were also made based on an individualized TCM diagnosis in an Italian study. 28
In evaluation of self-acupressure on stress, depression, and QOL in ischemic heart disease patients, one study incorporated daily self-assessment via testing pressure pain sensitivity (PPS) at certain acupuncture points. 30 After gauging PPS, a standardized self-acupressure treatment was then only applied if indicated, and in an ear-acupressure study conducted in the United Kingdom, auricular points were added to standardized points, from a small subsample, according to weekly symptoms. 35 Remaining studies prescribed standardized acupressure point protocols according only to the predefined biomedical symptom or condition.
All excepting one 28 of the acupressure RCTs, which examined a specific condition (n = 17), concluded positive findings 26,27,29 -35,38,40,45,47,48,50,51 or a trend toward improved health outcomes. 54 In some cases, however, conclusions were tentative due to study limitations that included small sample sizes 32,34,35,38,45 and a lack of blinding (n = 10). 26 –29,31,32,35,37,47,49 Although some studies compared two active acupressure protocols, 34,40,45,47,50,51 over a third (n = 8) compared the primary intervention with usual care only 30 –33,35,38,44,49 or with baseline data. 54
Five studies included a sham acupressure intervention as a secondary 27,39,40,45 or primary control arm, 48 incorporating the use of acupressure points away from the recommended study protocol. The study that reported no benefit in self-acupressure compared individualized TCM diet and self-acupressure for those on a wait list, for the same protocol with the addition of acupuncture. 28
Self-acupuncture
The majority of studies examining self-acupuncture protocols were U.K. based, with four studies evaluating outcomes of existing self-acupuncture protocols, being prescribed by General Practitioners (GPs), 55 nurse pain specialists, 57 or other hospital staff, 56,58 in a GP practice and general hospital settings, respectively, via post-treatment audits. One study documented a single-case study of GP-prescribed self-administered acupuncture, with the addition of electrostimulation for a severe pain presentation, 53 and a qualitative evaluation, 60 nested within a multisite RCT, 43 examined the practitioner and patient experience of teaching and adopting self-acupuncture as an intervention protocol. A U.S. study documented a single case of daily self-administered laser stimulation on acupuncture points with the addition of disposable press needles. 52
All of the self-acupuncture studies assessing pain outcomes 53,55 –57 reported positive findings, with the qualitative study concluding self-acupuncture to be an acceptable and manageable intervention for patients. 60
Self-moxibustion
One RCT undertaken in Uganda examined the health outcomes of newly diagnosed tuberculosis (TB) patients, who self-administered rice grain-sized moxibustion daily, for 6 months, to the moxibustion point ST36, in combination with standard TB drug therapy. 36 Patients were trained in moxa application at their first visit by a designated TB nurse. 36 Improved outcomes in becoming sputum negative were seen in the moxa group in the first month, and a significantly larger improvement in hemoglobin levels was noted in the moxa group at 6 months. 36
Adoption of prescribed lifestyle, diet, and exercise advice based on a TCM diagnosis
Three studies, with results published in six articles, examined interventions that incorporated a TCM whole-system approach to care. 41,64,65
All based in the United Kingdom, the first examined, in addition to pain and disability outcomes, self-care efficacy and TCM lifestyle advice acted upon by patients, 41 following 12 sessions of treatment within a pragmatic 3-arm RCT for chronic neck pain, via practitioner reporting. 42 The second examined, qualitatively, the perspectives of participants, 65 in relation to self-efficacy and the TCM treatment provided, within the same RCT, 42 and the third study examined, from the practitioner perspective, descriptions of TCM self-care advice provided, as well as the TCM rationale, adopted strategies to improve uptake and expected impact upon patient health, 64 within an RCT investigating traditional TCM-delivered acupuncture for back pain. 46
In both of these trials, self-care advice was individualized, integrated with TCM diagnostics, and delivered as an inherent part of each treatment session, with practitioners reporting that advice was most commonly related to exercise, relaxation, diet, rest, and work. 41 One of the self-acupressure studies, conducted in Italy, also incorporated aspects of a whole-system approach, with the two arms of the intervention comparing self-acupressure combined with differentiated TCM dietary modifications, with the same intervention alongside standardized acupuncture. 28
Discussion
This review provides an overview of the known published research examining TCM self-care practices in cultural contexts outside of Asia, other than qigong and t'ai chi. A number of important findings are highlighted in this review, which warrant further consideration.
The limited number of TCM self-care studies in context of the broader TCM field
First, a relatively low number of studies on TCM self-care practices have been published. This is surprising given the high rates of TCM use globally, 67,68 reflected not only in the number of consumers but also in the national registration of TCM as a health profession in numerous countries outside China, including national registration in Australia, 69 state registration of acupuncture in over 46 states in the United States, 70,71 and provincial regulation of TCM and/or acupuncture in 5 Canadian provinces, as well as significant recognition in other countries. Furthermore, there appears to be relatively little attention to holistic approaches to treatment in these studies. All but four of the studies 28,41,64,65 based their self-care intervention on acupuncture points or channels, rather than implementing and/or assessing a broader interpretation of TCM self-care.
It may be that the promising body of evidence emerging from the research into acupuncture 72 has placed “acupuncture” (and its meridian architecture), in application as well as in language, in a highlighted position in relation to the perception of what it is that comprises holistic TCM health care. This focus has potentially placed in the background an interest in utilizing and assessing the value of broader self-care aspects of TCM and foundational Chinese medicine philosophy and practice, despite their traditional place being considered highly important for patient recovery, prevention of illness, and long-term health. 10
Further to t'ai chi and qigong, which falls outside the scope of this review, these broader aspects can include maintaining daily rhythms in line with 24-h and seasonal cycles, supporting metabolism and immunity through dress and hygiene practices, and adjusting diet according to individualized differentiation and seasonal change. 73,74 A focus on single therapies and treatments, outside of a TCM context, may not be congruent to the stated focus of TCM on holistic and patient-focused care. Its increasing use in research contexts may be related to the fact that single therapies are easier to integrate into other existing programs and into the design context of a randomized controlled trial, even if they may not be representative of TCM care in clinical practice. 75
Evaluation of TCM self-care practices within a whole system of care approach
Individualization of treatment in TCM is also overlooked by most studies, even though it remains a core element of TCM practice. Of 37 articles retrieved, only 3 evaluated an individualized intervention delivered within TCM as a whole system of care, 41,64,65 and only a further 3 applied an intervention based upon an individualized TCM diagnosis. 28,30,45 In countries where professional registration is in place for TCM, registration standards require practitioners to undertake years of training, not only in acupuncture as a symptomatic treatment approach but also in TCM as a complete system of diagnosis and care, based in the constructs and paradigm of the medicine. 69 –71,76
Moreover, this ignores contemporary developments in practice of TCM such as individualized TCM diagnosis being codified for inclusion in the newest update of the International Classification of Diseases 77 and the fact that this individualized approach has been repeatedly identified as one of the primary reasons that patients are attracted to complementary medicine approaches such as TCM. 78 This comprehensive and individualized approach is, however, only sparsely reflected in research methodology in studies examining TCM.
Future research could more accurately assess the impact of TCM interventions as they occur in “real-world” practice settings, if designed in line with flexible individualized diagnoses, adapted according to the patient's real-time presentation, as is the recommended practice for those who are professionally accredited in the field. With this in mind, researchers may benefit from employing the pragmatic clinical trial methodology 79 to interrogate TCM interventions.
Positive findings and the relationship between health, self-efficacy, and self-care
Despite these limitations, there appears to be a promising emergent body of evidence for TCM self-care approaches. Of the TCM self-care studies that assessed health-related outcomes, the majority concluded positive findings (n = 24). 26,27,29 –32,34 –36,38,40,41,45,47,48,50 –55,57,59,80 However, there may be some issues with generalizability; only three studies 41,45,65 prescribed an intervention based upon an individualized differential TCM diagnosis suggesting that, in similarity to acupuncture studies, 72 effect size may be misrepresentative due to the limitations inherent in applying standardized intervention protocols.
Such limitations include the simplification of more complex diagnoses 41 to align with the current practice and language of biomedicine, as well as the simplification of the TCM intervention itself, to allow replication and ease of assessment within the context of clinical trials. Nevertheless, the promising results of studies in this review suggest that further investigation of TCM self-care approaches in broader health care settings is warranted.
Incorporation of individual TCM therapies within a whole-system context appears to improve results of those treatments. In an analysis of patients receiving acupuncture treatment in the context of a whole system of care approach, patients were found to have increased their self-efficacy, and for there to be an association between increased self-efficacy and significant reductions in pain and disability in relation to the condition assessed at 6 months postintervention. 42
In secondary analyses of the same study, self-care advice provided by practitioners was most commonly related to exercise, relaxation, diet, rest, and work, 41 with patients identifying a positive practitioner relationship, as well as a developing sense of embodiment and self-empowerment, as factors that contributed to sustaining long-term benefits. 65 In addition to self-efficacy, a German study, outside of the citations included in this review, assessing an integrative medicine inpatient program (n = 2486), concluded that patients' stage of change and their health locus of control (HLOC), that is, their beliefs in relation to control of health outcomes, were all predictors for health behavior change. 81
This relationship between beliefs, understanding of one's health, and improvement in self-efficacy is of interest relative to TCM self-care, which aims to engage the patients in an element of understanding as to why a certain practice may be affecting their health positively or adversely. This aspect of sharing knowledge and imparting understanding, within the TCM consult, may therefore encourage the patients to increase their internal HLOC to affect behavior change.
In a pragmatic U.K. study of self-care communication in TCM acupuncture consults, self-care advice was seen by practitioners as being integral to the patient's treatment and was found to be delivered in the context of a therapeutic relationship based on continuity, mutuality, and trust, 82 thus providing ongoing support in the potential encouragement of self-efficacy. These findings of improved self-efficacy are similar to the results of a New Zealand study that examined the impact of self-care advice on patients receiving acupuncture for primary dysmenorrhea. 83 Study participants reported that they felt the self-care advice received during appointment visits had been related to both an increase in self-efficacy and positive outcomes in relation to symptom control.
These findings suggest that health promotion activity is intrinsically built into contemporary TCM practice—just as it was in historical TCM practice—even when TCM care is not specifically targeting self-care. These positive results suggest that this aspect of TCM care should be encouraged and supported through education and regulation initiatives, which can sometimes favor competency in individual treatments over holistic medical paradigms. 84
Also of interest is the finding in the acupressure self-care study, included in this review, which examined the effect of acupressure on cervical ripening at the initiation of labor, in which Bishop scores were found to be significantly higher in the group where the acupressure was self-administered compared with when it was nurse-delivered. 47 Such a finding suggests that an increased internal HLOC may have improved patient outcomes in the self-acupressure group beyond the effects of the intervention itself and thus provides a case for further investigation into the comparison of practitioner-applied or patient-applied interventions. Future research involving TCM self-care (and self-care more generally) should thus consider HLOC as a mediating factor upon study outcome and could consider including comparative interventions with HLOC as a control.
TCM self-care studies and the issue of safety
The majority of studies in the review assessed a standardized treatment protocol in relation to a predefined biomedical condition. 34 –40,43,44,47 –53,56 –59,85 Such an approach allows for the design of a rigorous study methodology that can be more readily replicated and assessed in an RCT, however, brings with it the limitation of lacking the prescription of individualized diagnoses and treatments, which are the traditional and existent design of delivery for those practicing TCM, including in countries with legislated TCM registration in place. 69 –71
It must therefore be carefully considered whether such trials designed with symptomatic prescriptions, be they in acupuncture, herbal medicine, or self-care techniques, are truly assessing a holistic TCM approach, or rather, simply assessing a singular TCM technique within a compromised context that may not accurately reflect real-world practice.
Further to this issue is the concern of patient safety beyond the baseline observations of soreness, bleeding, bruising, or skin irritation at an acupressure or acupuncture site. With varying research-based evidence to indicate that acupuncture affects numerous internal systems, including the hormonal, circulatory, respiratory, and musculoskeletal systems, 72,86 –91 the ethical stance of applying standardized treatment, without assessing the patient's entire presentation, must be considered. In the context of this review, TCM treatment—whether practitioner-applied or self-applied—which is not carefully aligned with a comprehensive TCM diagnosis, may place the subject at risk of adverse treatment effects, when viewed from the perspective of TCM. Although some studies indicate that individualized TCM treatment protocols are not superior to standardized interventions in relation to the primary condition examined, 92,93 it must be noted that treatment outcome measures in these studies rarely extend to include other concomitant changes in baseline health status. Furthermore, slow and gradual changes would not warrant being noted as adverse events, and positive changes in another aspect of the patient's health are not, in most RCTs, recorded unless predetermined by the research team.
Individualized diagnoses versus simple TCM self-care approaches
The majority of studies reviewed applied a version of TCM self-care, similar to that of a prescribed standardized intervention, such as in the case of acupressure being applied to three set acupuncture points for patients with dysmenorrhea. 31 Broader lifestyle approaches, which draw on a TCM perspective, however, aim to impart understanding, along with a lifestyle change, which has the potential to improve self-awareness and self-efficacy. 42
For example, a TCM practitioner may recommend eating warm foods before and during a woman's menses, in line with the concept of encouraging improved blood flow and circulation, thus potentially leading to less menstrual pain; 83 advice that can be tailored further based upon the patient's presentation. Thus, it is the case that both individualized advice and prescriptions can be recommended from a TCM perspective, as would occur in a real-world clinical setting, and that general TCM concepts can be employed as self-care.
Review limitations and future areas of research
The findings of this review need to be considered within the context of certain limitations. First, the retrieved articles for this review have been selected with a specific focus on self-reported TCM care practices engaged with by the patient, outside of qigong and t'ai chi, as well as outside of Asia and Asian communities, employing search terms based upon categories used in the literature.
However, despite attempts to be as exhaustive as possible within the scope of the research question, the authors acknowledge that this focus may have inadvertently resulted in some articles being missed, such as those that did not specifically identify as TCM or East Asian Medicine, as well as articles with broader scope, which may have incorporated a whole systems approach and individualized treatment. Thus, the focus has landed primarily on physical activities undertaken by the patient, potentially resulting in the clustering of articles on self-acupressure and self-acupuncture.
Second, the relative simplicity and degree of cultural integration of many TCM and foundational Chinese medicine self-care practices, even in settings outside of Asia, suggest that analyzing these components in individual parts may provide a limited perspective on the topic. Future research could consider an approach that compares individual self-care components with existing cultural practices in context and the potential role such practices play in the overall health of an individual or community.
Conclusion
The positive findings indicated by results of studies into TCM self-care, in settings outside of Asia, beyond the sole practices of t'ai chi and qigong, suggest a potential benefit from such practices and that this field warrants further investigation. The limited amount of research retrieved does not allow for definitive conclusions on the effectiveness of TCM self-care interventions. However, the trend toward positive results in the trials uncovered suggests the potential benefit of TCM self-care practices, which, if assessed with greater validity in a real-world context, could potentially provide benefit to health outcomes in community and population health programs, or be incorporated into health promotion initiatives.
TCM self-care practices may also increase long-term health outcomes by increasing the patient's level of self-awareness, and internal HLOC, thus leading to long-term health-related behavior change.
Footnotes
Acknowledgment
This research is supported by an Australian Government Research Training Program (RTP) scholarship.
Author Disclosure Statement
No competing financial interests exist with respect to the research, authorship, and/or publication of this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
Supplementary Table S4