
Abstract
Objectives:
Chronic health conditions are a major challenge to the health care system. Medical Group Visits (MGVs) are a valuable health care delivery model used in a variety of medical settings and patient populations. We conducted a systematic scoping review of MGV research literature for chronic health conditions to summarize the characteristics and individual components of MGVs in the United States of America and Canada.
Design:
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses scoping review methodology and searched five databases using nine widely used MGV-related terms.
Subjects:
We included studies conducted in the United States and Canada, whose participants were >18 years old and attended an MGV conducted in a medical setting by a billable health care provider. We excluded groups related to diabetes, pregnancy, and cancer.
Results:
Of 3777 studies identified, we found 55 eligible studies of which 9 are randomized controlled trials and 46 are observational studies. The majority of studies were conducted in academic medical centers, were observational in design, and recruited patients using physician referrals. The three most frequently studied groups include a combination of several chronic conditions (n = 12), chronic pain conditions (n = 10), and cardiovascular disease (n = 9). Curriculum components included didactics (n = 55), experiential activities (n = 27), and socializing components (n = 12). Didactic areas include (1) medical topics such as symptoms management (n = 27) of which 14 included pain management, and (2) lifestyle/educational component (n = 33) that comprised of talks on nutrition (n = 29), exercise (n = 20), stress (n = 16), and sleep (n = 10). The top integrative medicine (IM) modalities (n = 13) included: mindfulness techniques (n = 8), meditation (n = 6), and yoga (n = 5). Substantial heterogeneity was observed in the recruitment, implementation, curriculum components, and outcomes reported.
Conclusion:
The MGV is a model of patient-centered care that has captured the attention of researchers. IM modalities are well represented in the curriculum components of MGVs. Further investigation into the components identified by this study, may help in better targeting of group interventions to patients and contexts, where it is most likely to be effective.
Introduction
The prevention and management of chronic health conditions are an ongoing challenge to the North American health care system. In 2014, the Center for Disease Control and Prevention reported that 60% of all American adults have one or more chronic disease 1 and accounts for an estimated expenditure of $5,300 per person annually. 2,3 Experts suggest the need for primary care system changes to the organization of outpatient practice as a means of preventing and tackling chronic disease. 4 One such example of change is an emerging outpatient care model called a Medical Group Visit (MGV).
There is no standardized MGV model or a universal definition of MGV. 5,6 As per existing literature. 7 MGV is conducted by a medical provider with billing privileges, who sees multiple patients sharing similar medical conditions or needs together in a group. MGVs deliver health care to groups of patients at the same time while maintaining essential elements of one-on-one care. It differs from other group therapies by the integration of a medical portion, such as vitals measurement, medication reconciliation, and patient education, among others. 6 –10 This model has also been reported as an effective adjunct to conventional one-on-one clinical visits for diabetes. 10 –12 However, a closer examination of the nondiabetes literature is necessary to report the successes and weaknesses of the MGVs and common themes emerging in the literature. By understanding the current components (i.e., types of providers and length of duration), and characteristics (i.e., location and types of conditions) of the MGV literature, providers will be able to better implement MGV in clinical settings.
References to MGVs or shared medical appointments can be found in the literature as early as the 1970s and are routinely conducted in large Health Care Organizations (HCOs), such as Cleveland Clinic and the Kaiser Permanente health care system. 13,14 Key features, reported in the literature on MGVs, include improved access to care, reduces stress and loneliness, increased adaptation to illness, and patient empowerment, consequently leading to improved health outcomes. 7,9,12,15 Additionally, MGV may offer increased access to experiential learning, nonpharmacological therapies, and Integrative Medicine (IM) modalities used to prevent or treat chronic disease. 16,17 Unlike individual office visits, improved health outcomes may be possible because of the various additional characteristics and components such as increased length of time, experiential modalities, social interaction embedded within a MGV. 18 These contributing components that create the foundation of MGVs have not been independently explored, rather, researchers present their findings on the MGV as a single entity when studying outcomes and efficacy.
There are several systematic reviews on the utilization and effectiveness of MGVs in pregnancy (Centering Healthcare Institute), cancer, and diabetes care that have shown MGVs to be noninferior to routine prenatal care, offer improved quality of life (QoL), and improve biophysical outcomes, respectively. 11,19,20 Therefore, these conditions will not be the focus of this review. Two previous systematic reviews on MGVs for chronic diseases only included randomized controlled trials (RCTs), which primarily focused on the effectiveness of MGVs and analyzed studies conducted worldwide. 5,7
In conducting this review that captures conditions within the realm of prevention and treatment of chronic health conditions, we intend to better identify and synthesize the common components utilized in MGVs that may not have been captured in other reviews. In this scoping review, we aim to answer two questions: (1) What are the emerging characteristics and components of MGV interventions in the literature on the prevention and treatment of chronic conditions? (2) What are the similarities and differences among the various components between the MGV interventions and how are these reported in the literature? Summarizing the unique characteristics and MGV intervention components allows us to identify gaps in the literature and inform future researchers on the essential structure of an MGV. This scoping review is not designed to answer clinical questions about the effectiveness of MGV interventions.
Methods
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines for conducting and reporting items for systematic reviews. 21 These methods also satisfy the recently published extension for scoping review (PRISMA-ScR). 22 We have included all items of the PRISMA-ScR checklist in our method and analysis.
Information source and search strategy
A comprehensive search strategy was developed with the aid of an academic librarian at Boston University School of Medicine. The search was conducted using electronic databases: MEDLINE® (through PubMed), PsycINFO, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Embase®, and Web of Science. The detailed search strategy is described in the Appendix Table A1.
Eligibility and selection
Two reviewers (M.P., I.R.) independently screened titles and abstracts to determine relevance using an a priori checklist, 7 whose reliability was tested on a subset of research articles. If the abstracts did not provide enough information, the full text of the article was reviewed. Any disagreements regarding the inclusion of articles were resolved through discussion and consensus with the senior coauthor (P.G.).
Inclusion criteria
We selected studies for review if they met the following population (i and ii) and intervention (iii) inclusion criteria. Presence of a control group or select outcome measures were not applicable to our inclusion process: (i) participants of studies that were included in this review must be adults >18 years of age as the pediatric age group was beyond the scope of this review; (ii) study included participants who either had a diagnosed chronic health condition (condition lasting 3 months or more, by the definition of the United States National Center for health statistics) or were at risk of developing it; (iii) study included a MGV intervention as defined by (1) group intervention conducted by a provider who can prescribe or bill for patients and (2) conducted within a medical setting; other inclusion criteria included (iv) study conducted in the United States or Canada; (v) study conducted between January 1990 and December 2017 to restrict outdated articles, as the focus was to report the latest trends in the literature; and (vi) study designs consisted of RCTs, observational, descriptive, and qualitative studies.
Exclusion criteria
Studies were excluded if they involved an intervention exclusively aimed at diabetes, pre- or postpartum care, cancer, infective diseases, or provided group psychotherapy in a nonprimary care setting. Peer-led groups and non-English language articles were also excluded along with studies that were presented as dissertations, capstone projects, or conference proceedings (both oral and poster presentations).
Data extraction
The included studies were extracted by two reviewers (M.P., I.R.). Reviewers independently reviewed three articles to test a data extraction sheet adapted from a pivotal Cochrane review. 7 Based on a consensus process involving all authors, we subsequently revised the sheet and created a data dictionary in REDCap®, where extracted information was stored. The final data extraction included the following five categories: (1) general characteristics (title of publication, first author, year of publication, journal name); (2) study characteristics (study design, study condition, recruitment strategy, inclusion and exclusion criteria); (3) patient population (sample size, insurance coverage of participants, and billing); (4) setting (academic health centers, community health centers [CHCs], HCOs); (5) characteristics (number of sessions, timing, duration, invitation of family members, medical personnel, curriculum); (6) outcomes measured (primary and secondary outcomes reported in studies).
Statistical analysis
Statistical analysis included exploratory data analysis and descriptive statistics (frequencies, mean, and percentages) conducted using Microsoft Excel 2016.
Results
Study selection and characteristics
The search identified 3777 citations (Fig. 1). Of the 73 full-text articles screened, 5523–77 studies met the inclusion criteria and comprised 46 (84%) cohort studies and 9 (16%) RCTs. Study details are provided in Appendix Table A2. Figure 1 illustrates the publication source and ineligibility reasons. The sample sizes in the reported studies varied from the smallest (6 participants) to the largest (1842 participants). Thirty-eight (69%) studies used quantitative methodology, eight (15%) adopted mixed methodology, five (9%) were qualitative studies, and four (7%) were descriptive studies.
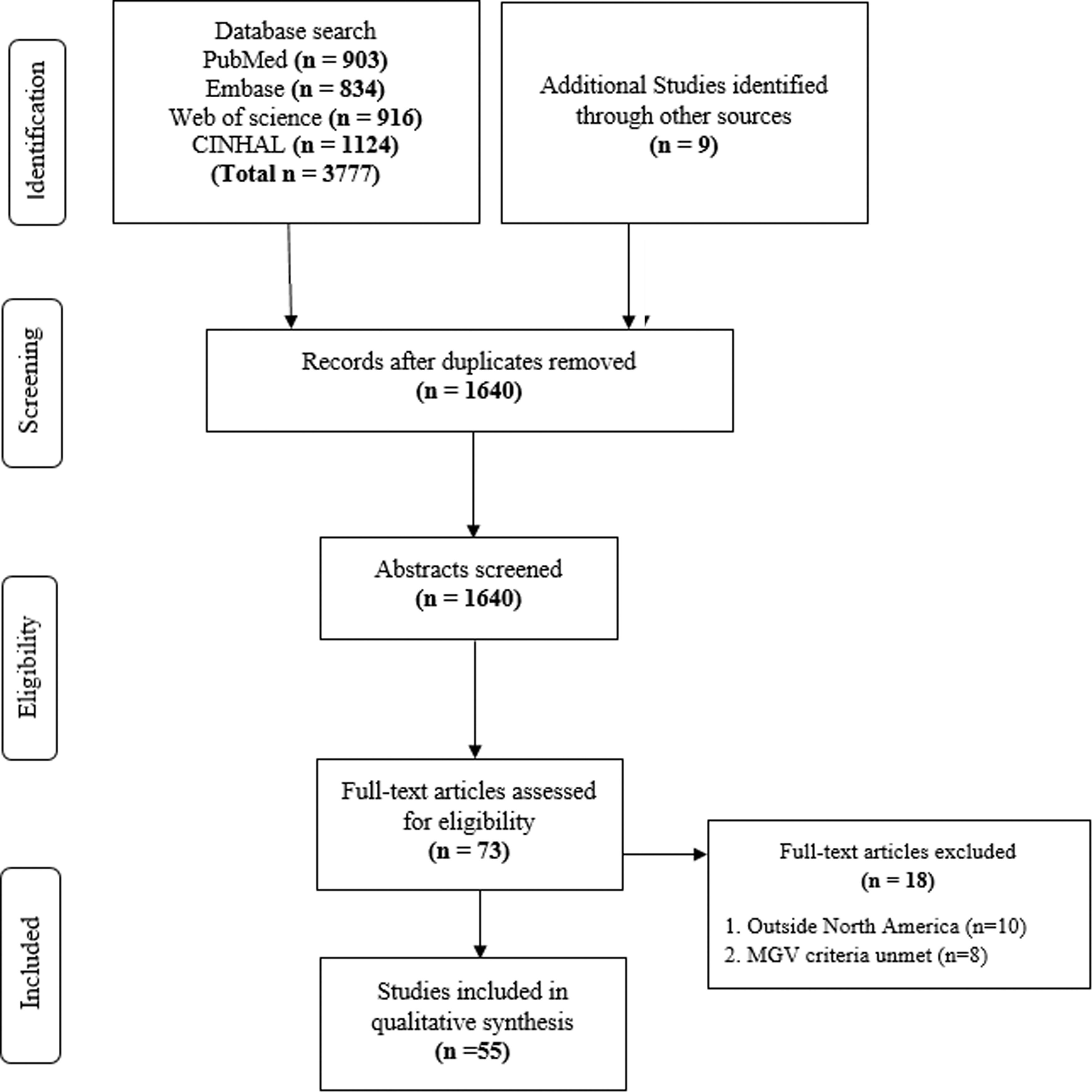
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram. CINHAL, Cumulative Index to Nursing and Allied Health Literature; MGV, Medical Group Visit.
Since 1990, there has been a steady increase in the study of nondiabetic/nonpregnancy/noncancer MGVs with a rapid increase seen after 2014. Over half (n = 32, 58%) of the selected studies were published after 2014. Forty-nine (89%) studies are published in scientific medical journals and six (11%) studies are published in allied health or public health journals. Eighteen studies were found from internal medicine journals, five studies in both policy and management and nursing journals, four studies were published in surgical, family medicine, or IM journals. Specialty journals focusing on Obstetrics and Gynecology (OB/GYN), psychiatry, pain medicine, substance use, and patient experience have one published study each.
Nineteen (34%) studies reported using the term “shared medical appointment(s),” the most commonly used term to describe MGVs. The other terms used were “group medical visit(s)” or “medical group visit(s)” (n = 11), “group visit(s)” (n = 9), “group appointment(s)” (n = 4), and “integrative medical group visit(s)” (n = 4). Sixteen (29%) studies compared MGVs with current existing standard of care, such as one-on-one clinical visits, whereas only one study used another group-based therapy as the comparator.
Studies used a variety of recruitment strategies such as physician referrals (n = 31, 56%), patient mailings (n = 15, 27%), phone outreach (n = 14, 26%), electronic medical record search (n = 9 16%), and flyer placement (n = 6, 11%).
Study setting
Of the 55 studies included, 8 studies were conducted in Canada, and 47 were conducted in the United States. Most of the studies took place at an Academic/University-affiliated hospital (n = 31, 56%), followed by CHCs (n = 10, 18%), HCOs (n = 11, 20%), and private clinics (n = 3, 0.05%).
Study population
The mean age of participants reported in the studies (n = 41) ranged from 39 to 80 years of age and 15 studies had a mean age of >65 years. Nine studies comprised only women participants, two studies had all male participants, and other studies had a mix of both. Twelve studies (22%) invited caregivers or family members to attend the group.
Characteristics and components of MGV
Duration of MGVs
The most common session duration was 90 min (n = 22), followed by 2-h sessions (n = 10), and 1-h sessions (n = 5). Eight studies did not report duration.
Facilitators of MGVs
Forty-two studies reported the presence of two to four health professionals, seven studies report only one member leading the MGV and six studies comprised of more than five health professionals on the team. The composition mix of the MGV team is as follows: physicians (n = 48, 93%), nurse practitioners (n = 18, 32.7%), nurses (n = 26, 47.3%), medical assistants (n = 15, 27.3%), nutritionist/dieticians (n = 13, 23.6%), psychologists (n = 10, 18.2%), pharmacists (n = 10, 18.2%), social workers (n = 9, 16%), physiotherapists (n = 6, 11%), physician assistant/yoga instructor/exercise instructor/occupational therapist (each had n = 2, 3.6%), and other (n = 13, 45.5%), such as students and researchers. While most personnel were present at all sessions, some attended a few sessions as a guest facilitator.
Group diagnoses and health conditions
All groups had common defining themes such as the same medical condition, similar risk factors, same sex, or age group. Twelve studies had a combination of several chronic conditions seen within the primary care setting. Ten included patients with chronic pain conditions of which five had a mix of chronic pain conditions and five focused on single pain conditions. Nine studies focused on cardiovascular conditions. Other MGV themes that were seen in studies included preventative care, screening, and advance care planning (Table 1).
Medical Group Visit Health Conditions Included Within Groups
The MGV contained a mixture of these conditions.
These conditions were represented by one study each unless otherwise reported.
MGV, Medical Group Visit.
Curriculum
While most studies had a curriculum defined a priori before the MGV began, eight studies allowed patients to choose their own topics and activities for discussion. All studies had a didactic component, where a health care provider lectured the group on various topics. These didactics were offered as educational videos in nine studies. Didactic areas include (1) medical topics, such as symptoms management (n = 27) of which 14 included pain management and 8 included alternate options for the disease treatment (e.g., nonopioid options for chronic pain conditions) and, (2) lifestyle/educational component (n = 33) that comprised talks on nutrition (n = 29), exercise (n = 20), stress (n = 16), and sleep (n = 10). Eight studies reported having a psychological component in their curriculum that included cognitive behavioral therapy (n = 5) and stress reduction (n = 4).
Studies also incorporated an experiential learning component by employing a variety of Mind–Body or IM activities (n = 13), such as meditation (n = 6), mindfulness techniques (n = 8), yoga (n = 5), t'ai chi/qigong (n = 3). Mindfulness techniques included body scan (n = 3), guided imagery (n = 2), and biofeedback and journaling (n = 2). Other experiential activities employed were group exercise (n = 7), cooking demonstrations (n = 3), completing advance care planning forms (n = 2), and music therapy (n = 1).
MGVs also provided “take home” items, such as MGV agenda and guides (n = 10), Compact Discs (n = 3), journals (n = 2), and monitors such as pedometers (n = 2), and blood pressure monitors (n = 1). A socializing component such as dedicated time to interact with peers using cooperative games (n = 6), and healthy meal and snacks (n = 11) were also reported. Goals and action plans for participants were suggested in nine studies (Table 2).
Description of Medical Group Visit Components
BP, blood pressure; CD, compact discs; MGV, Medical Group Visit.
Clinical and administrative requirements
While all studies report eliciting consent for research (when applicable), only 21 studies reported confidentiality or Health Insurance Portability and Accountability Act (HIPAA) documentation. Twenty-three studies described making changes to the medication of the study participants and only four studies reported vitals measurement in the MGV description. Seventeen studies (31%) reported billing for the MGV through the Current Procedural Terminology code 99212–99214, the routine appointment code with a complexity level 2, 3, or 4, respectively.
Outcomes
Patient satisfaction (PS) was the most frequently measured outcome as seen in 40 studies. Of these 40 studies, 38 studies reported high PS and 2 studies found no difference between the comparator and intervention. The second common outcome assessed was increase in patient knowledge (IPK), which was reported in 31 studies. Twenty-five studies reported on symptom severity, 17 studies reported on health care utilization, 13 studies calculated cost effectiveness, 11 reported on QoL and 8 studies reported staff experience (Table 3).
Outcomes Measured in Medical Group Visits
Among the nine RCTs, significant (p < 0.05) primary outcome results were seen in six studies; reduced Emergency Department visit (n = 2) in a mixed chronic disease group, 29,66 medication adherence in a heart failure group, 69 weight reduction and improvement of fruit and vegetable intake in a coronary artery disease group, 70 and IPK in a heart failure group (Table 4). 46
Randomized Controlled Trial Quality Assessment Results
a—Randomization adequate? Was the allocation sequence adequately generated?
b—Allocation concealment? Was allocation adequately concealed?
c—Outcome assessors blinded (hard outcomes)? Were Outcome assessors blind to treatment assignment for “hard outcomes” such as mortality?
d—Outcome assessors blinded (soft outcomes)? Were Outcome assessors blind to treatment assignment for “soft outcomes” such as symptoms?
e—Lack of measurement bias? Were the measures used reliable and valid?
f—All outcomes reported? Are reports of the study free of suggestion of selective outcome reporting (systematic differences between planned and reported findings)?
g—Incomplete outcome data adequately addressed.
h—Adequate power for main effects?
i—Other selection bias? Were systematic differences observed in baseline characteristics and prognostic factors across the groups compared?
j—Comparable groups maintained? Consider issues of crossover, adherence (major differences in adherence to the interventions being compared), contamination, or other systematic differences in care that was provided.
k—Conflict of interest.
Discussion
This systematic scoping review is the first to uncover the MGV characteristics and common components in a breath of study methodologies and provide supportive evidence to inform the research of MGVs for a variety of health conditions. This review identified 55 unique studies within the realm of chronic disease. An all-encompassing and broad inclusion criteria that combined nonlike conditions allowed us gather in-depth characteristics data. We found that a majority of studies were observational in design, recruited patients using physician referrals, and took place at academic and university-affiliated hospitals. Authors conducted MGVs for either similar health conditions or specific themes of focus and used an interdisciplinary team to facilitate sessions. The curriculum components largely included a didactic, experiential, and socializing component. Lastly, we identified key administrative components that MGVs have integrated into their structure. Figure 2 is a pictorial representation of the characteristic and components of MGVs.
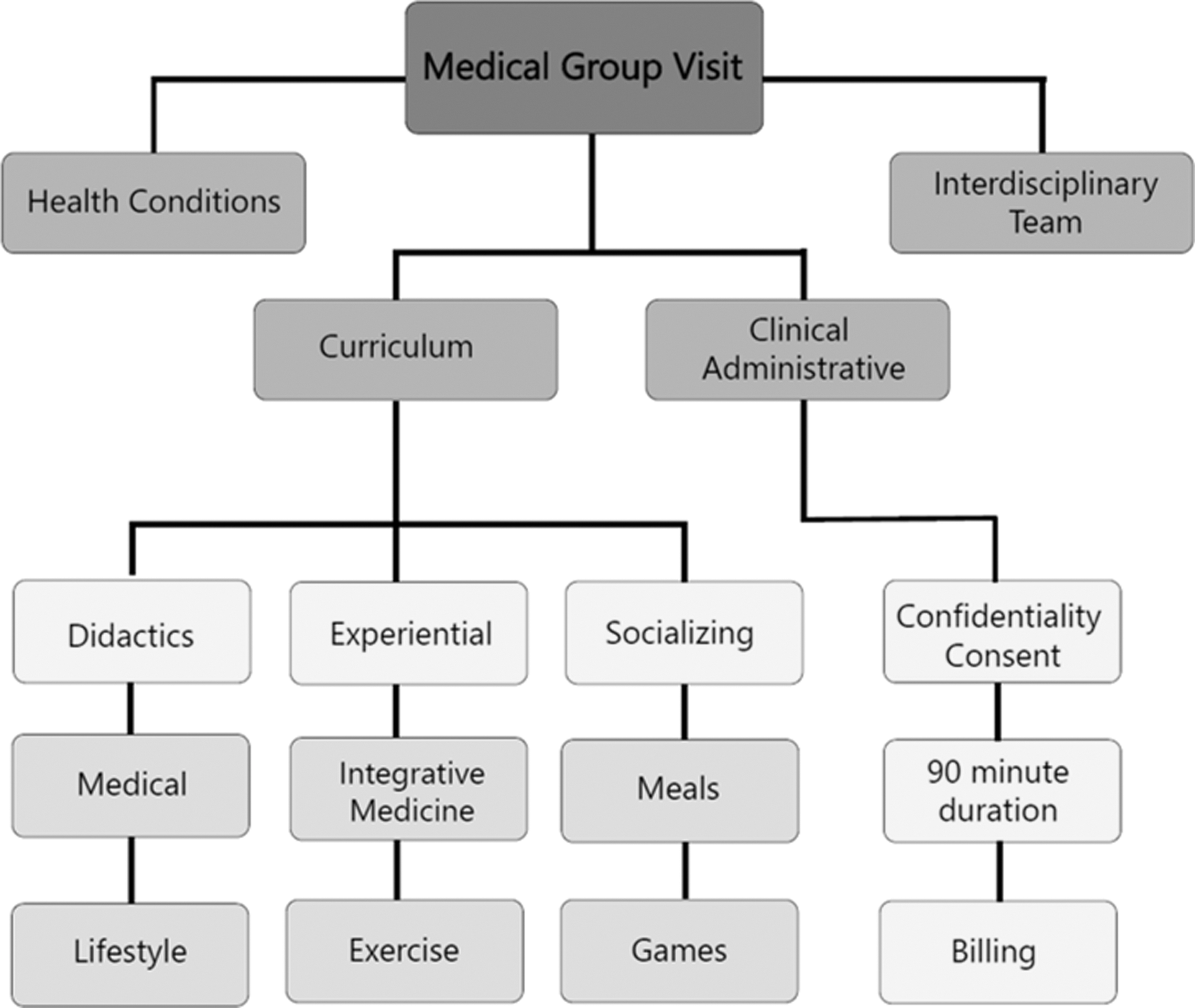
Characteristics and components of the medical group visit.
MGV literature
A rapid rise in the publication of MGV studies since 2014 in both primary care and subspecialties demonstrates its growing appeal and importance in managing chronic diseases. Sixty percent of the included studies were published in specialty (i.e., surgical, OB/GYN) or public health and allied sciences journal, highlighting the adaptability of the MGV methodology for varied specialty settings.
Age and sex
We found that demographic data are not always fully reported in the MGV literature, therefore, affecting the interpretation of our findings. As this is a review of MGVs for chronic health conditions, the population studied was, unsurprisingly, either middle aged or elderly. This is the ideal target population for MGVs as 88% of the population 65 years of age and older have one or more chronic condition causing significant health expenditure. 78 In recent years various disease management programs, treatment protocols, and patient education efforts have been developed to prevent progression of specific chronic conditions and to improve ongoing disease management. 79 The role of MGVs should be further considered as a model to address the huge demand for health care in the aging population with increasing case complexity.
Unsurprisingly, MGV literature reported a high female participation. It is well known that women are more likely to engage in health-promoting behaviors than men. 80,81 It is unknown if providers do not refer men to MGVs, or if men do not want to attend them. However, the study that included a male-only population showed high participant satisfaction and allowed the exchange of common gender-specific health education and preventative counseling. 26
Characteristics of MGV
The review by Kirsh et al. 18 identified MGV themes, such as dose, multiprofessional team, behavioral intervention, and peer-to-peer support. 17 Our scoping review has been successful in characterizing some of these themes. The “dose” of intervention can be defined by duration of individual session, frequency of session, and size. We identified that the average duration of MGVs was 90 min, but the frequency of meetings varied greatly from 1 to 10 sessions and depended on the type of patient condition. No studies in our review studied the ideal number of visits required to reach their outcomes or the ideal number of patients in a group.
In traditional one-on-one appointments, the number of people who can access care is dependent on clinician availability. In the interdisciplinary model, as used by most of the included studies, there are reports of increased efficiency through task shifting and perceived increase in time with provider. 49 An example provided by one study as a means of improving efficiency was to conduct examinations in front of the group. 76 They report that this practice saved time from going back and forth to a separate examination room and to the group room, and also was done with minimal patient discomfort and embarrassment. Another MGV utilized white noise or soft music while having in-room, private conversations saving a separate conversation after the group ended. 28 Although patients are accepting these time-saving measures, importance should be given to privacy, safety, and confidentiality. Consequently, all participants should complete HIPAA documentation, given the open sharing of private health information. In our study, only 21 studies reported using HIPPA waivers.
Out of 55 studies, only 1 study explicitly reported that there were no adverse events. 34 However, there were patient concerns through qualitative analysis about breaking patient confidentiality. Although refuted by previous studies, this remains a compelling concern for some patients. 82
The health conditions studied were varied and chronic pain was one of the top studied condition, an indication that complicated pain management may benefit from more than a one-on-one appointment. Studies 83 have utilized pain group education (e.g., back schools) to show improvement in diminishing pain and improved functional health; an easy achievable component during a MGV. MGVs may also be able to satisfy the American Pain Society guidelines, which recommends that patient receive education and self-care skills about pain management 84 through its emphasis on didactics.
Thirteen studies reported the use of IM modalities in their MGVs, the most frequently used modality for experiential learning. The use of mindfulness techniques was the most common IM modality seen in studies. Mindfulness has been studied for several psychiatric conditions, including anxiety and depression. 85 Chronic conditions are often associated with psychological responses and utilization of mindfulness in MGVs may increase flexibility of MGVs to accommodate mental health concerns. Using IM modalities during individual visits are likely limited by time and need for additional professionals. The frequent use of these modalities in MGVs and invitation of IM-trained guest facilitators offers evidence for its feasibility and importance in the management of chronic conditions.
An important aspect of the MGV is billing and reimbursement. Billing as an individual Evaluation and Management code (99212–99215) even in the group setting was the most popular method of billing seen in the included studies. An alternative way of reimbursement was through global billing (group visit was one part of a bundle of care), using other group codes such as nutrition management code or fee for service charge. While Medicare has not issued current payment codes, its response to billing queries was “a physician could furnish a medically necessary face-to-face E&M visit that is observed by other patients.” 86 Although it is reassuring that large payers such as Medicare are acknowledging the cost-saving potential of MGVs, there is still no nationally accepted standard billing code for MGVs. This is likely a deterrent for providers interested in pursuing MGVs in their practice.
Study limitations and outcomes
Many studies acknowledge their limitations of a small sample size, and the difficulty in a double blinding the interventions due to the nature of the MGVs. This inherent methodology bias was overcome by the one study, which used another group as a comparator. 40 An important source of bias arose from including patients who previously showed interest in attending MGVs to attain maximal attendance to reduce attrition bias. Studies also report hand picking patients who would be appropriate for the group and giving patients the option to randomize themselves. Additionally, the control group or “usual/standard-of-care” term is not well defined in most studies. While this usually meant individual, one-on-one appointments with the provider, a detailed description of the comparator group was not attained from the studies. The choice of comparator directly affects validity of studies and has many potential areas of bias, which should be addressed by future studies. 87 Moreover, there are several clinically and statistically significant outcomes reported above, but authors rarely report on the maintenance of this improvement after the study has been completed.
Strengths and limitations
The main strength of this scoping review is having a broad inclusion criterion which facilitated the detection of several diverse studies. This changed the focus from the study of well-defined conditions and robust study methodologies to collecting general characteristics and components data that have not been compiled previously.
One of the major limitations of this study was the data synthesis of studies with substantial heterogeneity and complexity of intervention content. While head to head comparisons are impractical for a scoping review such as this, the heterogeneity observed made assimilation of data a challenge. Another limitation is the inability to produce accurate characteristic compilation due to nonreporting of key data (i.e., mean age) by some studies. Other limitations include excluding articles published before 1990 to focus on latest trends, exclusion of studies that are part of psychological or psychotherapy research literature, and excluding European studies.
Future recommendations
In this scoping review, we identified components and characteristics of MGVs that are similar across the board. However, there is significant diversity in the intervention approach depending on the setting, population, and condition as described above. Further analysis of these approaches would help in better targeting of MGV interventions to patients and contexts, where it is most likely to be effective. We have also attempted to dissect the MGV structure to allow researchers to study individual components. For example, same-sex groups were employed by very few researchers and more research is needed to understand the risks and benefits of single-sex groups. Description of the MGV dose and long-term outcomes were lacking in studies and should be considered for future research. Inherent study design biases reported above will be difficult to eliminate but researchers should aim for adequate power and set up appropriate comparison groups.
Conclusions
This scoping review of the literature demonstrates that MGVs have a growing body of evidence. The mechanisms regarding why and how MGVs appeal to patients and result in better outcomes are multifold and this review has unpacked a few characteristics that may contribute to its recent interest in research and implementation. As health care systems are rapidly evolving, patient-centered care models, such as MGVs, can be used as an adjunct or alternative in chronic disease management, education, and providing training with self-management skills to more patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Appendix
Study Characteristics
| Author, year | Setting | Medical condition | Sample size (% female) | Mean age | Total group visit sessions/total groups | Group size | Duration (h) | Number and type of health personnel | Outcomes |
|---|---|---|---|---|---|---|---|---|---|
| Adams et al., 2015 | AUAH | Depression, anxiety, bipolar | 15 (60) | 54.5 | 14 sessions, 1 group | 12-Jun | 2 | 4—MD, PA, YI, EI | SSM |
| Ayoub et al., 2009 | HS | Screening for osteoporosis | 1372 [583 in I and 789 in C] (100) | 75.3 | 1 session, >1 group | 8-Jul | 2 | 2—MD, N | HU, MM |
| Campbell et al., 2009 | AUAH | Men's health | 261 (0) | n/r | 1 session, 38 groups | 7 | 1.5 | 2—MD, MA | PS, IPK |
| Chao et al., 2015 | AUAH | Pelvic pain | 26 (100) | 39.8 | 10 sessions, 3 groups | n/r | 2 | 1—NP | PS, SSM, QoL, IPK |
| Coleman et al., 2001 | HS | Asthma, COPD, CHF, diabetes, heart disease, hypertension | 295 [146 in I and 149 in C] 59% | 74 | 7, n/r | 12-Aug | 2 | 6—MD, N, PT, N/D, P, SW | HU |
| Cornelio-Flores et al., 2017 | AUAH | Chronic pain conditions | 19 (89) | 51.6 | 9 sessions, 2 groups | n/r | n/r | 2—MD, MA | PS, SSM, QoL, IPK |
| De Vries et al., 2008 | PC | COPD | 6 (33) | 67 | 4 sessions, 1 group | 6 | 1.5 | 5—NP, N, MA, PT, student NP | SSM, CE, HU, MM |
| Delichatsios et al., 2015 | AUAH | Metabolic disorders | 70 (80) | n/r | 1 session, 17 groups | 10-Aug | 1.5 | 4—MD, MA, N/D, medical student | PS, CE |
| Doorley et al., 2017 | CHC | Substance abuse | 77 (41) | 41 | 1 session, 82 groups | 10-May | n/r | 5—MD, N, P, Psy, social worker | MM |
| Dorsey et al., 2011 | AUAH | Parkinson disease | 30 [15 in I and 15 in C] 36.5% | 69.4 | 4 sessions, 6 groups | 14-Jun | 1.5 | 1—MD | PS, SSM, IPK, QoL |
| Dresner et al., 2016 | AUAH | Depression, anxiety, chronic pain condition, obesity | 19 (68) | 53.1 | 8 sessions, 7 groups | 12-Aug | 2.5 | 3—MD, N, RA | PS, SSM |
| Ely et al., 2011 | AUAH | Obesity | 29 [19 in I and 10 in C] 97% | 49.8 | 16 sessions, 2 groups | 19 | 1.5 | 3—MD, N, Psy | SE, SSM, QoL |
| Fletcher et al., 2006 | AUAH | Urological | 287 [177 in I and 110 in C] (24.9) | 63 | 1 session, >1 group | 12-Aug | 1.5 | 4—MD, NP, N, social worker | PS, CE, IPK |
| Fuchs et al., 2016 | AUAH | Anxiety and depression | 29 (45) | 50.97 | 1 session, 5 groups | n/r | 1 | 1—Psy | PS, SSM, HU, IPK |
| Gardiner et al., 2014 | AUAH | Chronic pain conditions, depression, hypertension, anxiety, obesity, diabetes | 65 (68) | 50.7 | 8 sessions, 7 groups | 12-Aug | 2.5 | 5—MD, massage therapist, meditation instructor | PS, SSM |
| Geller et al., 2011 | CHC | Preventative heart disease, diabetes, depression, | 57 (n/r) | 56.3 | 1 session, >1 group | n/r | 1.5 | 1—MD | QoL |
| Giladi et al., 2014 | AUAH | Macromastia | 57 (100) | n/r | 1 session, >1 group | 15-Jun | 1.5 | 3—MD, N, MA | PS, HU, CE, IPK |
| Harris, 2010 | AUAH | Post cardiac surgery | 34 (n/r) | n/r | 1 session, >1 group | n/r | 1.5 | 2—NP, N, MA | PS |
| Heyworth et al., 2014 | HS | Hypertension, cardiovascular disease, chronic pain condition, diabetes, tobacco use | 1842 [921 in I and 921 in C] (44) | n/r | n/r, >1 group | 10 | 1.5 | 4—MD, NP, Psy, social worker | PS, CE, HU, IPK |
| Housden et al., 2017 | AUAH | Rheumatoid arthritis, osteoarthritis, CHD, heart failure, obesity, diabetes | 24 [17 in I and 7 in C] (n/r) | n/r | 1 session, 7 groups | 28-Dec | n/r | 5—MD, NP, pharmacist | PS, SE, IPK |
| Jhagroo et al., 2016 | AUAH | Metabolic stones prevention | 176 [113 in I and 63 in C] (43.5) | 53.8 | 1 session, 5 groups | 9 | 1 | 2—MD, D | PS, IPK |
| Kirk et al., 2017 | HS | Hypertension and medication management | 47 [21 in I and 26 in C] (79) | 61.8 | 1 session, 4 groups | n/r | 1.5 | 2—MD, N, N/D, P, Psy, social worker | SSM, MM, IPK |
| Lavoie et al., 2013 | HS | Chronic pain condition, diabetes, cardiovascular illness, depression | 29 (65.5) | 62 | n/r, >1 group | 20-Dec | 1.5 | n/r—MD, NP, MA, N, primary health coordinator community/health representative | PS, SE, IPK |
| Levine et al., 2010 | HS | Geriatric population | 1236 [221 in I and 1015 in C] (65) | 78.2 | n/r, >1 group | 16-Dec | 1.5 | 3—N, MD, MA | PS, SE, HU, CE, IPK |
| Lin et al., 2008 | AUAH | Heart failure | 33 (27) | 73 | 2 sessions, >1 group | 8-Jun | 2 | >5—MD, N, N/D, P, Psy | PS, SSM, QoL, HU, MM, IPK |
| Lorentz et al., 2012 | AUAH | Postbariatric surgery follow-up care | 199 (n/r) | n/r | 1 session, >1 group | 5 | >3.5 | 4—MD, N, N/Bariatric program coordinator | PS, CE, HU |
| Lum et al., 2016 | AUAH | Advance care planning | 32 (59) | 79 | 2 sessions, 5 groups | 12-Aug | 2 | 2—MD, social worker | PS, IPK |
| Lum et al., 2017 | AUAH | Advance care planning | 118 (62) | 76 | 2 sessions, 16 groups | 11-Apr | 2 | 3—MD, MA, social worker | n/r |
| MacKay, 2011 | CHC | General OBGYN health | 103 (100) | 55 | 1 session, >1 group | 18–20 | 2 | 2—MD, MA | PS |
| Masley et al., 2001 | AUAH | Coronary heart disease | 97 [48 in C and 49 in I] 25.5% | 65 | 14 sessions, 2 groups | n/r | 1 | 1—NP | PS, CE |
| May et al., 2014 | HS | Geriatric syndrome screening | 136 (61.80) | 80 | 3 sessions, >1 group | 6–8 | 1.5 | 3—MD, N, MA | SSM, IPK |
| Mehl-madrona and Mainguy, 2017 | AUAH | Minor neurocognitive disorder | 32 (n/r) | n/r | 6 sessions, 2 groups | 15 or less | 2 | 3—MD, N, Psy | PS, SE, SSM, QoL, IPK |
| Miller et al., 2004 | CHC | Cardiovascular disease, diabetes, osteoarthritis | 28 (100) | 50 | 6 sessions, 86 groups | 7 | 1.5 | 2—MD, NP | PS, HU, MM |
| Montoya et al., 2016 | AUAH | Chronic kidney disease | 30 [16 in I and 14 in C] 53% | 68.1 | 6 sessions, 2 groups | 8 | 2 | 5—MD, NP, N/D, P, SW | IPK, PS, SE |
| Murray and Everson, 2005 | PC | Lifestyle modification | n/r (100) | 55 | n/r, >1 group | n/r | 1.5 | 4—MD, N, N/D, YI | n/r |
| Palaniappan et al., 2011 | HS | Obesity | 430 [74 in I and 356 in C] (70) | 49.7 | 1 session, n/r | 12-Jun | 1.5 | 1—MD | SSM |
| Pastore et al., 2014 | AUAH | Cardiovascular disease prevention in women | n/r (100) | n/r | n/r, >1 group | 12-Jun | 1.5 | >5—MD, NP, N/D, P, EI, diabetes educator | PS, SSM, MM, IPK |
| Patel et al., 2017 | AUAH | Carpal tunnel, trigger finger, hand arthritis, cysts, sprains, fractures | n/r (n/r) | n/r | 4 sessions, n/r | 10 | 1 | 5—Surgeon, NP, MA, PA, medical student | PS, SSM, CE, IPK |
| Paul et al., 2013 | CHC | Heart failure | 17 (29.5) | 65 | 1 session, 4 groups | 6 or less | 1.5 | 3—NP, MA, PT | PS, SE, SSM, CE, IPK |
| Rahaghi et al., 2014 | AUAH | Pulmonary arterial hypertension | 53 (74) | 65 | n/r, 7 groups | 10-Aug | 1.5 | 2—MD, N, Research fellow | PS, IPK |
| Rayburn, 2017 | CHC | Back pain | 98 (n/r) | n/r | 5 sessions, >1 group | 10 | n/r | 3—MD, N, MA, maintenance worker | PS, SSM |
| Roll et al., 2015 | CHC | Substance abuse | 28 (29) | 40.7 | n/r, >1 group | 10-Aug | 1.5 | 4—MD, N, P | PS, SSM, QoL, IPK |
| Romanelli et al., 2017 | CHC | Back/neck, joint/bone, nerve, muscle, headache, cancer | 130 (56.2) | 50 | 1 session, 14 groups | 10-Sep | 1.5 | 2—MD, MA | PS, SSM, QoL, IPK |
| Remick, 2014 | AUAH | Anxiety, bipolar, schizophrenia | 99 (55.6) | 55.76 | 11 sessions, 1 group | 8-Jun | 1 | 1—MD | PS |
| Scott et al., 2004 | HS | CHF, COPD, blindness, deafness, diabetes, asthma, ulcers, arthritis, hypertension, angina, MI, stroke, kidney disease, cancer, | 294 [145 in I and 149 in C] 59% | 74 | n/r, 19 groups | 8 | 1.5 | 6—N/D, P, OT, MD, N, PT | PS, SE, QOL, CE, HU, IPK |
| Shojania and Ratzlaff, 2010 | PC | Rheumatoid arthritis | 19 (68) | 52 | 6 sessions, 1 group | 13–15 | >3.5 | 3—MD, N, PT, N/D, occupational therapist | PS, CE, IPK |
| Singrey et al., 2015 | AUAH | Heart failure | n/r (n/r) | n/r | 8 sessions, 2 group | 15-Jun | 2 | >5—MD, NP, PT, P, N/D, Psy | SE, MM |
| Smith et al., 2014 | AUAH | Heart Failure | 198 [92 in I and 106 in C] 38% | 62.3 | 10 sessions, 2 groups | 5 | n/r | 4—NP, N/D, Psy | HU, MA |
| Stults et al., 2016 | HS | Mixed chronic conditions | 30 (33.3) | 70 | 5 sessions, >1 group | 30 | n/r | 3—MD, MA, Psy | PS, IPK |
| Thacker et al., 2005 | AUAH | General OBGYN health and preventive measures | 364 (100) | n/r | 1 session, 48 groups | 8-Jun | 1.5 | 4—MD, N, Psy, social worker | PS, HU, IPK |
| Vogler et al., 2017 | AUAH | Back pain, lower extremity pain, upper extremity pain, neck pain, neuropathy, arthritis, fibromyalgia | 35 (77) | 58 | 4 sessions, 20 groups | n/r | 1.5 | 4—MD, N, P | PS, SSM, QoL, HU, MM, IPK |
| Smith et al., 2008 | HS | Pelvic pain | 48 (100) | 49.1 | 10 sessions, 1 group | 10 | 2 | 2—NP, nurse midwife | PS, SSM, HU |
| Wong et al., 2015 | CHC | Diabetes, high BP, arthritis | 63 (65) | 62 | n/r, >1 group | 15-Oct | 1.5 | 4—MD, NP, N, P | PS, SE |
| Wong et al., 2016 | AUAH | Carpal tunnel | 75 [36 in C and 39 in I] 51.3% | 55 | n/r | 12-Aug | 35–45min | 2—MD, N | IPK, PS |
| Yehle et al., 2009 | CHC | Heart failure | 52 [13 in I and 10 in C] (40.38) | 66.95 | 1 session, 1 group | 6 | 1 | 2—MD, NP | SSM, CE, HU, IPK |
AUAH, Academic/University affiliated hospital; BP, blood pressure; C, control; CE, cost effectiveness; CHC, Community Health Center; CHD, coronary heart disease; CHF, congestive heart failure; COPD, chronic obstructive pulmonary disease; EI, exercise instructor; HS, health system; HU, health utilization; I, intervention; IPK, increase patient knowledge; MA, medical assistant; MC, medication changes; MD, physician; MT, massage therapist; NP, nurse practitioner; N, nurse; N/D, nutritionist/dietician; n/r, not reported; OBGYN, Obstetrics and Gynecology; P, pharmacist; PA, physician assistant; PC, private clinic; PT, physical therapist; PS, patient satisfaction; Psy, psychologist; QoL, quality of life; SE, staff experience; SSM, symptom severity measurement; YI, yoga instructor.