
Abstract
Objective:
The purpose of this pragmatic controlled trial was to examine changes in psychological and occupational well-being in professionals who attended a yoga-based program.
Setting:
The 5-day RISE (resilience, integration, self-awareness, engagement) program was delivered at the Kripalu Center for Yoga & Health. RISE included 5 h per day of yoga, meditation, lectures, and experiential activities.
Subjects:
Adult professionals from education, corrections, and social service institutions were pragmatically assigned to the RISE group (n = 61) or a waitlist control group (n = 60).
Outcome measures:
Measures of psychological and occupational well-being were completed before RISE (baseline), immediately after RISE (postprogram), and 2 months after RISE (follow-up). Analyses of covariance were conducted to compare change scores between groups.
Results:
Eighty-two participants (RISE n = 41, control n = 41) completed baseline and postmeasures and were included in the analysis, and 57 (RISE n = 27, control n = 30) also completed the follow-up. Relative to controls, the RISE group reported improvements in stress (p = 0.001, r 2 = 0.51), resilience (p = 0.028, r 2 = 0.34), positive affect (p = 0.001, r 2 = 0.52), negative affect (p = 0.001, r 2 = 0.52), mindfulness (p = 0.021, r 2 = 0.13), and job satisfaction (p = 0.034, r 2 = 0.08) from baseline to postprogram. From baseline to follow-up, compared with controls the RISE group showed improvements in stress (p = 0.001, r 2 = 0.33), resilience (p = 0.001, r 2 = 0.24), positive affect (p = 0.006, r 2 = 0.49), negative affect (p = 0.043, r 2 = 0.32), mindfulness (p = 0.001, r 2 = 0.28), empowerment (p = 0.005, r 2 = 0.20), and self-compassion (p = 0.011, r 2 = 0.19).
Conclusions:
The RISE program was associated with improvements in psychological and occupational well-being immediately after and 2 months after the program. Future research is needed to confirm these results.
Introduction
In this study, we are defining frontline professionals as those who are in stressful occupations and/or work with challenging, at-risk, or vulnerable populations. Such workers experience high levels of workplace stress, burnout, and compassion fatigue. 1 Examples of frontline professionals include police officers, first responders, teachers working with challenging populations, and mental health workers. Chronic occupational stressors, such as those faced by frontline professionals, put individuals at considerable risk for development of mental and physical health problems, 2 including increased risk for disease and mortality. 3 Workplace stress can also lead to higher employee turnover, 4 loss of productivity, and increased absenteeism, with 60% of all workers reporting loss of productivity due to stress in the previous month 5 and roughly 1 million U.S. workers absent for work each day due to stress. 6 The negative health outcomes associated with chronic occupational stress are not only prevalent but also preventable, and organizations that employ frontline professionals would benefit from providing their employees with evidence-based stress-reduction programs, particularly programs that are appropriate for frontline professionals.
Resilience is often defined as the ability to deal with challenges and adversity while maintaining or recovering psychological health. The development of resilience is critical for frontline professionals who frequently face repeated and sustained adverse circumstances in their work. The presence of resilience has been associated with psychological health, including reduced stress and improved mood, and occupational health, including higher job satisfaction and workplace happiness. 7 –13
Organizations would benefit from practical and cost-effective programs that improve employee resilience while also reducing costs associated with employee absenteeism and loss of productivity. Workplace programs aimed at fostering resilience often include components of mindfulness, self-compassion, self-regulation of stress, and cognitive behavioral techniques, and they have been shown to improve psychological health and job performance. 14,15
Yoga has been shown to improve psychological and occupational well-being in a variety of populations. 16 –18 Recent previous studies of yoga programs for frontline professionals have reported improved psychological and occupational well-being, including stress and resilience in university and government employees, 19,20 stress and mood in police officer trainees, 21 self-care, mindfulness, and burnout in nurses, 22 resilience, work engagement, and stress in intensive care unit workers, 23,24 work-related stress in mental health professionals, 25,26 anger and anxiety in active and retired armed forces members, 27 and stress and quality of life in academic medical center employees. 28 Recently, a Kripalu yoga-based program resulted in improvements in stress, depression, mindfulness, and aspects of self-compassion in mental health care professionals. 26 Despite these promising results, few studies have investigated the impact of brief, residential yoga-based programs developed specifically for professionals. 29
The yoga-based RISE (resilience, integration, self-awareness, engagement) program was developed for a variety of professional populations by the Kripalu Center for Yoga & Health (Kripalu). RISE is a secondary individual-level intervention as it seeks to provide employees with skills and practices that will improve their psychological health, particularly their resilience to stress. 30 In a recent single-arm pilot study of a 5-day residential RISE program with frontline professionals, improvements in mindfulness, stress, resilience, affect, vegetable intake, fruit intake, and sleep quality were reported from baseline to postprogram and were sustained at the 2-month follow-up. 29
The purpose of this study was to extend these previous findings through conducting a controlled trial comparing an RISE group with a waitlist control group. We hypothesized that relative to waitlist controls, the RISE program would yield significant improvements in measures of psychological and occupational well-being, and health-related behaviors.
Methods
Participants
Frontline professionals from education (e.g., teachers from low-income communities), corrections (e.g., police), and social services (e.g., mental health workers) sectors were invited by Kripalu to attend RISE in 2017 and 2018 through Kripalu's partnerships with local organizations. Although all of the invited participants were from occupations and institutions that were considered as likely to be stressful, there were no specific inclusion criteria regarding the stress levels of either the individuals or the institution's work environment. A total of 155 individuals were sent an invitation e-mail from study staff containing information about the study.
Ten days before the program, these individuals were sent another e-mail inviting them to consent to participate in the study with a link to the baseline survey. A total of N = 121 participants enrolled in the study and completed baseline measures (78% of the 155 RISE attendees). Participants were provided with a $15 gift card for each survey they completed. The Partners HealthCare Institutional Review Board at Brigham and Women's Hospital approved all aspects of this research.
Group assignment
Four residential RISE programs were administered per year, with a total of eight program cohorts across the study timeframe. RISE attendees were placed into one of the eight cohorts and an attempt was made to match pairs of participants in each group in terms of age, sex, and occupational sector. However, the scheduling of RISE was also based on availability and individual and organizational preference, therefore matched pairs were not always possible. Cohorts were paired so that an earlier cohort (e.g., February 2017) acted as the experimental RISE group and a later cohort (e.g., June 2017) acted as the waitlist control group. No attendees or their organizations were aware of their group assignment.
Data collection
Questionnaires were administered by using the Partners HealthCare version of the REDCap online software platform or on paper at three time points: baseline (1–10 days before RISE), postprogram (1–10 days after RISE), and follow-up (2 months after RISE).
Intervention
In brief, RISE was delivered as a 5-day residential immersion program at Kripalu. Attendees were housed at Kripalu and stayed in multiguest dormitory-style rooms. The program included 5 h of daily structured sessions of yoga postures, sitting meditation, mindfulness practices, breathing techniques, and education about mindful communication, mindful sleep preparation, and mindful eating. All RISE attendees completed the program in its entirety. RISE was developed and administered by highly experienced, certified yoga teachers with at least 200-h Yoga Alliance training and additional RISE program training. The RISE program has also been described extensively elsewhere. 29
Measures
Demographics
Participants completed a demographic questionnaire, which included age, sex, race, ethnicity, and education.
Psychological health and well-being
Stress
The Perceived Stress Scale (PSS) is the most widely used psychological instrument for measuring the perception of stress. The 10 items were designed to tap how unpredictable, uncontrollable, and overloaded respondents find their lives. The PSS displays adequate levels of reliability and validity. 30,31
Resilience
The Resilience Scale (RS) is a 14-item scale that measures an individual's level of resilience, which is considered a positive personality characteristic that enhances individual adaptation. 32 The RS displays high levels of reliability and validity. 33
Positive/negative affect
Positive and Negative Affect Schedule (PANAS) is a commonly used measure of positive and negative mood composed of 10 positive mood terms (e.g., interested, enthusiastic) and 10 negative mood terms (e.g., distressed, guilty). The PANAS displays good reliability and validity. 34
Mindfulness
The Five Facet Mindfulness Questionnaire (FFMQ) is a well-validated, reliable 39-item scale for the assessment of mindfulness. 35 The FFMQ assesses five different dimensions of mindfulness: observing, describing, awareness, nonjudgment of experience, and nonreactivity to inner experience. 35 For this study, we only reported the total mindfulness score.
Empowerment
The Psychological Empowerment Scale (PES) is a 12-item scale based on the original questionnaire developed by Spreitzer 36 and then modified by Shellman 37 to measure participants' psychological empowerment. The PES displays acceptable levels of reliability and validity. 36,37
Self-compassion
The Self-Compassion Scale—Short Form (SCS-SF) is a brief, well-validated, and reliable version of the SCS. 38,39 The SCS-SF includes 12 items that measure self-compassion along six factors; however, for this study, we only reported the total self-compassion score.
Satisfaction with life
The Satisfaction with Life Scale (SWLS) is a well-validated, short, 5-item scale that measures overall life satisfaction or global cognitive judgments of one's life. 40
Occupational well-being
Burnout
The Maslach Burnout Inventory—General Survey (MBI-GS) is a well-validated and reliable 16-item measure of professional burnout. 41 The MBI-GS measures burnout across three factors: Exhaustion (EX), Cynicism (CYN), and Professional Efficacy (PE).
Work engagement
The Utrecht Work Engagement Scale (UWES) is used to measure work engagement across 3 subscales: Vigor (VI), Dedication (DE), and Absorption (AB). 42 A total work engagement score is also obtained by summing the three subscales. The UWES-9 displays good validity and reliability. 42
Job satisfaction
The single-item Job Satisfaction Scale 43,44 measures job satisfaction with a single item, “At this moment, I am fairly satisfied with my job,” with the response rated from 1 (strongly agree) to 5 (strongly disagree). Lower scores represent higher job satisfaction.
Healthy behaviors and sleep quality
The Lifestyle Questionnaire is a self-report questionnaire of health-related behaviors, including diet and physical activity, and sleep quality that was developed by combining questions from other well-validated lifestyle behavior questionnaires, including measures of patient health behaviors 45 and the Pittsburgh Sleep Quality Index. 46
Program expectation
The Credibility Expectancy Questionnaire (CEQ) is a two-item scale modified for this study that measures the degree to which an individual feels that a particular treatment or program will be beneficial. Revised Item 1 reads: At this point, how much do you really feel that the Kripalu program will help enhance your quality of life? Participants rate this item on a scale from 1 (not at all) to 9 (very much). Revised Item 2 reads: By the end of the Kripalu program, how much improvement in your quality of life do you really feel will occur? Participants rate this item from 0% to 100%. The original CEQ displays adequate levels of reliability and validity.
Program impact
An Impact Questionnaire was created by the authors to assess perceived program feasibility, participants' continued use of RISE skills and practices, and the multiplier effect (i.e., sharing aspects of the program with coworkers). Immediately after RISE (post), on a visual analogue scale (VAS) from 0 (not at all) to 100 (very much so), participants were asked to indicate the degree to which they planned on practicing RISE skills and concepts (e.g., breathing techniques, yoga classes), how likely they were to share what they learned in the program with others, and how feasible it was for them to accommodate the program into their schedule.
At the 2-month follow-up, a VAS assessed: (1) the degree to which they had been practicing RISE skills and concepts (e.g., breathing techniques, yoga classes) since the program; (2) the degree to which they observed a positive shift in their workplace experience as a result of being in the program; and (3) the degree to which they shared what they learned in the program with others.
Data analysis
Analyses of variance (ANOVAs) were conducted to compare baseline scores between groups. Analyses of covariance (ANCOVAs) controlling for baseline differences were performed to compare change scores between groups for baseline to post, and baseline to the 2-month follow-up. Pearson correlations were performed between questionnaires' change scores (alpha level = 0.05). No adjustments were made for multiple outcome measures (e.g., to reduce type I error) based on the relatively small sample size and preliminary nature of this study. Missing data were dealt with through means replacements if <10% of item responses were missing for any given questionnaire. All quantitative data were analyzed by using IBM SPSS version 24.0 (IBM Corp, Armonk, NY).
Results
Participants
Of the N = 121 individuals who enrolled and completed the baseline measures, N = 82 also completed postprogram measures (68% of initial sample; labeled “partial completers”) and N = 57 participants completed all three time points, including the 2-month follow-up (47% of initial sample; labeled “full completers”). Only participants who completed at least the baseline and postmeasures were included in the initial analysis, leaving a final N = 41 in the RISE group and N = 41 in the control group (Fig. 1). The demographics for the analyzed sample (N = 82) are displayed in Table 1. There were no significant between-group differences on any demographic variable.

Participant CONSORT diagram. CONSORT, Consolidated Standards of Reporting Trials; RISE, resilience, integration, selfawareness, engagement.
Participant Demographics for Analyzed Sample (N = 82)
RISE, resilience, integration, self-awareness, engagement.
The baseline scores for participants from both groups who completed only the baseline measure (non-completers), participants who completed the baseline and postmeasures (partial completers), and participants who completed the baseline, post, and follow-up measures (full completers) are displayed in Table 2. A one-way ANOVA between the groups of non-completers, partial completers, and full completers revealed significant baseline differences in perceived stress, F(2, 113) = 5.57, p = 0.005, whereby the non-completers scored higher than partial completers (p = 0.001) and full completers (p = 0.023); negative affect, F(2, 112) = 3.69, p = 0.028, whereby non-completers scored higher than partial completers (p = 0.008) and full completers (p = 0.043); empowerment, F(2, 120) = 3.31, p = 0.040, whereby partial completers scored higher than full completers (p = 0.013); and self-compassion, F(2, 111) = 4.77, p = 0.010, whereby partial completers scored higher than non-completers (p = 0.003) and full completers (p = 0.014).
Baseline Means and Standard Deviations for Non-Completers (N = 39), Partial Completers (N = 25), and Full Completers (N = 57)
p < 0.05 compared with full completers.
p < 0.05 compared with partial completers.
p < 0.05 compared with non-completers.
FFMQ, Five Facet Mindfulness Questionnaire; MBI-GS, Maslach Burnout Inventory—General Survey; NA, Negative Affect; PA, Positive Affect; PES, Psychological Empowerment Scale; PSS, Perceived Stress Scale; RS, Resilience Scale; SCS, Self-Compassion Scale; SD, standard deviation; SWLS, Satisfaction with Life Scale; UWES-9, Utrecht Work Engagement Scale—9 item.
Organizational sector
Of the analyzed sample (N = 82), 30.5% were from the education sector (RISE n = 11, control n = 14), 29.3% were from the corrections sector (RISE n = 12, control n = 12), and 40.2% were from the social services sector (RISE n = 18, control n = 15). Participants from the education sector were the most likely to complete all three surveys (62% completed, n = 21), followed by corrections (58% completed, n = 18) and social services (32% completed, n = 18). An ANOVA revealed no significant baseline differences in outcome measures across the three sectors (all p-values >0.10).
Between-group baseline differences
An ANOVA revealed significant baseline differences between the two groups on several measures whereby the RISE group reported worse psychological health compared with the control group. Specifically, there were baseline differences in perceived stress, p = 0.004, RISE group (M = 18.64, standard deviation [SD] = 5.77), control (M = 14.63, SD = 6.20); resilience, p = 0.042, RISE group (M = 75.88, SD = 12.26), control (M = 81.20, SD = 10.85); positive affect, p = 0.019, RISE group (M = 32.11, SD = 8.06), control (M = 36.24, SD = 7.22); and negative affect, p = 0.018, RISE group (M = 23.13, SD = 5.96), control (M = 19.46, SD = 7.37). Therefore, posteriori ANCOVAs were conducted to control for baseline differences in perceived stress, resilience, positive affect, and negative affect across groups.
Psychological and occupational well-being
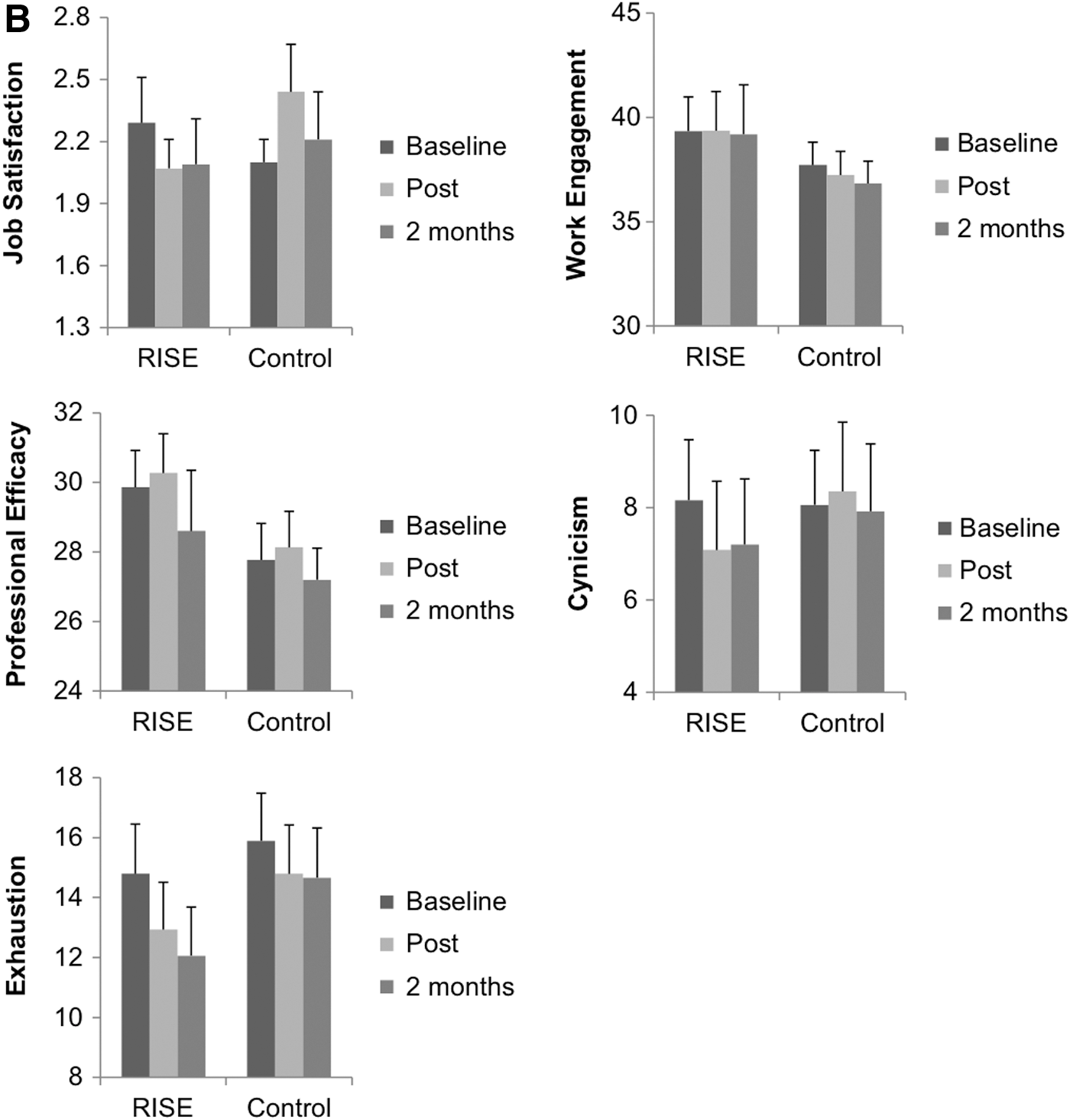
Figure 2 displays the adjusted means and SDs for psychological (Fig. 2A) and occupational (Fig. 2B) well-being measures at baseline, post, and follow-up. A one-way ANCOVA revealed that from baseline to postprogram, participants in the RISE group showed significant improvements in perceived stress, F(1, 72) = 26.96, p < 0.001, r 2 = 0.51; resilience, F(1, 74) = 5.07, p = 0.028, r 2 = 0.34; positive affect F(1, 73) = 22.10, p < 0.001, r 2 = 0.52; negative affect, F(1, 73) = 17.17, p < 0.001, r 2 = 0.52; mindfulness, F(1, 76) = 5.57, p = 0.021, r 2 = 0.13; and job satisfaction, F(1, 71) = 4.69, p = 0.034, r 2 = 0.08, compared with the waitlist control group (Table 3).
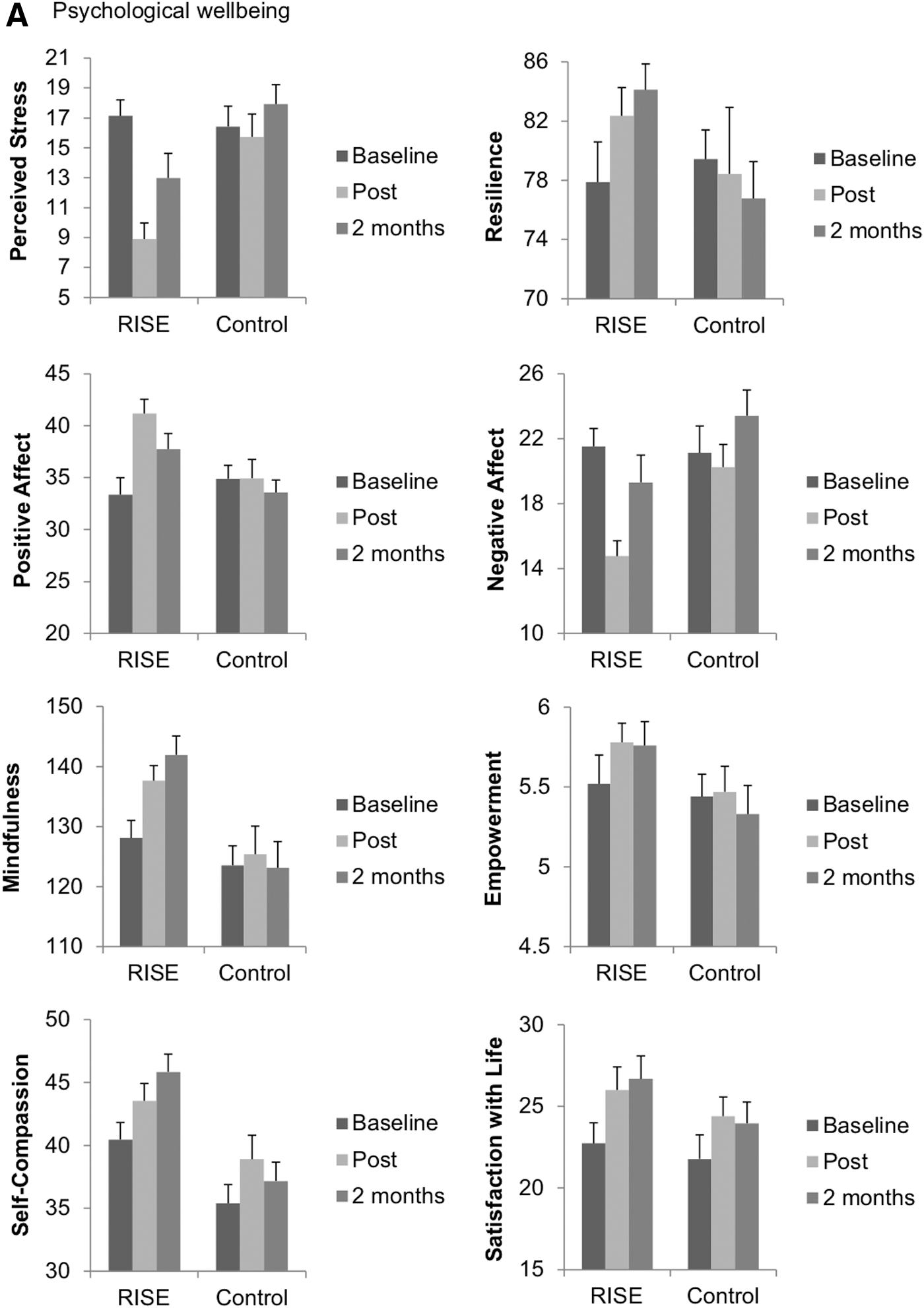
Adjusted means and standard errors of psychological
Adjusted Mean Change Scores (Post—Baseline, Follow-Up—Baseline), Within-Group Statistics (p), and Between-Group Statistics (p) for All Psychological and Occupational Well-Being Questionnaires
Bold values indicate significant results.
FFMQ, Five Facet Mindfulness Questionnaire; MBI-GS, Maslach Burnout Inventory—General Survey; NA, Negative Affect; PA, Positive Affect; PES, Psychological Empowerment Scale; PSS, Perceived Stress Scale; RISE, resilience, integration, self-awareness, engagement; RS, Resilience Scale; SCS, Self-Compassion Scale; SD, standard deviation; SWLS, Satisfaction with Life Scale; UWES-9, Utrecht Work Engagement Scale—9 item.
At the 2-month follow-up compared with baseline, participants in the RISE group showed significant improvements in perceived stress, F(1, 60) = 11.58, p = 0.001, r 2 = 0.33; resilience, F(1, 60) = 11.74, p = 0.001, r 2 = 0.24; positive affect, F(1, 60) = 8.18, p = 0.006, r 2 = 0.49; negative affect, F(1, 60) = 4.32, p = 0.043, r 2 = 0.32; mindfulness, F(1, 60) = 17.19, p < 0.001, r 2 = 0.28; empowerment, F(1, 62) = 8.37, p = 0.005, r 2 = 0.20; and self-compassion, F(1, 60) = 6.95, p = 0.011, r 2 = 0.19, relative to the waitlist control group. There was also a marginally significant improvement in the Burnout-exhaustion subscale in the RISE group compared with the waitlist control group, F(1, 59) = 3.73, p = 0.059, r 2 = 0.12 (Table 3).
Correlations between changes in perceived stress, resilience, positive affect, negative affect, empowerment, and self-compassion are displayed in Table 4 for the RISE group and Table 5 for the control group.
Pearson Correlations Between Questionnaire Change Scores for the Resilience, Integration, Self-Awareness, Engagement Group
p < 0.05; ** p < 0.01; *** p < 0.001.
FFMQ, Five Facet Mindfulness Questionnaire; NA, Negative Affect; PA, Positive Affect; PES, Psychological Empowerment Scale; PSS, Perceived Stress Scale; RS, Resilience Scale; SCS, Self-Compassion Scale; T1, baseline; T2, postprogram; T3, 2-month follow-up.
Pearson Correlations Between Questionnaire Change Scores for the Control Group
p < 0.05, ** p < 0.01, *** p < 0.001.
FFMQ, Five Facet Mindfulness Questionnaire; NA, Negative Affect; PA, Positive Affect; PES, Psychological Empowerment Scale; PSS, Perceived Stress Scale; RS, Resilience Scale; SCS, Self-Compassion Scale; T1, baseline; T2, postprogram; T3, 2-month follow-up.
Posteriori within-group analysis via paired samples t tests of the RISE group showed improvements in all measures from baseline to post and baseline to follow-up (all p-values <0.05) except for work engagement and the professional efficacy and cynicism dimensions of burnout.
Within-group analysis revealed that the control group also showed improvements in self-compassion from baseline to postprogram, t(35) = 4.17, p < 0.001; and satisfaction with life from baseline to postprogram, t(35) = 3.10, p = 0.004, and the 2-month follow-up, t(35) = 2.39, p = 0.022.
Healthy behaviors and sleep quality
There were no baseline differences in daily physical activity, fruit and vegetable intake, or sleep quality between the RISE and control groups (all p > 0.05). The adjusted mean change scores and SDs for physical activity, fruit intake, vegetable intake, and sleep quality are displayed in Table 6. A one-way ANCOVA revealed no between-group differences from baseline to post. At the 2-month follow-up, participants in the RISE group reported greater vegetable intake, p = 0.023, compared with participants in the control group.
Adjusted Mean Change Scores (Post—Baseline, Follow-Up—Baseline), Within-Group Statistics (p), and Between-Group Statistics (p) for Health-Related Behaviors and Sleep Disturbance
Bold values indicate significant results.
Average minutes per day.
RISE, resilience, integration, self-awareness, engagement; SD, standard deviation.
Analysis of within-group differences with paired samples t tests revealed improvements in the RISE group in physical activity, fruit and vegetable intake from baseline to post, which was sustained at the 2-month follow-up, and improvements in sleep quality from baseline to post. The control group showed no significant within-group differences.
Program expectation
Pearson correlations between participants' expected benefit of the RISE program on quality of life and questionnaire change scores revealed no significant relationships between Item 1, “At this point, how much do you really feel that the Kripalu program will help enhance your quality of life?” and changes in any outcome measure for the RISE group. However, there was a significant negative correlation between Item 1 and changes in positive affect from baseline to follow-up for the control group, r(34) = −0.34, p = 0.039. A significant correlation was revealed between Item 2, “By the end of the Kripalu program, how much improvement in your quality of life do you really feel will occur?” and changes in the exhaustion dimension of burnout from baseline to post for the RISE group; r(32) = 0.34, p = 0.045. There were no significant relationships between Item 2 and changes in any outcome measure for the control group.
Program impact
Feasibility
Participants rated the program as feasible to accommodate into their schedule, M = 78.97, SD = 23.64, N = 36.
Multiplier effect
At postprogram and follow-up, participants reported that they were likely to share what they learned in the program with others, M = 88.69, SD = 12.03, N = 39, and M = 69.30, SD = 19.50, N = 27, respectively. RISE participants showed a positive shift in their workplace experience, M = 67.18, SD = 17.76, N = 27.
Continuation of practice
At postprogram and follow-up, participants reported that overall, they planned to continue to practice the RISE techniques they learned, M = 67.97, SD = 18.82, N = 29, and M = 62.69, SD = 14.78, N = 20, respectively.
Participants' degree of planned practice of the yoga-based practices, skills, and concepts at post and the degree of actual practice of the yoga-based practices, skills, and concepts at the 2-month follow-up, and correlations between degree of practice at follow-up and preparedness to practice at post are displayed in Table 7.
Resilience, Integration, Self-Awareness, Engagement Participants' Self-Reported Degree of Practice at the 2-Month Follow-Up and Correlations Between Degree of Practice at Follow-Up and Preparedness to Practice at Post
p < 0.05; ** p < 0.01.
RISE, resilience, integration, self-awareness, engagement; SD, standard deviation.
Discussion
This was the first controlled trial of Kripalu's yoga-based RISE program. The RISE group showed significant improvements in perceived stress, resilience, positive affect, negative affect, mindfulness, and job satisfaction compared with waitlist control. There were no significant between-group differences in empowerment, self-compassion, satisfaction with life, burnout, work engagement, or healthy behaviors at the postassessment. However, the RISE group showed a marginally significant improvement in the exhaustion dimension of the burnout scale compared with the control group. At the 2-month follow-up, the RISE group reported continued improvements in all psychological health measures; perceived stress, resilience, positive affect, negative affect, and mindfulness, as well as additional improvements in empowerment, self-compassion, and vegetable intake compared with the control group. We also note that the control group showed significant within-group improvements in self-compassion at post and satisfaction with life at post and follow-up. These improvements could be due to participants reflecting on the questions in the survey and consciously or unconsciously modifying their behavior or outlook as a result (i.e., Hawthorne effect). However, at follow-up, self-compassion was no longer significant, and satisfaction with life decreased as compared with post, whereas these scores continued to increase in the RISE group at follow-up.
Occupational stress in frontline professionals can lead to severe health consequences, including increased risk of disease and mortality. Resilience is central to mediating workplace stress and reducing the negative outcomes such as compassion fatigue, burnout, and other mental health concerns, 47,48 The current results support the findings from our previous single-arm trial in which a similar cohort of frontline professionals showed improvements in many of the same measures, including resilience, stress, mindfulness, and affect. 29 In both studies, self-compassion improved only at the 2-month follow-up, suggesting that self-compassion may require a longer time scale to change than the other psychological constructs. 29 Importantly, self-compassion may protect against compassion fatigue, defined as providing ongoing empathy and compassion to others but neglecting one's own self-care. 49 Frontline professionals are at risk for compassion fatigue, making self-compassion an important target for improved psychological well-being in these populations. In addition to resilience, both self-compassion and mindfulness have also been proposed as psychological mediators for improvements in individuals' perception of their stress after yoga, 50 –52 and some researchers suggest that self-compassion and mindfulness enhance each other. 51 Future research with larger sample sizes and longer follow-up is needed to test whether these constructs mediate improvements in psychological and occupational well-being after RISE.
Although we detected improvements in job satisfaction, we did not observe improvements in work engagement or burnout between groups. A trend toward between improvements in the exhaustion dimension of burnout from baseline to follow-up was observed (p = 0.059). However, post hoc within subjects analysis revealed significant improvements in exhaustion from baseline to follow-up in the RISE group (p = 0.001) but not the control group (p = 0.299). One possible reason that we did not observe changes in the other dimensions of burnout or work engagement is that the participants were a heterogeneous group of frontline professionals from multiple sectors that have been shown to differ in their levels of these constructs. 51,53 For example, although not significantly different, participants from corrections had numerically higher baseline burnout rates on exhaustion and cynicism than education and social services, social services had higher baseline levels of work engagement than corrections and education, and education had higher baseline job satisfaction than corrections and social services. Further, measures of burnout and work engagement may only change over a longer time frame than 2 months and could also be dependent on level of practice after RISE. Additional research is needed to determine which interventions, outcome measures, and time frames are required to detect improvements in burnout within particular occupational sectors.
With respect to health-related behaviors, the RISE group reported increased vegetable consumption from baseline to the 2-month follow-up compared with the waitlist control group. Although there were no other between-group differences, the RISE group showed within-group improvements in physical activity, fruit and vegetable intake, and sleep quality from baseline to post and sustained improvements in physical activity and fruit and vegetable intake at the follow-up, whereas the waitlist group did not. Yoga practitioners report greater vegetable and fruit consumption than the general population, 54,55 and studies have reported increased vegetable and fruit intake after a yoga program. 48 Engaging in healthier behaviors after yoga interventions has been ascribed to increased mind–body awareness, whereby internal cues and their negative or positive sensations related to behaviors such as eating and physical activity are more easily noticed and drive behavioral choices. 56
Sustained improvement in psychological health after RISE is critical for continued prevention of chronic stress and is evidence that the skills are being practiced. A key component of the RISE program is integration of the RISE practices within the workers' daily workplace life, and tips for how to continue the practices and share them with others after the program. RISE participants reported continued use of the yoga-based practices at the 2-month follow-up, particularly the breathing practices. In an effort to induce a multiplier effect, during the program, RISE participants are encouraged to teach the practices and techniques to others, such as colleagues and clients, multiplying its impact within their work organizations. After RISE, participants reported that they were very likely to share what they learned in the program with other co-workers, and this was continued at the 2-month follow-up. They also reported a positive shift in their workplace as a result of their participation in RISE. An essential attribute of a workplace program for stress is its feasibility. On average, participants reported that it was feasible to fit the RISE program into their schedule after completion of the program. Therefore, the residential RISE program is a practical, feasible, and sustainable program that has shown preliminary efficacy for improving psychological health in frontline professionals relative to the waitlist control group.
This study was unique in that frontline professionals already attending the RISE program were invited to participate in the research evaluation. As such, we were able to pragmatically generate an effective waitlist control group with frontline professionals scheduled to attend RISE later in the same year. One strength of this pragmatic trial as compared with a more rigorously controlled study is the generalizability of the results to the real world, where the effects were actually observed. However, a limitation of this pragmatic approach is less control over the nature (e.g., demographics, sectors) of the two groups, and indeed, we observed between-group baseline differences in perceived stress, resilience, and affect. Although we statistically controlled for these differences by using an ANCOVA, future work would benefit from additional effort to insure matched pairs of sectors and demographics between groups to reduce baseline differences.
With the pragmatic method of subject recruitment, we contend that our outcome measure completion compliance rate cannot be compared with more traditional randomized controlled trials but should rather be contrasted with investigations of comparable studies in pragmatic/real-world environments. We retained 68% of the participants from baseline to post and 47% of the participants from baseline through to the 2-month follow-up, compared with an average retention rate of between 57% and 77% for other yoga or mindfulness retreat studies. 57,58 One reason for our slightly lower retention rates could be that frontline professionals are more prone to stress and compassion fatigue than the general population, which may have corresponded with a decreased likelihood of completing the later surveys. Indeed, we observed that participants who only completed the baseline survey reported higher levels of stress and negative affect than participants who also completed the other surveys.
There were some limitations of this study. First, the use of a waitlist control group is not as strong a comparison group as an active control condition that would control for time, effort, and attention. Future research could employ a control group that equates/matches for time, effort, and attention of the RISE program. Second, including a heterogeneous group of frontline professionals may have increased the variability in the data as opposed to using frontline professionals from the same organizational sector (e.g., education alone). We found some evidence of different baseline values across sectors; however, those differences were not statistically significant. Third, we did not employ imputation methods given that this is a pilot study with a small sample size; however, this may have biased the dataset. For example, participants who did not complete all measures reported higher baseline stress than those who completed all measures. Therefore, to address this limitation, future studies with larger sample sizes will employ intent-to-treat analyses. Fourth, there were significant relationships between expectation and changes in outcome measures, whereby the control group showed decreased positive affect with increased expectation, and the RISE group showed improved exhaustion with increased expectation. However, these relationships were not strong, and changes in exhaustion were not significantly different between groups. Therefore, improvements in outcome measures were unlikely to be due to changes in program expectation. Fifth, the demographics of this study are similar for individuals who typically practice yoga, that is, White, middle-aged women. Therefore, we have no information to understand whether the RISE program would be accessible to other demographics of frontline professionals. Future work would benefit from more diverse enrollment to increase the diversity of the study participants. Lastly, participants' home practice was not available, leaving us unable to assess variations in RISE practice outside of the program from the postassessment to the 2-month follow-up and uncertain how that practice may have influenced changes in outcome measures at the follow-up assessment. Approaches to collect frequency and duration of practice outside of the program will be implemented moving forward. Future studies will aim at evaluating changes in psychological and occupational health with a shorter 3-day RISE program, as well as comparing changes across occupational sector type. Investigations into cultural shifts in the workplace after RISE will also be explored.
Conclusion
The results of the current pragmatic controlled study indicate that the residential yoga-based RISE program improved psychological well-being in frontline professionals compared with waitlist controls. The practices and techniques learned at RISE continued to be used and integrated into participants' daily life and work and also shared with others, generating a multiplier effect. Workplace stress remains a growing concern for many organizations and effective, feasible programs that reduce employee stress and improve psychological health are needed to prevent workplace burnout and detrimental outcomes to health and well-being, as well as loss of productivity and absenteeism. The results from this study provide further compelling support that RISE is a feasible, effective program for improving the psychological well-being of frontline professionals. Future research is needed to confirm these results.
Footnotes
Acknowledgments
This work was supported by the Kripalu Center for Yoga & Health. The authors also gratefully acknowledge Jannelle Robinson for her contribution to this project. This research was funded by the Kripalu Center for Yoga & Health. The yoga program (RISE) being evaluated was developed by, funded, owned, and administered by Kripalu Center for Yoga & Health.
Authors' Contributions
N.L.T. recruited participants, collected and analyzed data, and wrote the article. M.M., S.B., and E.P. contributed to the conceptualization of the study, overseeing the delivery of the intervention, recruitment, and assisted with the article. J.A.D. supervised the overall project and provided statistical support and editing of the article. S.B.S.K. assisted in research design, supervision of study execution, IRB administration, data interpretation, and article preparation.
Author Disclosure Statement
N.L.T. is a paid postdoctoral consultant for Kripalu Center for Yoga & Health. M.M., S.B., E.P., and J.A.D. are or were employees of Kripalu Center for Yoga & Health. S.B.S.K. was funded by a research contract from the Kripalu Center for Yoga & Health to Brigham and Women's Hospital.