
Abstract
Objectives:
The main purpose of this study was to measure the effect of a single session of Reiki on physical and psychological health in a large nonclinical sample.
Design:
The study design was a single arm effectiveness trial with measures at pre-and postintervention.
Settings:
The study took place at private Reiki practices across the United States.
Subjects:
Reiki practitioners were recruited from an online mailing list to participate in the study with their Reiki clients. A total of 99 Reiki practitioners met the inclusion criteria and participated in the study. Reiki practitioners were instructed to give a flyer to each of their Reiki clients that contained information about the study and invited the client to complete a survey before and after their Reiki session.
Interventions:
Trained and certified Reiki Masters conducted the Reiki sessions in person, with each session lasting between 45 and 90 min.
Outcome measures:
The well-validated 20-item Positive and Negative Affect Schedule was used to assess affect, and brief, single-item self-report measures were used to assess a wide range of physical and psychological variables immediately before (pre) and after (post) the Reiki session.
Results:
A total of N = 1411 Reiki sessions were conducted and included in the analysis. Statistically significant improvements were observed for all outcome measures, including positive affect, negative affect, pain, drowsiness, tiredness, nausea, appetite, shortness of breath, anxiety, depression, and overall well-being (all p-values <0.001).
Conclusions:
The results from this large-scale multisite effectiveness trial suggest that a single session of Reiki improves multiple variables related to physical and psychological health.
Introduction
Reiki is a Japanese word that means spiritually guided life force energy. 1 It is a form of biofield therapy, which is based on the principle that fields of energy and information surround living systems and that these fields can be influenced by a practitioner to stimulate healing responses. 2 Most biofield therapies involve an energetic exchange between practitioner and client, which can be draining for the practitioner. Reiki is different in that the practitioner simply allows the Reiki energy to flow passively through their hands and into the client. 3 Reiki helps to restore the client's energies to a state of balance on the physical, emotional, and spiritual levels, thereby enhancing the client's natural ability to heal. 4
Over 800 hospitals (15%) in the United States currently offer Reiki to patients. 5 According to the latest information available, in a 2007 National Health Interview Survey, which included a comprehensive survey of Complementary and Alternative Medicine (CAM) use by Americans, more than 1.2 million adults and 161,000 children had used energy healing such as Reiki in the previous year. 6 Despite its widespread use, there is little research investigating Reiki's effectiveness in real-world settings, where Reiki often occurs. In particular, there has been no large-scale study examining how Reiki affects physical and psychological symptoms common to a variety of diseases and conditions, such as pain and anxiety in a general population sample.
Systematic reviews and meta-analyses of Reiki reveal that it has statistically significant improvements in many physical and psychological symptoms common to a wide range of diseases such as mood problems, anxiety, depression, fatigue, pain, and nausea. 7 –13 From 1989 to 2018, a total of 74 peer-reviewed research articles have been published on Reiki. Of the higher quality studies, those comparing Reiki to at least sham-Reiki or standard-of-care largely support the hypothesis that Reiki may reduce pain, anxiety, depression, and burnout and may increase relaxation and well-being.
A number of controlled experiments found Reiki to be more effective than sham Reiki. 12 Over the past 5 years, 31 peer-reviewed research articles have been published on Reiki. All but three of these were small-scale or pilot studies, and one of the larger scale studies was on hospitalized patients. 14 To date, there is yet to be a pragmatic effectiveness trial assessing individuals receiving Reiki in a nonclinical setting, despite this being where people often receive Reiki for managing their symptoms. Furthermore, Reiki provides immediate relief, whereby symptoms are commonly reduced during or immediately after the Reiki session. 14
The main purpose of the current study was to evaluate multiple measures of physical and psychological health using a single arm, pre–post design in a real-world, private practice setting. The secondary purpose was to assess the feasibility of conducting a large-scale multisite study remotely, including ease of recruitment, retention rate, and the clients' perception of data collection based on any informal qualitative feedback with the Reiki practitioners through e-mail. The authors investigated a range of indicators of physical and psychological health and well-being common to variety of illnesses and disease, such as affect, pain, tiredness, drowsiness, nausea, appetite, shortness of breath, depression, anxiety, and overall well-being. The authors hypothesized that a single Reiki session would significantly improve the majority of outcome measures, particularly pain, fatigue, depression, anxiety, and affect, and that it would be feasible to conduct a large scale multisite study remotely.
Materials and Methods
Participants
Reiki practitioners were recruited online through the Center for Reiki Research mailing list. An advertisement about the study was e-mailed to ∼5000 Reiki practitioners. Inclusion criteria for participating in the study as a Reiki practitioner were as follows: (a) being a certified licensed Reiki Master with the International Center for Reiki Training (ICRT) to ensure their commitment to the practice and that they abide by the ICRT's code of ethics, (b) having an active practice in the United States for at least 1 year in which clients are charged money for sessions, (c) providing at least two sessions per week that last 45–90 min, (d) Reiki must be the only modality they practiced in their sessions, and (e) having a computer available to the client that is Internet connected.
Of the 120 Reiki practitioners that expressed interest by the enrollment date, N = 99 Reiki practitioners met the inclusion criteria and participated in the study (83% of those interested). They were provided with an information sheet to give to their Reiki clients that described the purpose of the study and indicated that completion of the surveys indicated their consent to participate. There was no compensation for participating in the study for either the Reiki practitioners or clients. This study was approved by the [blinded] institutional review board.
Reiki as a practice
In a typical Reiki session, the client lies down on a massage table, bed, or sits comfortably in a chair. The client remains fully clothed and often has a blanket for extra comfort. A typical session lasts around 60 min whereby the Reiki practitioner places their hands above or gently resting on different locations on the client's body while they allow the energy to flow, which is often felt as heat, tingling, or other sensations. The number of hand positions depends on the Reiki tradition or needs of the client. Each position is held between 1 and 5 min or until the Reiki practitioner feels a sensation that the energy has stopped. Before and after the Reiki session, clients are often recommended to drink water to hydrate.
Study procedure
Interested Reiki practitioners were e-mailed a form by the researcher that provided information about their Reiki practice, including the number of years practicing Reiki, cost per Reiki session, average time of each Reiki session, and average number of Reiki sessions per week. They completed the form either electronically or handwritten and scanned and e-mailed the completed form back to the researcher. After being assessed as meeting inclusion criteria, they were e-mailed an information sheet for their clients and instructed through e-mail to hand it to their Reiki clients when they arrive for a session as usual. There were no exclusion criteria to participate as a Reiki client.
The information sheet invited the client to complete a survey before and after their Reiki session and included a link to the survey. They were provided information regarding the study; that it was voluntary and that not participating would not affect their relationship with their Reiki practitioner. Clients that agreed to take the survey completed an assessment immediately before the Reiki session (pre) and an assessment immediately following the Reiki session (post). Reiki clients completed the surveys online using Qualtrics survey software licensed to Harvard University. Each survey took ∼5 min to complete, totaling 10 min across both surveys. Informal e-mail communication between the Reiki practitioner and the researcher provided additional qualitative data on feasibility regarding any barriers to survey completion.
Physical and psychological health measures
Brief, unvalidated, self-report measures were included to assess a wide range of physical and psychological health symptoms in a short period of time immediately before (pre) and after (post) the Reiki session. Physical and psychological health-related measures included pain, tiredness, drowsiness, nausea, appetite, shortness of breath, depression, and anxiety, which were all assessed on a 10-point Likert scale ranging from 0 (No, e.g., pain) to 10 (Worst possible, e.g., pain). Overall well-being was assessed on a 10-point Likert scale ranging from 0 (No well-being) to 10 (Best possible well-being). The Positive and Negative Affect Schedule (PANAS) 15 was also used to assess changes in positive and negative affect. The PANAS is a well-validated and reliable (Cronbach alpha = 0.89) scale and is one of the most commonly used psychological measures to date. The 20 items (10 positive and 10 negative) are rated on a scale from 1 (Very slightly or not at all) to 5 (Extremely).
Reiki session characteristics
Reiki clients were asked to indicate their demographics, including their age, sex, ethnicity, and religious or spiritual belief, their reason for seeking the Reiki session, the support methods used (e.g., massage table and chair), the location of the session, and if they were taking medication for their symptoms.
Data analysis
Descriptive statistics, including frequencies, means, and standard deviations, were computed for the Reiki practitioner and Reiki session characteristics. Changes in Reiki clients' physical and psychological health measures from pre to post session were analyzed using paired samples t tests. Analyses of variance were used to compare characteristics of the Reiki session to changes in physical and psychological health variables. Missing data within the surveys were dealt with through mean replacement if 10% or less of the data were missing. If more than 10% of the data were missing, the survey was excluded from the analysis. Significance was set to p < 0.005 because of the large sample size and multiple comparisons. Data were analyzed using IBM SPSS statistical software version 22.0 (Geneva, Switzerland).
Results
Reiki practitioner characteristics
The characteristics of the Reiki practitioners' (N = 99) practice are displayed in Table 1, including average number of Reiki sessions per week, average length of Reiki session, cost per Reiki session, and the number of years practicing Reiki. Common reasons for seeking the Reiki session included relaxation, anxiety, pain, stress, cancer, overall well-being, spiritual growth, emotional healing, fatigue, general interest or curiosity, and peace.
Characteristics of the Reiki Practitioners' Practice
N = 99.
Reiki session characteristics
Over a period of 1 year beginning in May 2015, 1575 Reiki sessions were recorded, with 164 missing postsurvey responses, yielding a total of N = 1411 Reiki sessions included in the final analysis (90% of initial sample). Informal qualitative feedback through e-mail with Reiki practitioners indicated that some of the reasons why clients did not complete the surveys included the client not wanting to disrupt the positive feeling following the Reiki session, issues with the Internet or computer, and older clients having difficulty or being frustrated with the computer. There were no significant differences in presurvey scores between participants that completed both the pre- and postmeasures and those who did not complete the postmeasures (all p-values >0.05). The mean age of the Reiki clients was 49.0 years (range 18–89), 1143 (81%) were female, 246 (18%) were male, and 14 (1%) identified as other. With respect to race/ethnicity, 83% identified as Caucasian, 7% Hispanic, 2% African American, 1.9% Asian American, and 6% as other. With respect to religion and spirituality, 49% reported that they were Christian, 33% spiritual but not religious, 3% Buddhist, 2% Hindu, 1% atheist, and 11% other.
The characteristics of the Reiki sessions are displayed in Table 2, including the support method, location of the session, and whether they took medication for their symptoms.
Characteristics of the Reiki Sessions
N = 1141 Reiki sessions.
Improvements in physical and psychological health
At post, there was a significant improvement in pain, t(1401) = −33.62, p < 0.001, d = 0.90, 95% confidence interval (CI) [−1.90 to −1.69]; tiredness, t(1400) = −38.82, p < 0.001, d = 1.01, 95% CI [−2.76 to −2.49]; drowsiness, t(1396) = −22.32, p < 0.001, d = 0.60, 95% CI [−1.78 to −1.49]; nausea, t(1399) = −11.20, p < 0.001, d = 0.30, 95% CI [−0.55 to −0.39]; appetite, t(1392) = −11.94, p < 0.001, d = 0.32, 95% CI [−0.70 to −0.50]; shortness of breath, t(1397) = −16.13, p < 0.001, d = 0.43, 95% CI [−0.82 to −0.65]; depression, t(1396) = −28.50, p < 0.001, d = 0.76, 95% CI [−1.77 to −1.54]; and anxiety, t(1395) = −37.91, p < 0.001, d = 1.00, 95% CI [−2.69 to −2.43] (Fig. 1). Overall reported well-being also improved following the Reiki session, t(1379) = −23.94, p < 0.001, d = 0.64, 95% CI [−2.04 to −1.73] (Fig. 2). At post, both positive affect and negative affect significantly increased, t(1400) = 19.88, p < 0.001, d = 0.53, 95% CI [3.52 to 4.29] and t(1400) = −32.18, p < 0.001, d = 0.86, 95% CI [−5.89 to −5.21], respectively (Fig. 3). Table 3 displays the individual item-by-item changes for the PANAS. All positive affect and negative affect items showed significant improvements following the Reiki session, all p-values <0.001.
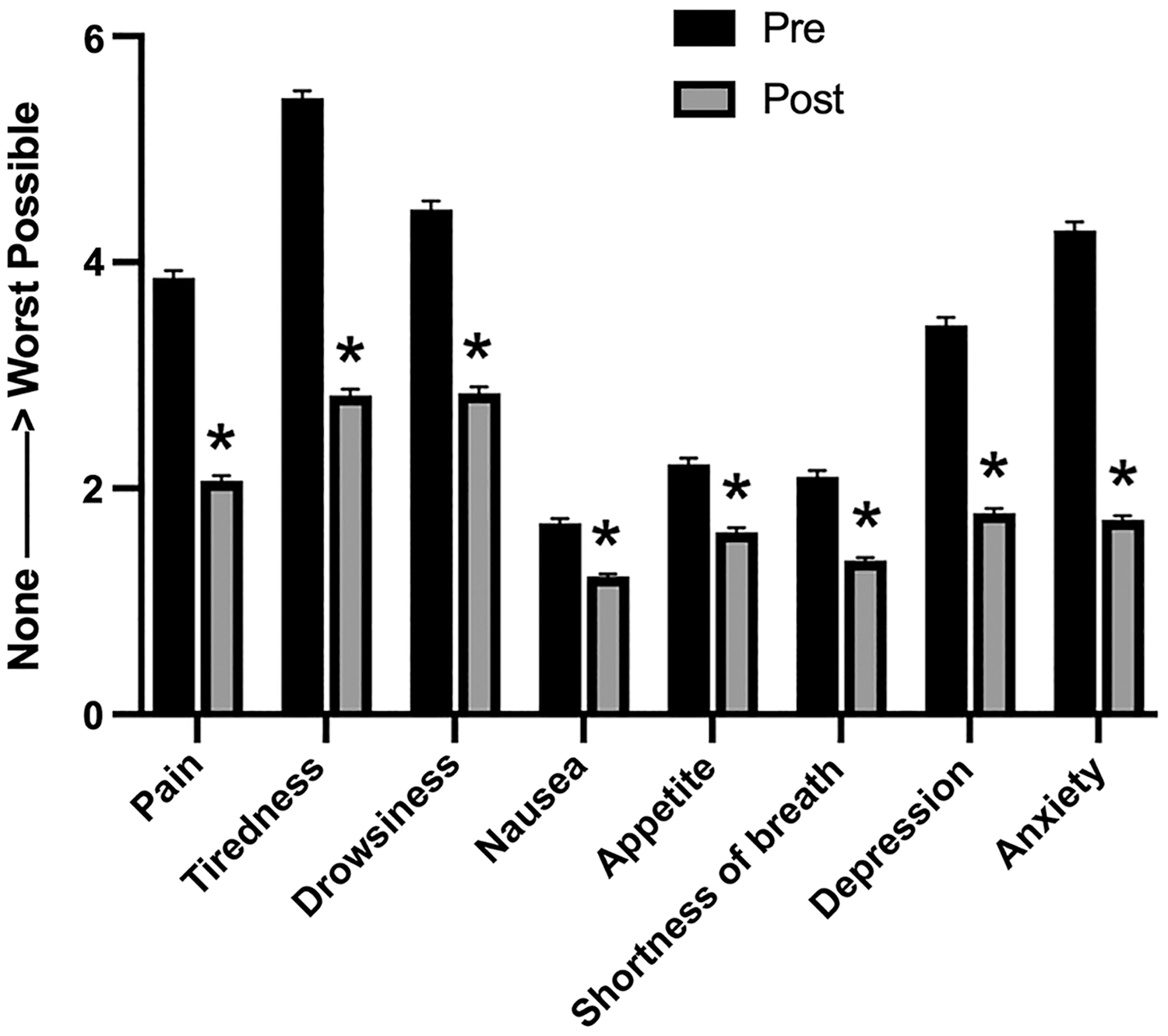
Reiki clients' mean scores on physical and psychological health variables before (pre) and after (post) the Reiki session. Error bars represent the standard error of the mean. *p < 0.001.
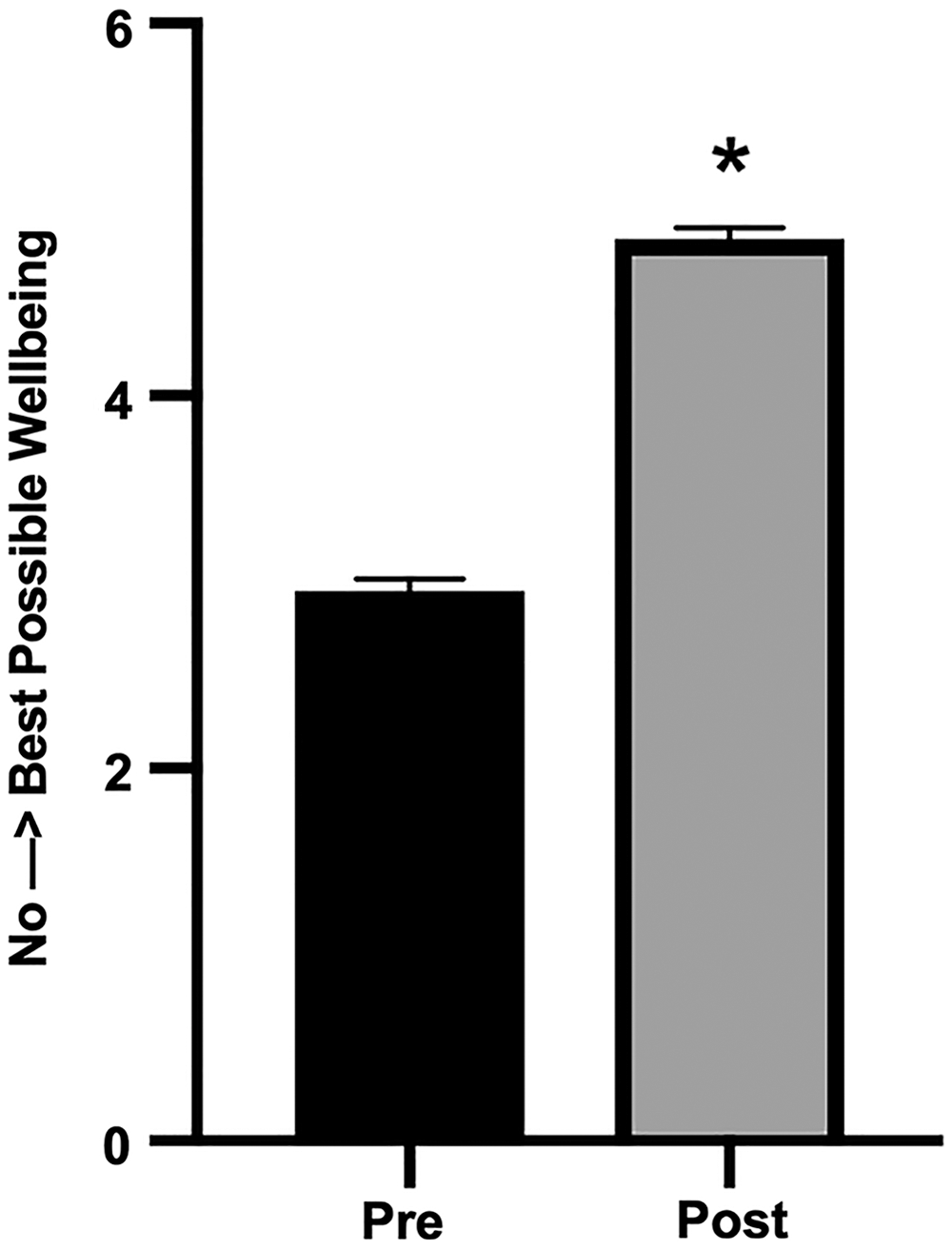
Reiki clients' mean scores on overall well-being before (pre) and after (post) the Reiki session. Error bars represent the standard error of the mean. *p < 0.001.
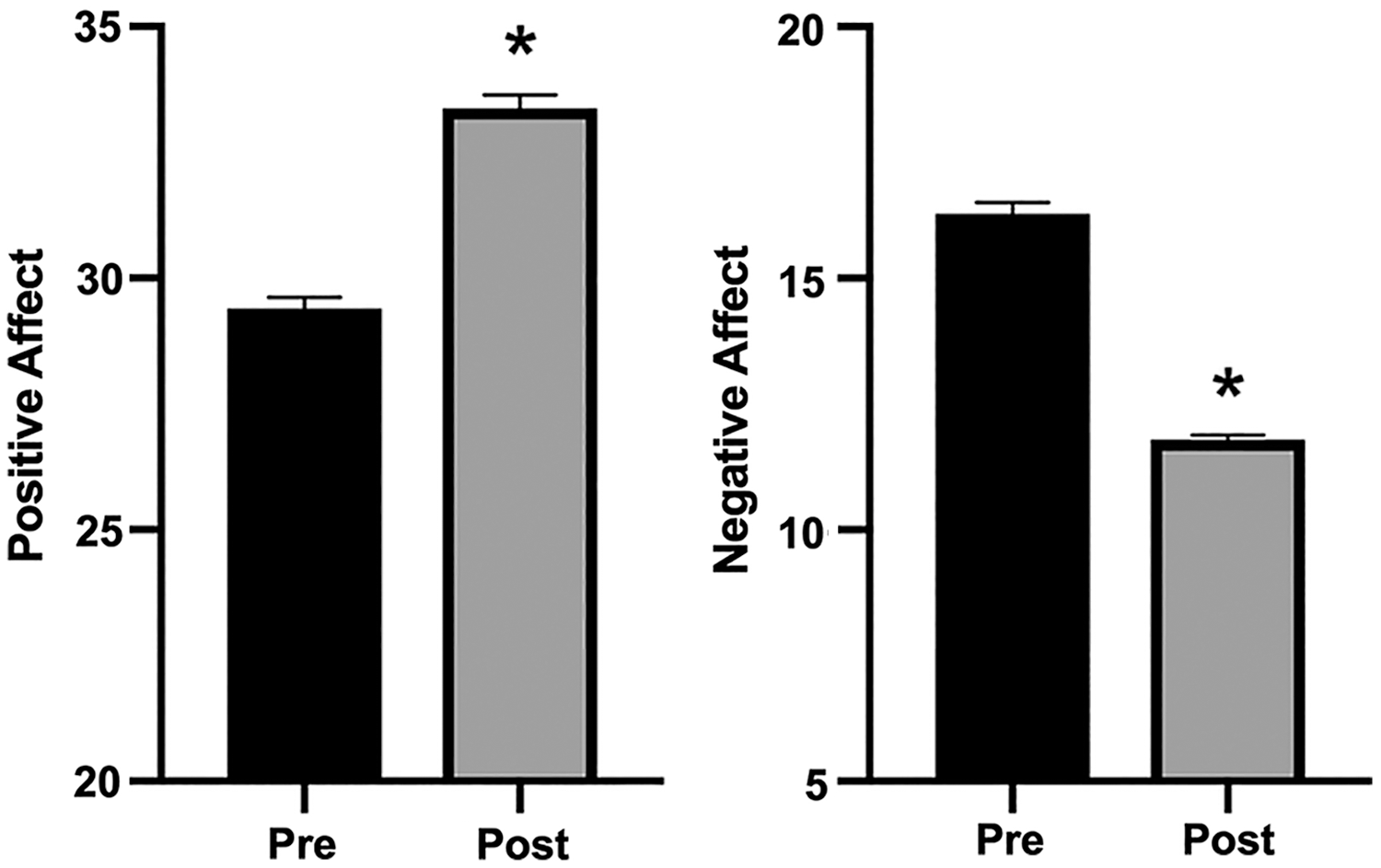
Reiki clients' mean positive affect and negative affect scores on the PANAS before (pre) and after (post) the Reiki session. Error bars represent the standard error of the mean. *p < 0.001. PANAS, positive and negative affect schedule.
Mean Scores and Standard Deviations and Statistics for Each Positive and Negative Affect Schedule Item at Pre and Post Reiki Session
Data were analyzed by paired samples t tests. All p-values <0.001.
CI, confidence interval; PANAS, positive and negative affect schedule; SD, standard deviation.
Pearson correlations between change scores (post–pre) for all physical and psychological health variables are displayed in Table 4. Change scores for all physical and psychological health measures were significantly correlated with each other, all p-values <0.001.
Correlations Between Change Scores (Post–Pre) for All Physical and psychological Health Variables
All p-values <0.001.
Anx, anxiety; App, appetite; Breath, shortness of breath; Dep, depression; Drow, drowsiness; NA, negative affect; PA, positive affect; Tired, tiredness; Well, well-being.
Discussion
This large-scale study was a real-world effectiveness trial of the effect of Reiki on common physical and psychological symptoms in a nonclinical population. Given the preliminary nature of Reiki research, and its widespread use in health care and private practice settings, large-scale effectiveness trials are an important first step toward conducting more rigorous controlled trials. As was hypothesized, a single session of Reiki improved physical and psychological health variables. The authors also observed correlations between changes in all outcome measures. With respect to their secondary aim, the study was feasible to conduct, with ease of recruitment and a high retention rate. However, there were some indicators for study improvement that will be discussed below.
The population used for this study allowed for an assessment of a large number of clients that typically seek Reiki for acute symptom management outside of the hospital setting. The Reiki clients were typical of populations reported to seek CAM, mostly white middle-aged females. 6 Therefore, a strength of the study is the generalizability of the results to a broad population, whereas most Reiki research has been with specific clinical populations. Most Reiki clients also reported a spiritual or religious belief system, with only 1% reporting that they were atheist. The authors found that 36% of Reiki clients reported taking medications for the symptoms they were managing with Reiki.
The study was found to be feasible, with participant recruitment not posing any challenges, as 83% of the interested Reiki practitioners met the inclusion criteria. Furthermore, the retention rate for completion of the postsurvey was high at 90%. Informal qualitative feedback on survey incompletion suggests that future studies would benefit from providing paper options for Reiki clients less comfortable with filling out the survey on a computer. Further qualitative data regarding why the clients were seeking a Reiki session and their experience during the session will be reported elsewhere.
The current results point to the therapeutic potential of Reiki for a variety of conditions that correspond with multiple physical and psychological health symptoms. The results of the current study show that individuals are receiving immediate benefits for their symptoms from receiving Reiki in practitioners' home and wellness centers. Most improvements in physical and psychological health showed medium-to-high effect sizes. The authors observed the highest effect sizes (Cohen's d) for improvements in tiredness (1.04), anxiety (1.01), pain (0.90), negative affect (0.86), and depression (0.76). Therefore, individuals with health concerns corresponding with the aforementioned symptoms may show the most promise for treating with Reiki. Indeed, the results of this nonclinical real-world study are consistent with small sample clinical trials in which Reiki was associated with improvements in well-being 16 –21 and alleviation of pain, 3,22 –24 emotional stress, 25 –28 anxiety, 21,23,26,28 and depression. 25,29 Positive affect was below norm levels at pre and increased to norm levels at post, whereas negative affect was at norm and decreased to below norm levels following Reiki. Therefore, a single session of Reiki can provide immediate benefits to affect, and multiple studies have reported affect to be a key factor in physical and psychological health, through pathways such as promotion of healthy behaviors, improved immune system function, and increased social support to name a few. 30,31
Although not addressed in the current study, a common criticism of Reiki is that its beneficial effects are due to a placebo response. However, experiments with sham Reiki active controls, in which a person untrained in Reiki uses the same hand positions as a Reiki practitioner on client or patient, also have a therapeutic effect, such as reducing self-reported anxiety. 4,12,32 Although sham Reiki has some therapeutic benefits, Reiki appears to be more effective than sham Reiki based on current pilot studies, 10,25,26,33 –36 although one study reported no difference between sham Reiki and Reiki for treating fibromyalgia. 37 It is difficult to study the placebo response in a population who is paying Reiki practitioners to provide them with Reiki. However, one solution would be to pay Reiki practitioners through research funding to give Reiki sessions for free to a group of clients knowingly recruited for research. Half of those clients could be randomly selected as the control group and would be met by a colleague of the practitioner untrained in Reiki but with knowledge of the hand positions, to act as a sham provider.
The current study had several limitations that warrant discussion. First, this was a pragmatic effectiveness trial assessing the effect of Reiki in clients that were already seeking Reiki, increasing the likelihood of expectation effects. Future work will take this into account by including measures of clients' expectation. Second, while the authors understand the limitation of no control group, the study design was a pragmatic approach, a useful methodology for assessing the impact of outcomes in a real-world scenario. Therefore, the authors would like to suggest that the real-world generalizability of these results is a strength of the current study. This pragmatic approach has recently been championed by National Center for Complementary and Integrative Medicine (NCCIH), which has been making great efforts to foster and support real-world research and implementation science. 38,39
Third, there was a lack of standardization across Reiki sessions in terms of style of Reiki and length of session. To attempt to account for this, Reiki practitioners were required to be certified, licensed Reiki Masters with the ICRT, practicing for at least 1 year, the session had to be between 45 and 90 min, and they could offer only Reiki during the session (e.g., no other CAM modalities). Fourth, with the exception of the PANAS, all measures were single-item scales, which tend to have lower validity and reliability than multi-item scales. However, the goal was to efficiently measure as many physical and psychological variables as possible in under 5 min. Future work will use validated multi-item scales to assess changes in variables that showed the largest effect sizes; anxiety, tiredness/fatigue, pain, depression, and overall well-being.
Fifth, the majority of the Reiki clients were middle-aged Caucasian women who identified as Christian or spiritual; therefore, the ability to generalize these results to other demographics or belief systems is limited. A sixth limitation is that the authors were unable to pair the Reiki practitioners and their clients due to the clients' inaccurate reporting of the identification numbers in the survey. The authors also did not assess whether the clients had been to the practitioner before in the past. Therefore, future work will aim to pair practitioners and their clients through automated electronic means and also measure whether the client had been to the practitioner before, and how frequently. Finally, since the clients were paying for the service, they likely have high expectations for the benefits of the Reiki session. A future study in which the clients do not pay for the Reiki sessions could be compared with the present study to determine the effect of “fee for service” on the results.
In conclusion, Reiki acutely improved physical and psychological symptoms associated with many health conditions, including affect, pain, depression, anxiety, tiredness, drowsiness, nausea, shortness of breath, appetite, and overall well-being. Reiki can provide immediate relief for many health conditions and is used for this purpose inside and outside of the hospital setting. This multisite real-world effectiveness trial was feasible to conduct and provided important preliminary data on the effectiveness of a single session of Reiki to improve physical and psychological symptoms. These results are highly preliminary and should be interpreted as such. More research needs to be conducted to confirm or refute these findings. Therefore, the results from this study will be used to conduct a future multisite trial using a control group, such as massage therapy, in a real-world setting. Future research will also prioritize investigation of symptoms that showed the largest effect sizes, as well as inclusion of follow-up assessments. In addition, the progress of clients will be followed over multiple Reiki sessions to evaluate changes over a longer time frame.
Footnotes
Acknowledgments
The authors thank the International Center for Reiki Training for their support of this research and Corey Bippes for his assistance with the study.
Author Disclosure Statement
N.L.T. received funding from the International Center for Reiki Training to conduct this study. This research did not receive any additional grants from funding agencies in the public, commercial, or not-for-profit sectors. There are no other disclosures.
Funding Information
No additional funding was received for this article.