
Abstract
Objectives:
In the fall of 2017, Fresh and Savory, a Culinary and Lifestyle Medicine Teaching Kitchen (TK) program proved systematically feasible as a Shared Medical Appointment (SMA). A portable TK complemented physician consultations, interactive didactic presentations, nutritious cooking, and mind–body exercises. A series of SMAs were launched to develop a system for physicians to address patients' nutritional and lifestyle needs.
Interventions:
MedStar Health implemented three TK SMA programs to improve patients culinary and lifestyle skills and improve relevant habits. Two cohorts were recruited from Internal Medicine and Cardiology (Internal Medicine/Cardiology I and II) and completed an 8-week program leveraging a culinary and lifestyle medicine curriculum. One cohort (Sports Performance) was held with young, elite athletes completing a 4-week program regarding athlete's nutrition and lifestyle. Feasibility was assessed through patient surveys, staff program operation assessments, and reimbursement.
Results:
Fifty-three unique patients attended SMA programs, 4–18 patients per weekly session; 223 appointments billed in 2018. E&M code 99213 was billed at $157 and reimbursed, on average, at $116 per patient encounter. During a 4- to 8-week SMA program, changes in patient vitals were statistically insignificant, yet habit changes showed clinical significance. Patients noted increased knowledge of plant-based meals, importance of sleep, and adding mindfulness and exercise to their weekly routine.
Conclusions:
This exploration investigated the feasibility to implement TK SMA programs at MedStar Health. Developing financial and operational infrastructure for TK SMAs requires financial, staffing, location, and population considerations. TK SMAs proved patient demand for opportunities to develop healthy behaviors. However, sufficient time is required to recruit patients. Vital signs may not acutely improve over an 8-week period, however, small habit changes may improve health outcomes longitudinally and additional exploration is required to assess longitudinal patient outcomes. Financially, SMAs suggest a sustainable and effective approach to integrative medicine in health care.
Introduction
Of the 300
Forty-five percent of cardiometabolic deaths are associated with poor diet choices. 2 Meals eaten outside of the home are most common sources of processed foods such as processed meats, refined grains, and sugar-sweetened beverages. Eating meals prepared at home is negatively associated with weight gain and risk of associated diseases, such as type 2 diabetes. 3 Lifestyle changes, including healthy diet, exercise, stress management, and community support can reverse coronary artery disease. 4 Despite the research supporting lifestyle modifications as a recommended treatment for cardiovascular disease (CVD), physicians do not counsel patients in adopting lifestyle treatments as often as expected. 5 Primary care physicians (PCP) have a growing number of patients with chronic conditions and increased complexity. 6 PCPs commonly see patients for symptoms related to and management of chronic illnesses, such as CVD, diabetes, and metabolic syndrome, all of which can be treated with healthy lifestyle improvements. 7
In 2017, MedStar Health, the largest health care system in the Washington D.C. and Maryland area, implemented a pilot Culinary and Lifestyle Medicine program, Fresh and Savory. This 8-week program was modeled as a Shared Medical Appointment (SMA), a medical appointment where patients learn about and discuss health in a group. The program taught patients evidence-based lifestyle skills to reduce primary and secondary CVD risk. Curriculum included didactic presentations by experts and experiential hands-on learning through a teaching kitchen (TK), a learning laboratory in which patients learn life skills, such as cooking, exercise, and mindfulness. 8
In 2018, the program opened recruitment to patients in internal medicine. Subsequently, a similar 4-week program was developed for elite athletes. The current investigation assesses the feasibility of implementing Fresh and Savory, a hands-on TK modeled as a SMA, at MedStar Health.
Shared Medical Appointments
SMAs are patient visits where a clinician consults with patients in a group setting. Our model combines a well-known SMA structure developed by Ed Noffsinger, Cooperative Health Care Clinics (CHCC) 9,10 with a TK. In each of our programs, the same unique group of patients attend weekly sessions incorporating health education didactic presentations with nutritious hands-on cooking and demonstrations.
SMAs can improve provider productivity, increase quality of and access to care, enhance chronic disease management, and potentially reduce provider burnout. 11 Studies have shown positive outcomes associated with SMAs, including reducing emergency room visits and readmissions, improving quality of life for patients with migraines, increasing patient trust, and improving eating habits associated with lowering biomarkers associated with chronic illnesses. 12 –17
Program overview
Fresh and Savory's primary goal was to equip patients with culinary and lifestyle skills to enhance relevant lifestyle behaviors. To address the difficulty patients experience when making lifestyle habit changes, the program offered an experiential learning approach to diet and lifestyle. The design incorporated a portable TK with didactic curriculum taught by experts. Our curriculum covered the five pillars of well-being—nutritious cooking, physical activity, relaxation techniques, sleep, and connectedness. Qualitative feedback from patients and consistent evaluation of program operations, addressed real-time program improvements. As quality improvement research, we assessed the feasibility of SMAs utilizing TKs within MedStar Health.
Materials and Methods
Our process of developing and implementing SMAs was cyclical (Fig. 1). Pilot programs informed program operations and logistics such as time, preparation, and quality and availability of equipment. Patients provided qualitative feedback on enjoyment of recipes and activities. Recruitment methods and confirming interested patients were then established. Administrative tasks (i.e., budgeting, ordering supplies, and planning schedules) were completed 4 weeks before beginning. SMA sessions followed the program designs detailed below. After each session, the team evaluated what went well and what did not, and each week, administrative tasks were completed. At each programs' conclusion, feedback was analyzed to reflect further improvements.
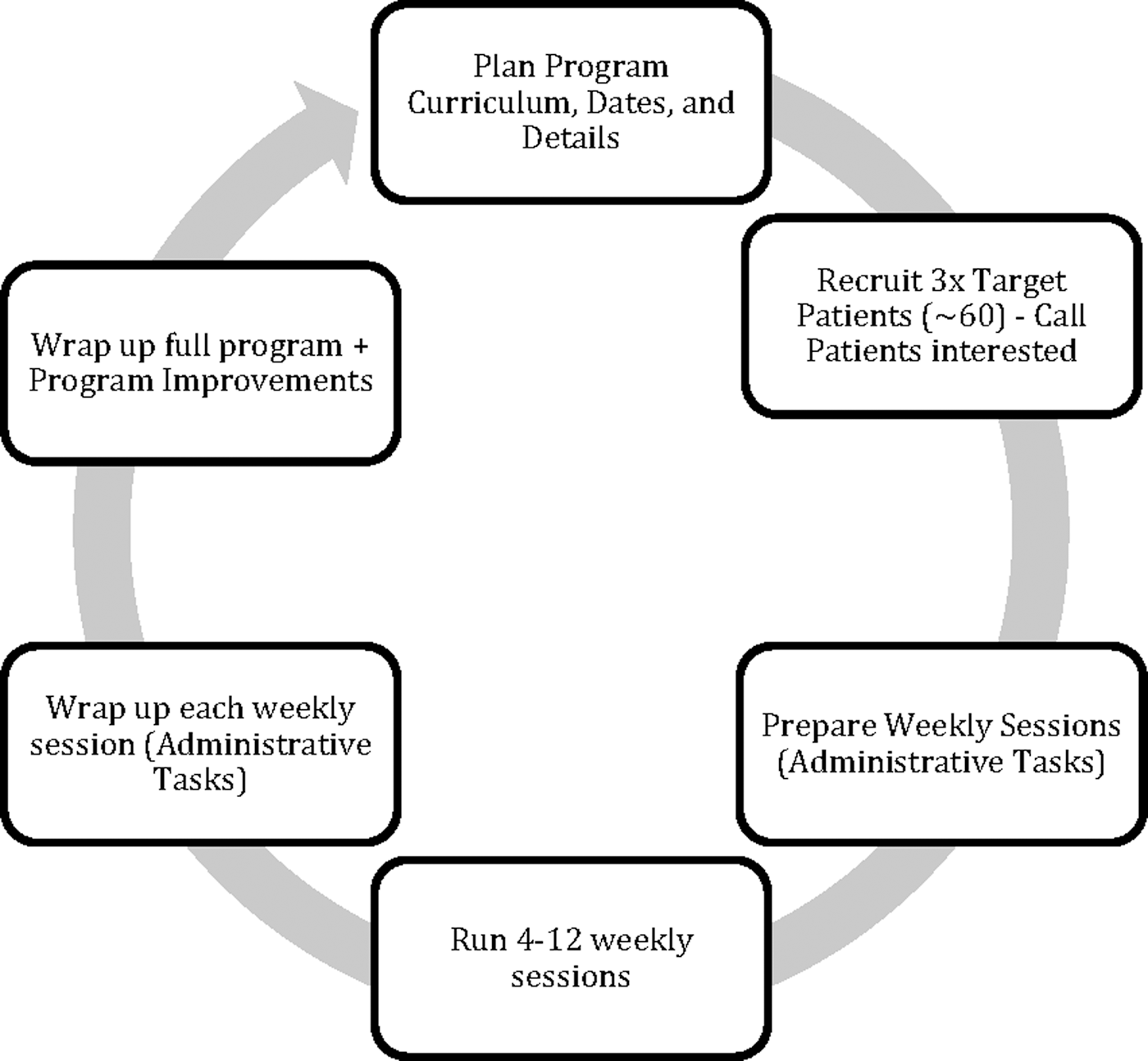
Process of running and assessing SMA Programs. SMA, Shared Medical Appointment.
Recruitment
During 2018, three patient cohorts completed the Fresh and Savory program. Thirty to 50 patients were recruited for Internal Medicine/Cardiology I and II on an ongoing basis. Physicians in Internal Medicine and Cardiology Associates at MedStar Lafayette Center (MLC), an ambulatory site in downtown Washington, D.C., recruited patients. Thirteen existing athletes in the sports performance training program at MLC, were recruited for Sports Performance. Recruitment materials included program fliers passed out by doctors and clinic staff (all), a local news segment (Internal Medicine/Cardiology II), and invitation by Blue Cross Patient-Centered Medical Home (Internal Medicine/Cardiology II). Program staff called interested patients to answer questions and confirm attendance (Internal Medicine/Cardiology I and II). Patients received weekly text appointment reminders and weekly emails with resources and reminders (Internal Medicine/Cardiology I and II).
Program Design for Internal Medicine/Cardiology I and II included eight, 2-h sessions consisting of 5–10-min mind–body exercise, and 40 min of both didactic presentations and hands-on activities. Mind–body exercises, such as mindful breathing and guided imagery, opened each session. Didactic presentations discussed the five pillars of health: nutritious cooking; sleep; exercise; relaxation; and community. Table 1 is an example lecture schedule for both Internal Medicine/Cardiology cohorts I and II. Topics remained consistent but were reorganized regarding speaker availability. Culinary skills and recipes, examples in Table 2, were introduced through hands-on cooking and demonstrations of plant-based meals utilizing modular cooking stations.
Example Lecture Schedule for Internal Medicine/Cardiology I and II
CVD, cardiovascular disease.
Skill Building and Recipes Included in Program Design
Program Design for Sports Performance included four, 2-h sessions following a similar format as Internal Medicine/Cardiology. Didactic presentations were relevant to elite athletes, including injury prevention and sports nutrition (Table 3). Skill building and recipes included making smoothies and energy bites, choosing healthy meals on the go, and mental imagery to improve performance (Table 2).
Lecture Schedule for Sports Performance
Data collection
Changes to data collection methods were adjusted to test different methods of capturing data considering patients' time, program workflow, and desired information; Table 4 outlines the methods used.
Data Collection Methods for Each Shared Medical Appointment Program
Vitals, taken by a Medical Assistant each week, included blood pressure, weight, and heart rate.
Individual patient consultations were completed throughout the 2-h session. The physician talked with each patient in the room discussing patient's goals, progress, medications, and other medically relevant information. A problem-focused history, brief physical exam, and assessment and plan were documented in patients' charts.
Electronic surveys
Internal Medicine/Cardiology I patients were emailed electronic surveys through Tonic for Health, an online patient-facing data collection platform. The surveys inquired about lifestyle behaviors over the past month at baseline and 7 days each week. Questions included habits of sleep, exercise, healthy eating and cooking, connectivity, and stress perception chosen from validated supplementary questionnaires with adjustments for desired time frame. 18,19
“Passports”
Sports Performance and Internal Medicine/Cardiology II filled out paper booklets, (“Passports”) each week recording their goals, program feedback, and lecture notes. The questions, not validated, included “What is your goal for this week?,” “What inspired you this week?,” “What confused you this week?,” the goal being to prompt feedback. Patients also recorded SMART goals for the program overall and each week and could record associated habits.
Billing
Each patient was billed under level 3 E&M code 99213. Patients paid for appointments through insurance or self-payment. Insurance coverage included Medicare plans and private insurance. Reimbursement per patient encounter was compiled by the billing specialist.
Team Evaluations reviewed qualitative successes and improvements according to staff. “Glows and Grows” were discussions to acknowledge what was going well with the program, “Glows,” and what could be improved, “Grows.” The Internal Medicine/Cardiology cohorts used an electronic Google Form to gather quantitative and qualitative data for each session.
Statistical analysis
Mean and standard deviations were calculated for blood pressure, heart rate, and weight for the Internal Medicine and Cardiology I cohort. We used a mixed-effects model using a random intercepts model combined with time, in weeks, as a fixed effect for each. The change was observed over a period of 8 weeks. Data were recorded when patients attended the SMA.
Qualitative feedback collected from patient Passports were tagged by category and week. Patients' SMART goals were used as a tool for motivational interviewing related to their medical status and content learned during the program.
Results
Three TK SMAs were successfully implemented with real-time improvements. Robust attendance for the two Internal Medicine/Cardiology cohorts proved feasibility and demand among this patient population. However, attendance for the Sports Performance program suggested recruitment processes need to be improved and other considerations for this population need to be addressed.
Patient demographics
Presented in Table 5, the Internal Medicine/Cardiology I and II had an older population at an average age of 64.47 and 62.83, respectively; both programs were primarily female and African American. Sports Performance had a younger population at an average age of 22.73, majority male, and Caucasian.
Patient Demographics per Program Cohort at MedStar Lafayette Center
Attendance feasibility
The financial assessment of our pilot program revealed at least 12 patients, on average, needed to attend weekly sessions to match direct program costs. During 2018, the three programs seen had 223 patient encounters over 20 weeks; on average, 11 patients per week. Both Internal Medicine/Cardiology programs had an average of 12.875 and 11.88 patients, respectively, attend weekly sessions. Sports Performance had limited average patient attendance of 6 (Table 6). Figure 2 exemplifies the consistency of attendance at each program. Drop-out and nonattendance included patients with other medical concerns, family or work obligations, and travel.

Recruiting adequate patients created a consistent core group of participants near target of 12 patients.
Weekly Attendance by Cohort and Total Patient Encounters
Patient reimbursement
A PCP conducted the SMAs at MedStar Health and billed a 99213 level 3 E&M code. In 2018, appointments were charged at a rate of $157 and earned 0.97 relative value units (RVU).
Assessed by week, Table 7 compares the total reimbursement between programs, including the first pilot to exemplify the growth of the program and the necessity of sufficient patient encounters. On average, Medicare plans reimbursed $74 and $83 and private insurers reimbursed $134 and $131 in Internal Medicine/Cardiology cohorts I and II, respectively. The Sports Performance cohort, a younger population, had no Medicare patients; private payers reimbursed $140 on average; and self-pay was charged $157 (Table 8). In the Sports Performance cohort, one patient paid out of pocket. Coverage varied between plans. In total, $27,513 was reimbursed for three cohorts at MLC. The amount earned per week and per program was directly related to the patient attendance (Fig. 3).
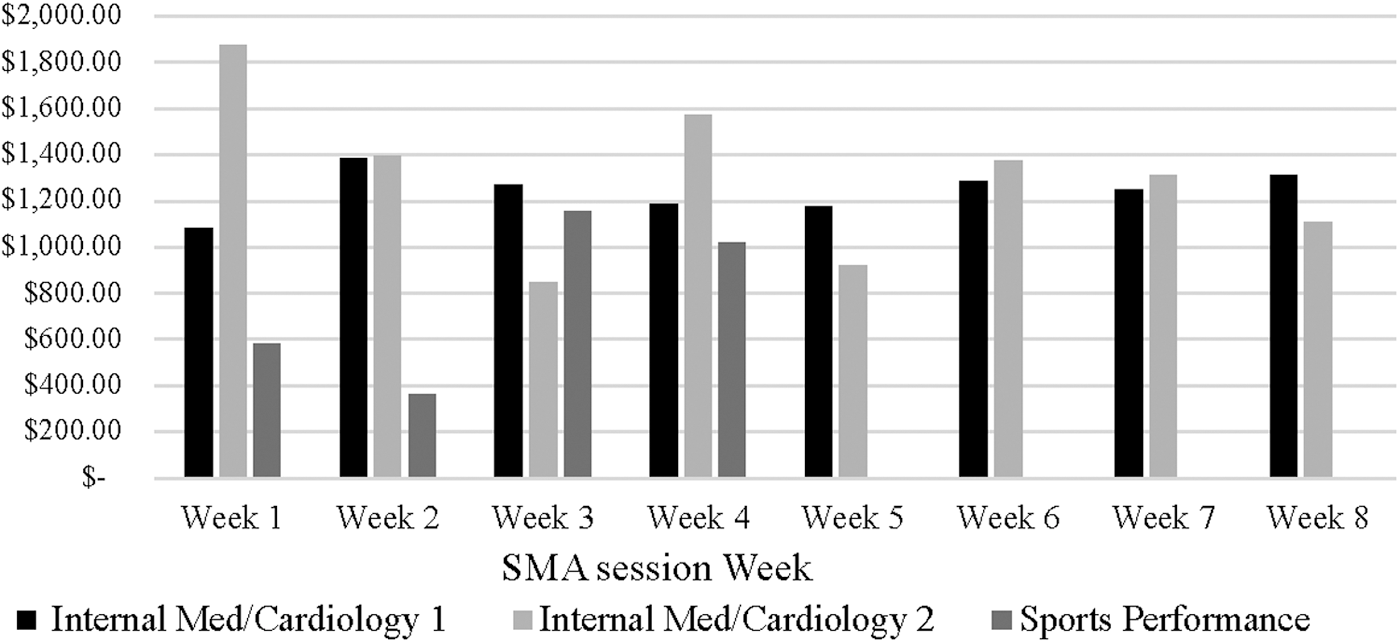
All three programs at MLC in 2018 earned $27,513. MLC, MedStar Lafayette Center.
Weekly Program Reimbursement by Cohort
Distribution of Insurance Medicare Versus Private Payer
Relative value units
In total, all programs earned the lead provider 213.4 RVUs for 223 appointments.
Program equipment costs
Original start-up costs for our portable TK was designed for 8–10 people. “Start-up” materials are the costs of equipment and supplies expected to only be purchased once to start a program and for periodic improvements or expansion. Staff salaries and operation costs were considered separately. Additional supplies were purchased in 2018 to accommodate more people and purchase higher quality supplies. Altogether, about $5,520 was spent on Start-up Equipment, while total program income was $27,513 over three cohorts (Table 9).
Program Costs by Cohort and Total
Statistical significance
Only a fraction of the patients answered the quantitative habit change surveys collected online through Tonic for Health in the Internal Medicine/Cardiology I cohort (Tables 10 and 11). Patient vitals in the Internal Medicine/Cardiology I cohort (blood pressure, heart rate, and weight) slightly decreased over the 8 weeks, however, change was not statistically significant (Table 12). Repeat blood pressure was obtained after a brief resting period for patients with high initial blood pressure readings. High readings were attributed to rushing, traffic, work, and stress.
Baseline Healthy Habits Quantitative Results for Internal Medicine/Cardiology I
Frequency scale: 1 = less than once a month, 2 = once a month, 3 = a few times a month, 4 = about once a week, 5 = a few times a week, 6 = daily.
Weekly Quantitative Follow-Up Questions for Patients in Internal Medicine/Cardiology I
Agreement scale: 1 = strongly disagree, 2 = disagree, 3 = somewhat disagree, 4 = neither agree nor disagree, 5 = somewhat agree, 6 = agree, 7 = strongly disagree.
Self-rating ranges from 1 to 106.
Vitals at Each Weekly Shared Medical Appointment Session
One patient had two completely different sets of vitals because they attended the group on the same day they had an office clinic appointment.
One patient had their heart rate and weight measured at different time points.
Suggested behavior changes
Although quantitatively patients did not change their habits or vitals significantly, patients expressed anecdotal evidence of lifestyle behavior changes according to Passports and one-on-one visits. Patients indicated increased sleep and culinary confidence, and reduced stress as well as medication dosage. Patients qualitatively expressed they were enjoying the program and continued interaction with the staff through email, such as sending photos of healthy recipes made at home. Past participants returned to participate, volunteer, and share their lifestyle changes.
Popular quinoa and chickpea dishes were replicated by participants to share with friends and family. Participants from Sports Performance reported continued use of mindfulness visualization techniques performance, healthier snack choices while traveling, and replacing fast food with plant-based meals made at home as indicated during training sessions post-SMA. Patient comments included: “I was surprised that eating healthy can taste so good”; “I now eat and cater delicious healthier lunch options to my clients”; “This program was the jumpstart I needed to live a healthier life without sacrificing my love for cooking and eating.”
Patient qualitative data
Ten of the 21 patients in the Internal Medicine/Cardiology cohort II recorded SMART (Specific, Measurable, Achievable, Realistic, Timely) goals in the Passport documents. The Passports prompted patients to acknowledge why this goal was important to them. Patient goals included creating a daily practice utilizing relaxation techniques, cooking plant-based meals twice weekly, and increasing sleep from 4 to 7 h at least three nights per week. Goals were addressed by the provider in one-on-one visits through motivational interviewing. For example, the patient whose goal was to increase sleep, the provider helped them to make an actionable plan of bed time 20 min earlier 3 days a week. Obstacles identified during their visit were stress associated with a new job search.
In the patients' Passport they had the option to log weekly habits associated with their SMART goals, however, only eight filled it in at baseline and two to seven patients each week. Of those that tracked their weekly habits in their Passport booklet, the habits were often associated with their goal. For example, if the goal was to drink more water, patients tracked their water intake that week. If their goal was to add more weight training to their exercise routine, they tracked what type of exercise they performed that week.
Discussion
Attendance for both Internal Medicine/Cardiology cohorts demonstrated that with effective time, planning, and a wide pool of patients to recruitment from, a TK SMA is feasible. A total of $27,513 was earned between three SMA programs of 223 patient encounters. Recruiting at least three times as many patients desired to attend each session was important to attain adequate and consistent participation in each session. With a recruitment pool of only 13 patients, pilot program attendance for the Sports Performance cohort exemplified the importance of recruiting early and three times more than the amount of recommended patients. Qualitative data collected exemplifies promise for influencing patients' habit changes and potentially significant clinical outcomes. A longitudinal study of patient outcomes is needed to understand the effect of the program beyond 4 to 8 weeks.
Reimbursement
After analysis of the business plan, including operating costs, start-up costs, reimbursement, and other fees, the attendance to reach the break-even point, where the direct program costs equal the revenue from the program, was 12 patients per week, for an 8-week program, totaling 96 patient encounters. However, additional factors affect reimbursement potential, including payer mix (i.e., Medicare vs. private payers) and lead physician-to-patient ratio (i.e., maximum number of patients a physician can reasonably see and bill during the program). Additionally, reimbursement may vary by year, hospital, or location. We billed a 99213 E&M code for each appointment; other Current Procedural Terminology codes would yield different reimbursement rates.
Recruitment
To have at least 12 patients attend per week, three times as many needed to be recruited for each program. Our waiting list had 30 to 50 patients on it at a given time and each patient was called and confirmed. Patients who did not attend had other obligations, such as travel and would miss too many sessions, others had work or family conflicts. To accommodate more than 12 patients, we planned for 20 patients and our team was prepared to make changes if needed. The lead physician successfully saw all patients one-on-one and patients willingly stayed after hours for consult if needed.
Insufficient time and resources were put into Sports Performance versus Internal Medicine/Cardiology I and II. Sports Performance had a total of 22 patient encounters over 4 weeks as the initial pilot program for this new population. The recruitment period for these athletes was short and required additional vetting due to patients requiring parental consent and participants were not existing MedStar Health patients. However, the last 2 weeks of the program increased in attendance. Future Sports Performance programs should consider recruiting from other departments such as orthopedics and physical therapy as well as utilize strategies such as patient confirmation calls and ongoing recruitment.
Retention
In each program, the majority of patients attended five or more sessions. Reasons for not attending all sessions or leaving the program early included: other medical treatments or issues unrelated to the program, extra stress to work or family life, work or family obligations, timing of the program—especially during rush hour traffic, and travel. The Sports Performance, held in the summer, patient obligations included sporting events, vacations, and other entertainment events; weeks following events had peak attendance (Fig. 2).
Conclusion
This exploration investigated the implementation and feasibility of TK SMAs at MedStar Health. We sought to understand the operations and resources required to provide patients an effective lifestyle program incorporating a TK. Secondarily, we explored the potential outcomes of a weekly program to improve patient health and chronic disease risk through lifestyle.
Each program iteration was adapted to test operational improvements. Future operational improvements include improving recruitment processes by increasing outreach efforts several weeks before first session, and earlier for a new population or location.
Future programs seek to understand the effect of this SMA program on long-term behavior changes. Considerations for data collection may include short survey, administered through automated text messages; however, responses may be limited by demographics, including age. Therefore, validated questions sent through secured email as well as provided through paper may be beneficial. Sustainability should be further addressed for long-term outcomes, and one option is the development of intermediate and advanced level TK SMA programs.
Our team continues using information gathered during each program to make improvements to the operational procedures and program design. Patient feedback helps us understand the topics patients would like to learn more about as well as other experiences that can be improved. This feedback and our experiences implementing and improving new SMA programs, has influenced the development of a guide to disseminate new programs across the hospital system. This will walk physicians through the steps needed to plan and implement their SMA program at a MedStar Health location. Each portion of the guide are suggestions for new SMA teams to form each aspect pertinent to their program.
This study was waived by the MedStar Health Research Institute IRB Board as a quality improvement study.
Footnotes
Acknowledgments
The authors wish to thank the MedStar Institute for Innovation and MedStar Health Administrative and Clinical staff for the support, continuation, and expansion of the programs. Additionally, they would like to thank all of their past and current presenters, patients, and volunteers. This project was funded by the MedStar Institute for Innovation and continues to be funded as a program in operation at MedStar Health.
Ethics Approval
Waived by the MedStar Health Research Institute IRB—Quality Improvement.
Previous Presentations
Author Disclosure Statement
No competing financial interests exist.