
Abstract
Objectives:
Bupleurum chinense (BC; Radix Bupleuri) formulae are widely used in herbal medicine clinical practice for major depressive disorder (MDD). This study provides an up-to-date and comprehensive systematic review and meta-analysis of BC formula for MDD.
Design:
Randomized controlled trials were retrieved from English and Chinese databases, from their inceptions to March 2019. Included studies compared BC formula alone or as integrative medicine to selective serotonin reuptake inhibitor (SSRI) antidepressants. Studies included adults 18–65 years of age. People with other types of depression or physical comorbidities, such as poststroke depression, bipolar, and other mental or physical disorders, were excluded. Meta-analysis was performed using STATA software. Grading of Recommendations Assessment, Development, and Evaluation was also conducted to assess the quality of evidence.
Results:
Thirty studies compared BC formula to antidepressants and 25 studies compared BC formula plus antidepressants to antidepressants alone. BC formula was more effective than antidepressants at improving depression severity measured on the Hamilton Rating Scale for Depression (HRSD) (standardized mean difference [SMD] −0.35, 95% confidence interval [CI] −0.52 to −0.18, I 2 = 81.2%). Integrative use of BC formula plus SSRIs was also superior to SSRIs alone at improving HRSD scores (SMD −1.03, 95% CI −1.43 to −0.62, I 2 = 94.2%). However, heterogeneity of the included studies was high and quality was low. The total number and severity of adverse events in the BC formula groups were less than that in the antidepressant groups.
Conclusions:
BC formula alone or given as integrative medicine with antidepressants reduced depression severity. However, the evidence is low quality and at risk of bias. Well-designed studies are needed to validate the results we identified in this review.
Introduction
Major depressive disorder (MDD), commonly referred to as depression, unipolar depression, or clinical depression, is one of the most common mood disorders affecting individuals and societies worldwide. 1,2 It is associated with significant disability and mortality, and accounts for more than 40% of all mental disorders and substance abuse disorders. 3 It is characterized by sadness, loss of interest, and decreased energy, as well as other symptoms, including reduced self-esteem, loss of confidence, inappropriate or excessive guilt, and thoughts of death or suicide. 4
Depression is increasing in prevalence 5 and is predicted to be the second most common burden of disease by 2020. 6 The Global Burden of Disease Study reported that the disability-adjusted life years for MDD ranked 15th in 1990 and 11th in 2010. 7 It is estimated that as many as 12% of the population, both in developed and developing countries, will experience depression in their lifetime. 8
In primary care practice, people with depression are commonly prescribed antidepressants, such as selective serotonin reuptake inhibitors (SSRIs). 9,10 However, these treatments often need to be maintained even after remission and patients can become noncompliant when using antidepressants. 1,11 –13 Noncompliance is sometimes due to adverse events, such as dry mouth, dizziness, gastrointestinal effects, sexual dysfunction, sedation, and weight gain. 14 –17 Discontinuing medication and noncompliance have been reported to be associated with increased risk of recurrence of depression and high medical costs. 18,19
People with depression often use herbal medicine to alleviate symptoms or to avoid adverse events caused by antidepressants. In addition, they often believe herbal medicines are safe. 20,21 Research also indicates depression is an indicator and predictor of herbal medicine use. 22,23 However, there is a lack of evidence showing a statistically significant benefit or reduction in harms of herbal medicine compared to antidepressants. 24,25
Research has revealed a variety of chemicals, pharmacological agents, and clinical benefits of herbs for depression. 26,27 Bupleurum chinense DC (termed BC in this article) [Radix Bupleuri; Family: Apiaceae; Chinese name: Chai hu] is one of the most important herbs in Chinese medicine for depression and has been widely used in Asia and increasingly used in Western countries. Approximately, 74 compounds have been isolated from BC, including essential oils, triterpenoid saponins, polyacetylenes, flavonoids, lignans, fatty acids, and sterols. 28 BC is commonly combined with other herbal ingredients to make a formula (e.g., BC is combined with Citrus reticulata, Ligusticum chuanxiong, Citrus aurantium, Paeonia lactiflora, Glycyrrhiza spp., and Cyperus rotundus to make Chai hu shu gan san; or with Angelica sinensis, P. lactiflora, Atractylodes macrocephala, Poria cocos, Glycyrrhiza spp., Mentha haplocalyx, and Zingiber officinale to make Xiao yao san).
Previous systematic reviews of randomized controlled trials (RCTs) of BC formula, including Chai hu shu gan san and Xiao yao san, indicate that BC formula may be effective for depression, subclinical depression, including dysthymia, and secondary depression, such as poststroke depression. 29,30 However, the results from previous reviews were limited by poor quality studies. This systematic review provides an updated and focused assessment and analysis of the effecacy and safety of all types of BC formula for MDD compared to SSRI antidepressants.
Methods
We followed the methods described in the Cochrane Handbook of Systematic Reviews. 31
Inclusion and exclusion criteria
This review is a part of a larger project initiated by the China–Australia International Research Centre for Chinese Medicine and a systematic review protocol is registered with PROSPERO (CRD42018091770). The inclusion and exclusion criteria were predefined by the review team before data extraction.
Participants
Included studies were prospective, parallel RCTs, with participants 18–65 years of age and diagnosed with depression based on established clinical guidelines, including the Diagnostic and Statistical Manual of Mental Disorders (DSM), 4 the Chinese Classification of Mental Disorders (CCMD-3), 32 and the International Classification of Diseases (ICD-10). 33 We excluded studies that included participants with other types of depression, such as bipolar disorder, dysthymia, depressive symptoms caused by other mental or physical disorders, or depression caused by another medical condition or a substance.
Interventions and comparators
We included studies that used oral BC formula alone or in combination with other herbs as the intervention. We chose SSRIs as the comparator in this review, because clinical guidelines recommend SSRIs to treat depression. 16,34,35 We excluded studies that did not specify the type of antidepressants used as comparator.
Outcomes
Prespecified outcomes included clinician-rated scales, such as the Hamilton Rating Scale for Depression (HRSD), 36 and self-rated scales, such as the Zung's Self-Rating Depression Scale (SDS) 37 and the Montgomery-Asberg Depression Rating Scale. 38 These scales measure depression severity and related symptoms. Other outcomes included number of participants who relapsed or achieved remission, quality of life, functional capacity (e.g., social adjustment scales), suicidality, and adverse events.
Search strategy
We searched English and Chinese databases from their inceptions to March 2019. English databases included PubMed, Excerpta Medica Database (Embase), Cumulative Index of Nursing and Allied Health Literature (CINAHL), Cochrane Central Register of Comparatorled Trials (CENTRAL), and Allied and Complementary Medicine Database (AMED). Chinese databases included China BioMedical Literature (CBM), China National Knowledge Infrastructure (CNKI), Chongqing VIP (CQVIP), and Wanfang.
Search terms were mapped to controlled vocabulary in three groups: (1) condition (depression, depressive disorder, unipolar depression, major depression, major depressive disorder, and related terms); (2) intervention type (Chinese herbal medicine, herbal medicine, Bupleurum chinense, and related terms); and (3) study design (randomized controlled trials and related terms) (Supplementary Table S1).
In addition to electronic databases, we searched the reference lists of previous systematic reviews and their included studies. We also searched clinical trial registries for completed studies, including the United States National Institutes of Health register (
Data extraction
Search results from the English and Chinese databases were merged and duplicates were removed. Three reviewers (L.Y., J.L.S., and Y.M.D.) screened titles and abstracts and disagreements were resolved by discussion with a fourth reviewer (A.L.Z.). Full texts were obtained and screened against the inclusion criteria. Two reviewers (L.Y. and Y.M.D.) independently extracted data from relevant studies in EpiData software (EpiData Association, Odense, Denmark). Data checking and disagreements were resolved by discussion with a third reviewer J.L.S. Data included author names, publication year, title, journal, location, study design, diagnostic criteria, age, gender, intervention, comparator, outcome measures, treatment duration, sample size, dropouts, and adverse events.
Risk of bias
Two reviewers (L.Y. and Y.M.D.) independently used the risk of bias assessment tool from the Cochrane Handbook to assess risk of bias for each publication. 31 A third reviewer (J.L.S.) resolved any disagreement about risk of bias. Potential publication bias was assessed using Funnel plots and Egger's test.
Data analysis
Studies were synthesized using meta-analysis. Continuous outcome data were analyzed using mean difference (MD) and 95% confidence intervals (CIs). When different versions of outcome measures were used, standardized mean difference (SMD) was used for data analysis. Statistical heterogeneity was assessed using the I 2 statistic. An I 2 over 50% was considered to be an indicator of substantial heterogeneity. 31 Subgroup analyses were planned based on participant characteristics and study design, such as treatment duration, low risk of bias for sequence generation, and different versions of outcome measures.
Results
Characteristics of the included studies
Database searches identified 30,733 citations. After removing duplicates and excluding ineligible studies, we included a total of 55 RCTs (Fig. 1). 39 –93 Thirty of these RCTs (54.5%) compared BC formula to SSRIs, and 25 RCTs (45.5%) compared BC formula plus SSRIs to SSRIs alone (Table 1). All clinical studies were conducted in China and published from 2006 to 2017. Studies enrolled 5572 participants (sample size range: 46–480). Participants' ages ranged from 18 to 65 years. The duration of depression ranged from 1 month to 15 years, including single and recurrent episodes. Treatment duration ranged from 2 to 12 weeks (Table 1).
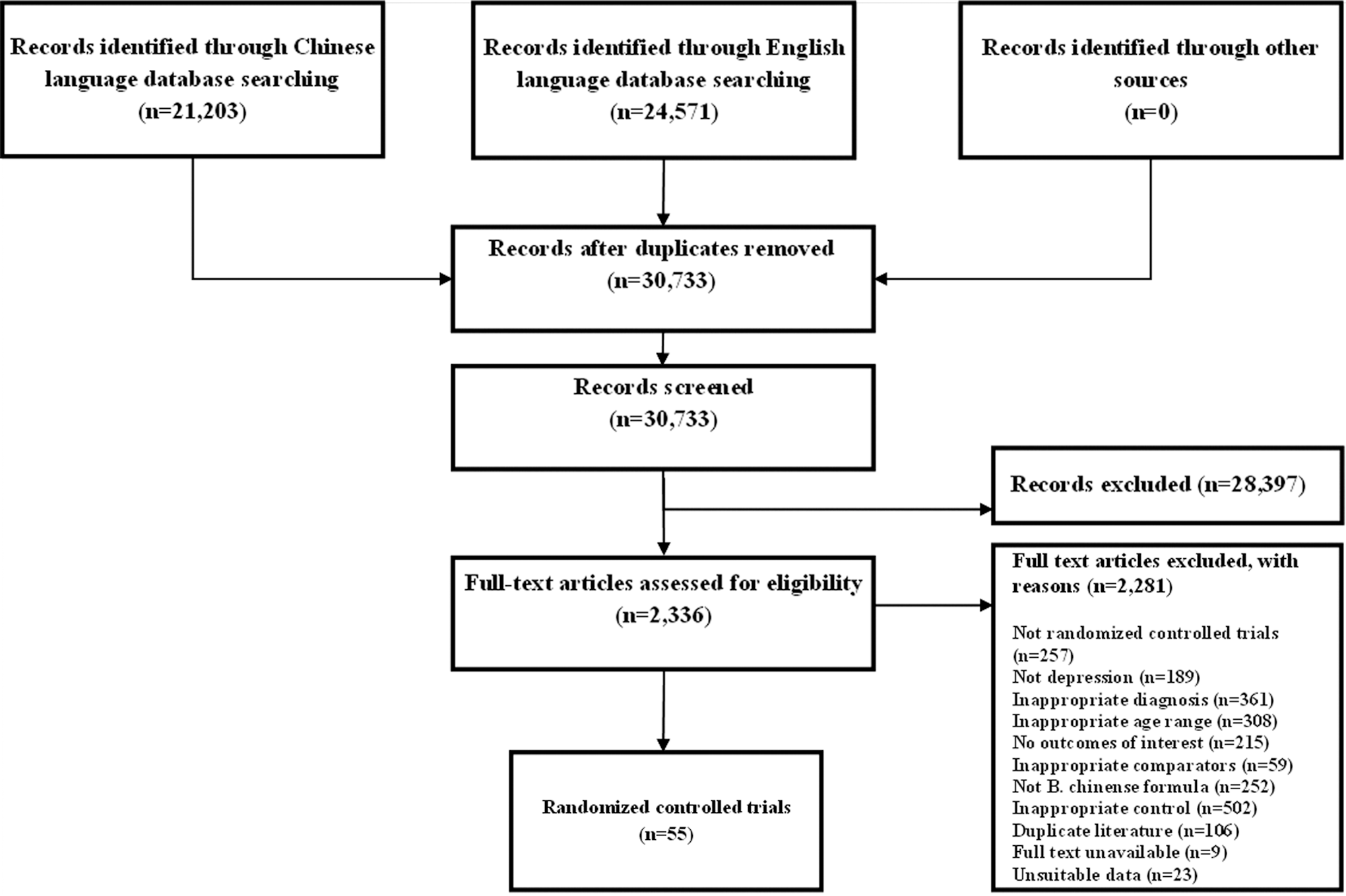
Flow chart of study selection process.
Characteristics of Included Studies
Risk of bias abbreviations: SG, sequence generation; AC, allocation concealment; BPt, blinding of participants; BPn, blinding of personnel; BOA, blinding of outcome assessment; IOD, incomplete outcome data; SOR, selective outcome reporting; Other, defined as baseline balance for the HRSD and SDS scores.
Risk of bias judgments: L, low risk; U, unclear risk or no information available; H, high risk.
AEs, adverse events; bid, twice per day; C, control groups; HRSD, Hamilton Rating Scale for Depression; I, intervention groups; qd, once per day; RCT, randomized controlled trial; SDS, Zung Self-Rating Depression Scale; SF-36, 36-Item Short Form Health Survey; SSRIs, selective serotonin reuptake inhibitors; TESS, Toxic Exposure Surveillance System; tid, three times per day.
All BC formula treatments were orally administered by the following herbal preparations: decoctions, oral solutions, capsules, granules, pills, and tablets. The studies used 49 BC formula and 103 different herbs. The most common formulae (including their modified forms) were Xiao yao san/wan (12 studies, 21.8%), Chai hu shu gan san (5 studies, 9.0%), Suan zao ren tang (2 studies, 3.6%), and Bu shen shu gan hua yu tang (2 studies, 3.6%) (Table 1).
The studies included the following SSRIs: fluoxetine (29 studies, 52.7%), paroxetine (16 studies, 29.1%), sertraline (7 studies, 12.7%), citalopram (2 studies, 3.6%), and escitalopram (1 study, 1.8%). All comparators were fixed dose and recommended by current clinical guidelines. 16,34,94
In terms of outcome measures, depression symptoms were commonly assessed using the HRSD (54 studies, 98.2%) and SDS (7 studies, 12.7%). Quality of life was assessed using the Short Form 36-Item Health Survey (SF-36) in one study (1.8%). Relapse and remission of depression, functional capacity, and suicidality were not assessed in the included studies. Adverse events were reported in 22 studies (40%). All events were considered mild (Table 4).
Risk of bias
All studies were described as randomized; however, only 14 (25.5%) described an appropriate method of random sequence generation and were judged at low risk of bias. Two (3.6%) described an appropriate method of allocation concealment, while 53 (96.4%) did not describe the details of allocation concealment, so were judged as having unclear risk of bias. Blinding of participants and personnel was reported in six studies (10.9%); these were judged to be at low risk of bias, while the remaining 49 studies (89.1%) were judged at high risk of bias. The method of blinding of outcome assessors was judged at low risk of bias in eight studies (14.5%). Outcome data were available for most studies, with 54 (98.1%) judged at low risk of bias. Selective outcome reporting was judged at unclear risk in all the studies because protocols were not available. Risk of bias assessment for each study is included in Table 1 and Figure 2.

Risk of bias.
Publication bias
Funnel plots and Egger's tests were reviewed for two comparisons. For BC formula versus SSRIs for HRSD, the funnel plot was asymmetrical and publication bias was detected (Egger's test t = −2.37, 95% CI −4.8 to −0.35, p = 0.025). However, for BC formula plus SSRIs versus SSRIs for HRSD, the funnel plot was symmetrical and publication bias was not detected (Egger's test t = −1.41, 95% CI −15.27 to 2.91, p = 0.17). The number of studies reporting other outcomes was less than 10, and funnel plot evaluation was not appropriate (Fig. 3).
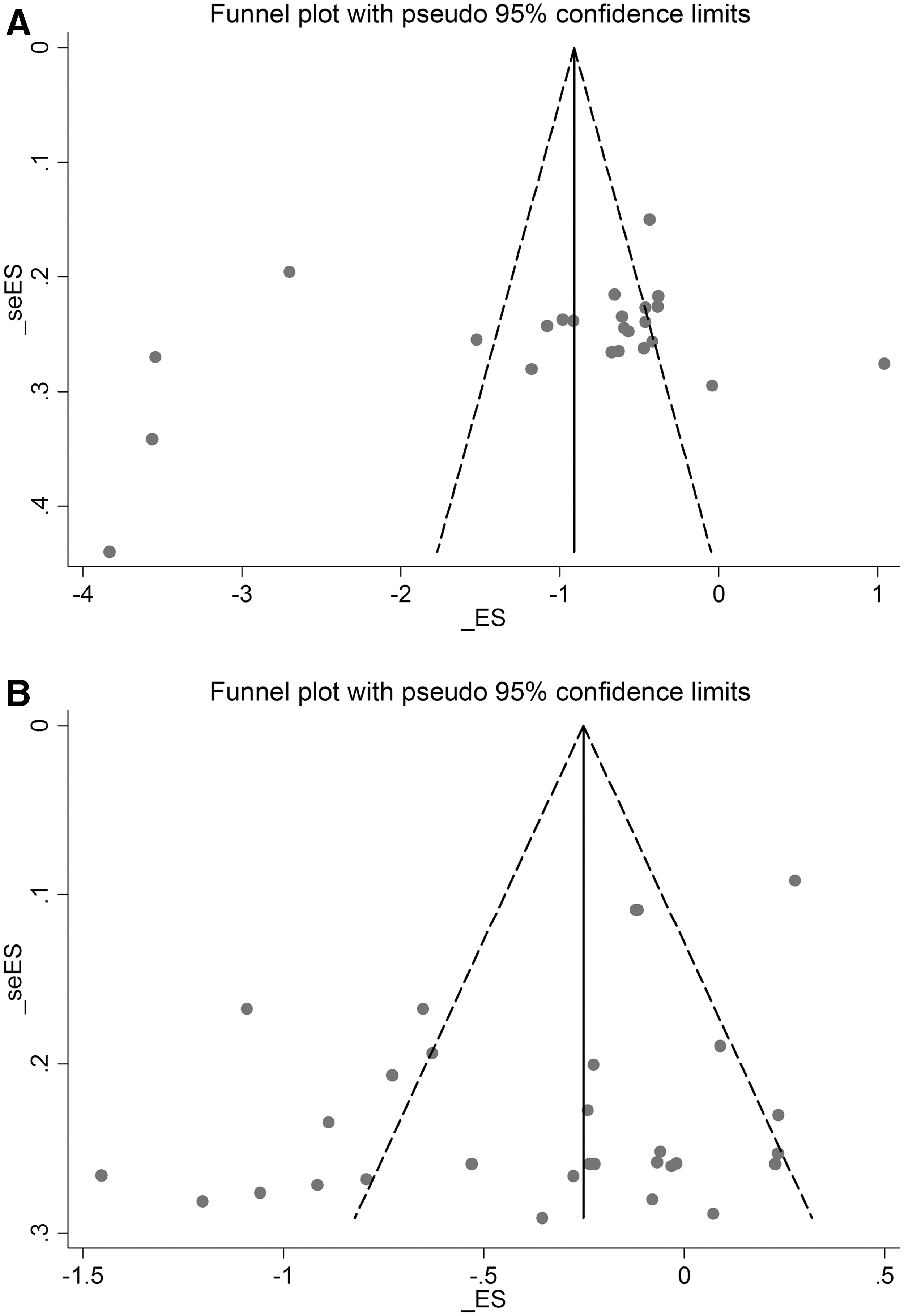
Funnel plots for publication bias.
BC Formula Versus SSRIs
Hamilton Rating Scale for Depression
Thirty of the 55 studies (3459 participants) used the HRSD to assess severity of depression (Table 1). 39 –41,45,49,50,53 –55,57–61,63,64,68,69,71,76,81 –85,87,88,90,92,93 Several versions of the HRSD, including HRSD-17 and HRSD-24, were used across these studies. Therefore, SMD was used to pool studies. After 2–12 weeks of treatment, significant reductions in the HRSD scores were seen in BC formula groups compared to SSRI groups (SMD −0.35 [−0.52 to −0.18]; I 2 = 81.2%), although heterogeneity was substantial, and quality of the evidence was very low (Fig. 4 and Table 2).
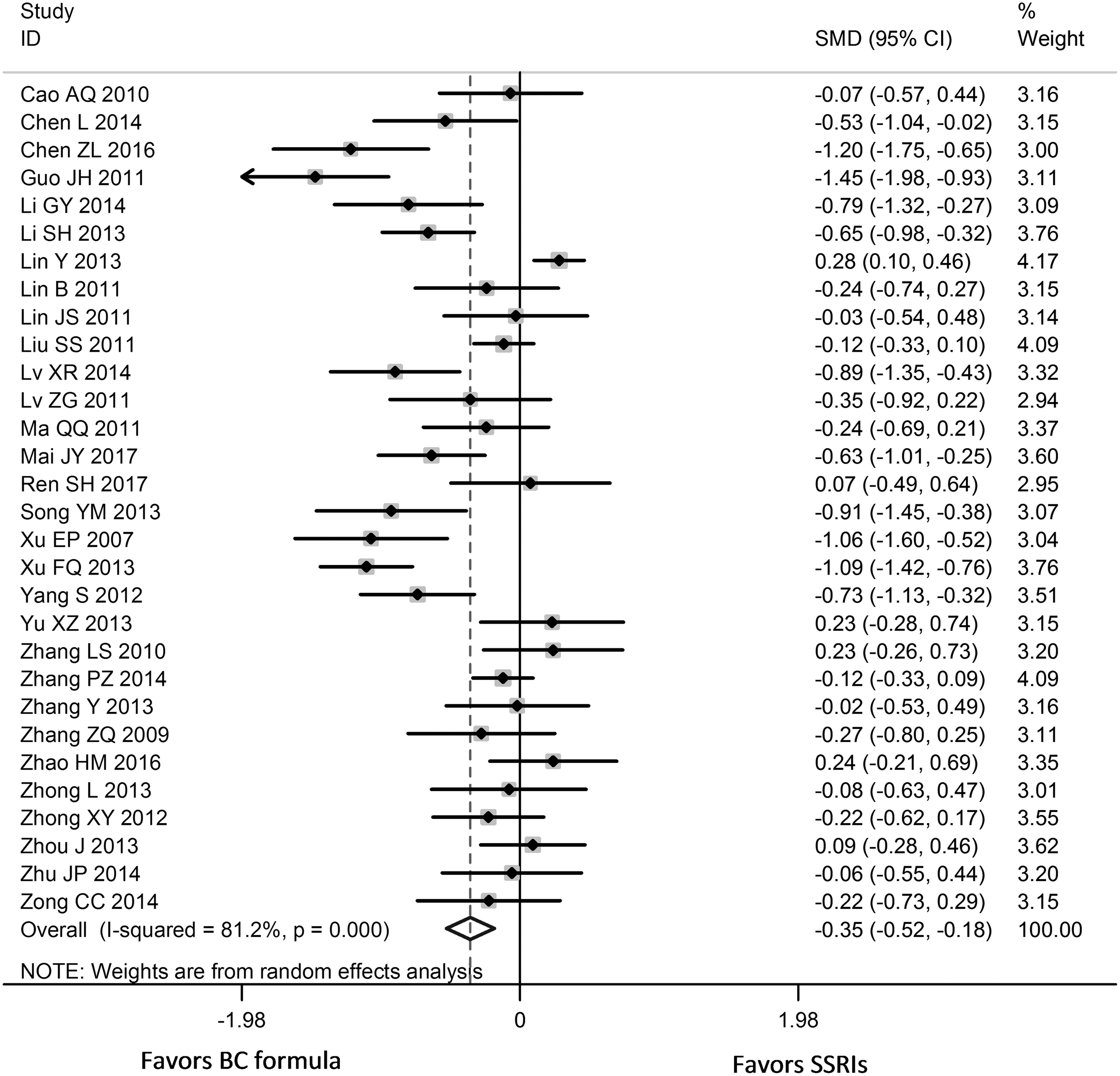
Forest plot comparing BC formula to SSRIs, in terms of Hamilton Rating Scale for Depression. Note that despite a significant difference between groups, studies had risk of bias, which should be considered when interpreting results from this figure.
Summary of Findings of Bupleurum chinense Versus Selective Serotonin Reuptake Inhibitors
The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
GRADE Working Group grades of evidence.
High quality: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.
Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect.
Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect.
Downgraded one level for unclear sequence generation and allocation concealment, lack of blinding of participants and personnel.
Downgrade one level for considerable statistical heterogeneity.
Downgrade one level for publication bias.
Downgrade one level for small sample size.
BC, Bupleurum chinense; CI, confidence interval; MD, mean difference; SD, standard deviation; SMD, standardized mean difference.
In terms of studies judged at low risk of bias for sequence generation, there were no significant differences between BC formula and SSRIs after subgroup analysis. Treatment for 6 weeks or less in 20 studies favored BC formula (SMD −0.33 [−0.50 to −0.16]; I 2 = 68.5%), as did treatment equal to or greater than 6 weeks in 10 studies (SMD −0.41 [−0.80 to −0.02]; I 2 = 90.2%). BC formula reduced depression severity more than the SSRI fluoxetine (SMD −0.42 [−0.64 to −0.21]; I 2 = 85.0%, 21 studies), but there was no statistical difference when compared to the SSRI paroxetine or sertraline. Subgrouping the HRSD version (Version 17) showed that BC formula was superior to SSRIs (SMD −0.25 [−0.47 to −0.04]; I 2 = 67.8%, 11 studies), although it was not superior in the HRSD-24 subgroup (SMD −0.19 [−0.46 to 0.08]; I 2 = 76.6%, 10 studies). Heterogeneity remained substantial after subgrouping and the reasons were not identifiable.
Zung's Self-Rating Depression Scale
The SDS was assessed in four studies comparing BC formula to SSRIs (283 participants). 53,68,81,88 Treatment duration ranged from 3 to 9 weeks. Two studies used fluoxetine as comparator, and the other two used paroxetine. After treatment, BC formula was superior to SSRIs (MD −1.53 [−3.03 to −0.03]; I 2 = 23.8%); low quality evidence (Table 2).
Adverse events
Twelve (40.0%) of the studies comparing BC formula with SSRIs reported adverse events. 40,45,49,50,55,57,58,63,71,85,87,92 People allocated BC formula interventions reported 125 adverse events and people allocated SSRIs reported 286 adverse events. Ten studies reported details about adverse events. In BC formula groups, 85 detailed adverse events were reported. Dry mouth (16 cases) and loss of appetite (16 cases) were the most common, followed by nausea (9 cases). In the SSRI groups, 196 detailed adverse events were reported, including dry mouth (53 cases), loss of appetite (31 cases), and nausea (14 cases). Two studies reported the nature of the events, but did not specify the number of adverse events in the SSRI group (Table 4). 55,63
BC Formula Plus SSRIs Versus SSRIs
Hamilton Rating Scale for Depression
Twenty-four studies, including 2041 participants, used the HRSD to compare the effects of BC formula plus SSRIs with the same SSRIs alone. 43,44,46 –48,51,52,56,62,65 –67,70,72 –75,77–80,86,89,91 After 4–12 weeks of treatment, BC formula plus SSRIs reduced the severity of depression more than SSRIs alone (SMD −1.03 [−1.43 to −0.62]; I 2 = 94.2%; low quality evidence) (Fig. 5 and Table 3).

Forest plot comparing BC formula plus SSRIs to SSRIs alone, in terms of Hamilton Rating Scale for Depression. Note that despite a significant difference between groups, studies had risk of bias, which should be considered when interpreting results from this figure.
Summary of Findings of Bupleurum chinense Plus Selective Serotonin Reuptake Inhibitors Versus Selective Serotonin Reuptake Inhibitors
The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
GRADE Working Group grades of evidence.
High quality: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate quality: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.
Low quality: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect.
Very low quality: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect.
Downgraded one level for unclear sequence generation and allocation concealment, lack of blinding of participants and personnel.
Downgrade one level for considerable statistical heterogeneity.
Downgrade one level for small sample size.
Adverse Events
In nine studies at low risk of bias for sequence generation, subgrouping also showed that BC formula plus SSRIs was superior to SSRIs alone (SMD −0.90 [−1.38 to −0.43]; I 2 = 90.0%). Treatment with BC formula for equal to or less than 6 weeks produced lower HRSD scores between groups (SMD −0.65 [−1.01 to −0.29]; I 2 = 87.4%, 15 studies). Treatment for greater than 6 weeks had similar results (SMD −1.63 [−2.42 to −0.84]; I 2 = 96.2%, 9 studies). Subgrouping by HRSD version (Version 17) showed that BC formula plus SSRIs was superior to SSRIs alone in 13 studies (SMD −0.67 [−0.87 to −0.47], I 2 = 59.4%).
Zung's Self-Rating Depression Scale
Three studies, including 289 participants, used the SDS to compare BC formula plus SSRIs with SSRIs alone. 42,44,67 After 4–12 weeks of treatment, SDS scores in the BC formula plus SSRIs groups were significantly lower than those in the SSRI-alone groups (MD −7.19 points [−8.39 to −5.99]; I 2 = 0.0%); low quality evidence (Table 3).
Short Form SF-36 Health Survey
One RCT evaluated 90 participants using the SF-36 to measure quality of life. 48 Individual health domains were not reported, but an aggregate score was given. BC formula plus paroxetine was superior to paroxetine after 8 weeks of treatment (MD 13.53 [9.82–17.24]) (Table 3).
Adverse events
Ten studies mentioned adverse events. 43,44,52,56,65,70,73,77,79,80 In the BC formula plus SSRIs groups, 118 events were reported, while in the SSRI groups, 174 events were reported. Nine studies provided adverse event information. Diarrhea was the most common adverse event in the BC formula plus SSRIs group (17 cases), while constipation was the most common adverse event in the comparator groups (22 cases). Other adverse events included hypersomnia, nausea, and vomiting (Table 4). Eight of the studies reported adverse events on the Toxic Exposure Surveillance System (TESS); after treatment, TESS was lower, indicating less severe and fewer adverse events in the integrative medicine group compared to SSRIs alone (MD −1.12 [−1.69 to −0.55] I 2 = 93.2%) (Table 3).
Discussion
BC formula may be effective for improving clinical symptoms and alleviating depression severity. It also appers to be safe, with the number of adverse events in the BC formula groups being half that of the SSRI groups. In addition, meta-analyses for depression severity measured on the HRSD and SDS scales consistently indicated that BC formula has a promising effect when given alongside SSRIs or alone for reducing depression severity. However, heterogeneity and limitations in study methodology should be considered when interpreting these results. Meta-analysis showed that at the end of treatment, there was a significant difference in the HRSD and SDS scores between BC formula and SSRI groups, indicating a potentially clinically important effect. 31 This result was consistent with previous systematic reviews of herbal medicine for depression. 95 –98
Our review indicates that BC formula for depression is effective in the short term, similar to acute-phase treatment with antidepressants. 99,100 When BC formula was used as integrative medicine, the pooled results showed that it may reduce the severity of depression compared to SSRIs alone. The total number of adverse events in the BC formula groups was less than that in SSRI groups.
Improvements of BC formula groups, either integrative use or used alone, were more obvious after treatment for 6 and 12 weeks. Research indicates that a minimum of 8–10 weeks of treatment is needed for optimal symptom reduction. 35,101
Contemporary experimental research suggests that herbal compounds or compound combinations act on various targets and pathways to produce antidepressant effects. Preclinical studies have shown these herbs' antidepressant effects are related to their antioxidant and neurotransmitter properties. 102,103 Xiao yao san/wan has reported antidepressive effects in preclinical studies. 104 Chai hu shu gan san has also shown its effects are comparable to the antidepressant drug fluoxetine. 105,106 More research into key herbal compounds of B. chinense and BC formula in animal models or neuronal cells is needed to further elucidate the possible mechanisms of action of this herb.
Limitations of the study
Included studies were not free from bias. They also had methodological shortfalls, such as unclear sequence generation and allocation concealment, and a lack of blinding of participants and personnel. Considerable heterogeneity was also noted and could not be resolved by subgroup analysis. It may be due to variable etiologies, severity of depression, disease history, study protocols, and outcome measurements. The BC formula interventions were considered to be the same and therefore merged in meta-analysis. However, there were differences between studies in terms of treatment duration, other herbal ingredients, dosage, and medication compliance that may have contributed to heterogeneity.
Future studies
Future clinical studies of BC formula for MDD need rigorous methodology, including clearly stated methods of sequence generation and allocation concealment. Future studies should also publish their protocols and be registered with a clinical trial registry to minimize reporting bias and increase transparency in reporting of the results.
Cause of depression, severity, disease history, treatment preference, and expectancy should be taken into consideration when designing trials and selecting participants. Selecting similar participants, in terms of etiology, age range, and severity, may help to achieve more comparable and reliable results. Assessing clinically important outcomes, such as relapse and remission of depression, quality of life, functional capacity, and suicidality, would provide a comprehensive understanding of the effect of BC formula. As for treatment expectancy, it may influence treatment effect and modify clinical decisions, and should be considered when designing trials and drawing conclusions.
Treatment duration in the included clinical trials ranged from 2 to 12 weeks and only a few reported follow-up data. Depression is a lifelong disease and should be monitored every 1–2 weeks during treatment. Follow-up assessment would provide long-term data and further strengthen the evidence.
Future clinical studies should also report the items required by the Consolidated Standards of Reporting Trials (CONSORT) 107 and its extensions for herbal medicine. 108,109 Informative reporting of trial participants, reason for intervention selection, comparator, and results of validated outcome measures will provide high-level clinical evidence, and will benefit practitioners, researchers, patients, and knowledge translation.
Conclusions
BC formula alone or given as integrative medicine with SSRIs may reduce depression severity. The current evidence should be interpreted with caution due to bias and methodological shortfalls in the included studies, and heterogeneity in meta-analysis. BC formula does not appear to increase the risk of adverse events. New studies with rigorous methodologies in well-defined populations, including short- and long-term follow-up, will help validate the promising evidence identified in this review.
Footnotes
Acknowledgments
The authors sincerely acknowledge the support of staff at the Discipline of Chinese Medicine, School of Health and Biomedical Sciences of RMIT University, and research staff at the Evidence-Based Medicine and Clinical Research Service Group of the Guangdong Provincial Hospital of Traditional Chinese Medicine, in providing resources. We also acknowledge the help of staff at the Department of Psychology and Sleep Medicine of the Guangdong Provincial Hospital of Traditional Chinese Medicine. This work was supported by the China–Australia International Research Centre for Chinese Medicine (CAIRCCM)—a joint initiative of RMIT University, Australia, and the Guangdong Provincial Academy of Chinese Medical Sciences, China. We also received additional funding from the Ministry of Science & Technology of China (International Cooperation Project, Grant No. 2012DFA31760) and Guangdong Provincial Hospital of Traditional Chinese Medicine (Grant No. YN2016QL05 and YN2015QN23).
Author Disclosure Statement
No competing financial interests exist.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.