
Abstract
Objectives:
To assess the change in the bone mineral density (BMD) score, bone-specific biomarkers (serum vitamin D3, tartrate-resistant acid phosphatase 5b [TRAP-5b], and osteocalcin), quality of life, Ayurvedic symptoms (Asthikshaya Lakshanas), and fracture risk assessment tool (FRAX) scores following treatment with Panchatikta Ghrita (PG), a classical herbal formulation as add-on therapy to calcium and vitamin D3 supplements.
Study design:
Randomized, open-labeled, comparative, controlled clinical study.
Location:
TN Medical College and BYL Nair Hospital, Mumbai, India.
Study participants:
Eighty adult patients, aged between 40 and 75 years, diagnosed to have osteopenia (BMD T-score between −1 and −2.5 in at least two of the three joints tested—lumbar spine L1–L4, left femur-neck, left forearm-radius total).
Study intervention:
Treatment group received two tablespoons of PG (10 mL in lukewarm milk) along with calcium and vitamin D3 supplements twice a day, whereas control group received only calcium and vitamin D3 supplements twice a day for a period of 12 months.
Outcome measures:
BMD, bone-specific biomarkers (vitamin D3, TRAP-5b, and osteocalcin), quality of life, Ayurvedic symptoms, and FRAX scores were evaluated before and at 6 and 12 months.
Results:
Eighty patients were enrolled; of which, 65 patients completed the study while 15 patients dropped out. Improvement in the BMD scores was observed at 6 and 12 months with the maximum benefit in the lumbar spine region. Significant improvement in the bone-specific biomarkers, namely serum vitamin D3 (p < 0.001), osteocalcin (p < 0.001), and TRAP-5b (p < 0.05), was observed in the PG-treated group compared with the standard treatment group. Improvement in the quality of life, Ayurvedic symptoms scores, and risk reduction in FRAX scores of major osteoporotic fracture risk and hip fracture risk was greater with PG, although not statistically significant.
Conclusions:
The study findings demonstrate that PG slows down the bone degeneration processes by its stabilizing effect on the bone-specific biomarkers, indicating its potential usefulness as preventive therapy in osteopenia. The positive improvement noted in this study needs to be confirmed in studies with a larger sample size and longer duration.
Introduction
Osteopenia is considered the initial step along the path to osteoporosis, a serious condition in which bone density is extremely low. If the bone mineral density (BMD) T-score is between −1.0 and −2.5, it is called as osteopenia. 1 There is a wide range of fracture risk in osteopenia, which is related to age, BMD, and clinical risk factors. Data from Indian studies have shown that osteopenia was more prevalent than osteoporosis among postmenopausal women and men. 2,3
Bone fractures due to osteopenia and osteoporosis are important because both the diseases are very painful, although some spinal (vertebral) fractures are painless. Along with the pain, hip fractures are a serious problem because they require surgical repair. 4 Also, up to 30% of patients require long-term nursing home care after a hip fracture. 5 Fractures, generally in the elderly, are associated with increase in overall mortality (death rate). There is ∼20% mortality following hip fracture due to complications, such as immobility, pneumonia, and many other reasons. 6
Hormone replacement therapy (HRT) along with the prevention of bone loss is useful in reducing the incidence of vertebral and hip fractures. However, long-term HRT is associated with increased risk of breast cancer, thromboembolism, and hypertension, and hence, it is not generally considered as the first-line treatment for osteoporosis. 7 –9
Although selective estrogen receptive modulators (SERMs) have a protective effect on the bone, their effect on BMD is lower than that of estrogens. Long-term treatment with SERMs like raloxifene did significantly reduce vertebral fractures in women with osteoporosis, although the effect on hip fractures was not significant. 10 SERMs are very effective at preventing and treating osteoporosis in postmenopausal women, particularly in the initial 5 to 10 years after menopause. 11
Bisphosphonates are safe and effective in reducing fracture risk in patients with osteoporosis; however, concerns have been raised regarding their association with side effects, such as gastrointestinal tolerability, musculoskeletal pain, osteonecrosis of the jaw, atrial fibrillation, atypical fractures, and esophageal cancer, which have resulted in poor compliance and persistence with therapy. 12 –16
Thus, due to long-term adverse effects of synthetic drugs, researchers and scientists are now looking toward clues from the Traditional systems of medicine for the treatment of certain chronic debilitating diseases, which include osteoporosis. In Ayurveda, there is no direct mention of the condition “Osteoporosis” in the ancient texts of Ayurveda; there are references stating to decrease in asthi or bone tissue with advancing age. This condition creates imbalance of the vata dosha, which further deteriorates the bone. As per Ayurveda, this condition is treated using medicinal plants with katu (pungent) and tikta (bitter) properties. 17 Panchatikta Ghrita (PG) is one such classical Ayurvedic formulation with a combination of plants with katu and tikta properties. These plants are said to possess tikta rasa (bitter taste), ushna (heat-generating property that helps in reducing the vata dosha), virya (potency of drug action), madhur (sweet), and katu vipaka (reflects the fate of the drug) properties. Tikta rasa increases the asthidhatvagni (stabilizes the interplay between the anabolic and catabolic stages of bone metabolism), which in turn improves the nutrition of the tissues (dhatus). This helps stabilize the asthi dhatu and the deranged vata dosha, which in turn decreases the degeneration seen in the bone tissue (asthi dhatu). 18,19 This formulation has thus been claimed to help relieve the pain associated with bone degeneration and also helps in tissue regeneration. 20
Hence, the authors proposed to conduct a randomized, open-labeled, comparative, controlled clinical study to assess the antiosteoporotic efficacy of this classical Ayurvedic formulation in patients with osteopenia when given along with calcium and vitamin D3 supplements and to compare its effects with that of calcium and vitamin D3 supplements, the standard of care (SOC) in osteopenia.
The primary study objectives were (1) to assess the change in the BMD score in patients treated with PG at the end of treatment and (2) to compare the change in the BMD score between patients treated with PG, and calcium and vitamin D3 supplements. The secondary objectives were (1) to compare the change in the bone-specific biomarkers (serum vitamin D3, osteocalcin, and tartrate-resistant acid phosphatase 5b [TRAP-5b]) between the two study groups at the end of treatment, (2) to assess the clinical safety of PG, (3) to compare the change in quality-of-life scores between the two study groups at the end of treatment, (4) to compare the change in Ayurvedic symptom scores (Asthikshaya Lakshanas) between the two study groups at the end of treatment, and (5) to compare the fracture risk assessment tool (FRAX) scores between the two study groups at the end of treatment.
Materials and Methods
Patient enrollment
The study was initiated in March 2016 after receiving approval from the Institutional Ethics Committee for Academic Research Projects (ECARP) of a tertiary care public hospital in an urban metropolitan city and was conducted in accordance with the locally applicable good clinical practice (GCP) and ethical guidelines. 21,22 Potential participants were identified from the Ayurvedic and Endocrinology outpatient departments of this hospital. They were screened for the eligibility criteria after explaining the trial purpose and procedures and written informed consent. Those patients of either sex between the age group of 40–75 years, suffering from osteopenia with a BMD T-score between −1 and −2.5 in at least two of the three joints tested (anterio-posterior spine L1–L4, left femur-neck, left forearm-radius total), and with the history of fractures that may have occurred with a minor injury or fall were included. Patients consuming drug(s) known to affect bone metabolism, for example, SERMs, bisphosphonates, calcitonin, vitamin D3 (more than 60,000 U), and corticosteroids (more than 5 mg/day of prednisolone of equivalent) for more than 3 months, methotrexate, anticonvulsants, diuretics, and others, and patients suffering from osteomalacia, tumors, osteonecrosis, infections, and other bone-softening metabolic disorders, congenital disorders (dysosteogenesis and Marfan syndrome), leukemia, lymphoma, metastases (bony and other), pathological fractures secondary to bone metastases from cancer, osteogenesis imperfecta, renal osteodystrophy, malabsorption syndrome, and others were excluded from the study. Target enrollment was 80 patients (40 in each group). The study is registered with CTRI—No. CTRI/2018/07/014904.
Study details
Enrolled participants were patients randomly assigned in a 1:1 ratio by a computer-generated randomization program to one of the two study groups, with patients in the treatment group—PG group—received the classical PG formulation (10 mL in 300 mL lukewarm milk) orally in a dose of two tablespoons along with calcium and vitamin D3 supplements (containing elemental calcium 1200 mg and vitamin D3 [cholecalciferol] 800 IU/day) twice a day, whereas patients in the control group—SOC group—received only calcium and vitamin D3 supplements twice a day. The participants in the treatment group were given spoons and measuring glasses with markings of 10 and 300 mL, respectively, to ensure that the given dose of the formulation was taken in desired amount of milk. Patients were requested to participate in the study for 1 year.
Study intervention
PG classical herbal formulation was prepared as per the Ayurvedic Pharmacopoeia of India, Part II (formulations). Vol I, Part-I, 6:26 (No.31) at a Good Manufacturing Practices (GMP)-certified Ayurvedic Pharmacy, which included eight different plant parts as its ingredients. 23 The details are listed in Table 1. Quality control analysis was performed on the prepared formulation before use, and a single batch was used for the entire study.
Details of the Ingredients Present in Panchatikta Ghrita Classical Herbal Formulation
Outcome measures
At the end of the study duration, that is, 1 year, the primary outcome measure was the change in the BMD score in both groups. The secondary outcomes measures were changes in (1) bone-specific biomarkers (serum vitamin D3, osteocalcin, and TRAP-5b), (2) clinical safety of PG, (3) quality-of-life scores, (4) Ayurvedic symptom scores (Asthikshaya Lakshanas), and (5) FRAX scores between the two study groups at the end of treatment.
Clinical assessment
Detailed clinical history and physical examination were carried out at every study visit. Adverse events were also monitored at the monthly visits and by telephone calls between visits. Patients were also requested to report any adverse event that they experienced between the study visits during the study period to the study investigators via phone calls or personal visits to the study site.
Bone mineral density
Dual energy X-ray absorptiometry (DEXA) scan was performed at the baseline visit to measure the BMD and the T-scores as per the World Health Organization (WHO) guidelines. The scan was repeated at 6 and 12 months.
Fracture risk using the fracture risk assessment tool
This tool was developed by the WHO in 2008 to determine the 10-year probability of fracture risk of an individual. 24 Here, the fracture risk is calculated in men or women based on age, body mass index, and independent risk variables comprising a prior fragility fracture, parental history of hip fracture, current tobacco smoking, long-term use of glucocorticoids, rheumatoid arthritis, other causes of secondary osteoporosis, and daily alcohol consumption of three or more units. Based on these calculations, the 10-year probability of the major osteoporotic fracture risk (MOFR) and the hip fracture risk (HFR) is obtained for an individual. In this study, the MOFR and HFR were determined at baseline, 6 months, and at the end of the study (12 months).
Laboratory assessment
Blood was collected aseptically at the baseline visit for the various study-related hematological (hemoglobin, complete blood count) and biochemical (calcium, blood urea nitrogen, creatinine, total proteins, serum bilirubin, serum glutamic oxaloacetic transaminase, serum glutamic pyruvic transaminase, and alkaline phosphatase) investigations and also the bone-specific biomarkers, namely serum vitamin D3, TRAP-5b, and osteocalcin levels. These tests were performed again at 6 and 12 months of the study.
Patient-reported outcomes
Quality-of-life assessment was performed using the International Osteoporosis Foundation Quality-of-Life questionnaire (QUALEFFO-41) 25 at baseline, 6 months, and 12 months and the score documented. The QUALEFFO-41 is a validated, self-administered disease-specific questionnaire. It possesses 5 domains (41 items in total): pain (5 items), physical function (17 items), social function (7 items), general health perception (3 items), and mental function (9 items). Items are scored in the reverse order (the minimum number on the scale is assigned to the best answer and the maximum to the worst answer), except for the items No. 33, 34, 35, 37, 39, and 40. The responses to these six items are scored in the correct order, that is, the minimum number on the scale is assigned the worst answer and the maximum number is assigned the best answer. The score of each domain is calculated as an average value of all the answered items linearly transformed on a scale 0–100. The total QALEFFO score is calculated as a sum of all answers to items and then linearly transformed on the scale 0–100. The worse the health-related quality of life (HRQOL) condition is, the higher the score gets. The scoring algorithm is made in a way to calculate the total score proportionally to the answered items (when a missing value is present, the calculations are corrected according to the number of missing values). According to the scoring algorithm, the missing value should not have exceeded 30%, otherwise the domain or the total score becomes inaccurate. The QUALEFFO-41 questionnaire is presented in Supplementary Appendix SA1.
An Ayurvedic symptoms-based questionnaire (Asthikshaya Lakshanas) was also prepared using references from Ayurvedic texts 26 and publication 27 to document bone-related complaints. The questionnaire underwent content validation with a team of 5 Ayurvedic physicians with 5–7 years of experience (content validity ratio of 0.8), was then pilot tested in 24 participants, and its reliability was confirmed with an internal consistency of 0.7 using Cronbach's alpha test. This questionnaire was administered to the participants at six monthly intervals to assess any improvement in patient symptoms following therapy over the study period (Supplementary Table S1).
Statistical analyses
The study was planned as a randomized, comparative two-arm study using a continuous response variable (BMD) with equal number of patients in each group. As there was no previous literature available of similar studies using this formulation, the sample size was calculated assuming a 10% expected difference between the study groups with standard deviation of 15%. Thus, the sample size came to about 36 patients in each group so as to be able to reject the null hypothesis that the population means between the two groups are equal with probability (power) of 80% and type I error probability associated with this test of this null hypothesis was 5%. Assuming 10% dropout, the authors considered a sample size of 40 patients in each group.
With respect to data analysis, efficacy data parameters were assessed using per-protocol analysis while intention-to-treat analysis was performed for the safety parameters. Continuous measures are presented as mean and standard deviation at each time point. Kolmogorov–Smirnov tests were performed to assess the normality of the quantitative variables. If normally distributed, repeated-measures ANOVA (analysis of variance) was used to verify whether statistically significant differences exist among the treatment and control groups followed by the Tukey–Kramer multiple comparisons post hoc test. For those parameters that did not pass the normality test, Kruskal–Wallis or Friedman tests were used followed by Dunn's multiple comparisons post hoc test. When the comparisons were performed between only two of the groups, Student's t tests or Mann–Whitney tests were used, as applicable. Statistical analyses were performed using GraphPad Instat version 3.06 (GraphPad Software, San Diego, CA).
Results
Participant characteristics
One hundred and twenty-eight participants with osteopenia were screened for eligibility to participate in the study following written informed consent. Of these, 48 participants were not found to be eligible. Thus, 80 participants were randomized to either of the 2 study groups and were administered the study medications as per the group that they were randomized. Of these, 32 participants from the PG group and 33 patients from the SOC group completed the study. Eight patients dropped out from the PG treatment group; of which, five did not follow-up mainly due to poor adherence, whereas seven patients did not follow-up from the SOC group. Overall patient adherence to the study was 87.5% for the herbal treatment (PG) group and 82.5% for the SOC group. Compliance with regard to consumption of the study medicines was assessed at monthly intervals in terms of missed doses reported by the patients and amount of the formulation left in the bottle returned at every visit by the patient for the PG group and by pill count for the SOC group. Compliance was found to be 78.14% ± 8.87% in the PF group compared with 80.32% ± 8.92% in the SOC group. The study flow chart and the reasons for discontinuation are shown in Figure 1. Demographic and Prakriti details of the study participants are described in Table 2. There were no significant differences in baseline characteristics between the two groups.
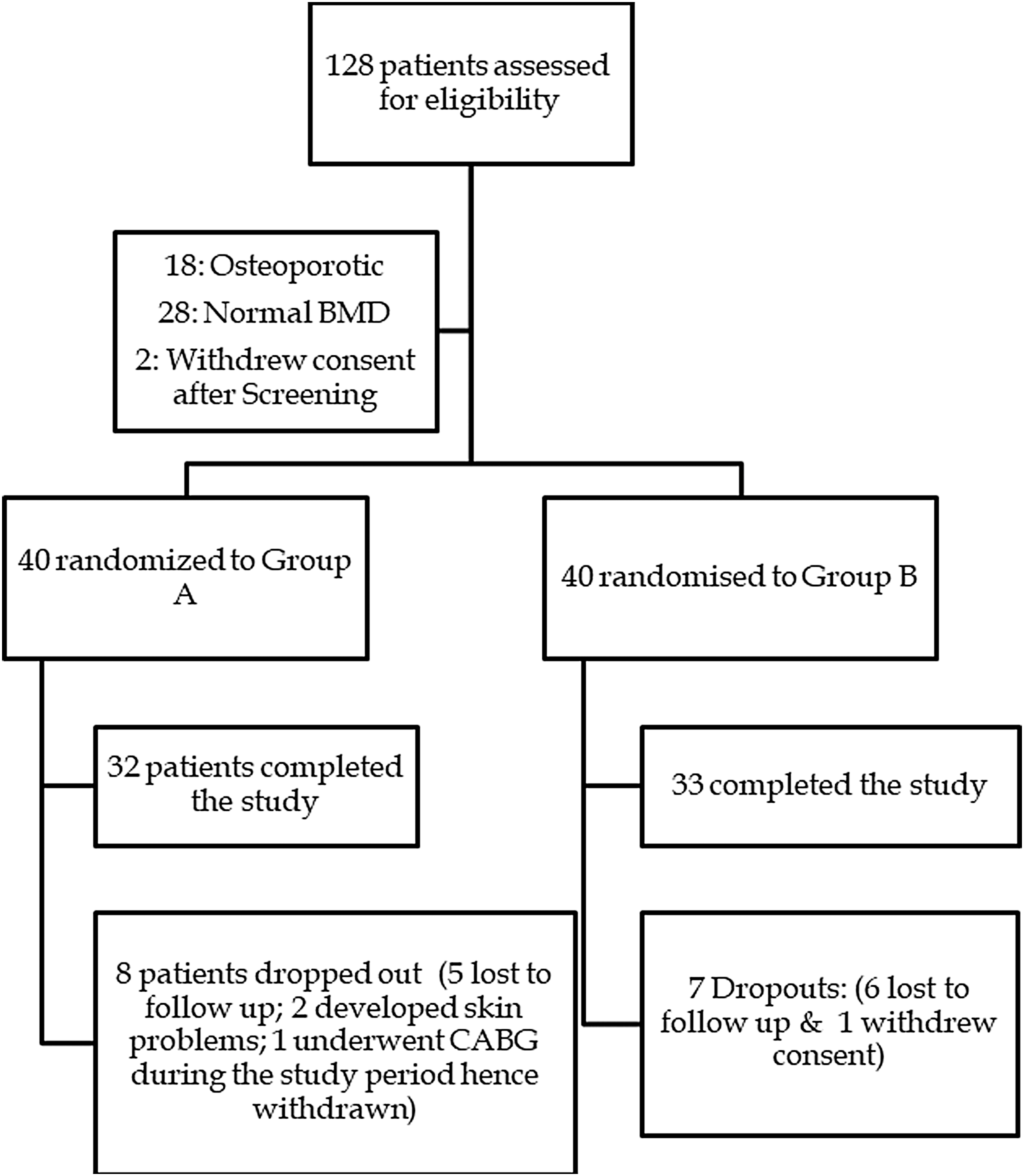
Study flow chart showing patient's progress in the study.
Group-Wise Demographic and Prakriti Details of the Study Participants
PG, Panchatikta Ghrita; SOC, standard of care.
Primary outcome measure
Effect on BMD T-score
Improvement in the BMD scores was observed at the end of 6 months, which was sustained at 12 months in both the study groups with higher overall T-scores observed in the PG group compared with the SOC group at both time points, although not statistically significant. Maximal improvement was observed in the lumbar spine and left forearm regions. In case of the SOC group, although an improvement in the T-score was observed at 6 months, the effect was not sustained at 12 months (Table 3).
Bone Mineral Density (T-Score) of the Two Study Groups (Region-Wise and Overall Values)
Results are expressed as mean ± SD (95% confidence interval).
p > 0.05 = not significant.
Analytical test used: repeated-measures analysis of variance with post hoc test as the Tukey–Kramer multiple comparisons test for within-group analysis and Student's unpaired t test for between-group analysis.
PG, Panchatikta Ghrita; SD, standard deviation; SOC, standard of care.
Secondary outcome measures
Increase in serum calcium, although not statistically significant, was observed in the PG group, whereas a decrease was observed in the SOC group at the end of 6 and 12 months (Fig. 2). In case of the bone-specific biomarkers, the serum vitamin D3 level was higher in the PG group than in the SOC group at 6 and 12 months, which was statistically significant at 12 months (30.3 ng/mL vs. 22.3 ng/mL) (Fig. 3). Similarly, a decrease was observed in both serum osteocalcin and TRAP-5b levels, with the fall being significantly higher in the PG group compared with the SOC group at both 6 and 12 months indicating decreased bone turnover (Figs. 4 and 5).
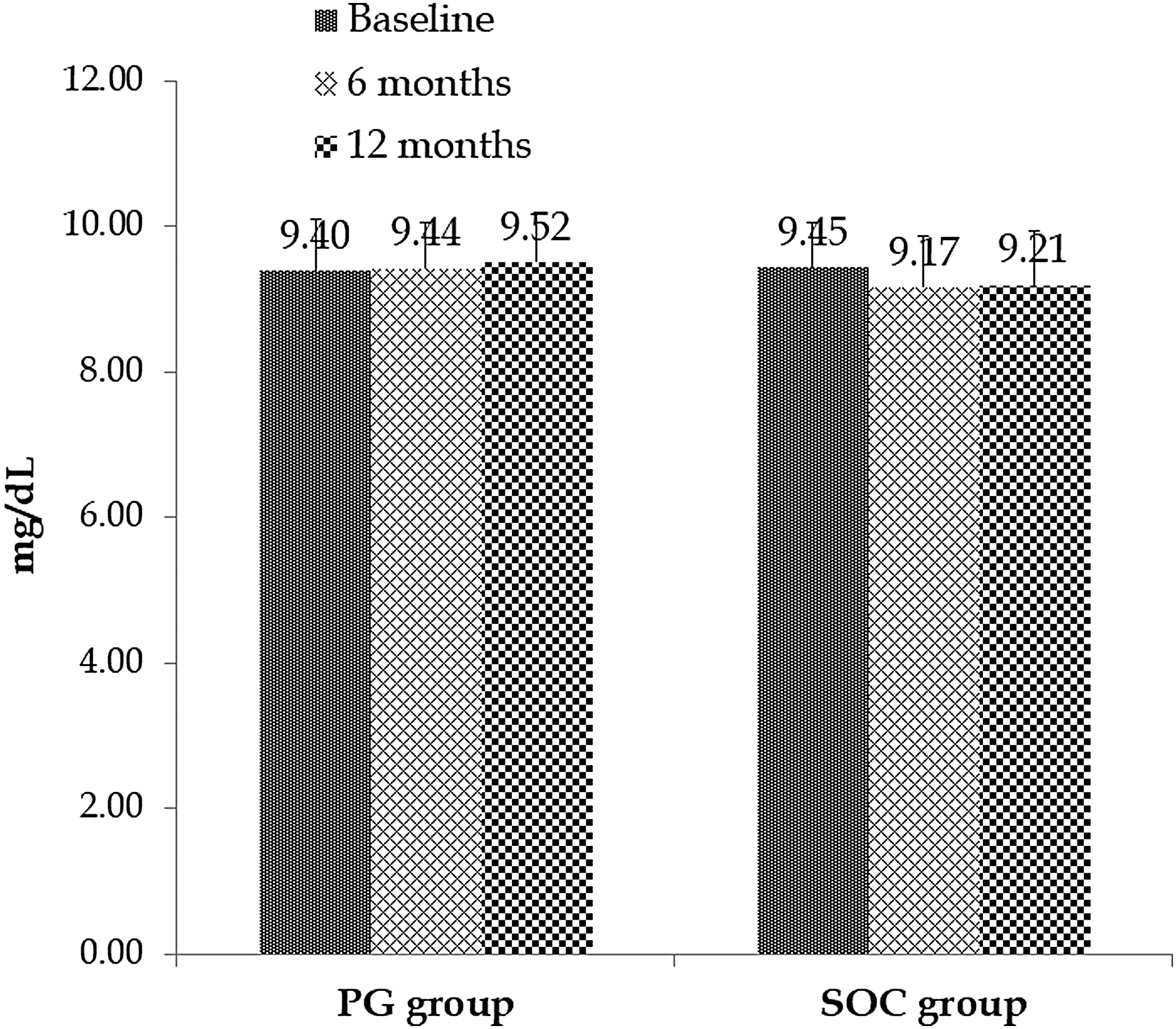
Serum calcium levels in both the study groups. Results are expressed as mean ± SD. SD, standard deviation.
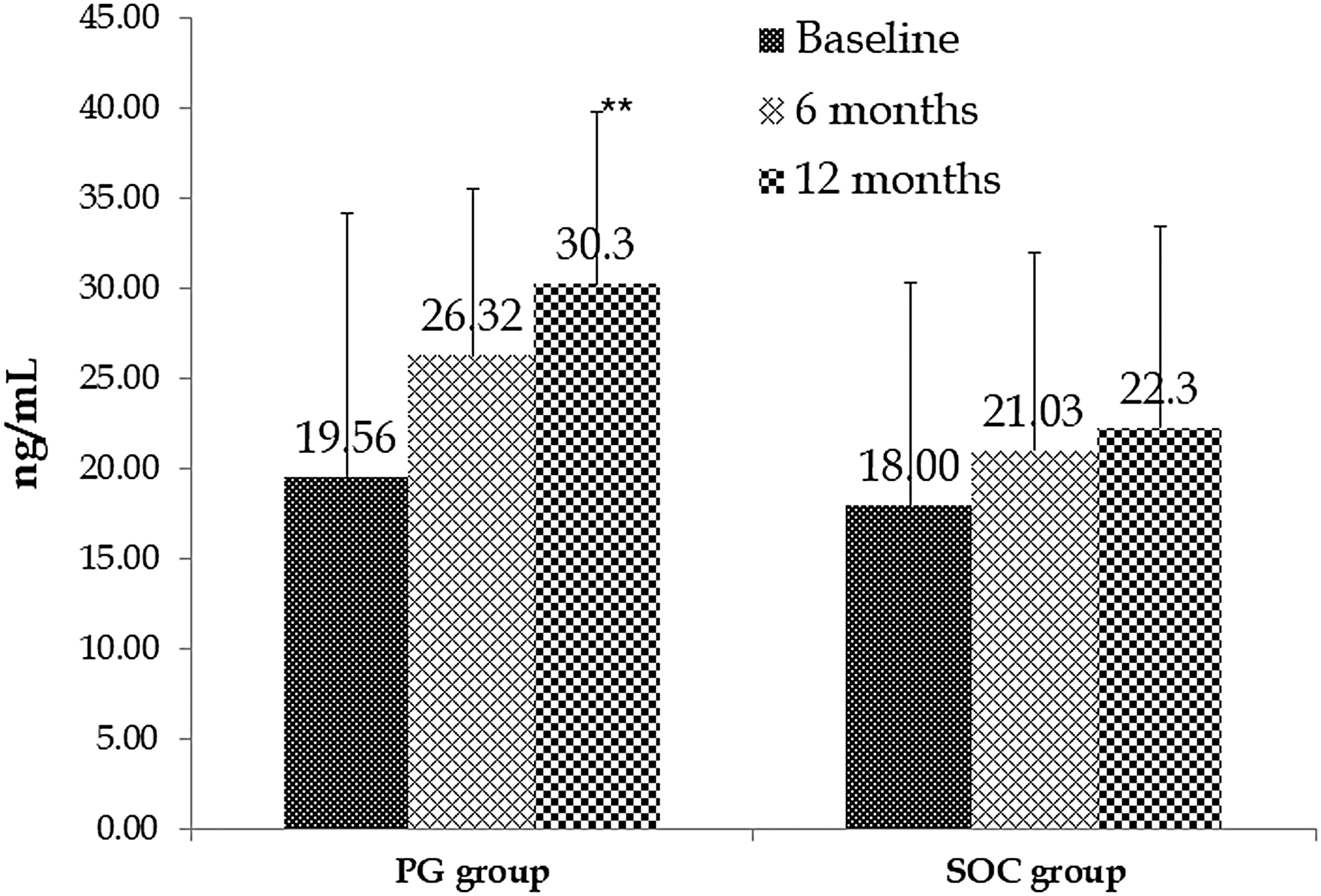
Serum vitamin D3 levels in both the study groups. Results are expressed as mean ± SD; **p < 0.01 compared with baseline values (ANOVA with the Tukey–Kramer multiple comparisons test). ANOVA, analysis of variance; SD, standard deviation.
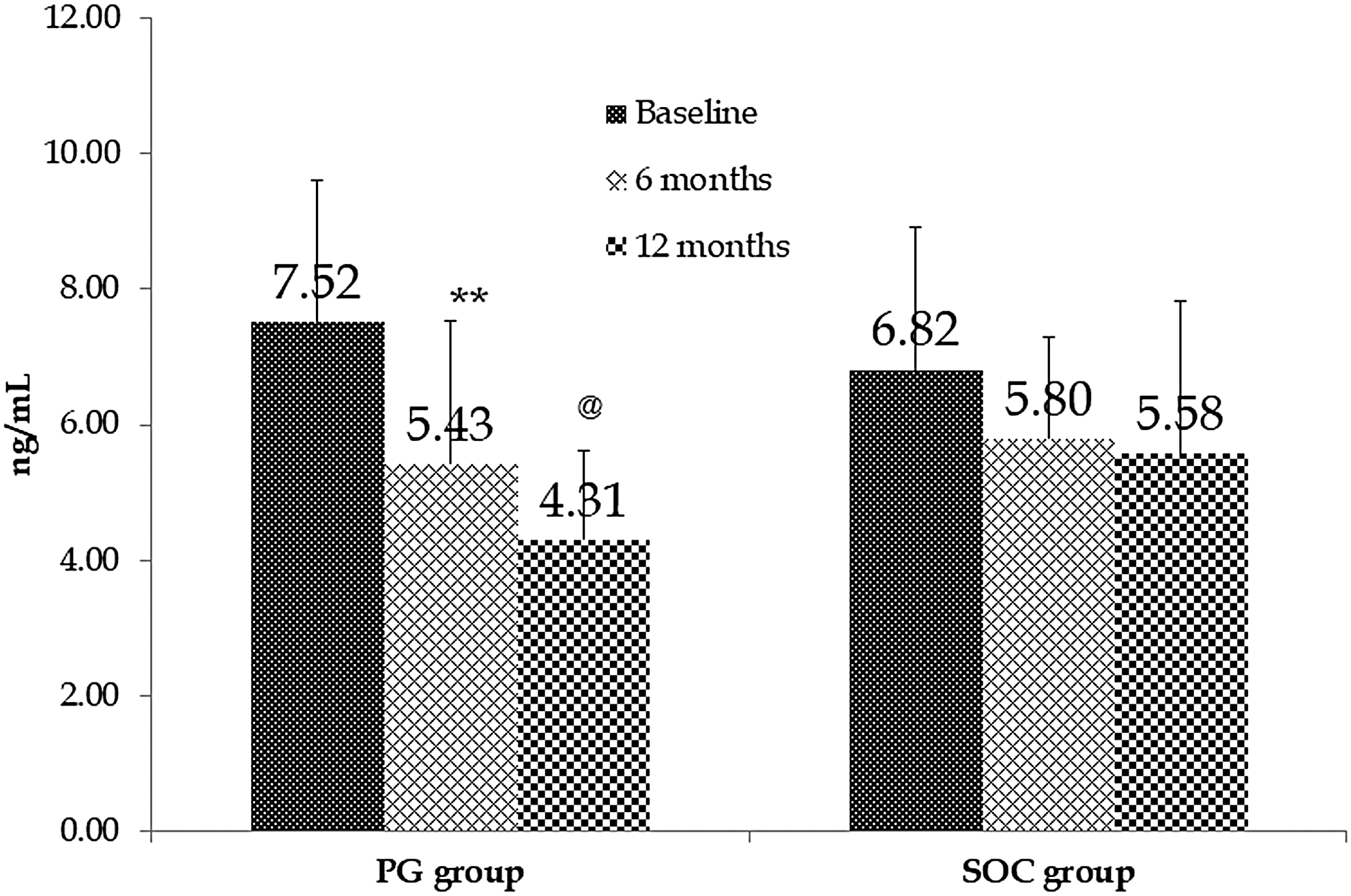
Serum osteocalcin levels in both the study groups. Results are expressed as mean ± SD; **p < 0.01 compared with baseline values (ANOVA with the Tukey–Kramer multiple comparisons test); @ p < 0.05 at 12 months compared with the SOC group (unpaired t test). ANOVA, analysis of variance; SD, standard deviation; SOC, standard of care.

Serum TRAP-5b levels in both the study groups. Results are expressed as mean ± SD; *p < 0.05 compared with baseline values (ANOVA with the Tukey–Kramer multiple comparisons test); @ p < 0.001 at 12 months compared with the SOC group (unpaired t test). ANOVA, analysis of variance; SD, standard deviation; SOC, standard of care; TRAP-5b, tartrate-resistant acid phosphatase 5b.
Using the FRAX tool, the MOFR (%) and the HFR (%) were calculated for the study patients at baseline, and whether the study medications offered any improvement in the scores at 6 and 12 months was also assessed. A decrease in the MOFR and the HFR was observed in both the groups following medication; however, the fall in the scores was significantly higher in the group receiving PG at the end of 12 months of treatment (Tables 4 and 5).
Major Osteoporotic Fracture Risk (%) in Both the Study Groups
Results are expressed as mean ± SD (95% confidence interval).
* p < 0.05 and ** p < 0.01 compared with baseline values (Friedman's test followed by Dunn's multiple comparisons test).
MOFR, major osteoporotic fracture risk; PG, Panchatikta Ghrita; SD, standard deviation; SOC, standard of care.
Hip Fracture Risk (%) in Both the Study Groups
Results are expressed as mean ± SD (95% confidence interval)
p < 0.05 compared with baseline values (Friedman's test followed by Dunn's multiple comparisons test).
HFR, hip fracture risk; PG, Panchatikta Ghrita; SD, standard deviation; SOC, standard of care.
An improvement in the quality of life and Ayurvedic symptoms score (Asthikshaya Lakshanas) was observed at the end of 6 and 12 months in both the groups; however, the fall in both the scores was higher in the PG group compared with the SOC group, although not statistically significant (Fig. 6 and Table 6, respectively).
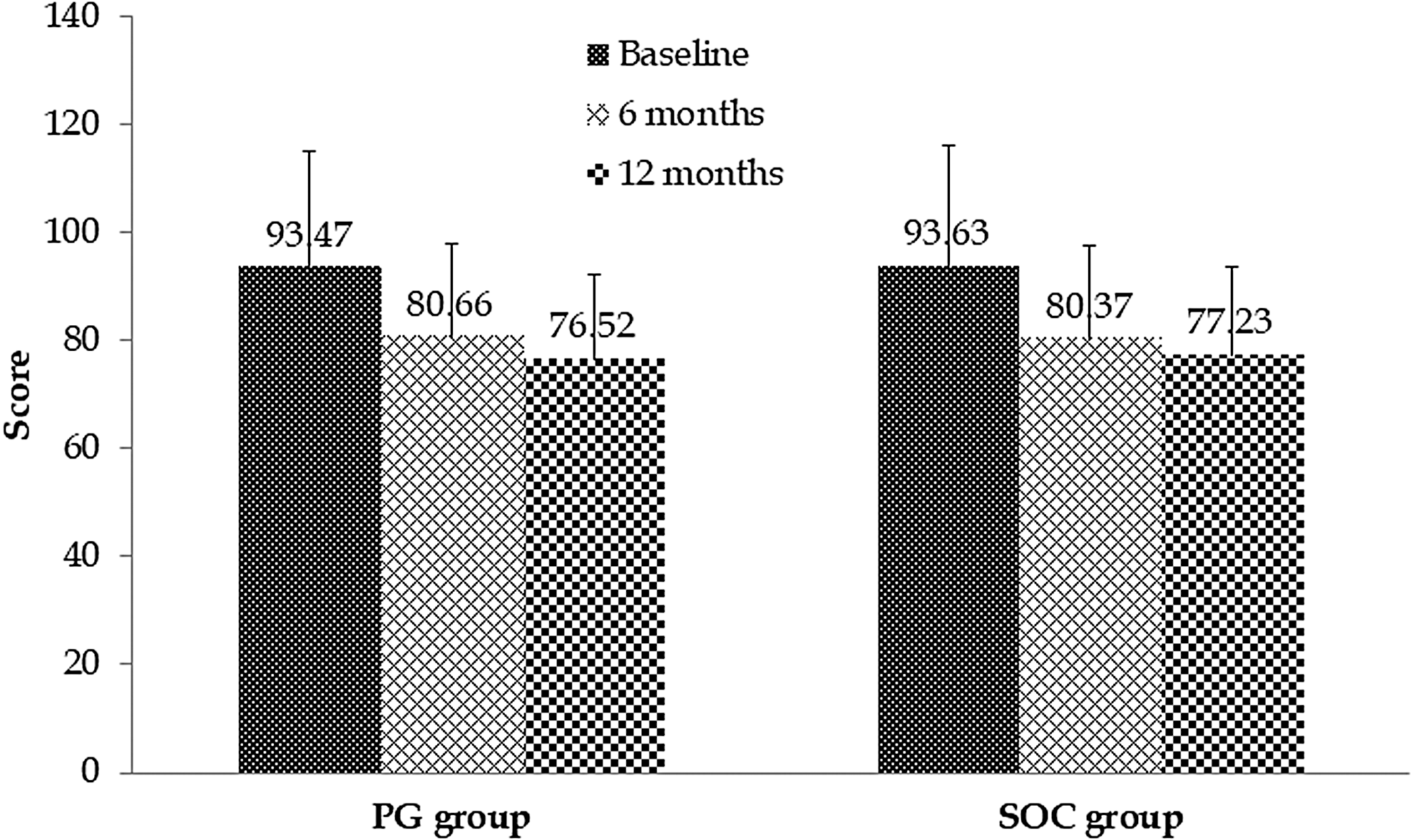
Effect on quality of life (QUALEFFO-41) in both the study groups. Results are expressed as mean ± SD. SD, standard deviation.
Effect on Ayurvedic Symptoms Score (Asthikshaya Lakshanas)
Results are expressed as mean ± SD.
PG, Panchatikta Ghrita; SD, standard deviation; SOC, standard of care.
Safety assessment
No serious adverse events were reported. Two patients in the PG group developed skin-related reactions during the study and dropped out from the study. One adverse event (chest pain) was reported in a patient from the SOC group in the third month, which was unrelated to the study medications; however, the patient withdrew consent to participate further. One patient in the SOC group complained of repeated episodes of constipation and hence withdrew consent for further participation. With regard to the laboratory tests, there was no significant change in any of the laboratory parameters over the study duration.
Discussion
Osteoporosis is characterized by low bone mass, with microanatomical deterioration of bone tissue leading to bone fragility, thus increasing the susceptibility to fracture. Although exact numbers are not available, based on available data, 25 million Indians may be affected with osteoporosis. 28 Bone fractures due to osteopenia and osteoporosis are a common occurrence resulting in increased morbidity and mortality. 29,30 Postmenopausal osteoporosis is becoming a major public health problem in India. This health issue in India is different from the rest of the world as normative index of Indian women is lower compared with their Western counterparts. 31 Indian women are also frequently deficient in vitamin D, which is essential for positive bone metabolism. 32 This emphasizes the need for early screening of osteoporosis and early identification of high-risk groups so that early initiation of treatment can be achieved. Nutritional status and dietary calcium intake directly related to BMD have been found in India. 3
DEXA scan is the most acceptable modality worldwide for the diagnosis and quantification of osteoporosis. In India, however, it is expensive and not widely available, and hence, population screening of all high-risk women is difficult. The use of bone-specific biomarkers can give clue of bone density and can be utilized for screening of osteoporosis, and it can also be utilized to monitor the success in treatment. Baseline measurements of resorption markers are useful before the commencement of antiresorptive treatment and can be checked at regular intervals to monitor response and adherence to treatment. 33,34
Calcium and vitamin D intake plays an important role in determining bone health. Studies by different authors have shown that healthy lifestyle (diet, exercise, and sunlight exposure) can have a major positive impact on the bone metabolism and bone health. Pharmacological interventions are expensive and should therefore be targeted to those individuals who are at high risk of fractures. 28,35,36
Despite the availability of various pharmacological agents to manage osteoporosis, the disease prevalence is still rising. Some of the reasons are as follows: (1) underdiagnosis of osteopenia/osteoporosis, (2) lack of clarity of the effectiveness of therapy on fracture prevention, (3) optimal duration of bisphosphonate treatment, and (4) risk of adverse effects seen with these agents with long-term therapy. In such situations, preventive treatment with Traditional systems of medicine can offer hope to patients, wherein the major risk of fractures in osteoporosis can be avoided.
In Ayurveda, there is no direct reference of osteoporosis or osteopenia, but the condition can be correlated with different diseases mentioned in Ayurveda, such as Asthidhatukshaya, 26 Asthi-Majjakshaya, 37 and vatavyadhi. In Ayurveda, polyherbal formulations are generally used in the therapy of Asthi kshaya wherein the combination of different plant drugs provides a synergistic therapeutic effect due to their differing properties and also helps minimize the adverse effects seen with modern medicine. As per Ayurveda, Vata disorders are generally found in the older age group with deterioration of the tissues (dhatus) present in the body. Vata dosha is one of the important factors in bone-related (Asthi) diseases as there is a unique relationship between Vata and Asthi. 17 Hence, mitigation of the deranged vata dosha at an earlier stage, that is, osteopenia (Asthikshaya), is recommended.
PG formulation contains plants, such as Azadirachta indica (Nimba), Trichosanthes dioica (Patola), Solanum xanthocarpum (Kantakari), Tinospora cordifolia (Guduchi), and Adhatoda vasica (Vasa), which have primarily katu (pungent) properties along with tikta (bitter) properties that are helpful in slowing down the degeneration processes. 38 Based on the properties of these five plants, the name Panchatikta has been given to the formulation. The Ghrita present in the formulation acts as a carrier for these herbs to reach the level of the bones to exert a maximum effect. 20 The formulation was administered with milk for two reasons—first, milk helps in combating the vitiated vata dosha seen in osteopenia, and second, to improve the palatability of the formulation. 20 Extracts or fractions of some of these plants, such as A. indica (Nimba), 39 S. xanthocarpum (Kantakari), 40 and T. cordifolia (Guduchi), 41 have also been shown to promote osteoblast differentiation and mineralization in experimental studies.
Previous experimental studies of the authors showed that PG has an antiosteoporotic effect on both the glucocorticoid-induced osteoporosis rat model and ovariectomized rat models of osteoporosis. 42 A significant decrease in the number of osteoclasts and an increase in bone hardness and elasticity and improvement in bone-specific marker levels were observed in rats treated with PG compared with diseased group, with results being similar to that observed with alendronate. Hence, the clinical study was planned to assess its effectiveness in the clinical settings.
In this clinical study, it was observed that 85% of patients belonged to the older age group (>50 years) with the male:female ratio around 1:5. This is probably due to the fact that the rate of bone resorption increases after the age of 50 years in both genders and is more in women due to postmenopausal hormonal imbalance. 43 In Ayurveda, it is considered that the derangement (mandta) of the metabolic activity (agni) of bone tissue (asthi dhatu), that is, dhatuagnimandta is higher in the elderly population, which results in decrease in bone formation resulting in osteopenia (asthikshya). 47 A look at the Prakriti distribution of the study participants showed a predominance of Kaphapradhan and Vatapradhan prakriti in the osteopenic condition. These findings are similar to that observed by Kukade et al. wherein they observed a predominance of Vatapradhan prakriti in patients with osteoporosis. 44 Although osteopenia is warranted to be predominant in Vatapradhan prakriti, in the present study, the authors found kapha pradhan prakriti (n = 37) in comparatively greater proportion than Vata prakriti (n = 25). An explanation for the same may be that the etiopathogenesis of Vata-related disorders (Vatavyadhi) is of two types, namely Dhatukshayajanya (vitiation of only Vata dosha) and Avarodhjanya (vitiation of both Vata and Kapha dosha). The present study probably had a larger number of participants with Avarodhjanya etiopathogenesis. Analysis of the outcome with respect to the Prakriti status of the participants was not performed when applying the intervention or during analysis as the sample size per Prakriti was small, and this was a limitation of the study.
Treatment with PG improved the BMD in these patients over 12 months, with a maximum improvement observed in the lumbar spine (17%) compared with the control group (6.65%). Although not statistically significant, the improvement in the BMD was persistent over a period of 12 months indicating a slowing of the degenerating process in the bone. This improvement was higher than that with the calcium and vitamin D supplements both in the present study and in previous studies. 45 –47 Long-term duration studies will, however, help confirm the positive trends seen in the BMD scores more effectively.
A look at the bone-specific biomarkers showed a significant increase in the serum vitamin D3 level compared with the baseline values (30.3 ng/mL vs. 19.56 ng/mL) in the PG-treated group at 12 months. The association between vitamin D3 and BMD is debatable, with some studies suggesting that a low serum vitamin D3 level is associated with low BMD, 48 –51 whereas other studies found that vitamin D and calcium supplementation was associated with small reductions in the rate of bone loss (0.54% at the hip and 1.19% at the lumbar spine). 52 In the present study, the authors did find a positive association between vitamin D3 levels and improvement in the BMD score in the PG group compared with the control group (although not significant) indicating that the formulation had a synergistic effect with vitamin D3 level, which may help in the prevention of falls and fractures.
Osteocalcin is a small protein synthesized by mature osteoblasts and plays an important role in bone formation. Serum osteocalcin has been considered a specific biomarker of osteoblast function for evaluation of bone formation rate in osteoporosis. Raised osteocalcin levels are associated with increased activity of osteoblasts, indicating increased bone turnover. 53,54
TRAP-5b is normally secreted by osteoclasts during bone resorption and is thus used as a reference for osteoclast activity. It has high specificity and sensitivity in comparison with other bone biomarkers and hence is frequently used as a bone resorption biomarker. 55,56
Thus, the authors measured the levels of these two biomarkers to assess the effect of the formulation on bone turnover, which would in turn provide us with a dynamic measure of bone remodeling. The authors found a significant reduction in both serum osteocalcin and TRAP-5b levels compared with the baseline values in the PG-treated group. This fall indicating a decrease in bone turnover was higher than that with calcium and vitamin D3 supplements alone.
These results were similar to that observed in other diet-based studies, wherein consumption of vitamin D- and calcium-fortified soft white cheese, 57 dried plums, 58 or soy products 59 showed a lowering of the bone biomarker levels earlier than the improvement in the BMD.
Thus, to conclude, the findings of this study demonstrate that PG, when given as add-on therapy to calcium and vitamin D3 supplementation, does slowdown the bone degeneration processes as seen by its stabilizing effect on the bone-specific biomarkers, indicating its potential usefulness as preventive therapy in osteopenia. The bone-stabilizing effects of the formulation also lead to a reduction in the risk of major osteoporotic fractures and an improvement in the quality-of-life scores including the Ayurvedic symptom score over a period of 1 year. Thus, consuming this formulation may help the osteopenic patients by preventing the progression to osteoporosis. Further evaluation of this formulation as a long-term preventive therapy treatment (2–5 years) may be required to validate its effectiveness in osteopenia.
Footnotes
Acknowledgment
The authors acknowledge the technical support provided by Dr. Ashwini Mhamane, Ms. Deepali Ganachari and Ms. Sonam Shinde during the conduct of the study.
Author Disclosure Statement
No competing financial interests exist. The Department of AYUSH, Government of India had no involvement in the data analysis, interpretation, or reporting of the results of this research.
Funding Information
The study was conducted with financial support from the Department of AYUSH, Government of India.
Supplementary Material
Supplementary Appendix SA1
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.