
Abstract
Objectives:
Falls are common in Parkinson's disease (PD). Exercise interventions can prevent falls. This review aims to (1) explore the existing evidence regarding the cost-effectiveness of exercise-based fall prevention programs for people with PD and (2) discuss the implications of the review findings for future research and clinical practice.
Design:
Databases AMED Allied and Complementary Medicine, CINAHL, CRD, EBSCO, EMBASE, MEDLINE, PubMed, Scopus, and Web of Science were searched from their inception until June 2019. Randomized and nonrandomized trials that included an economic evaluation of fall prevention programs for people with PD were considered. Quality of the economic evaluation was assessed using the Consensus on Health Economic Criteria list (CHEC-list), and the methodological quality was assessed using the Physiotherapy Evidence Database (PEDro) and Cochrane risk of bias tool.
Results:
Nine hundred and sixty-five studies were screened to include three studies involving 556 participants. Quality of economic evaluation assessed using CHEC-list was high. The methodological quality was high for two studies and low for one study. Tested interventions included Tai Ji Quan, physiotherapist-led, supervised, weekly and monthly balance, and strengthening exercises. The duration of the interventions ranged from 10 weeks to 6 months, while the intervention frequency ranged from two sessions per week to one session per month. Treatment sessions lasted for 60 min in all three studies. One high economic and methodological quality study comparing Tai Ji Quan with resistance and stretching exercises reported least cost resource use among Tai Ji Quan group (USD 80,441) and greater incremental number of falls prevented. All three tested interventions had an 80% probability of being cost-effective with the corresponding country-specific threshold incremental cost-effectiveness ratio values.
Conclusions:
The findings provide some evidence for exercise-based intervention as a cost-effective treatment option for preventing falls in PD; however, due to the limited number of available studies, heterogeneity of the interventions, and diversity of assessment settings, a firm conclusion cannot be established. Additional studies evaluating the cost-effectiveness of fall prevention programs involving larger samples and using different treatment parameters in various settings are warranted.
Introduction
Parkinson's disease (PD) is a complex neurodegenerative disorder that results in a spectrum of complications for both the individual and their families. 1 Approximately 13,000 (0.186%) people in Hong Kong and 0.2% of people worldwide have PD. 2,3 Major motor symptoms of PD, including hypokinesia, rigidity, resting tremor, postural instability, shuffling, and freezing of gait progressively affect balance, restrict mobility, and eventually increase the risk of falls. 4,5 Apart from motor impairments, PD can also affect cognitive function and mood. 6 Cognitive impairments such as poor selective attention is related to increased postural instability and frequent falls. A recent systematic review reported that 35% to 90% of people with PD fall at least once after being diagnosed with PD, with an average fall rate of 61% with 39% of all falls being recurrent. 7
Falls are considered to be the most severe complication of PD as they can lead to injuries, depression, fear of falling, morbidity, and even mortality. 8 These complications can severely affect the ability to perform activities of daily living, quality of life, and the life expectancy among people with PD. 9 In addition, studies have shown that PD is costly for the individual, their caregivers, the health care system, and the society in terms of social and economic burden. 10,11 Falls incur both direct and indirect costs, including costs of health care service utilization, sustained productivity losses, and affect the quality of life of the caregivers. 12 The economic burden due to hospitalization is substantially high at 20% or more of the annual cost for PD in the United States 13 and the United Kingdom. 14 In China, the economic burden per PD patient was estimated at US$3,225.94 annually. 15 There is an urgent need to implement effective fall prevention programs that are cost-effective among people with PD.
There have been an increasing number of studies investigating the effects of different exercises and pharmacologic-based fall prevention strategies in people with PD. A recent meta-analysis reported that exercise programs can improve gait performance and balance and reduce the rate of fall over the short- and long terms in people with PD. 16 However, few studies have investigated the cost-effectiveness of such fall prevention programs. Moreover, to their knowledge, no systematic review of these studies has been carried out. Fall prevention programs for PD may incur significant costs (e.g., in terms of staff, equipment, and treatment expenses) to the providers, individuals, and caregivers. By conducting a cost-effectiveness analysis, one can capture both the benefits and costs of an intervention in one comparable unit. A cost-effective analysis can also provide information, including (but not restricted to) the cost per fall prevented, the cost per extra person avoiding mobility deterioration, and the cost per quality-adjusted life-year (QALY) gained. In this study, the authors sought to perform a systematic review to (1) identify the existing evidence evaluating the cost-effectiveness of exercise-based fall prevention programs for people with PD and (2) discuss the implications of the review findings for future research and clinical practice on cost-effective exercise-based fall prevention programs for people with PD.
Materials and Methods
This systematic review is presented in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA; Appendix A1) guidelines. 17 The study protocol was registered in the PROSPERO International Prospective Register of Systematic Reviews (Registration No: CRD42018105296) before data collection began. The following electronic databases were then searched from database inception until June 2019: AMED Allied and Complementary Medicine, CINAHL, CRD, EBSCO, EMBASE, MEDLINE, PubMed, Scopus, and Web of Science. The search terms were constructed as three main themes: cost-effectiveness, falls, and PD. Related and similar terms for each theme were combined using “OR,” and the search themes were combined using “AND.” The search strategy for Medline database is reported in Appendix A2.
Randomized controlled trials (RCTs) and nonrandomized trials evaluating the cost-effectiveness of exercise-based fall prevention programs among people with PD were included in this systematic review. To be included, the fall prevention intervention had to have been: (1) delivered or supervised by a physiotherapist or an instructor, (2) provided to individuals with PD, and (3) an exercise-based intervention. In addition, the study must have included cost-effectiveness or cost-utility outcomes. Studies were excluded if they were: (1) study protocols, (2) conference abstracts since these do not provide details of the cost-effectiveness analysis, and (3) published in a language other than English. The outcome measures for this systematic review were the QALY and the incremental cost-effectiveness ratio (ICER).
Two reviewers (L.F.P. and L.K.L.) independently screened the titles, abstracts, and full texts of the retrieved studies using the eligibility criteria. Discrepancies were resolved by discussion, and a third reviewer (S.W.) was consulted for any unresolved discrepancies. The following information was extracted from the included studies: author name(s), country and year of publication, characteristics of the target population, sample size, type of intervention and comparator, study perspective, cost data, economic outcome measure, discounting, currency, and author's conclusions. The data extraction that was conducted by two authors (L.F.P., L.K.L.) were checked for consistency.
The Consensus on Health Economic Criteria list (CHEC-list), 18 Physiotherapy Evidence Database (PEDro) scale, 19 and the Cochrane risk of bias tool were used to assess the quality of the studies included in this systematic review. The CHEC-list is an appraisal tool for rating the quality of the economic evaluation. The scale includes 19 items that assess the internal and external validity of an economic evaluation study. Each item is scored “yes” or “no.” The CHEC-list allows measurement and comparison of the quality of economic evaluations among studies in systematic reviews. 18,20
The PEDro scale and the Cochrane risk of bias tool were used to assess the methodological quality of the included studies. The PEDro consists of 11 items relevant to the methodological quality of RCTs. The scale has been found to be valid and reliable in assessing the methodological quality of RCTs. The methodological quality of the included studies was interpreted as “high” if it scored six or more points and “low” if it scored five points or lesser. 21 The Cochrane risk of bias tool has seven items that assess the methodological quality of included studies. The items of the Cochrane risk of bias tool cover all the fundamental bias in a RCT. 22 The quality appraisal using CHEC-list, PEDro, and the Cochrane risk of bias tool was completed by two independent reviewers (L.F.P., L.K.L.). Any disagreements were discussed until consensus was reached.
Results
The search identified 965 studies, of which 76 were duplicates. After screening the title, abstract, and full-text screening, three studies were included for this systematic review. 23 –25 The flow of the screening process is illustrated in Figure 1. Appendices A3 and A4 report the reasons for excluding studies following the abstract and full-text screening. All the included studies were published after 2012. The country of origin of the included studies were the United Kingdom, 23 United States, 24 and Australia. 25 The three studies recruited 556 people with PD. The sample size ranged from 130 to 231, and the mean age of the participants ranged from 68 to 71 years.

Flow of study search.
One study compared Tai Ji Quan exercise program with a resistance exercise program and stretching exercise program. 24 Tai Ji Quan, also known as t'ai chi, is a Chinese martial art. Tai Ji Quan originated in the village of Chenjiagou more than 300 years back. The evolution of Tai Ji Quan has led to the emergence of the five basic styles, including Chen, Yan, Wŭ, Wű, and Sun. 26 Tai Ji Quan is practiced around the world for its positive influence on physical and mental health. 26 The other two studies compared weekly 23 and monthly 25 physiotherapist-led balance and lower limb strengthening exercises with usual care. In terms of outcome measures, all three studies included the number of falls as the primary outcome and used indirect utility estimated QALYs as a secondary outcome. A summary of the characteristics of the included studies is presented in Table 1.
Summary of the Characteristics of the Included Studies (n = 3)
ICER, incremental cost-effectiveness ratio; PDQ-8, Parkinson's Disease Questionnaire-8; QALY, quality-adjusted life-year.
Quality of Assessment Using PEDro Scale
+, item is satisfied; −, item is not satisfied.
PED
Quality of Economic Evaluation According to CHEC-List
+, item is satisfied; −, item is not satisfied; CHEC-list, Consensus on Health Economic Criteria list; NA, not applicable.
The Summary of Cost and Cost-Effectiveness of the Studies
AUD, Australian Dollar; ICER, incremental cost-effectiveness ratio; N/A, not available; PDQ-8, Parkinson's Disease Questionnaire-8; QALYs, quality-adjusted life-years; USD, United State Dollar.
All the three included studies met 17 or more of the 19 items of the CHEC-list indicating high quality. None of the included studies had a follow-up longer than 12 months; therefore, item 14 of the CHEC-list on “Discounting” was rated “not applicable” (NA) across all three studies and was counted as one point. Two of the included studies did not discuss the generalizability of the study findings. 23,24 The methodological quality, according to the PEDro score, was high for two studies 24,25 and low for one study. 23 The Cochrane risk of bias assessment found a lack of blinding for both participants and personnel delivering intervention across all three studies. This risk is subject to the nature of research where blinding of the participants and study personnel is not possible. All three studies applied random allocation and between-group comparisons. The PEDro and CHEC-list scores of the included studies are reported in Tables 2 and 3. Figures 2 and 3 illustrate the methodological quality appraisal according to the Cochrane risk of bias tool.
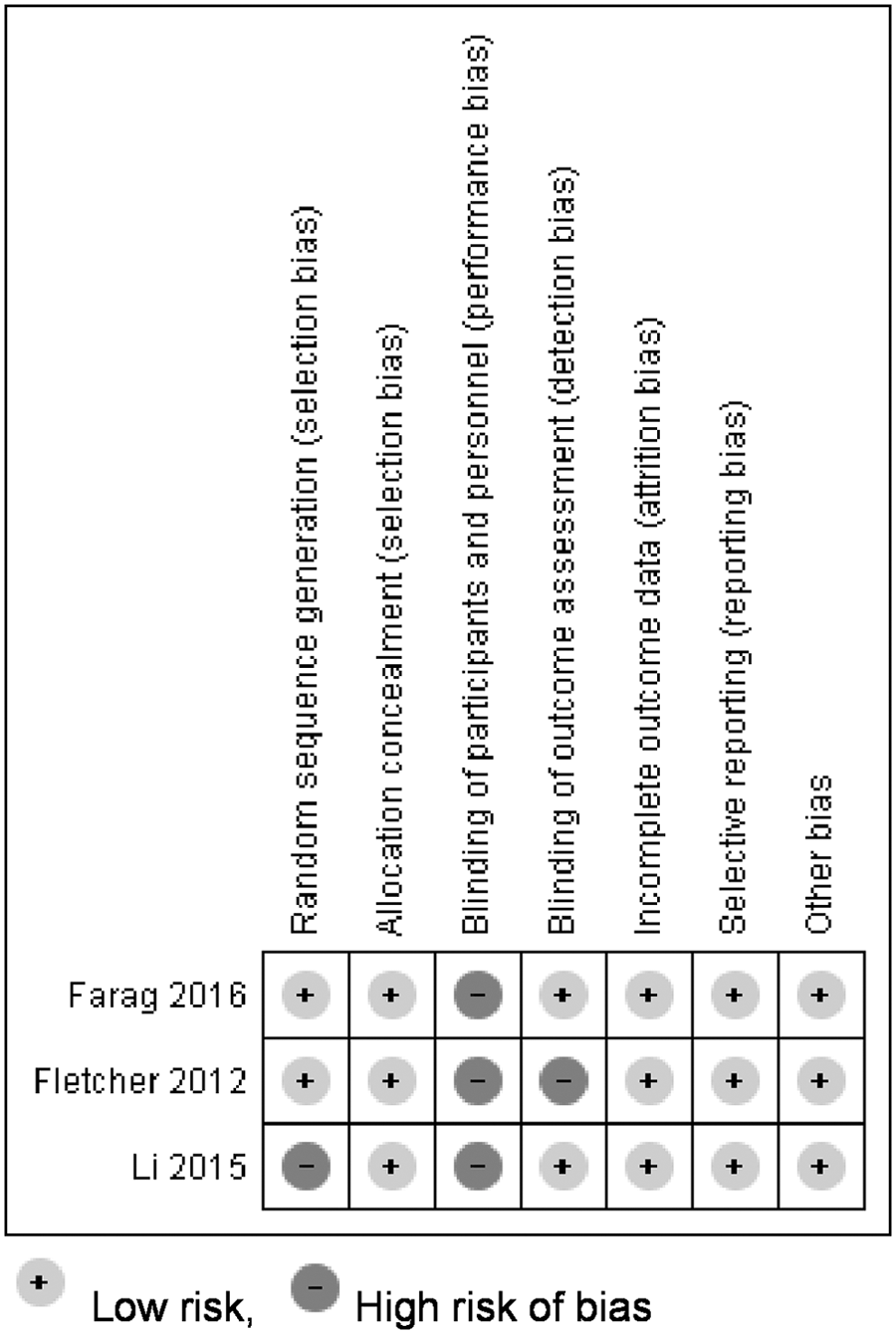
Cochrane risk of bias for all the included studies.
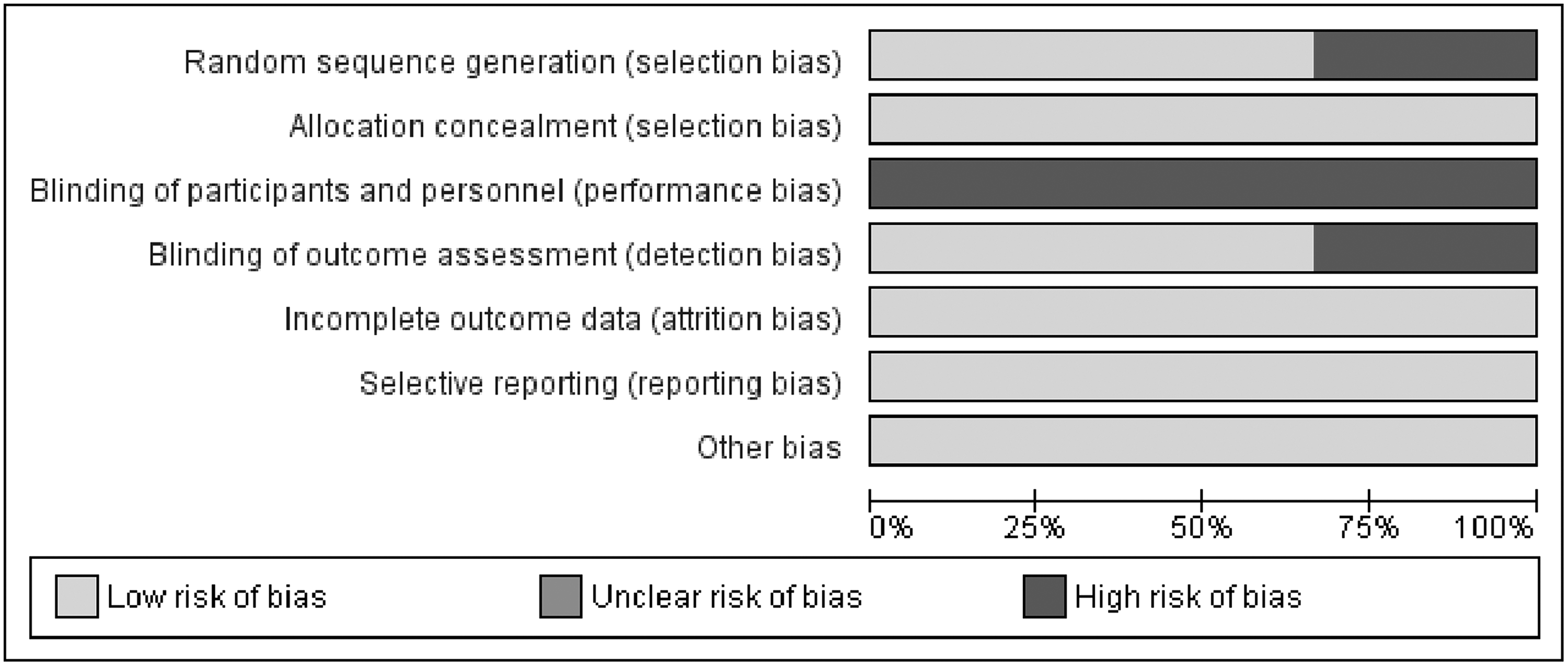
Summary of the methodological quality of the included studies according to the Cochrane risk of bias tool.
The duration of the interventions ranged from 10 weeks 23 to 6 months, 25 while the intervention frequency ranged from two sessions per week 23 to one session per month. 25 Treatment sessions lasted for 60 min in all three studies. The tested exercises included structured Tai Ji Quan sessions delivered by a certified t'ai chi trainer 24 and progressive tailored balance and strengthening exercises for the upper and lower limbs delivered by a physiotherapist. 23,25 All of the interventions were delivered in a community-based center followed by home practice, allowing the participants to perform unsupervised exercises. One study followed up with the participants at 10 weeks postintervention, 23 Li and Harmer conducted follow-up at 9 months postintervention, 24 and Farag et al. completed the final assessment after 6 months of intervention without a follow-up assessment. 25
Two studies considered the economic evaluation from a health care perspective, 24,25 and one study provided estimations based on both health care and societal perspectives. 23 Two studies used the EuroQol 5 Dimension (EQ-5D) 23,24 and one study used the Short-Form 6D (SF-6D) Scale 25 to estimate the QALY. All three studies reported the cost of delivering the intervention based on the cost of the program, venue, workshops for trainers, wages for the instructor(s), and participants' travel costs. The ICER, which is the ratio between the differential mean cost of the intervention to the difference in the QALY, was estimated using the cost of health care utilization, cost of medicines, and cost of intervention delivery. Among the studies reporting the cost-effectiveness from a health care perspective, one study comparing Tai Ji Quan against resistance and stretching exercise reported $3,394 (US$, 2011) per participant per additional QALY gained, 24 while the other study comparing monthly exercise sessions over 6 months for preventing falls against usual care reported A$338,800 (Australian $, 2012) per additional QALY gained. 25 One study conducting an economic evaluation from a societal perspective, comparing once-weekly exercises and twice-weekly balance training home exercises for 20 weeks against usual care, reported the ICER for health care cost as −£4,900 per QALY and −£1,400 per QALY for combined health care and social care cost. 23 The incremental cost-effectiveness of the fall prevention program in terms of the number of falls prevented was reported by two studies, both assessing cost-effectiveness from a health care perspective. 24,25 Six months of Tai Ji Quan training composed of two weekly sessions showed an average reduction of $175 (US$, 2011) 24 per additional fall prevented, and monthly exercise classes plus two to four home visits over 6 months resulted in a reduction of A$574 (Australian $, 2012) 25 per fall prevented. Regarding the net medical cost observed through the follow-up period, one study reported both direct (health care) and indirect (social) costs, 23 while two studies reported on direct costs alone. 24,25 Among the studies comparing exercise intervention against usual care, one reported a higher cost means in the intervention group (intervention group = A$634,436, control group = A$442,984, base year 2012, cost estimated for 24 weeks). 25 The authors indicated that the increased health care costs among the intervention group were due to a higher rate of hospital admissions in this group. The study by Fletcher et al. reported a lower overall cost means for the intervention group (acute health care: intervention group = £263, control group = £524 and primary health care: intervention group = £93, control group = £88, base year 2008/09 estimated for 20 weeks). However, the mean social cost was higher among the intervention group (intervention group = £252, control group = £159). 23 The increase in social cost among the intervention group was reported to be due to increased social and home care assessments. 23 The study comparing three interventions head-to-head reported that the lowest health care costs were among Tai Ji Quan participants (mean health care cost: Tai Ji Quan = $80,441, resistance training = $88,952, and stretching = $111,896, base year 2011, cost estimate for 54 months). The included studies reported that the tested interventions had an 80% probability of being cost-effective with the corresponding country-specific threshold ICER values (Aus $20,000 in Australia and £20,000 in the United Kingdom). A summary of the cost and cost-effectiveness of the studies included in the current review is listed in Table 4. All three studies reported that tested fall prevention programs were potentially cost-effective.
Discussion
This systematic review sought to evaluate evidence regarding the cost-effectiveness of exercise-based fall prevention programs for people with PD. Three studies were included in the review. The included studies provided some evidence for exercise-based intervention as a cost-effective treatment option for preventing falls in people with PD. The interventions tested were Tai Ji Quan 24 and community-based physiotherapist-led weekly and monthly balance, and strength training exercises. 23,25 The findings of this systematic review should be interpreted with caution as the tested interventions were found to be cost-effective only in the service providing country, for the setting(s) of the study, and the costs incurred for intervention delivery and medical expense for the patient during that period of the year. Transferring the findings of an economic evaluation across countries poses multiple challenges and discussing the methods for transferring the findings across jurisdiction is beyond the scope of this review. The authors refer to reviews published elsewhere for additional information on transferability of economic evaluation findings. 27,28
The type of exercises that the authors suggest are in line with the findings of systematic reviews on cost-effective exercise-based interventions for fall prevention among older adults 29,30 ; however, generalizing these findings to people with PD has some limitations. The American College of Sports Medicine recommends the use of cardiovascular exercises, neuromotor exercises, and exercises to improve flexibility and strength in people with PD. 31 Postural instability and poor balance are common and are worsened by the presence of nonmotor PD symptoms. During training, the emphasis is placed on exercises to improve postural stability, gait, and balance. 31 In addition, close supervision during exercise training is recommended when the individual has poor balance and cognitive impairments. 32 Therefore, exercise programs for people with PD need to be tailor-made and follow established guidelines. 31
Considering the costs of implementation and the benefits attained through fall prevention programs, Tai Ji Quan appears to be a favorable option. Tai Ji is a traditional Chinese martial art from ancient China. Tai Ji practice among the elderly is common in East Asian countries, and over the past decade, the technique has attracted international attention due to its health benefits. Tai Ji is thought to improve balance and prevent falls by facilitating an even weight distribution between the lower limbs, improve knee joint proprioception, and increasing the lower limb muscle strength. 33 Their previous review highlighted the significance of Tai Ji in preventing falls among people with PD. 21 The current review provides evidence for its cost-effectiveness. The lack of the need for direct supervision by an instructor once Tai Ji movements are learned, peer support during group practice sessions, and its adaptability of this martial art across different age groups make Tai Ji a suitable and appropriate leisure-based outdoor activity for preventing falls among people with PD.
Rising concerns regarding the optimal use of health care resources have resulted in an increase in cost-effectiveness analyses over the past decade. However, the present systematic review identified only three studies evaluating the cost-effectiveness of exercise-based fall prevention programs for people with PD. The results of this review provide an indication to the researchers, clinicians, and policy makers on conducting future research testing the cost-effectiveness of fall prevention programs among people with PD.
Their review search yielded one study that closely met their inclusion criteria; however, it was excluded as it was a conference abstract that did not provide detailed information on the study methodology and economic evaluation. The study was conducted in Australia and compared the effectiveness and cost-effectiveness of 40–60 min of progressive balance and strengthening exercises thrice per week for 6 months duration against usual care for preventing falls among people with PD. 34 The ICER of the exercise program was A$570 per fall prevented, and the intervention was found to have 80% probability of being cost-effective at the threshold of A$2,000 per fall prevented. That study concluded that the intervention was cost-effective in people with mild but not severe PD.
PD is a progressive disease, but none of the studies evaluated the cost-effectiveness of fall prevention programs in relation to PD severity. Falls occur most frequently in PD patients with Hoehn and Yahr stage III or higher. 35 Farag et al. 25 proposed that their exercise intervention was more cost-effective and effective for the low-disease severity subgroup. Due to variations in the clinical presentation of individuals with different disease severity, generalizing the available findings to all people with PD especially to those with severe PD is limited. Future studies should evaluate the outcome and cost-efficacy of treatment options for preventing falls among people who have a range of PD severities and determine the extent to which PD severity moderates the outcomes.
There are some limitations to the findings of this systematic review. First, the authors were not able to draw conclusions regarding the parameters for cost-effective fall prevention program due to the heterogeneity of the included studies in terms of the interventions, outcome measures, time horizon, and costs. In addition, the countries of origin of the included studies were restricted to the United Kingdom, United States, and Australia. Given country-specific differences in culture, economics, and health care policies, the results of the present review have limited generalizability to the countries in Asia and Africa. The significance and need for economic evaluations may be even higher in less developed countries due to the lack of resources, a lack of high-quality medical services, and the high demand for medical and rehabilitation services. Owing to the absence of a global threshold value for estimating cost-effectiveness, the World Health Organization recommends using of one of the following methods to estimate cost-effectiveness: (1) threshold based on per capita national income, (2) benchmark interventions, and (3) estimation using league tables. 36 Future economic evaluation studies on exercise-based fall prevention programs are warranted in Asian and African countries. Second, this review excluded conference abstracts. It is possible that some findings regarding the cost-effectiveness of fall prevention programs were missed. Third and more importantly, the authors restricted their inclusion of economic evaluations to prospective randomized and nonrandomized trials. Although alternate methods of economic evaluation such as retrospective database analysis and decision-analytic modeling are available, 37 economic evaluation piggy-backed on prospective and randomized trials are considered as more valid and scientific evidence for economic evaluation in health care. 38 Based on the good quality evidence for the cost-effectiveness of fall prevention programs in people with PD, the search yielded only three studies. Considering the limited number of economic studies on fall prevention in this population, future reviews are recommended to include all designs of economic evaluations. Finally, due to the heterogeneity of the studies in terms of the interventions, country of origin, outcome measures, and included costs, the authors were unable to conduct a meta-analysis.
Despite the study's limitations, this is the first systematic review to evaluate the cost-effectiveness of fall prevention programs for people with PD. Strengths of this systematic review include: (1) use of a comprehensive and detailed search strategy to identify studies on cost-effectiveness of exercise-based interventions for preventing falls among people with PD; (2) being comprehensive, as it included all studies from the date of inception of relevant databases; and (3) using standardized appraisal tools for rating a study's methodological quality and the quality of its economic evaluation.
Conclusion
This systematic review provides some evidence to support exercise-based interventions as a cost-effective treatment option for preventing falls among people with PD. Three studies of high CHEC-list quality and low to high PEDro quality reported that Tai Ji Quan and community-based physiotherapist led lower limb strengthening and stretching exercises are potentially cost-effective in preventing falls for people with PD. Additional studies, including samples of people with a range of PD severity, and in a variety of different countries, including Asia and Africa, as well as additional studies in Australasia, America, and Europe, are warranted to help determine the role that PD severity plays in moderating the efficacy of these treatments and to assess the generalizability of the findings of this review.
Footnotes
Acknowledgments
Review registration: PROSPERO 2018 CRD42018105296.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Start-up fund for early career, The Hong Kong Polytechnic University, Hong Kong.
Appendix