
Abstract
Objectives:
In this pilot study, the effect of 970 mg Chi-Ju-Di-Huang-Wan (CJDHW) plus 30 mg four-substance decoction (Si Wu Tang; CJDHWSWT) was evaluated, in terms of its ability to alleviate dry eye symptoms and its therapeutic mechanism.
Methods:
This double-masked prospective investigation has recruited dry eye patients who have been randomly selected into two groups, namely treatment (n = 15) versus nontreatment (n = 15). In the treatment group, a daily oral intake of CJDHWSWT plus eye drops systane ultra was given for 90 consecutive days. In the nontreatment group, only defined eye drops were prescribed. The examinations included Schirmer's test, fluorescein-stained superficial punctate keratitis (SPK), artificial tear consumption, tear vascular endothelium growth factor (VEGF) level, and ocular surface disease index. The drug safety tests included liver and kidney functions, and complete blood counts. The candidates were observed during the screening visit and the following three monthly follow-ups. The data were analyzed by unpaired Student's t-test.
Results:
Compared to no significance in the nontreatment group, CJDHWSWT significantly (p = 0.03) increased the tear secretion after 3 months of intake. Furthermore, in contrast to no significance in the treatment group, there were significant alterations, including (i) increased fluorescein-stained SPK areas (p = 0.03); (ii) increased artificial tear instillation amount (p = 0.03); (iii) elevated tear VEGF protein levels (p = 0.03) in the nontreatment group; and (iv) significant improvement in clinically relevant phenomenon (e.g., reading limit and uncomfortable feeling in windy conditions), after treatment of artificial tear plus oral intake of CJDHWSWT. As shown by the post-treatment normal defined laboratory data, there were no adverse drug effects.
Conclusions:
This study has supported that CJDHWSWT is safe and effective in relieving dry eye's clinically relevant symptoms/phenomena. CJDHWSWT avoided the tear VEGF upregulation probably induced by dry eye-associated hypoxia/ischemia.
Introduction
Tear insufficiency or over evaporation might lead to dry eye. Lipid and mucus are other components of tear film. In symptomatic dry eye, the patients might have the following complaints. These include dry eye sensation, tearing at a windy/dry/air-conditioned atmosphere, photosensitivity, gritty, eye soreness/pain, itchiness and feeling of a burn. There are also others, namely blurred vision, visual field constriction, and difficulty at reading/driving/watching. Around 7 to 10 million of Americans are in need of artificial eye drops or ointment, with medical expense more than US$100 million annually. 1,2 Anyhow, dry eye irritation could just be alleviated by the defined supplements, or, currently, a punctal plug to maintain the ocular surface moisture or reduce the tear passage for a short period. 3 Dry eye is related to prolonged inflammatory status of the lacrimal system, including gland, conjunctival goblet cell or mebomian gland that might injure the cornea, conjunctiva, or eye lid. Thus, there might be therapeutic effects from the following agents, namely steroids, nonsteroid anti-inflammatory drugs, or cyclosporine. 3 Dietary nutrients such as antioxidant astaxanthin or systemic omega-3 have been demonstrated to be effective in dry eye with the pathogenic influences in the mentioned lacrimal system. 4,5 Tear film supplies oxygen to the avascular cornea and removes its metabolic wastes. In other words, tear insufficiency (dry eye) might lead to ocular hypoxia/ischemia. Ischemia is associated with reactive oxygen species production and vascular endothelium growth factor (VEGF) upregulation. 6,7 These subsequently lead to an oxidative stress, which might be detrimental to the defined lacrimal system or adjacent ocular tissues. 5 These also included corneal neovascularization, superficial punctate keratitis (SPK), tear aqueous insufficiency, and so on.
Chi-Ju-Di-Huang-Wan (CJDHW) is composed of Lycii Fructus (Gou qi zi), Chrysanthemi Flos (Ju hua), both containing antioxidants zeaxanthin and lutein, 8 and Rehmanniae Radix Preparata (Shu di huang), including disaccharide trehalose 9 and glucoside catapol, 10 as well as five other components. Lycii Fructus possesses Lycium barbarum polysaccharide that has effects on animal models of retinal disease (e.g., ischemia/reperfusion) acting by mechanisms, namely antioxidation, vasomodulation, neuroprotection, and immunomodulation. 11,12 Trehalose has been reported to be an osomoprotectant compatible solute in artificial tear drops, which stabilizes the peptide bond to allow proper folding, despite negative changes in temperature and pressure. 13 Furthermore, the two main components, Dāngguī and Chuān Xiōng, of Si Wu Tang (SWT) contain the active composition ferulic acid. 14 Ferulic acid is able to protect against retinal ischemia by acting as a free radical scavenger. Moreover, SWT is widely accepted to have a vasomodulating effect. Therefore, a combination of Chi-Ju-Di-Huang-Wan plus Si Wu Tang (CJDHWSWT)'s active components was presently utilized to evaluate the integral effect of all these components on dry eye signs/symptoms associated with VEGF expression. Whether there would be any therapeutic effect or anti-VEGF mechanism of 970 mg CJDHW combined with 30 mg four-substance decoction (SWT; CJDHWSWT) on the dry eye was evaluated in this study. In this study, the 1 g of CJDHWSWT was prepared based on the amount (30 mg) of SWT derived from that of an active composition ferulic acid in another animal research. 14 Thus, this results in 970 mg of CJDHW being chosen for this experiment.
The investigation was carried out by the following parameters, namely best corrected visual acuity (BCVA), Schirmer's test, cornea fluorescein staining, the consumption of artificial tear, the enzyme-linked immunosorbent assay (ELISA) to measure the level of VEGF in tears from the filter paper, and ocular surface disease index (OSDI). 15 The drug safety tests included liver/kidney functions, complete blood counts (CBC), and glucose levels.
Materials and Methods
Ethics
The masked pilot research was performed at the Cheng Hsin General Hospital (CHGH), Taipei, Taiwan. The Institutional Review Board at CHGH (CHGH-IRB; Approval No: (361)102-09) agreed this prospective research, which complied with the 1947 Nuremberg Code, the 1964 Declaration of Helsinki.
Patients
In this pilot investigation, the informed consents have been collected from the dry eye patients who have undergone clinical screening and been randomly selected into two groups, namely treatment (n = 15; males:females = 4:11; age: 59.73 ± 6.73) versus nontreatment (n = 15; males:females = 3:12; age: 53.07 ± 6.55). In the treatment group, a daily oral intake of CJDHWSWT plus ocular instillation of systane ultra (Alcon Laboratories, TX) eye drops was given for 90 consecutive days. Compliance with taking the treatment of CJDHWSWT was monitored by querying the subjects at each visit. In the nontreatment group, only ocular instillation of defined eye drops was prescribed. In this study, nontreatment or treatment group should be more specifically defined as nontreatment or treatment of CHDHWSWT, but without a prohibition of the use of the artificial tear, Systane. This study is somewhat similar to a recent experimental design 16 ; Systane Ultra has been also used as an adjunct treatment in that study of Optimel Eye Drops (Melcare, Australia), which improved symptoms of dry eye.
Evaluation methods and statistical analysis
The clinical screening included liver/kidney function tests and CBC. The examinations were mentioned above, including checking BCVA, Schirmer's test, cornea fluorescein staining, the consumption of artificial eye drops, and the ELISA for measuring the tear VEGF levels, as well as OSDI. Liver and kidney functions as well as CBC were also included in the drug safety evaluation. The candidates were followed up during the screening visit and every 4 weeks for 12 weeks. In other words, in addition to the screening visit, there were three monthly follow-ups (F/Us) after the daily intake of CJDHWSWT for each month. The data were expressed as mean ± standard deviation. The unpaired Student's t-test was utilized to analyze the data. A value of p < 0.05 was considered significant. Among 55 applicants, 25 unqualified ones were excluded and 30 candidates were recruited. Overall, there were no dropouts throughout the study.
Inclusion and exclusion
Inclusive criteria were listed as follows: between 20 and 78 years of age as well as defined dry eye symptoms. In addition, the three tests were included: basal Schirmer's test values with tear on the filter paper <5 mm at 5 min after use of topical 0.5% proparacaine anesthetics, 17 or one to nine areas of positive fluorescein-stained SPK in the total nine areas. 18 Furthermore, tears in the filter paper were evaluated for the protein levels of VEGF. Moreover, the 12-question OSDI questionnaire (with grade 0–4; the higher the mark, the poorer the life condition) was programmed to evaluate the patient's life condition. 15 The questionnaire includes the questions as follows: (A) Have you experienced any of the following symptoms during the last week: (1) Eyes that are sensitive to light? (2) Eyes that feels gritty? (3) Painful or sore eyes? (4) Blurred vision? (5) Poor vision? (B) Have your eyes limited you in performing any of the following activities during the last week: (6) Reading? (7) Driving at night? (8) Working with a computer or ATM? (9) Watching TV? C. Have your eyes felt uncomfortable in any of the following situations during the last week: (10) Windy conditions? (11) Places with low humidity (very dry)? (12) Areas that are air conditioned? As mentioned above, scores for answers are defined as 4 (all of the time), 3 (most of the time), 2 (half of the time), 1 (some of the time), and 0 (none of the time). The exclusive criteria included eye surgery/trauma 1 month before the screening visit, nasolacrimal duct obstruction, known hypersensitivity to or intake of CJDHW, SWT, or any other ingredient in either formula, pregnancy, breast feeding, and use of oral contraceptive drugs, menorrhagia, dysmenorrhea, uterine myoma, tumor (breast, ovary or uterus), peptic ulcer, constipation, hepatitis B/C, acquired immune deficiency disease, and any other systemic diseases (liver, kidney, blood, or cardiovascular). Within the research period, the intake of the following drugs or health food supplements was suggested to discontinue: any formula containing supplements of lutein, zeaxanthin, ginkgo biloba, vitamin A, or omega-3; topical azithromycin; steroids; cyclosporine A; pilocarpine eye drops; tetracycline ointment; oral tetracycline; doxycycline; and androgen supplements. This has been also monitored at each visit to determine that none of the prohibited items was used by candidates during this trial. Of note, electronic notifications were sent to patients on a weekly basis, as a reminder of their drug intake and the above-mentioned instructions/rules to abide by. Note all the candidates went on ordinary diet as usual without much change at this trial.
Enzyme-linked immunosorbent assay
Measurement of the level of VEGF
The level of VEGF was determined using ELISA. 19 The total protein present in each sample was determined using a bicinchoninic acid protein kit (Thermo Fisher Scientific). 20 The VEGF levels in the supernatant were measured with a VEGF-A ELISA kit (BMS277/2TEN human VEGF-A; eBioscience, Vienna, Austria) according to the manufacturer's instructions. An anti-human VEGF-A antibody had been previously coated onto microwells. After twice washing each well with 400 μL wash buffer within 15 min, the human VEGF-A present in the tear samples from the filter paper (1:5; 20 μL tear samples diluted in 80 μL sample diluent) or various concentrations of VEGF-A standard protein (100 μL; dissolved in distilled water) bind to the antibodies coating the microwells kept at room temperature for 2 h on a shaker (400 rpm). After twice washing each well with 400 μL wash buffer (phosphate-buffered saline [PBS] with 0.05% Tween 20 [PBST]), 100 μL biotin-conjugated anti-VEGF-A antibody (diluted in assay buffer: PBST and 0.5% bovine serum albumin) was added to each well for 1 h on a shaker (400 rpm) to bind to the VEGF-A captured by the coated antibody. After twice washing to remove unbound biotin-conjugated anti-VEGF-A, 100 μL streptavidin–horseradish peroxidase (HRP; diluted in assay buffer; 1:100) was added and bound to the biotin-conjugated anti-VEGF-A antibody on a shaker (400 rpm). Following 1-h incubation, the unbound streptavidin-HRP was removed after washing twice. Finally, 100 μL of 3,3′,5,5′-tetramethylbenzidine (100 μM) solution, which can be oxidized by HRP, was added to each well for 30 min. The color then changes to yellow with the addition of 100 μL stop solution (sulfuric acid solution, 100 μM). The maximum absorbance (optical density) at 450 nm was detected with a spectrophotometer (ELx800; Biotek) immediately. The VEGF concentration of each sample was determined by constructing a standard curve using various amounts of pure VEGF (1,000, 500, 250, 125, 62.5, 31.2, 15.6, and 0 pg/mL). The instrument was adjusted to zero with 100 μL sample diluent, which served as the blank. The results are expressed as an optical intensity relative to that of the control group (normalized to 100%).
Results
Schirmer test
At various time points (screening visit; first monthly follow-up [1st mon F/U]; second monthly follow-up [2nd mon F/U]; and third monthly follow-up [3rd mon F/U]), the Schirmer test-measured tear amounts (mm) of the CJDHWSWT treatment group in contrast to those of the nontreatment group were listed as follows (Fig. 1 and Table 1): 5.7 ± 3.3 versus 5.6 ± 2.7 (n = 15); 6.9 ± 3.8 (n = 15) versus 6.9 ± 3.3 (n = 14); 7.6 ± 5.1 (n = 14) versus 7.3 ± 4.4 (n = 13); and 10.2 ± 8.1 (n = 15) versus 7.3 ± 4.4 (n = 15). Compared to no significance in the nontreatment group, there was a significant (p = 0.03) increase in the tear secretion after 12 weeks of oral intakes of CJDHWSWT.
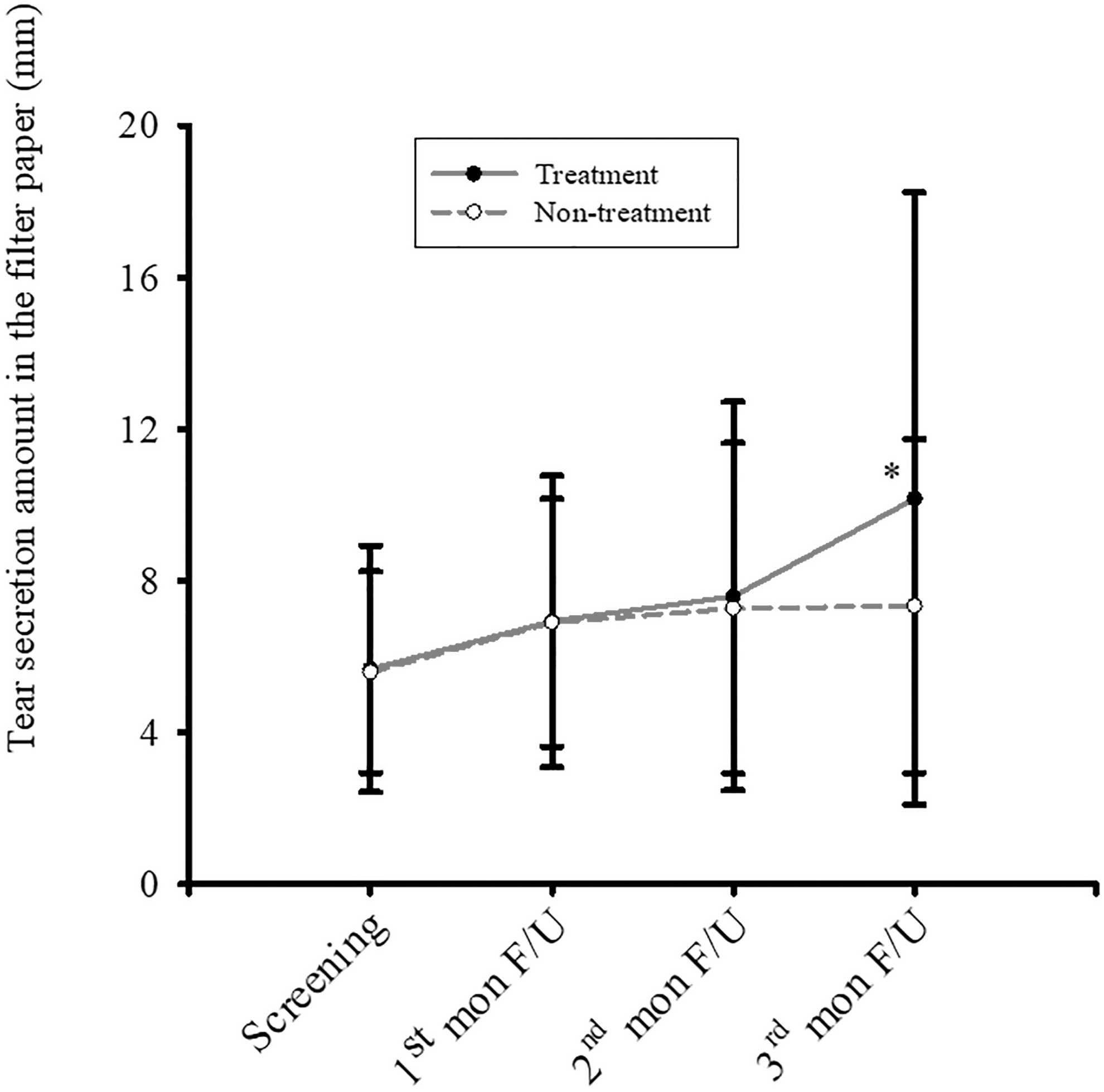
At different time points, as measured by the Schirmer's test, in contrast to no significant difference in the nontreatment group, the 3-month oral CJDHWSWT treatment appears to significantly (*p = 0.03) increase the basal tear secretion compared to the screening visit. The data were expressed as mean ± standard deviation. 1st mon F/U, first monthly follow-up; 2nd mon F/U, second monthly follow-up; 3rd mon F/U, third monthly follow-up; CJDHWSWT, Chi-Ju-Di-Huang-Wan plus Si Wu Tang.
Basal Tear Secretion Was Measured by the Schirmer's Test of the Nontreatment Versus Chi-Ju-Di-Huang-Wan Plus Si Wu Tang Treatment Group
The 3-month oral CJDHWSWT seems to significantly enhance the basal tear secretion compared to the screening visit. The data were expressed as mean ± standard deviation.
1st mon F/U, first monthly follow-up; 2nd mon F/U, second monthly follow-up; 3rd mon F/U, third monthly follow-up; CJDHWSWT, Chi-Ju-Di-Huang-Wan plus Si Wu Tang; Screen, screening visit.
Corneal fluorescein stain
At various time points (screening visit; 1st mon F/U; 2nd mon F/U; and 3rd mon F/U), the “areas” of positive fluorescein-stained SPK of the CJDHWSWT treatment group in contrast to those of the nontreatment group were listed as follows (Fig. 2 and Table 2): 3.7 ± 1.9 versus 2.7 ± 1.4 (n = 15); 4.1 ± 1.2 (n = 15) versus 3.5 ± 1.3 (n = 14); 3.8 ± 1.8 (n = 14) versus 4.3 ± 1.6 (n = 13); and 4.1 ± 1.8 (n = 15) versus 4.1 ± 1.8 (n = 15). Furthermore, in contrast to no significance in the treatment group after 12 weeks of oral intake of CJDHWSWT, compared to the initial areas of the fluorescein-stained SPK at the screening visit (2.7) in the nontreatment group, there were significantly more areas of fluorescein-stained SPK (p = 0.03; 4.1) in the defined nontreatment group.
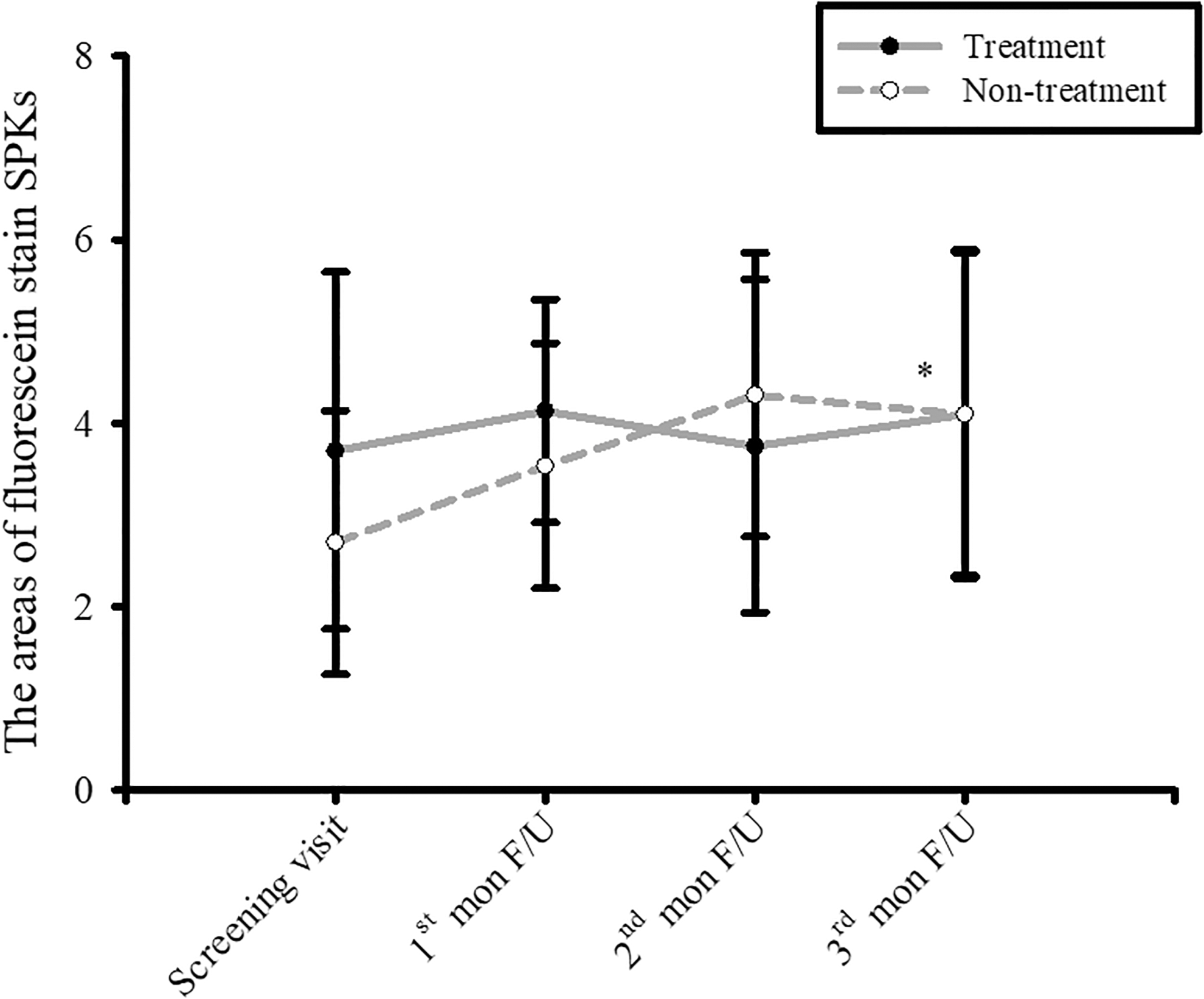
At various time points, in contrast to no significant difference in the CJDHWSWT treatment group after 12 weeks of oral intakes of CJDHWSWT, there were significantly more areas of fluorescein-stained SPKs (*p = 0.03) in the nontreatment group at the 3rd mon F/U compared to the screening visit. The data were expressed as mean ± standard deviation. 1st mon F/U, first monthly follow-up; 2nd mon F/U, second monthly follow-up; 3rd mon F/U, third monthly follow-up; CJDHWSWT, Chi-Ju-Di-Huang-Wan plus Si Wu Tang; SPK, superficial punctate keratitis.
At Various Time Points, the Areas of Fluorescein-Dyed Superficial Punctate Keratitis of the Nontreatment Versus Chi-Ju-Di-Huang-Wan Plus Si Wu Tang Treatment Group
Significance (in nontreatment group: screening visit vs. third month F/U). The data were expressed as mean ± standard deviation.
1st mon F/U, first monthly follow-up; 2nd mon F/U, second monthly follow-up; 3rd mon F/U, third monthly follow-up; SPK, superficial punctate keratitis.
Artificial tear use
At the following four time points (screening visit; 1st mon F/U; 2nd mon F/U; and 3rd mon F/U), the eye drop use (g/month) of the CJDHWSWT treatment group in contrast to those of the nontreatment group were listed as follows (Fig. 3 and Table 3): 1.8 ± 0.8 (n = 15) versus 1.8 ± 1.2 (n = 14); 2.6 ± 1.7 (n = 15) versus 2.8 ± 1.9 (n = 13); and 2.4 ± 1.8 (n = 15) versus 3.2 ± 2.4 (n = 14). Furthermore, in contrast to no significance in the treatment group after 12 weeks of oral intake of CJDHWSWT, compared to the initial artificial tear instillation (1.8 = [the amount at the end of 1 month instillation] − [that at screening visit]), there was significant (p = 0.03) increased use of the final artificial tear instillation (3.2 = [the amount at the end of 2nd mon F/U] − [that at the end of 3rd mon F/U”]) in the nontreatment group at the 3rd mon F/U.
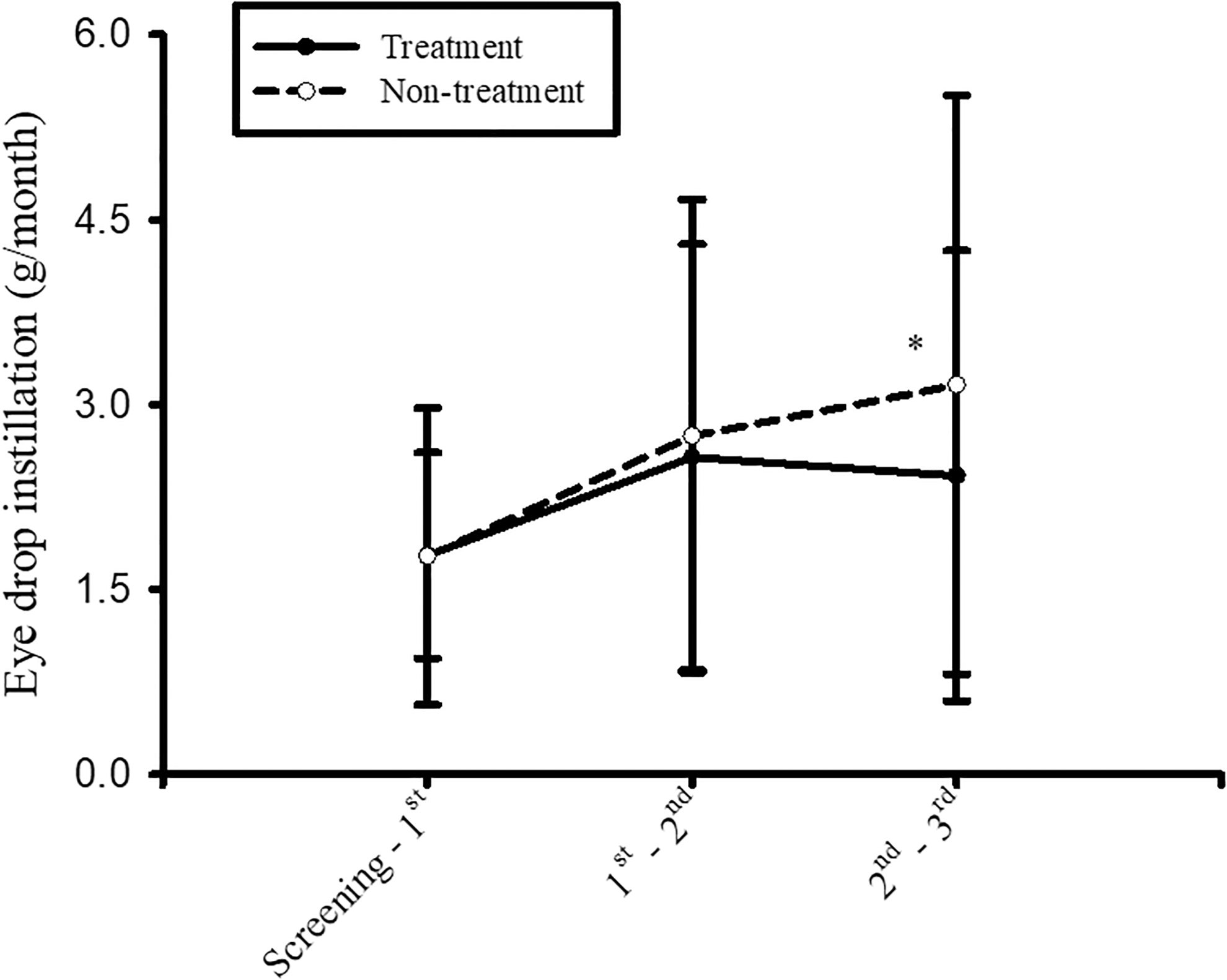
At various time points, in contrast to no significant difference in the treatment group after 12 weeks of oral intake of CJDHWSWT, there was a significantly increased amount of artificial tear instillation (g/month; *p = 0.03) in the nontreatment group (the amount of difference in instillation between the 1st mon F/U and the screening visit as well as the 2nd mon F/U and the 3rd mon F/U). The data were expressed as mean ± standard deviation. 1st mon F/U, first monthly follow-up; 2nd mon F/U, second monthly follow-up; 3rd mon F/U, third monthly follow-up; Screening−1st, the amount of eye drops in the bottle at the screening visit minus that at the first monthly F/U; 1st−2nd, the amount of eye drops in the bottle at the first monthly F/U minus that at the second monthly F/U; 2nd−3rd, the amount of eye drops in the bottle at second monthly F/U minus that at the third monthly F/U; CJDHWSWT, Chi-Ju-Di-Huang-Wan plus Si Wu Tang.
At Various Time Points, the Eye Drops Use Amount (g/Month) of the Nontreatment Versus Chi-Ju-Di-Huang-Wan Plus Si Wu Tang Treatment Group
There was significant increase in the use of artificial tear instillation in the nontreatment group at the third monthly F/U compared to the screening visit. The data were expressed as mean ± standard deviation.
Screen−1st mon F/U, amount difference between the screening visit and first month F/U; 1st−2nd mon F/U, amount difference between the first month F/U and second month F/U; 2nd−3rd mon F/U, amount difference between the second month F/U and third month F/U; F/U, follow-up; Screen, screening visit.
Tear protein levels of VEGF
At the various time points (screening visit; 1st mon F/U; 2nd mon F/U; and 3rd mon F/U), the tear VEGF protein levels of the CJDHWSWT treatment group in contrast to those of the nontreatment group were listed as follows (Fig. 4 and Table 4): 288 ± 306 versus 166 ± 78 (n = 15); 248 ± 325 (n = 15) versus 296 ± 180 (n = 14); 310 ± 433 (n = 14) versus 200 ± 134 (n = 13); and 285 ± 341 (n = 15) versus 248 ± 144 (n = 15). Furthermore, in contrast to no significant difference in the treatment group, there was significant elevated levels of tear VEGF protein (p = 0.03) from 166 ± 78 at the screening visit to 248 ± 144 (n = 15) at the 3rd mon F/U in the nontreatment group.
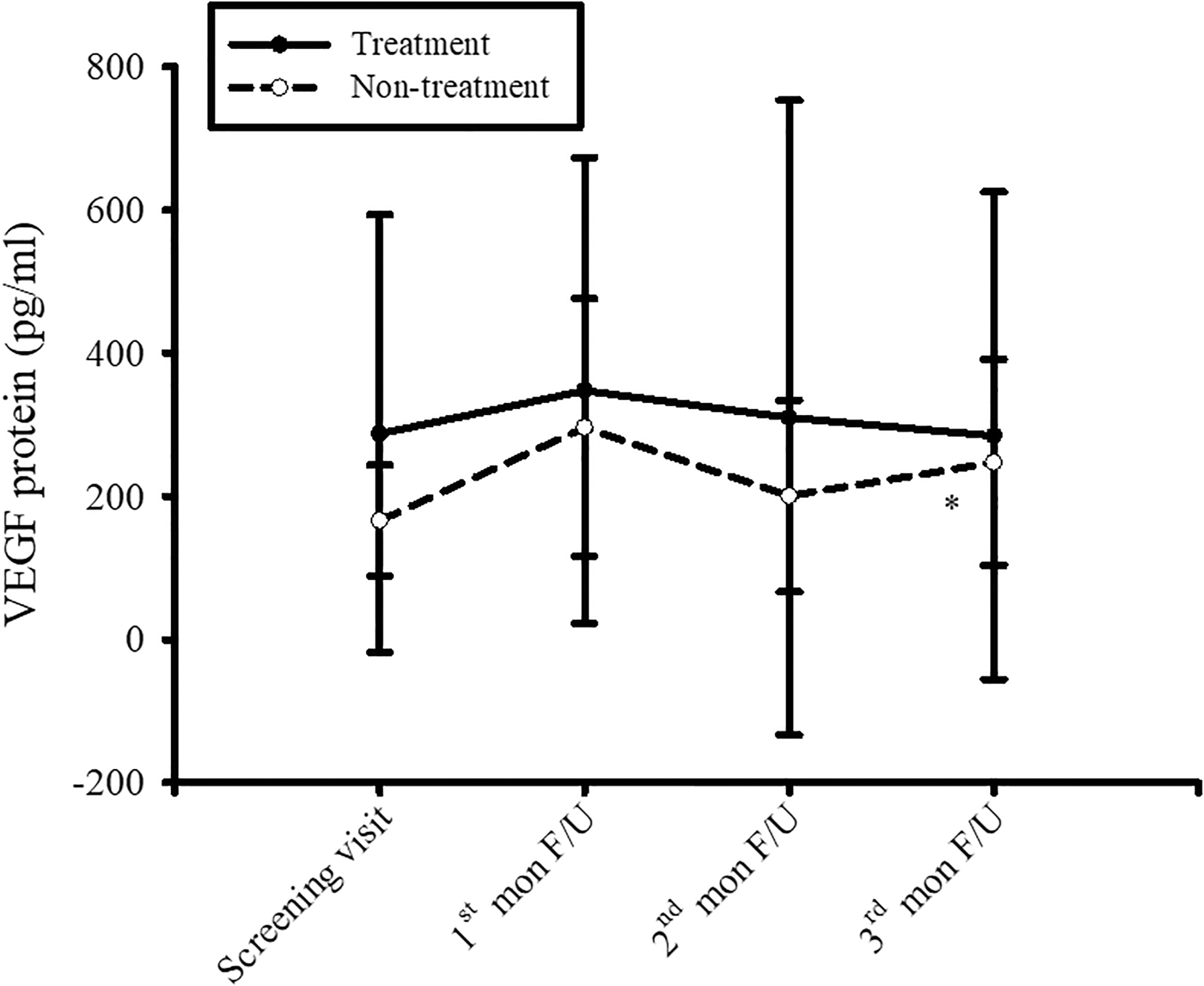
At various time points, in contrast to no significant difference in the treatment group with 3-month oral intakes of CJDHWSWT, there were significantly elevated levels of tear VEGF protein (*p = 0.03) in the nontreatment group from the screening visit to the 3rd mon F/U. The data were expressed as mean ± standard deviation. 1st mon F/U, first monthly follow-up; 2nd mon F/U, second monthly follow-up; 3rd mon F/U, third monthly follow-up; CJDHWSWT, Chi-Ju-Di-Huang-Wan plus Si Wu Tang; VEGF, vascular endothelium growth factor.
Tear Protein Levels of Vascular Endothelium Growth Factor of the Nontreatment Versus Chi-Ju-Di-Huang-Wan plus Si Wu Tang Treatment Group
Significance (In nontreatment group: Screening visit versus third month F/U). The data were expressed as mean ± standard deviation.
1st mon F/U, first monthly follow-up; 2nd mon F/U, second monthly follow-up; 3rd mon F/U, third monthly follow-up; Screen, screening visit.
OSDI
At various time points (first visit; 1st mon F/U; 2nd mon F/U; and 3rd mon F/U), the OSDI scores of the CJDHWSWT treatment group in contrast to those of the nontreatment group were listed as follows: 28.7 ± 15.9 versus 27.3 ± 16.3 (n = 15); 27.1 ± 16.8 (n = 15) versus 29.8 ± 23.2 (n = 14); 27.8 ± 14.8 (n = 14) versus 29.0 ± 19.7 (n = 13); and 23.7 ± 9.1 (n = 15) versus 25.6 ± 20.0 (n = 15). Furthermore, in contrast to no significant difference in the nontreatment group, there was “a trend,” although not significant, to improve the eye discomfort (p = 0.29) from 28.7 ± 15.9 at the first visit to 23.7 ± 9.1 (n = 15) at the 3rd mon F/U in the treatment group, after 12 weeks of oral intake of CJDHWSWT.
In addition (Table 5), in contrast to Systane treatment alone, Systane plus oral intake of CJDHWSWT showed a greater trend in improvement. In this case, 11 out of 12 defined clinically relevant symptoms or phenomena had shown this trend, except for the query “Eyes that are sensitive to light?” Of interest, after treatment of Systane plus oral intake of CJDHWSWT, there was a significant improvement in two clinically relevant phenomena, namely reading limit (p = 0.02) and uncomfortable feeling in windy conditions (p = 0.04). As the Systane (nontreatment) group compared with the Systane+CJDHWSWT (treatment) group, both presently revealed a trend to improve 3 out of 12 defined clinical relevant symptoms or phenomena, namely “Eyes that are sensitive to light? (score change = −0.27 ± 1.10 versus −0.07 ± 1.22),” “Eyes that feel gritty? (score change = −0.13 ± 1.06 versus −0.27 ± 1.10),” and “Working with a computer or ATM? (score change = −0.29 ± 1.00 versus −0.43 ± 1.28).” The lower the score, the better the final outcome.
Ocular Surface Disease Index: The Results for Changes (Last and First Visit Score Difference) of Clinically Relevant Symptoms or Phenomena of Individual Questions
A value of p < 0.05 was considered significant. Above-mentioned 12 symptoms and phenomena in this ocular surface disease index are scored as followed: All of the time, 4; Most of the time, 3; Half of the time, 2; Some of the time, 1; and None of the time, 0. The number of candidates in Gr 1 or Gr 2 is 15, respectively.
CJDHWSWT, Chi-Ju-Di-Huang-Wan plus Si Wu Tang; Gr 1, group 1; Gr 2, group 2.
As demonstrated in Table 6, the results for changes from the baseline to the final visit total OSDI score (questions 1–12) of Systane+CJDHWSWT (treatment) group were not significantly different from those of Systane (nontreatment) group, namely −5.21 ± 17.28 (baseline: 28.9 ± 16.1 and final: 23.7 ± 9.1) versus −1.7 ± 13.6 (baseline: 27.3 ± 16.3 and final: 25.6 ± 20.0). Those changes of the following three subscales were also not significantly different and listed as follows, sensory symptoms (questions 1–3): −0.27 ± 0.75 (baseline: 2.87 ± 0.68 and final: 2.60 ± 0.35) versus −0.33 ± 2.13 (baseline: 3.53 ± 2.47 and final: 3.20 ± 2.83), functional vision (questions 4–9): −2.13 ± 5.57 (baseline: 7.20 ± 4.57 and final: 5.07 ± 3.24) versus −0.27 ± 4.98 (baseline: 5.53 ± 4.00 and final: 5.40 ± 4.81), environmental triggers (questions 10–12): −0.33 ± 2.29 (baseline: 3.53 ± 2.50 and final: 3.20 ± 1.52) versus −0.27 ± 1.91 (baseline: 3.67 ± 3.02 and final: 3.40 ± 2.97), and subtotals of these three subscales (questions 1–12): −2.73 ± 8.34 (baseline: 13.53 ± 7.70 and final: 10.80 ± 4.43) versus −0.87 ± 6.55 (baseline: 12.80 ± 7.66 and final: 11.93 ± 9.53). Except the changes of the sensory symptoms, when compared to the nontreatment group, there was “a trend,” although not significant, to improve those changes of functional vision, environmental triggers, subtotal of three subscales, and total score of OSDI from first visit to the final F/U in the treatment group, after 12 weeks of oral intake of CJDHWSWT. Therefore, the overall conclusion on OSDI is that there is no significant difference between groups.
Ocular Surface Disease Index: The Results for Changes (Last and First Visit Score Difference) of Sensory Symptoms, Functional Vision, Environmental Triggers, and Subtotal Scores of the Three Subscales and Total Score of Ocular Surface Disease Index
Statistically, no significant difference existed between two groups. Above-mentioned 12 symptoms and phenomena in this OSDI are scored as follows: All of the time, 4; Most of the time, 3; Half of the time, 2; Some of the time, 1; and None of the time, 0.
Results represented in brackets are in the format as follows: (First visit's mean ± SD–Last visit's mean ± SD). For example, in the last row of the table, a data of (28.86 ± 16.09–23.65 ± 9.07) are interpreted as the following two points: (1) Upon the First visit, a baseline OSDI value of 28.86 ± 16.09 was recorded. (2) Upon the Last visit, a final OSDI value of 23.65 ± 9.07 was recorded. The number of candidates in Gr 1 or Gr 2 is 15, respectively.
CJDHWSWT, Chi-Ju-Di-Huang-Wan plus Si Wu Tang; Gr 1, group 1; Gr 2, group 2; OSDI, ocular surface disease index; Qs, questions; SD, standard deviation.
Laboratory data
Compared to the pretreatment normal defined laboratory data of liver function, kidney function, and blood sugar, there were no adverse drug effects, as shown by the post-treatment normal ones (CJDHWSWT treatment vs. nontreatment). Serum glutamic oxaloacetic transaminase (aspartate aminotransferase) was 25.1 ± 5.5–25.8 ± 5.3 versus 22.2 ± 4.8–24.1 ± 7.5. Serum glutamate pyruvate transaminase (alanine aminotransferase) was 23.1 ± 7.4–23.4 ± 9.1 versus 19.8 ± 5.5–20.5 ± 6.0. Blood urea nitrogen was 13.9 ± 3.5–14.1 ± 4.7 versus 12.1 ± 2.4–12.3 ± 3.9. Creatinine was 0.7 ± 0.2–0.7 ± 0.2 versus 0.7 ± 0.1–0.7 ± 0.2. Uric acid was 5.7 ± 1.3–6.0 ± 1.3 versus 4.9 ± 1.3–5.0 ± 1.3. Glucose was 97.7 ± 8.7–98.0 ± 16.1 versus 100.7 ± 13.4–102.0 ± 11.9. In addition, BCVAs (Snellen E) were not significantly different at various time points and were 1.0 ± 0.2 at screening visit as well as 1.1 ± 0.3 at 1 month, 1.0 ± 0.1 at 2 months, and 1.1 ± 0.2 at 3 months after administration of CJDHWSWT.
Discussion
Eye drops, gel, and ointment still play the main role in treating dry eye. Steroid and nonsteroid anti-inflammatory agents as well as cyclosporine, tetracycline, and antioxidants 5 might have adjunct effects. A recent study 5 might support that dry eye could be induced by oxidative stress. One report 2 has proved that CJDHW is effective in treating dry eye. However, the underlying mechanism of CJDHW's effect on dry eye is in need of further investigation. In our recent publication, CJDHW has an anti-ischemic effect by inhibition of apoptosis. 7 Furthermore, the two main components, Dāngguī and Chuān Xiōng, of SWT contain the active composition ferulic acid. 14 Ferulic acid is able to protect against retinal ischemia by acting as a free radical scavenger.
Tear secretion, corneal epithelial stabilization, and artificial tear use
As shown in this result, basal tear secretion was measured by Schirmer's test following the use of topical anesthetic. Dry eye was defined as values with tear on the filter paper <5 mm at 5 min measurement. 11 As supported by this result (Fig. 1 and Table 1), the oral CJDHWSWT (10.2 mm after 3 months of treatment), in contrast to no significant difference in the nontreatment group, appears to significantly increase in the secretion of the major lacrimal gland compared to the screening visit (7.3 mm). Compared to no significant difference in the treatment group, there were significantly numerous fluorescein-stained areas of SPKs in the nontreatment group (Fig. 2 and Table 2; nontreatment group: 2.7 at the screening visit–4.1 “areas” of SPKs at the 3rd mon F/U). In contrast, the areas of SPKs were not significantly altered in the CJDHWSWT treatment group (3.7 at the screening visit–4.1 areas of SPKs at the final visit). The oral CJDHWSWT significantly stabilized the corneal condition by preventing from the deterioration of SPKs. In view of the use of artificial tear instillation in the treatment group, there was significantly more consumption in the amount of artificial tear in the nontreatment group (Fig. 3 and Table 3; nontreatment group: 1.8 g/month after 1 month of instillation versus 3.2 g/month after 3 months of instillation). In contrast, the eye drop instillation amount was not significantly changed in the CJDHWSWT treatment group (1.8 after 1 month of instillation–2.4 g/month after 3 months of instillation). This result is relevant to the above-mentioned results (Figs. 1 and 2 and Tables 1 and 2), namely increased lacrimation and corneal stabilization in the treatment group.
Compared the Systane group with the Systane+CJDHWSWT group, both presently demonstrated a trend to improve 3 out of 12 defined clinically relevant symptoms or phenomena as mentioned in the Results and Table 5. However, the improvement in two clinically relevant phenomena (e.g., gritty and computer working) has implied that the effect of Systane was less effective compared with CJDHWSWT+Systane, although not significantly. Moreover (Table 5), compared with Systane treatment alone, Systane plus oral intake of CJDHWSWT showed a greater trend to improve 11 out 12 defined clinically relevant symptoms or phenomena, except “Eyes that are sensitive to light?.” Interestingly, after treatment of Systane plus oral intake of CJDHWSWT, there was a significant improvement in two clinically relevant phenomena, namely reading limit and uncomfortable feeling in windy conditions. These findings have further supported that the combined effect of CJDHWSWT+Systane was significantly more efficient than the effect of Systane that was proved to show significant ocular discomfort score improvement. 21 The effect of CJDHWSWT was clinically useful in treating dry eye in terms of improvement in clinically relevant dry eye-related symptoms/phenomena, lacrimal gland secretion increase, corneal epithelial stabilization, and artificial tear use reduction. The latter one might also indicate the decrease of medical expense and preservative consumption.
Concentrations of tear VEGF protein
Dry eye is known to be related to autoimmune disorder such as Sjogren syndrome, oxidative stress, and inflammation. Dysfunction might be involved in lacrimal gland (aqueous), meibomian gland (mebum, i.e., tear lipids), and/or conjunctival goblet cell (mucus). This is the pioneering research to study whether ischemia might also play a role in dry eye. VEGF is one of the main factors found in the ischemic cascade. In the nontreatment group, the concentrations of tear VEGF protein were significantly increased (Fig. 4 and Table 4; nontreatment group: 166 at the screening visit to 248 at the 3rd mon F/U). In contrast, there was no significant difference in the tear VEGF levels in the CJDHWSWT treatment group (288 at the screening visit to 285 after 3 months of treatment). This direct biochemical result is consistent with a previous indirect clinical evidence, namely subconjunctival injection of an anti-VEGF agent, avastin, in managing with dry eye. 22 These present data might imply that dry eye could be induced by, at least in part, ischemia, which might be protected by CJDHW and/or SWT. Not inconsistent with recent reports, 7,14 the combination of CJDHW and SWT (CJDHWSWT) might provide anti-ischemic, anti-apoptotic, and anti-oxidative effects. Compared to the pretreatment defined normal laboratory data, there were no adverse drug effects, as shown by the post-treatment normal ones. The CJDHWSWT formula is safe and effective in treating dry eye by, at least in part, inhibition of VEGF stimulation.
This research has limitations, including a small sample size (n = 30), due to its pilot study nature. Theoretically, an investigator makes an academic guess for unknown parameters based on pilot investigations or previous publications. Since no information is available in the effect of CJDHWSWT on dry eye, the performance of a small sample-sized pilot experiment first was presently considered before attempting a larger study. Additionally, the present doses of CJDHW (<1 g) and SWT (<0.1 g) are, respectively, less than one twelfth fold (1/12) and one one hundred twentieth fold (1/120) of the traditionally prescribed daily dose. The traditional daily dose is 12 g of CJDHW and 12 g of SWT. 2 In the future study, a significant improvement in OSDI might be achieved by administration with a half of 12 g of CJDHW and SWT, that is, 6 g of each formula, which could be conducted in a future larger sample-sized study.
Conclusions
This human pilot study has supported that CJDHWSWT is safe and effective for dry eye by significant lacrimal gland secretion increase, corneal epithelial stabilization, and artificial tear use reduction. Both FA, the active component of SWT, and CJDHW have been proved to have an anti-ischemic effect previously. Consistently, this result has implied that CJDHWSWT's defined effects on dry eye might act by inhibition of dry eye-associated ischemia-induced VEGF upregulation. Nevertheless, further investigation needs to be carried out.
Footnotes
Acknowledgment
Thankfulness is conveyed to Taipei Veterans General Hospital adjunct with TCM Biotech International Corporation for the research grant, 2015 Industry-Government-Academy Cooperation Project. We also owe our sincere thanks to Ms. Ting Chen and Hsin-Mei Lin for their skillful techniques in molecular biology as well as to Professor Ralph Kirby and Mr. Howard Wen-Haur Chao for their expertise in revising the article and the proof.
Authorship Statement
Hsiao-Ming Chao designed this project, wrote the first draft of the article, was involved in the analysis of the results, and read/revised the submitted article. Wen-Jin Chao responded one-by-one to the critical comments from three reviewers and re-wrote/redrew the article/![]() . Shu-Qiu Tan helped in conducting this clinical trial and collecting all these data. Jorn-Hon Liu read/revised the submitted article. Mi-Mi Chen and Huei-Wen Shiu helped collecting all these data.
. Shu-Qiu Tan helped in conducting this clinical trial and collecting all these data. Jorn-Hon Liu read/revised the submitted article. Mi-Mi Chen and Huei-Wen Shiu helped collecting all these data.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors would like to convey their thanks to Taipei Veterans General Hospital adjunct with TCM Biotech International Corporation for the research grant, 2015 Industry-Government-Academy Cooperation Project (T-14013).