
Abstract
Objective:
The present study was conducted to investigate the effect of Viola odorata extracted syrup on the quality and patterns of sleep in patients with depression or obsessive–compulsive disorder (OCD) as add-on therapy.
Design:
A pilot double-blind randomized placebo-controlled trial.
Settings/Location:
Psychiatric Clinic of Imam Hossein Hospital, Tehran, Iran.
Subjects:
Participants were 16–15 years of age with mild and moderate depression or OCD having insomnia.
Interventions:
This pilot study was conducted on patients with insomnia divided into two groups with depression (40 patients) or OCD (43 patients). Each group randomly assigned into two arms with the same conditions at baseline. The intervention arm daily received 5 mL V. odorata syrup every 12 h for 4 weeks, and the control arm received 5 mL placebo syrup every 12 h for 4 weeks. None of the participants was deprived of their routine treatment for depression or OCD.
Outcome measures:
The scores of insomnia symptoms were evaluated using total score of the Pittsburgh Sleep Quality Index (PSQI) and the scores of its components, the depression score using the final Beck depression inventory-II (BDI-II) score, and OCD score using the Yale–Brown Obsessive–Compulsive Scale (YBOCS).
Results:
The total PSQI score was found to be improved significantly in the intervention arms with depression or OCD (p < 0.001) compared with the corresponding control arms. Significant improvements were also observed in the final mean difference of BDI-II (p = 0.009) and YBOCS (p = 0.001) scores in the intervention arms.
Conclusions:
V. odorata syrup significantly improved insomnia symptoms and the scores of depression and OCD.
Introduction
Sleep is a highly organized bioprocess whose disorders can cause daytime sleepiness, anxiety, and poor performance. 1 –4 Insomnia is defined as having at least 4 weeks of symptoms, such as difficulty falling asleep, sleeping or having a nonrestorative sleep, despite having enough time to sleep coupled with a disruption to daily functioning. 5,6 . Insomnia is more prevalent in adults, and negatively affects quality of life and requires higher levels of health care services. 7 –13 The huge financial burden of insomnia is associated with overutilization of health services, reducing workplace productivity and excessive employee absenteeism, which annually cost over $100 billion. Patients with insomnia normally report stress, anxiety, and depression. 14,15
The prevalence of depression as the second most common chronic disease has linearly increased. 16,17 The prevalence of depression and insomnia has been reported as high, and patients with depression have been reported to have difficulty starting or maintaining sleep. 18 –20 Significant associations were observed in a longitudinal epidemiologic study between insomnia and depression. Insomnia lasting over 2 weeks was also found to predict major depressive episodes in the upcoming interviews. Approximately two-thirds of patients with a major depressive episode have insomnia. Moreover, 17%–50% of patients without depression living with insomnia for at least 2 weeks over the previous 6 months were found to have experienced a major depressive episode. 21,22
Although the symptoms of obsessive–compulsive disorder (OCD) as a prevalent psychiatric disorder do not include sleep problems, OCD was found to be associated with insomnia. 6,23 –25 The sleep disorder observed in patients with OCD differs from that in healthy individuals, as with increasing sleep recovery, symptoms of OCD can decrease. 6,24 –26 The amount of time spent asleep divided by the total amount of time in bed defined as sleep efficiency and the total sleep time were found to decrease in patients with OCD. 23,27 Moreover, the delayed sleep phase disorder pattern is prevalent in patients with severe OCD. A recently conducted meta-analysis reported a slightly higher proportion of slow-wave and lower rapid eye movement sleep pattern in the OCD group compared with healthy subjects. 24
Insomnia can be treated with modern medicine, including pharmacotherapy, and may recur in case of discontinuing this type of medication or administering nonmedicinal therapies. 6 The effects of traditional Persian medicine (TPM) on treating insomnia has been investigated with a focus on Viola odorata, which was found to exert sedative and hypnotic effects in animals or human. 28 –30 The mean melatonin level in the V. odorata was found to be 0.8 ng/g using high-performance liquid chromatography with UV detection (a hot water extract) and 1.1 ng/g using the enzyme-linked immunosorbent assay (an alcoholic extract). 31 Melatonin as a nutritional supplement is popularly used as a nonprescription therapy for treating insomnia symptoms. 32 As an active ingredient of V. odorata, 31 it can therefore contribute to the hypnotic and circadian-shifting effect of V. odorata. 32
Compared with diazepam, V. odorata extract proved to exert better dose-dependent sedative and preanesthetic effects on rats. In fact, 400 mg/kg body weight of the V. odorata extract was significantly more effective than 1.2 mg/kg body weight of diazepam. Given the superiority of V. odorata over diazepam as a commonly prescribed medication for treating insomnia, 30 using V. odorata as an alternative to diazepam for treating insomnia is recommended that should be studied in detail to prove its efficacy. In addition, V. odorata improved sleep and the scores of the insomnia severity index in patients with chronic insomnia after a month, and it was found as a safe herbal agent with few side effects developing proper and effective tolerance in the patients. 29
Up to our knowledge, the effect of V. odorata on insomnia in patients with depression or OCD has not been addressed in literature yet. The present randomized double-blind placebo-controlled trial was therefore performed to investigate the effect of V. odorata syrup on the quality and patterns of sleep in patients with insomnia and depression or OCD.
Materials and Methods
Participants
The present study was conducted in January–November 2017 as ongoing recruitment on a population comprising male and female outpatients with insomnia and mild-to-moderate depression or OCD, 16–50 years of age, presenting to the psychiatric clinic of Imam Hossein Hospital affiliated to Shahid Beheshti University of Medical Sciences, Tehran, Iran. The study began by collecting demographic data of participants. Interviews were conducted based on the Diagnostic and Statistical Manual of Mental Disorders, 5th Edition (DSM-V) criteria, 6 and a psychiatrist confirmed diagnosis of depression based on the scores of the Beck depression inventory-II (BDI-II) questionnaire 33 and OCD based on the score of the Yale–Brown Obsessive–Compulsive Scale (YBOCS). 34
The research team briefed the eligible candidates on the study objectives and procedure, ensured the confidentiality of their information, and included them in the study after they signed written informed consent forms. Depression was diagnosed as minimal in the patients receiving a score of 0–13 from the BDI-II, as mild in those receiving 14–19, as moderate in those receiving 20–28, and severe in those receiving 29–63. None of the participants was deprived of their routine treatments for depression or OCD during the trial. The patients had a right to withdraw from the study at their own discretion, which did not interfere with the process of their treatment.
The inclusion criteria comprised mild-to-moderate depression or OCD, insomnia symptoms confirmed based on the Pittsburgh Sleep Quality Index (PSQI), 35,36 an age of 16–50 years, signing written informed consent forms for participation in the study, and taking selective serotonin reuptake inhibitors for at least 1 month. The exclusion criteria comprised physical illnesses, including pulmonary diseases, allergic rhinitis, cardiac disease, infections, liver and kidney diseases and cancers, psychotic disorders, generalized anxiety disorder, a history of smoking and drug abuse, neurological diseases such as Parkinson's disease and Alzheimer's disease, breathing-related sleep disorders, and simultaneous use of pharmaceutical or nonpharmaceutical therapies for insomnia, pregnancy, and breastfeeding.
After diagnosing depression or OCD, the psychiatrist prescribed either sertraline or fluvoxamine as the first-line therapy for all the study patients. The medicine dose was increased to its mean effective dose and maintained for the 1 month of the present trial when no changes were made in the medication regimens for treating OCD or depression in the participants. The patients were then prescribed the V. odorata syrup or placebo depending on their subgroup. At the beginning of the intervention, sleep hygiene worksheets were distributed among the patients and “dos and don'ts” were detailed to them.
The present study was approved by the Ethics Committee of Shahed University of Medical Sciences, Tehran, Iran on April 9, 2017 (Code: IR Shahed REC. 1395.232), and registered in the Iranian Registry of Clinical Trials (IRCT ID: 2017040833294N1).
Syrup preparation method and interventions
The aerial parts of the dried V. odorata flower were collected from Kurdistan Province, Iran in October 2016. This plant was identified by herbalist Kamalinejad, who knew this plant well. The samples of this plant were identified and kept in the herbarium of the Department of Pharmacognosy, Shahid Beheshti University of Medical Sciences (herbarium code: SBMU-8088). The placebo syrup and V. odorata syrup were prepared in the School of Pharmacy, Shahid Beheshti University of Medical Sciences. According to the instructions provided in TPM textbook, 37 V. odorata flower syrup was prepared by adding 50 g of the aerial part of the dried V. odorata flower to 1 L of boiled water at 80°C and kept in a container for 2 h and then straightened out. The water was then vacuumed at 50°C with a rotary vacuum evaporator.
The total dry weight of the extract was 10 g. A 50% sugar solution was added to the extract to make the final extract concentration of the syrup equal to 50 g/L, which was measured through stability testing. The extract ratio was obtained as 1:6, and the placebo was prepared in the Department of Pharmacognosy, Shahid Beheshti University of Medical Sciences using the pharmacopoeia simple syrup formula, including the standard color and flavor additives resembling the V. odorata syrup color and taste. A group of volunteers qualitatively tested the taste and color of the two different types of syrup and confirmed them as identical. Two similar bottles were eventually filled with the products and kept in a refrigerator.
Every participant in the intervention arm daily received 5 mL of V. odorata syrup every 12 h, and every participant in the control arm daily received 5 mL of the placebo syrup every 12 h. The patients were advised to take a dose of the syrup overnight 1–1.5 h before bedtime and the next dose 12 h later. They were also warned to avoid taking the medicine with food given the potential drug–food interactions. Both types of syrup were identical in terms of bottle, color, and taste, and were prepared by a person who was not involved in the present clinical trial.
The syrup bottles were distributed among the participants, and they were asked to use them at home for 1 month and return after 1 month to complete the PSQI and the BDI-II or the YBOCS questionnaires. Furthermore, they were all provided with a phone number to contact the research team in case of any drug complications or questions. The authors also telephoned them twice a week to know about their medication and potential problems. The participants who had at least 20% of the syrup left after 1 month were considered noncompliant with the treatment, excluded from the study, and referred to a psychiatrist for medical counseling.
Objective and hypothesis
The present study was conducted to determine the effect of V. odorata syrup on the total score of the PSQI score and the scores of its components, including subjective sleep quality, habitual sleep efficiency, sleep disturbances, daytime dysfunction, sleep latency and sleep duration, as well as BDI-II and YBOCS scores in patients with mild-to-moderate depression or OCD whose insomnia had been confirmed based on the PSQI score.
The three hypotheses of the present study included observing significant differences in PSQI scores, BDI-II scores, and YBOCS scores in the intervention arms compared with the control arms. The null hypothesis included the rejection of the aforementioned hypotheses.
Outcomes
Changes in the scores of insomnia symptoms measured with the PSQI between baseline and 1 month after the intervention were considered the primary outcome of the present study. Changes in depression scores measured with the BDI-II and in OCD scores measured with the YBOCS between baseline and 1 month after the intervention were considered the secondary outcome of the present study.
Sample size
The sample size was calculated as 18 in each group with a test power of 85% and a statistical significance level of 5% (α = 0.05). Considering a nonresponse rate of 30% associated with drop-out and loss to follow-up, the final adjusted sample size was calculated as 26 in each study group using the formula n* = n/(1 − q), in which n* represents adjusted sample size, n the initial sample size, and q the expected no-response proportion. 38 Convenience sampling method was also used to select the participants.
Randomization procedure and allocation concealment
Randomization was performed using a simple random-number table. As a key component of an effective randomization, allocation concealment is used for implementing a random allocation sequence without the foreknowledge of allocation codes and randomization list in a way that intervention is kept unknown until the study is unblinded. 39 Allocation concealment was performed in the present study by assigning a person who was unaware of the included subjects and the collection, monitoring, and management of data to allocate glass bottles of syrup to the participants. These similar dark and carefully packaged bottles were numbered according to the random sequence generated and concealed by an independent statistician who was not involved in the study. They were assigned by the research team to one of the two arms upon their completion of the questionnaires.
Blinding
The participants and the administrative team, including the principal investigator, were kept blinded to the intervention allocation in this randomized double-blind clinical trial. The participants, the medical staff at the psychiatric clinic, the study assistants and the colleagues involved in handling or collecting the data were also blinded. After collecting the data and performing a preliminary analysis on them, an independent statistician who developed the randomization sequence at the beginning of the study performed the unblinding of this trial in the presence of the researcher, an academic supervisor, and a representative from the medical school.
Statistical analysis
The quantitative data were described as mean values using the t test, the Mann–Whitney U test, ANOVA, the Kruskal–Wallis test, and the Wilcoxon test. The Kolmogorov–Smirnov test was used to investigate the distribution normality. The paired t test or the Wilcoxon test was used to compare the mean baseline with the final results, and the t test or the Mann–Whitney U test to investigate the mean difference between baseline and the final results. Data were analyzed in SPSS Statistics for Windows, version 18.0 (SPSS, Inc., Chicago, IL). p < 0.05 was set as the level of statistical significance.
Results
Forty-nine of 83 eligible patients with insomnia and mild-to-moderate depression assigned to the depression group were randomly divided to two arms, that is, an intervention arm of 25 and a control arm of 24. Five patients were excluded from the intervention arm, including one due to loss of follow-up, two due to recovery, and two due to withdrawal from the study. Four patients were excluded from the control arm, including two due to loss of follow-up, one due to withdrawal, and one due to lack of interest in the syrup. Twenty subjects were ultimately analyzed in each arm.
Fifty-three of 92 eligible patients with insomnia and OCD assigned to the OCD group were randomly assigned to an intervention arm of 27 and a control arm of 26. Four patients were excluded from the intervention subgroup, including one due to loss of follow-up, one due to recovery, and two due to withdrawal from the study. Six patients were excluded from the control arm, including three due to loss of follow-up, two due to withdrawal from the study, and one due to recovery. Data of 23 participants in the intervention arm and 20 in the control arm were therefore analyzed. Every participant in these four arms was also assigned to one of four other subgroups by age, including at most 25, 26–35, 36–45 years, and at least 46 years.
Figure 1 shows the CONSORT flow diagram associated with participants in the depression group, and Figure 2 shows the diagram associated with the OCD group. The study was conducted from January 2017 to November 2017. After recruiting 83 participants in the depression group and 92 in the OCD group, 34 were excluded for some reasons from the depression group as shown in Figure 1 and 39 from the OCD group as shown in Figure 2.
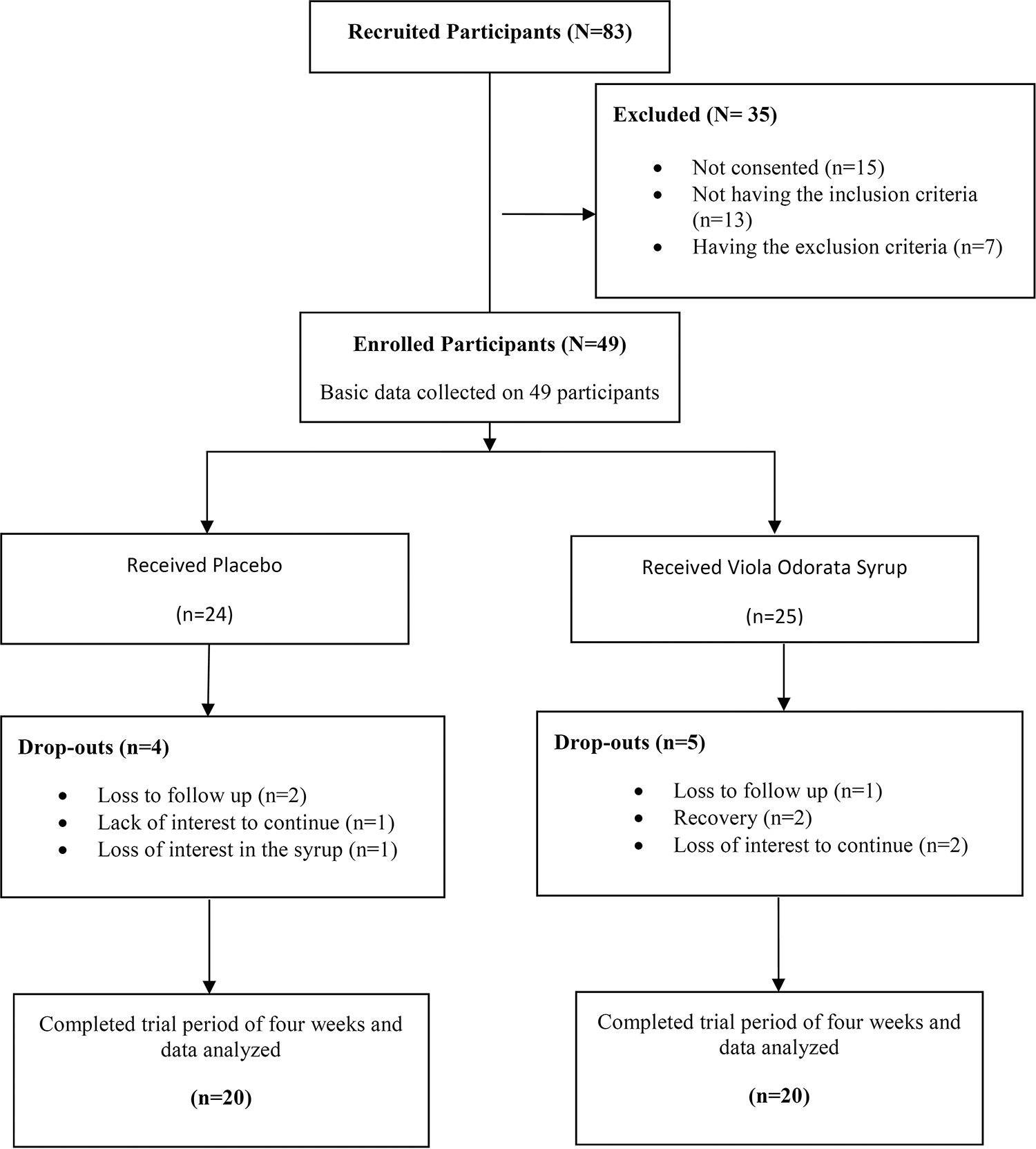
The flowchart of the distribution of participants with depression and insomnia during the study.

The flowchart of the distribution of participants with obsessive–compulsive disorder and insomnia during the study.
According to Table 1, the actual dropout rate during the trial was 18.4% (9/49) for the depression group and 19.0% (10/53) for the OCD group, instead of the planned 30% for each group. The overall completion rate was therefore 81.6% (40/49) in the depression group and 81% (43/53) in the OCD group (Table 1). This rate was also 80% (20/25) and 85% (23/27), respectively, in the intervention and control arms of the depression group and 83% (20/24) and 77% (20/26) in the corresponding arms of the OCD group. None of the participants reported any side effects at the end of the trial.
Demographic Characteristics of the Study Participants
p1: Comparison of the baseline demographic characteristics between the intervention and control arms; p2: Comparison of the total final PSQI score between the intervention and control arms; p3: Comparison of the final BDI-II Score or the final YBOCS Score in the intervention arm or in the control arm of depression and OCD groups.
BDI-II, Beck depression inventory-II; F, female; OCD, obsessive–compulsive disorder; M, male; PSQI, Pittsburgh Sleep Quality Index; YBOCS, Yale–Brown Obsessive–Compulsive Scale.
Table 1 presents the demographic characteristics of all the study subjects, suggesting no initially significant differences between the intervention and control arms of the patients with depression or OCD in terms of age (p = 0.255 and p = 0.255, respectively), gender (p = 0.716 and p = 0.528, respectively) and level of education (p = 0.347 and p = 0.390, respectively). The two arms of either the depression or OCD group had therefore the same conditions at baseline.
At the end of the study, no significant differences were observed between two genders and between the four age subgroups and between the three education subgroups in terms of the total PSQI score and the BDI-II score or the YBOCS score in the intervention and control arms of the depression and OCD groups (Table 1).
Tables 2 and 3 presents the results associated with the effect of V. odorata syrup on the total score of the PSQI and the scores of its components, including subjective sleep quality, habitual sleep efficiency, sleep disturbances, daytime dysfunction, sleep latency, and sleep duration, respectively, in the patients with depression and OCD as follows:
Comparison of Baseline Scores and Total Final Score of the Pittsburgh Sleep Quality Index and Its Components Between Intervention and Control Arms of Patients With Depression and Insomnia
: Significance level: below 0.05.
p1: Comparison of the baseline score between the intervention and control arms; p2: Comparison of the final score between the intervention and control arms; p3: Comparison between the baseline score and the final scores in the intervention or control arm; p4: Comparison of the mean difference between the intervention and control arms.
PSQI, Pittsburgh Sleep Quality Index; SD, standard deviation.
Comparison of Baseline and Final Total Pittsburgh Sleep Quality Index Score and Its Components Between Intervention and Control arms of Patients With Obsessive–Compulsive Disorder and Insomnia
Significance level: below 0.05.
p1: Comparison of the baseline score between the intervention and control arms; p2: Comparison of the final score between the intervention and control arms; p3: Comparison between the baseline score and the final scores in the intervention or control arm; p4: Comparison of the mean difference between the intervention and control arms.
PSQI, Pittsburgh Sleep Quality Index; SD, standard deviation.
The difference in the score of baseline subjective sleep quality between the intervention and control arms of the patients with depression was not significant (p = 0.946, Table 2) and of those with OCD was significant (p = 0.007, Table 3). The final score, however, significantly improved in the intervention arm compared with the control arm of both the patients with depression (p = 0.001, Table 2) and OCD (p = 0.001, Table 3). In the depression group, the difference between the final score and the baseline score was significant in the intervention arm (p < 0.001, Table 2) and not significant in the control arm (p = 0.93, Table 2). Similarly, significant improvements were observed in the intervention arm (p = 0.041, Table 3) compared with the control arm (p = 0.06, Table 3) of the OCD group. The mean difference was also significantly higher in the intervention than the control arm of both the depression group (p < 0.001, Table 2) and the OCD group (p = 0.023, Table 3).
No significant differences were observed in the score of baseline habitual sleep efficiency between the intervention and control arms of the patients with depression (p = 0.961, Table 2) or OCD (p = 0.922, Table 3). The final score, however, significantly improved in the intervention arm of the depression group (p = 0.012, Table 2) and OCD group (p = 0.005, Table 3) compared with the corresponding control arms. In addition, the final score significantly improved compared with baseline in the intervention and control arms of the depression group (p < 0.001 and p = 0.023, respectively, Table 2) and the OCD group (p < 0.001 and p = 0.039, respectively, Table 3). The mean difference was also significantly higher in the intervention arm than in the controls of the depression group (p = 0.003, Table 2) and the OCD group (p = 0.001, Table 3).
No significant differences were observed in the score of baseline sleep disturbances between the intervention and control arms of the patients with depression (p = 0.134, Table 2) or OCD (p = 0.896, Table 3). The final score, however, significantly improved in the intervention arm compared with the control arm of the depression group (p = 0.004, Table 2) and the OCD group (p = 0.002, Table 3). Moreover, the final score significantly improved compared with baseline in the intervention arms of the depression group (p < 0.001, Table 2) and the OCD group (p < 0.001, Table 3) and the control arm of the OCD group (p = 0.01, Table 3), although the change was not significant in the control arm of the depression group (p = 0.56, Table 2).
The mean difference was also significantly higher in the intervention than the control arm of the depression group (p < 0.001, Table 2) and the OCD group (p = 0.001, Table 3).
No significant differences were observed in the score of baseline daytime dysfunction between the intervention and control arms of the patients with depression (p = 0.684, Table 2) or OCD (p = 0.245, Table 3). The final score, however, significantly improved in the intervention arm compared with the control arm of the depression group (p = 0.001, Table 2) and the OCD group (p < 0.001, Table 3). The final score also significantly improved compared with baseline in the intervention arms of the depression group (p < 0.001, Table 2) and the OCD group (p < 0.001, Table 3), although the change was not significant in the control arms of the depression group (p = 0.09, Table 2) and the OCD group (p = 0.111, Table 3).
The mean difference was also significantly higher in the intervention than the control arm of the depression group (p < 0.001, Table 2) and the OCD group (p < 0.001, Table 3).
No significant differences were observed in the score of baseline sleep latency between the intervention and control arms of the patients with depression (p = 0.807, Table 2) or OCD (p = 0.295, Table 3). The final score, however, significantly improved in the intervention arm compared with the control arm of the depression group (p = 0.01, Table 2) and the OCD group (p < 0.001, Table 3). The final score also significantly improved compared with baseline in the intervention arms of the depression group (p < 0.001, Table 2) and the OCD group (p < 0.001, Table 3) and the control arm of the depression group (p = 0.003, Table 2), although the change was not significant in the control arm of the OCD group (p = 0.079, Table 3).
The mean difference was also significantly higher in the intervention arm than in the control arm of the depression group (p = 0.01, Table 2) and the OCD group (p < 0.001, Table 3).
No significant differences were observed in the score of baseline sleep duration between the intervention and control arms of the depression group (p = 0.987, Table 2) and the OCD group (p = 0.545, Table 3). The final score, however, significantly improved in the intervention arm compared with the control arm of the depression group (p = 0.025, Table 2) and the OCD group (p = 0.003, Table 3). The final score also significantly improved compared with baseline in the intervention arms of the depression group (p < 0.001, Table 2) and the OCD group (p < 0.001, Table 3) and in the control arms of the depression group (p = 0.001, Table 2) and the OCD group (p = 0.003, Table 3).
Furthermore, the mean difference was significantly higher in the intervention arm than in the control arm of the depression group (p = 0.002, Table 2) and the OCD group (p < 0.001, Table 3).
The difference in the total baseline PSQI score was not significant between the intervention and control arms of the patients with depression (p = 0.757, Table 2) and significant between the arms of the patients with OCD (p = 0.014, Table 3). The final score also significantly improved in the intervention arm compared with the control arm of the depression group (p < 0.001, Table 2) and the OCD group (p < 0.001, Table 3). Moreover, the final score significantly improved compared with baseline in the intervention and control arms of the depression and OCD groups (p's < 0.001, Tables 2 and 3).
Furthermore, the mean difference was significantly higher in the intervention arm than in the control arm of the depression group (p < 0.001, Table 2) and the OCD group (p < 0.001, Table 3).
According to Tables 2 and 3, reductions in the total PSQI score observed in the arms of both the depression and OCD groups were associated with the routine treatment of depression and OCD or instructions provided based on sleep hygiene worksheets. The mean differences in the total score of the PSQI and the scores of all its components were also significantly higher in the intervention arms compared with the control arms.
According to Table 4, the difference in the baseline BDI-II score was not significant between the intervention and control arms of the depression group (p = 0.563), although the final score significantly improved in the intervention arm compared with the control arm (p = 0.008). The final score also significantly improved compared with baseline in the intervention arm (p < 0.001) and the control arm (p = 0.005). In addition, the mean difference was significantly higher in the intervention arm compared with the control arm (p = 0.009). Despite the reduction in the final BDI-II score due to routine depression therapy in both arms of the study, the mean difference was significantly higher in the intervention arm compared with the control arm.
Comparison of Baseline and Final Beck Depression Inventory-II and Yale–Brown Obsessive–Compulsive Scale Scores Between the Intervention and Control Arms of the Patients with Depression or Obsessive–Compulsive Disorder Having Insomnia
Significance level: below 0.05.
p1: Comparison of the baseline score between the intervention and control arms; p2: Comparison of the final score between the intervention and control arms; p3: Comparison between the baseline and final scores in the intervention or control arm; p4: Comparison of the mean difference between the intervention and control arms.
OCD, obsessive–compulsive disorder; SD, standard deviation.
According to Table 4, although the baseline YBOCS score was not significantly different between the intervention and control arms (p = 0.855), the final score significantly improved in the intervention arm compared with the control arm (p = 0.018). The final score also significantly improved compared with baseline in both the intervention (p < 0.001) and control (p = 0.011) arms. The mean difference was, however, significantly higher in the intervention arm compared with the control arm (p = 0.001). Despite the reduction in the final YBOCS score due to routine OCD therapy in both arms of the study, the mean difference was significantly higher in the intervention arm compared with the controls.
Discussion
The two arms of the trial had the same baseline conditions in both groups. In both of the study groups, the final scores of all the components of the PSQI and the total final PSQI score significantly improved in the intervention arm compared with the control arm. In addition, the final scores of all the components of the PSQI and the total final PSQI score significantly improved in both the intervention and control arms compared with baseline scores, except for the scores of subjective sleep quality and daytime dysfunction in the control arms of both groups, and the score of sleep disturbance in the control arm of the patients with depression and the score of sleep latency in the control arm of the patients with OCD.
Furthermore, the mean differences in all the components of the PSQI and the total PSQI score were significantly higher in the intervention arm than in the control arm of both the study groups. Despite the significant reductions in the final BDI-II score and the YBOCS score compared with baseline due to routine depression and OCD treatments in both arms, the mean differences were significantly higher in the intervention arm than in the control arm.
A randomized double-blind placebo-controlled trial by Feyzabadi et al. 40 prescribed intranasal violet oil drops for patients with chronic insomnia for 1 month. These patients who did not receive any treatments were provided with sleep hygiene instructions. Moreover, the score of sleep quality was determined with the PSQI, and the score of the insomnia severity index significantly improved in the participants who reported no adverse effects. These results are consistent with those obtained in the present study, although the present study patients, who had insomnia and depression or OCD, were not deprived of routine treatments for depression or OCD.
A randomized clinical trial by Hejazian et al. 41 investigating the effects of V. odorata oil nasal drops on sleep quality in elderly using the PSQI reported significant improvements in sleep quality, increases in sleep duration, reductions in sleep disorders, and improvement of delays in falling asleep. Similarly, the present study found the oral administration of this herbal medicine to improve sleep quality in the patients with insomnia and depression or OCD using the same questionnaire. The differences between the cited and the present study are twofold.
First, the present study included a wide age range, including below 25 to over 46, whereas these authors selected the participants from older adults living in a nursing home. Second, the total score of the PSQI and the scores of its components improved and the mean differences associated with the final BDI-II score and the YBOCS score were significantly higher in the intervention compared with control arm of both groups of the patients with insomnia, who had associated psychiatric disorders.
An experimental study with a pretest/posttest design by Feyzabadi et al. 29 on the effect of 1-month intranasal V. odorata on 50 patients with chronic insomnia, who had not been previously treated, reported significant positive effects on inducing sleep in the patients and few adverse effects, which is consistent with the present findings in patients with insomnia obtained using a more effective design and examining several factors while reporting no serious adverse effects. In contrast to the design by Feyzabadi, a randomized double-blind placebo-controlled trial was used in the present study given the fact that intervention-based studies are considered the gold standard for comparison, as they yield almost 100% reliable evidence. 42
The present study aimed at obtaining credible data on the effect of V. odorata syrup as an add-on therapy on insomnia in patients with psychiatric disorders based on a pilot randomized double-blind placebo-controlled trial. The strengths of this study comprised a low dropout rate and therefore a high completion rate, and its limitations consisted of its relatively short duration of 1 month, which did not allow for long-term assessments of therapeutic effects and complications of the herbal product. To obtain more reliable results, similar studies are recommended to be conducted with longer courses of treatment and follow-up after the cessation of the treatment.
The other limitation was failing to collect information about changes in the lifestyle of the participants during the trial or any data that may provide some explanation for observed improvements other than the intervention itself. This type of limitation is also recommended that be addressed in future research. Given the subjective data collection method used in the present study, objective sleep measures such as polysomnography, observations, and other sensors are recommended that should be addressed by future researchers.
In addition to improvements in the total score of the PSQI and the scores of its components in both the study groups, significant improvements were observed in the BDI-II score and the YBOCS score of the patients with insomnia and mild-to-moderate depression or OCD in the intervention arms compared with the control arms after administering V. odorata syrup in the former. These improvements can be attributed to several factors, including the potential better control of the associated psychosocial disorders in the patients after their recovery from insomnia, and the therapeutic effects of an active ingredient of the plant on depression and OCD, which needs to be confirmed through controlled animal and human studies.
The potential recovery associated with the prescribed medication besides V. odorata syrup can also contribute to these improvements. Given that the medicinal treatment was the same in both the intervention and control arms, this possibility should be confirmed in the future by examining the efficacy of the V. odorata syrup in those not receiving any medications. Distributing sleep hygiene worksheets among the patients and providing them with instructions at the beginning of the study can also contribute to the outcomes, which should be also confirmed in the future by examining the efficacy of the V. odorata syrup in patients receiving no sleep hygiene trainings given that these worksheets were distributed in both the intervention and control arms.
Moreover, a potential bias toward complementary medicine in the subjects can partly explain those observed improvements in this study.
Conclusion
Administering V. odorata syrup caused significant improvements in the PSQI score in patients with depression and OCD having insomnia, BDI-II score in patients with depression and insomnia, and the YBOCS score in those with OCD and insomnia.
Footnotes
Acknowledgment
The authors would like to express their gratitude to the Deputy of Research of Shahed University of Medical Sciences for their support.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.