
Abstract
Objective:
Traditional Chinese Medicines (TCMs), as well as physiotherapy and chemical drugs, are recommended for the treatment of cervical spondylosis by Chinese guidelines for cervical spondylosis diagnosis and treatment. The aim of this study was to evaluate whether TCM Jingshu Granules are cost-effective in patients with cervical radiculopathy in China.
Methods:
A multicenter, double-blinded, randomized placebo-controlled trial was performed. A total of 480 patients were recruited from 14 tertiary hospitals in China and were randomly divided into an experimental group (Jingshu Granules) or control group (placebo) at a 3:1 ratio. All patients received 4 weeks of treatment. Clinical outcomes and cost data were collected during the trial, including the neck disability index (NDI), visual analog scale (VAS) of pain, VAS of numbness, 36-Item Short Form Health Survey (SF-36) score, willingness to pay (WTP) for VAS of pain, direct medical costs, and transport costs. From a social perspective, a decision-tree model and cost-effectiveness analysis were conducted.
Results:
The treatment group has a significant advantage in reducing NDI (9.41 ± 10.51 vs. 4.83 ± 8.43, p < 0.05), VAS of pain (22.72 ± 15.08 vs. 12.86 ± 13.45, p < 0.05), and VAS of numbness (16.96 ± 17.53 vs. 11.64 ± 16.54, p < 0.05), respectively, while there was no significant difference in the improvement of quality of life (QoL; SF-36 score, p > 0.05). The expected mean cost of the experimental group was 1144.34 yuan, and the effective rates were 57.9% for NDI and 72.9% for VAS of pain. The expected mean cost of the control group was 767.41 yuan, and the effective rates were 33.3% for NDI and 51.6% for VAS of pain. For the primary indicators (VAS of pain and NDI), the incremental cost-effectiveness ratio was 17.69 and 15.32, respectively. The WTP per efficacy for pain resolution of patients was 19.10 yuan. Setting the WTP as threshold, Jingshu Granules were found to be a cost-effectiveness strategy, and sensitivity analysis showed that the effective rates and inspection fees of both groups had a greater impact on the results of both groups.
Conclusions:
Jingshu Granules were shown to be effective for treating patients with cervical radiculopathy. This treatment was found to be cost-effective when considering VAS of pain and NDI as clinical outcome indicators compared to no treatment (placebo). A clinical study with longer duration or real world study is needed to determine the impact on QoL of patients in the future.
Introduction
The tremendous pressure of modern work and study together with large changes in lifestyle have led to a marked increase in neck flexing, which has resulted in a higher prevalence of cervical spondylosis with a trend of prevalence in young adults. 1,2 A previous retrospective cohort study showed that among 47,560 patients with adult thoracolumbar spinal deformity, the prevalence of cervical spondylosis was 13.1%. 3 In China, the prevalence of cervical spondylosis has been estimated to be 13.76%, although it differs among the urban, suburban, and rural populations (13.07%, 15.97%, and 12.25%, respectively) and was higher in females than in males (16.51% vs. 10.49%, respectively). 2 According to a global burden of disease study, 4 neck pain was one of the top ten disability factors in 301 chronic diseases of patients from 188 countries. It has been shown that cervical spondylosis causes inconvenience to patients' daily life, thus impacting overall quality of life (QoL) and health. 2,5 –8
Cervical spondylosis has several types based on the clinical symptoms from the affected tissue, including cervical spondylotic myelopathy, cervical radiculopathy (CR), neck-type cervical spondylosis, and other types. 9 Among them, the incidence of CR is 60%–70% of all cervical spondylosis cases, 10,11 which accounts for the highest proportion. In 2010, the North American Spine Society (NASS) defined CR as “pain in a radicular pattern in one or both upper extremities related to compression and/or irritation of one or more cervical nerve roots. Frequent signs and symptoms include varying degrees of sensory, motor, and reflex changes, as well as dysesthesias and paresthesias related to nerve roots without evidence of spinal cord dysfunction (myelopathy).” 12
Treatment options for CR can be loosely classified into surgical treatment and nonsurgical treatment. 13 Approximately 75%–90% 14 can achieve symptom relief using a conservative approach. In 2015, a consensus 15 was reached on nonsurgical approaches for treating CR, which include neck immobilization, physiotherapy, and pharmaceutic intervention. Drugs such as non-steroidal anti-inflammatory drugs, opiates, neurotrophic drugs, muscle relaxants, hydrating agents, steroids, and Traditional Chinese Medicines (TCMs) can be used according to patient condition. The WHO Western Pacific Region guidelines on treating CR list the strength of recommendation of TCMs as B, suggesting that basic therapy must restore liver and kidney function, thus promoting blood circulation and relieving blood stasis. 16 However, the Evidence-based Clinical Guidelines for Multidisciplinary Spine Care developed by the North American Spine Association state that current research and evidence are not sufficient to support the use of pharmaceuticals for the treatment of CR. 17
Compared to chemical compounds, natural compounds based on TCM theory (i.e., TCMs) have unique advantages for improving clinical symptoms, reducing complications, protecting target organs, and avoiding adverse reactions. Therefore, they are widely used in clinical practice. Jingshu Granules, which came to market in 2001 as an essential drug in China (national list of essential medicines, v2009, v2012, and v2018), contain concentrated herbal granules made of extracts from notoginseng radix, angelicae sinensis radix, carthami flos, gastrodiae rhizoma, chuanxiong rhizoma, cinnamomi cortex, and bovis calculus artifactus. These granules function by warming and activating meridian, improving blood flow, clearing blood stasis, and promoting microcirculation and blood rheology. In this study, the authors provide evidence for the use of Jingshu Granules in CR therapy and related policy-making initiatives by conducting a pharmacoeconomic evaluation for the treatment of CR based on clinical efficacy obtained from a randomized controlled trial. The aim of this study was to evaluate whether Jingshu Granules are more clinically effective and cost effective than placebo in patients with CR in China.
Materials and Methods
Study design
A multicenter, double-blind, placebo parallel-controlled clinical trial was performed. One course of treatment was defined as 4 weeks since the study was placebo controlled and for the convenience of observing the drug's efficacy. This study (Registration No. ChiCTR1900021012) was conducted in strict compliance with the Helsinki Declaration and Good Clinical Practice and was approved by the Ethics Committee, Peking Union Medical College Hospital (Approval No. HS-927). The authors chose clinical output and cost as the core elements of value assessment for the intervention. A cost-effectiveness analysis was performed based on a decision-tree model.
Study population and treatment
From July 7, 2016 to June 26, 2017, a total of 480 patients were recruited from 14 tertiary hospitals, which are located in Beijing, Shanghai, Guangdong, Jiangsu, Zhejiang, Tianjin, Henan, Hubei, Jiangxi, and Chongqing; these hospitals are distributed in most areas of China except for northwest and northeast regions. Patients were randomly divided into the experimental group (Jingshu Granules) and the control group (placebo) at a 3:1 ratio. Patients were eligible for the trial if they fulfilled the following inclusion criteria: (1) diagnosed with CR; (2) 4 points ≤ visual analog scale (VAS) ≤6 points; (3) 18–65 years of age; and (4) agreed to participate in study and provided informed consent.
Patients were not eligible if they fulfilled any of the following exclusion criteria: (1) diagnosed with cervical spondylotic myelopathy; (2) experiencing pain from cervical extraspinal lesions, such as thoracic outlet syndrome, tennis elbow, carpal tunnel syndrome, cubital tunnel syndrome, frozen shoulder, biceps tendinitis, and so on; (3) required surgery to treat CR, defined as (i) ineffective symptom management or effective but frequently recurrent symptoms that severely affected normal life and work after receiving standard and systematic nonsurgical therapies for more than 3–6 months; (ii) progressive muscle atrophy due to cervical root lesions; or (iii) significant symptoms of cervical root irritation or severe acute pain that seriously affected sleep and normal life; (4) presence of serious primary disease affecting the cardiovascular system, cerebrovascular system, liver, kidney, or hematopoietic system; (5) abnormal liver and kidney function (alanine aminotransferase, aspartate aminotransferase > 3 upper limit of normal (ULN), or Creatinine > ULN); (6) history of mental illness, alcohol, or drug abuse; (7) known allergy to multiple drugs or any ingredient of the study drug; (8) pregnant, willing-to-be pregnant (except for termination of pregnancy), or lactating women; (9) use of any other drug intended to treat CR 1 week before study drug administration; (10) participation in other drug clinical studies 3 months before screening; or (11) patients who were inappropriate to participate in the study for other reasons judged by investigators.
In the clinical trial, patients and investigators were all blinded. A multistage, stratified random method was used to assign patients into the two groups. Consecutive numbers equal to the sample size were generated by SAS software and then assigned to patients. The corresponding drugs were sequentially administered according to the order of the subjects. Placebo was chosen for the control arm since there are currently no highly effective drugs available for the treatment of CR and patients' condition does not progress rapidly without medication for 1 month. Patients in the experimental group received Jingshu granules (batch No. 150801; specification: 6 g/bag) orally thrice a day using one bag each time. Patients in the control group received placebo (batch No. S150801; specification: 6 g/bag) using the same approach. The package, size, shape, color, and smell of placebo were consistent with Jingshu granules. Both drugs were manufactured by Anhui Jingfang Pharmaceutical Co., Ltd.
Measuring clinical efficacy
Neck disability index (NDI), VAS of pain, and VAS of numbness were measured at the start of dosing, as well as 2 and 4 weeks after the start of dosing. Changes between the observations at the fourth week and starting point were calculated as the performance metrics. To further measure drug effectiveness, the efficacy classification of the main clinical indicators (NDI and VAS of pain) was distinguished. To assess the health status of patients, the SF-36 questionnaire was used, which generates scores from eight dimensions based on patient reported outcomes.
NDI was published in 1991 and was the first instrument designed to assess self-rated disability in patients with neck pain. 18 It includes 10 items, each with 6 response categories (range 0–5; total score range 0–50). The higher the score, the greater the disability. NDI is calculated as follows: NDI (%) = (total score for each item/number of items completed by the subject × 5) × 100%. In the reference “Traditional Chinese Medicine Diagnosis and Treatment Efficacy Standards,” which was published by the State Administration of Traditional Chinese Medicine of the People's Republic of China in 1995, 19 the evaluation criteria of NDI efficiency are as follows: (1) clinical recovery: disappearance of the original symptoms and restoration of the muscular strength and functions of the neck and upper limb to normal so that patients can participate in labor and work unaffectedly; symptoms relieved ≥90%; (2) remarkably effective: original symptoms improve significantly, pain in the neck, shoulder, and back is relieved, and functions of the neck and upper limb improve remarkably; symptoms relieved ≥75%; (3) improved: the original symptoms and the pain in the neck and shoulder is alleviated, but some symptoms and dysfunction still exist; symptoms relieved ≥30%; and (4) invalid: no change in symptoms or even worse after treatment; symptoms are relieved ≤30%. The proportions of patients achieving classification of clinical recovery, remarkably effective, and improved were added together as the effective rates.
In 1972, Woodforde and Merskey 20 first used VAS for pain intensity assessment. VAS is characterized by a line of 0–100 mm, whereby one end represents no pain and the other end represents unbearably severe pain. The degree of pain is indicated by patients at a certain point on the line. According to the weighting method, 21 the percentage of pain relief = A − B/A × 100%, where A represents the VAS score before administration and B represents the VAS score after administration. The efficacy grading standards are as follows: (1) clinical recovery: VAS weighted value ≥75%; (2) remarkably effective: VAS weighted value of 50%–75%; (3) improved: VAS weighted value of 25%–50%; and (4) invalid: VAS weighted value ≤25%. The proportions of patients achieving classification of clinical recovery, remarkably effective, and improved were added together as the effective rates.
Measuring costs
Considering the current medical situation of patients with CR in the real world, the cost measurement only included costs that were incurred when patients sought medical treatment and excluded the costs of standard tests used for clinical research, such as computed tomography (CT), ECG, liver and renal function tests, and routine examination of hematuria. From a social perspective, the authors also tracked medical and nonmedical costs of patients, including transportation fees, registration fees, inspection fees, drug costs, and treatment for adverse reactions incurred at the start of dosing, as well as 2 and 4 weeks after the start of dosing. The authors then calculated the total cost per patient over 4 weeks. The study involved 14 hospitals across 11 provinces. The bid price of Jingshu Granules in the corresponding province in 2017 was adopted and then converted to a unit price of test drugs using a coefficient. Since the clinical trial duration was 4 weeks, the discount rate was 0%.
The authors also measured patients' willingness to pay (WTP) for pain treatment at the three time points by asking the following question: If there is a treatment available that can make your pain caused by CR completely disappear until it no longer occurs, how much are you willing to pay for it? An open-ended question format was adapted, which means no numerical restrictions were imposed on the respondent's WTP. Therefore, this WTP measurement not only reflects the patients' pain improvement but also provides a threshold for measuring cost-effectiveness.
Model description
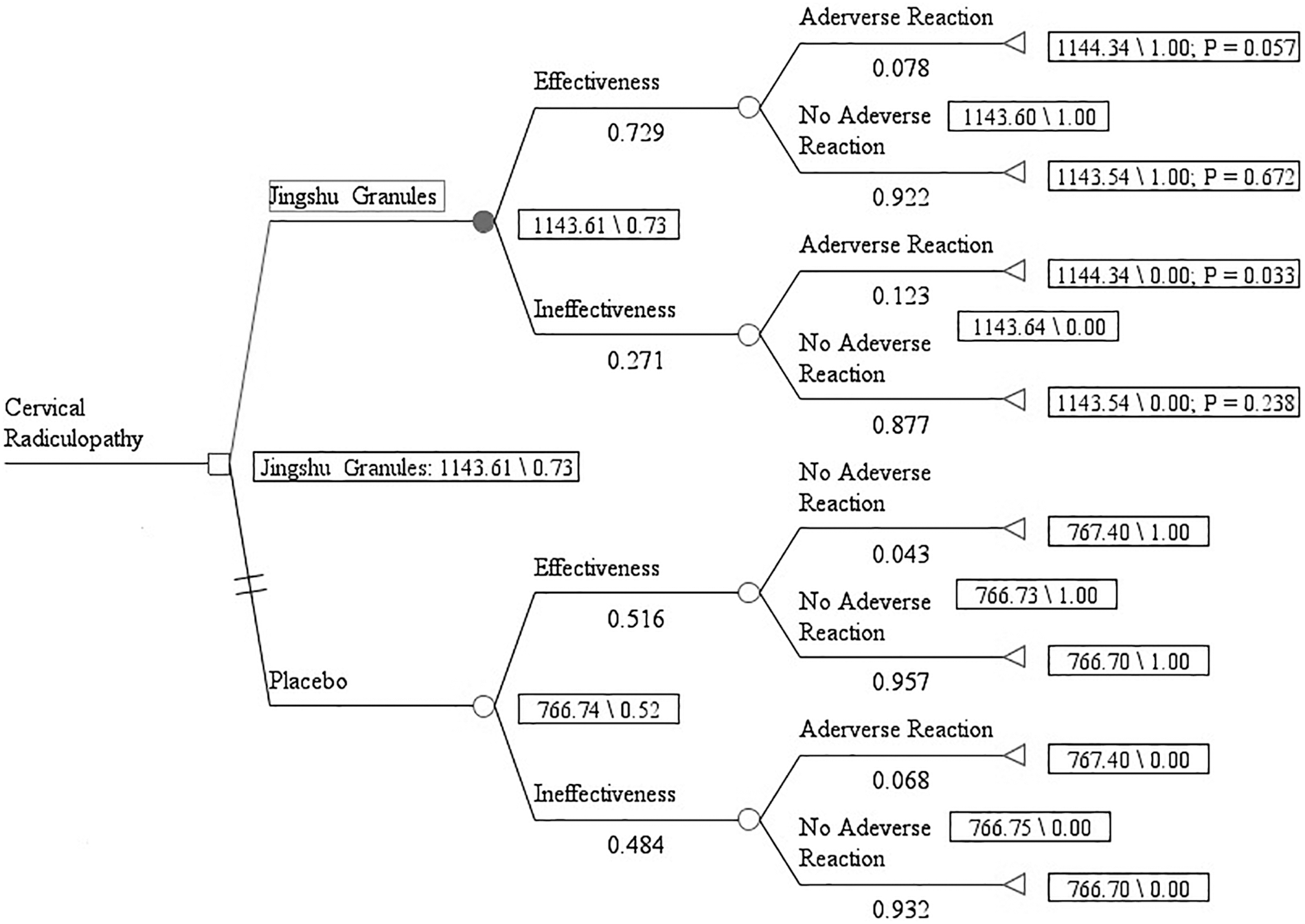
A simple decision-tree model was constructed using TreeAge Pro 2011 to analyze the cost-effectiveness of Jingshu Granules, since the condition of CR patients was not complicated (Fig. 1). In this model, the interventions were Jingshu Granules and placebo, and the outcomes were assessed as effective rates or ineffective rates. Adverse drug reactions may also occur during treatment. The authors set the duration as one course of treatment (4 weeks) and conducted a short-term pharmacoeconomic evaluation.

Decision-tree model structure. # indicates the complement of the corresponding branch probability. P, probability.
Model inputs were derived from clinical trials. According to the effective and invalid frequency, as well as the cases of adverse drug reactions, the effective rates and the incidence of adverse drug reactions were calculated. The parameter “0” indicated an invalid outcome, while “1” indicated an effective outcome. The authors calculated the incremental cost-effectiveness ratio (ICER) after costs and effectiveness data were collected. Due to the wide geographical distribution of hospitals where the clinical trial was conducted, differences and uncertainties in the cost measurement existed, and the efficacy of treatment and compliance varied with patients. Therefore, a sensitivity analysis was performed.
Statistical analysis
The data were double entered using EPIDATA 3.1, and statistical analysis of the data was performed using EXCEL 2007 and SPSS 17.0. The authors conducted chi-squared tests for basic information and effective rates of patients. If the differences between clinical outcomes were satisfied with normality and homogeneity of variance, then a t test was adapted; if not, the Wilcoxon rank sum test was considered. The authors used the rank sum test for costs because of its non-normality. All statistical tests used a two-sided significance level of 0.05. Statistical significance was considered as p ≤ 0.05.
Results
Patient characteristics
A total of 480 patients were enrolled in the trial with 360 patients in the experimental group and 120 patients in the control group. After removing cases that were lost to follow-up or did not meet eligibility requirements, 299 patients in the experimental group and 91 patients in the control group were included in the final analysis (Fig. 2). There were no significant differences in the education, occupation, total annual household income, transportation for seeking medical advice, or the degree of restriction of normal activities of the patients in the two groups (p > 0.05; Table 1).

Flow chart of patients in the course of the research.
Basic Information of Patients in the Two Groups
Efficacy outcomes
Patients in the experimental group (Jingshu Granules) had a statistically significant reduction in NDI, VAS of pain, and VAS of numbness compared to patients in the placebo arm. Moreover, patients in the treatment arm exhibited significant mean reductions after 4 weeks in NDI (9.41 ± 10.51 vs. 4.83 ± 8.43, p < 0.05), VAS of pain (22.72 ± 15.08 vs. 12.86 ± 13.45, p < 0.05), and VAS of numbness (16.96 ± 17.53 vs. 11.64 ± 16.54, p < 0.05), respectively, compared to the start of dosing (Table 2).
Outcomes of Neck Disability Index, Visual Analog Scale of Pain, and Visual Analog Scale of Numbness
NDI, neck disability index; VAS, visual analog scale.
The authors next determined the efficacy classification for NDI and VAS of pain since they were primary indicators. As shown in Table 3, the effective rate of the experimental group was 24.53% higher than the placebo group (57.86% vs. 33.33%, p < 0.001, respectively) for NDI and 21.26% higher than the placebo group (72.91% vs. 51.65%, p < 0.001, respectively) for the VAS of pain.
The Grades of Efficacy for the Main Indicators in the Two Groups
For the SF-36 questionnaire, no statistically significant differences were observed between the two groups (p > 0.05), although most of the changes in the eight dimensions were better in the treatment arm compared to placebo (Table 4).
SF-36 Score of Two Groups at Each Time Point
SF-34, 36-Item Short Form Health Survey.
The adverse reaction rates were 9.36% in the experimental group and 5.49% in the control group (Table 5). Diarrhea, upper respiratory tract infection, headache, and dizziness were the most frequently noted adverse reactions. Given that most of the adverse reactions were mild and resolved without treatment, this study did not consider them in the efficacy evaluation but mainly measured the corresponding costs for treatments.
Adverse Reaction Rates for the Two Groups
Costs and cost-effectiveness
The costs of each medical item and total costs are listed in Table 6. The total cost for each patient in the experimental group was 1144.34 yuan and 767.41 yuan for the control group. Since the expected cost and output of the experimental group were all greater than the control group, an incremental cost-effectiveness analysis was required. The ICER was used as the main criterion for determining whether Jingshu Granules were cost-effective by analyzing whether the marginal cost of unit efficacy was below the acceptable level (ICER) or not. Overall, treatment with Jingshu Granules incurred an incremental cost of 376.87 yuan and gained more effective rates of 24.6% for NDI and 21.3% for VAS of pain, yielding an ICER of 15.32 and 17.69, respectively. The results from the decision-tree model and cost-effectiveness assessment are shown in Figures 3 and 4 and Table 7.

Results of the decision-tree model structure for NDI. NDI, neck disability index.
Results of the decision-tree model structure for VAS of pain. VAS, visual analog scale.
Costs of Each Medical Item and Total Costs in the Two Groups
Main Outcomes of Economic Evaluation for Neck Disability Index and Visual Analog Scale
ICER, incremental cost-effectiveness ratio.
In this study, the authors measured patients' WTP for elimination of pain, which showed a downward trend for both groups as the treatment progressed (Table 8). The data clearly showed that changes in the experimental group over 4 weeks were greater than in the control group (1392.16 vs. 1100.00, p < 0.05). The more WTP is reduced, the better the patients' pain improvement, so the authors divided the reduced WTP by the effective rate gained in the Jingshu Granules arm to get the patients' WTP per efficacy as the threshold. When considering VAS of pain as an outcome indicator, Jingshu granules were found to be cost-effective since the reduced WTP of pain per efficacy was 1392.16 yuan/72.9% which equals to 19.10.
Patients' Willingness to Pay for Pain at Three Time Points
Although patients' WTP for improving NDI was difficult to measure in view of patients' cognitive burden caused by the complicated nature of NDI, which is composed of ten aspects on neck pain and abilities related to daily activities, the threshold above can nevertheless be applied to NDI given that it already included pain measurement and more. Therefore, Jingshu Granules were found to be cost-effective compared to placebo when considering VAS of pain and NDI as the clinical outcome indicators, since the WTP for NDI must be higher than the WTP for pain.
Sensitivity analysis
If the data followed normal distribution, then the 95% confidence interval was taken as the range of values. If not, then the lower and upper quartiles were used as the range. The range of adverse reaction rates floated was set as ±10%, a one-way sensitivity analysis was performed, and the results are presented as a tornado diagram. As shown in Figure 5, the effective rates and inspection fees of both groups had a greater impact on the results regarding NDI. The results of VAS of pain were highly similar to NDI and thus will not be described further.

The results of one-way sensitivity analysis for NDI.
Discussion
This study found that Jingshu Granules had significant advantages in reducing NDI, VAS of pain, and VAS of numbness compared to placebo control, while no significant improvement was observed in QoL between the two groups. Zheng et al. previously showed in animals that Jingshu Granules can control the pain caused by CR. 22 Moreover, a previous clinical trial completed at four hospitals showed that Jingshu Granules can reduce the TCM syndrome score and VAS score and increase the scale score of clinical efficacy significantly. 23 Their study also confirmed the effectiveness of Jingshu Granules, but the results from the patient-reported outcome score may need a longer treatment duration to be verified.
The clinical treatment options and the number of economic studies on various treatments for CR are diverse, but to date there has been insufficient economic evaluation of CR treatment with a single drug. Their study calculated cost, efficacy, and improvement of disease burden based on the medical situation of patients with CR in the real world. The cost-effectiveness analysis showed that CR treatment with Jingshu Granules was economically acceptable. Thus, these findings could serve as evidence for the inclusion of drug therapy in clinical guidelines for the treatment of CR.
Placebo-controlled trials are most lacking for existing nonsurgical therapies for CR, since the vast majority of studies used positive control drugs to obtain relative effects. 24 Placebos are known to induce certain effects in some diseases, such as with analgesia and depression, where the effective rate can be as high as 60% and 30%–40%, respectively. Therefore, it was reasonable to observe the effective rates of the placebo in reducing NDI and VAS of pain in their study. The cost of placebo was negligible, and the efficacy was influenced by many factors compared to positive control drugs adapted in general pharmacoeconomic evaluations, which may limit the value of economic evaluation. Considering that the targeted disease was CR, whereby one approach often taken by patients is to do nothing, the findings of this study have considerable impact given that a placebo control represents a potential real-world situation.
The economic evaluation in this study has several limitations. The clinical efficacy data were obtained from a multicenter, double-blind, placebo parallel-controlled clinical trial, which may be subject to potential selection and information bias inherent in the study design, although with higher internal validity, promotion of applicability remains to be confirmed. Unfortunately, the difference in the SF-36 scores between the two groups was not significant, and thus, long-term follow-up would be more helpful for identifying differences. Finally, the authors did not count the adverse reactions in the efficacy since most of them resolved without treatment. To further improve the accuracy of the assessment, a long-term clinical study or real-world study might be needed for high-quality evidence.
Conclusion
Compared with placebo, Jingshu Granules are effective in reducing NDI, VAS of pain, and VAS of numbness. When considering NDI and VAS of pain as clinical outcome indicators, treatment with Jingshu Granules is a cost-effective option for patients with CR.
Footnotes
Acknowledgments
The founders participated in the design of the clinical trial, as well as data collection of costs and clinical outcomes, but had no role in the design of the pharmacoeconomic research, data analysis, or data interpretation.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The study was funded by InCROM CHINA.