
Abstract
Background:
The commercialization of essential oils has expanded their presence in the United States, and emerging studies demonstrate that they may have a place in Western medicine. One oil with a significant body of evidence is lavender essential oil, which may have benefits in wound healing.
Objectives:
This review aims to present the scientific literature on therapeutic lavender essential oil with the goal of expanding the current repertoire of cost-effective wound healing options available to physicians and patients.
Methods:
A review was conducted according to PRISMA guidelines in PubMed, Cochrane Library, and Embase from June 2018 through March 2019 to identify articles related to lavender essential oil in the context of wound healing.
Results:
This search yielded 36 unique studies, 20 of which remained after screening. This review utilizes human clinical trials (n = 7), animal trials (n = 5), in vitro studies (n = 2), and previously conducted reviews (n = 6). Overall, these studies demonstrated a faster rate of wound healing, increased expression of collagen, and enhanced activity of proteins involved in the tissue remodeling process in wounds treated with lavender essential oil.
Conclusions:
The current body of literature suggests a potential therapeutic benefit of lavender essential oil in wound healing. However, standardization of the chemical composition and additional high-quality human clinical trials are needed to further evaluate the safety and efficacy of lavender essential oil in clinical practice.
Introduction
Postoperative wounds can be disfiguring, inconvenient, and disabling. Current wound care modalities, however, are limited, dated, and often expensive. In 2004, it was predicted that by 2010, the U.S. public would be spending over $15 billion annually on wound care products. 1 In 2014, it was estimated Medicare alone spent between $28.1 and $96.8 billion on care for all wound types, including surgical and traumatic wounds and diabetic and vascular ulcers. A conservative estimate for the average cost of caring for an individual wound in that same year was $3,415. Surgical wounds, although not the most expensive on a per-wound basis, were the most prevalent wound type and resulted in the highest overall spending. This burden has since increased as the rate of surgical procedures in this country continues to climb. 2,3 These rising costs have created a growing demand for reliable cost-effective options. As a result, many studies have been conducted in recent years to investigate claims of the wound healing properties of various alternative therapies. One therapy with a significant body of evidence is lavender essential oil.
Lavender's use in medicine can be traced back to the first century
Lavender's utility in wound healing specifically was discovered in 1910 when a French chemist applied lavender essential oil to his burnt hand following a laboratory accident and reported a quick healing process. It was subsequently used by military physicians in World War II to disinfect and heal wounds. 6 Recently, there has been a resurgence of interest in lavender essential oil's utility in wound healing, although it has been over a decade since the literature has been reviewed and consolidated in a clinically meaningful way. To do this, the authors summarize the evidence from in vitro, animal, and human clinical trials to describe the effects of lavender essential oil on multiple types of wounds, including surgical skin wounds, simulated inflammatory wounds, episiotomy wounds, and oral mucosal wounds. In addition, they outline possible mechanisms of action for the effects noted in the reviewed studies and evaluate whether they should be considered a therapeutic option for future clinical practice (Fig. 1).

Photograph of Lavandula angustifolia Mill, used with permission from Gary A. Monroe. 11 Lavandula (known commonly as lavender) is a genus of flowering plant comprising over 20 unique species. Lavender's essential oil is produced by secretory structures on the surface of the plant. The essential oil contains a number of volatile compounds, including terpenoids, a class of oxygenated hydrocarbons. Predominant among these are linalool, a 10-carbon terpenoid, and its acetate ester, linalyl acetate. 4,12 These terpenoids are reported to protect the plant against environmental changes in light, temperature, and CO2 levels. 4 They also have a proven role in repelling pathogens and herbivorous predators while attracting pollinators. 13
Methods
This review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) protocol. Searches were performed from June 2018 to March 2019 in Embase, MEDLINE via PubMed, and Cochrane Library using MeSH terms and keywords. The terms “lavender essential oil” AND “wound healing” were used for each of the searches, and there was no restriction placed on particular years of publication or study design. The search yielded 36 unique articles, 35 of which remained after screening out articles not available in English. Abstracts of the remaining articles were screened for relevance to lavender essential oil and wound healing. Fifteen articles were excluded at this level, resulting in 20 studies to be included in this review.
A high percentage of relevant articles were yielded by this method, likely due to the specific search terms and limited number of databases used, as well as the inclusion of animal and in vitro studies in addition to human clinical trials. More details on methodology decisions can be found in the Discussion.
The quality of the human clinical trials selected for inclusion was determined based on the adequacy of random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, and completeness of outcome data, as well as the lack of selective reporting and other bias. This assessment of risk of bias, performed in alignment with the assessment methods described in the Cochrane Handbook for Systematic Reviews of Interventions, was used to identify limitations of these included studies (Fig. 2).
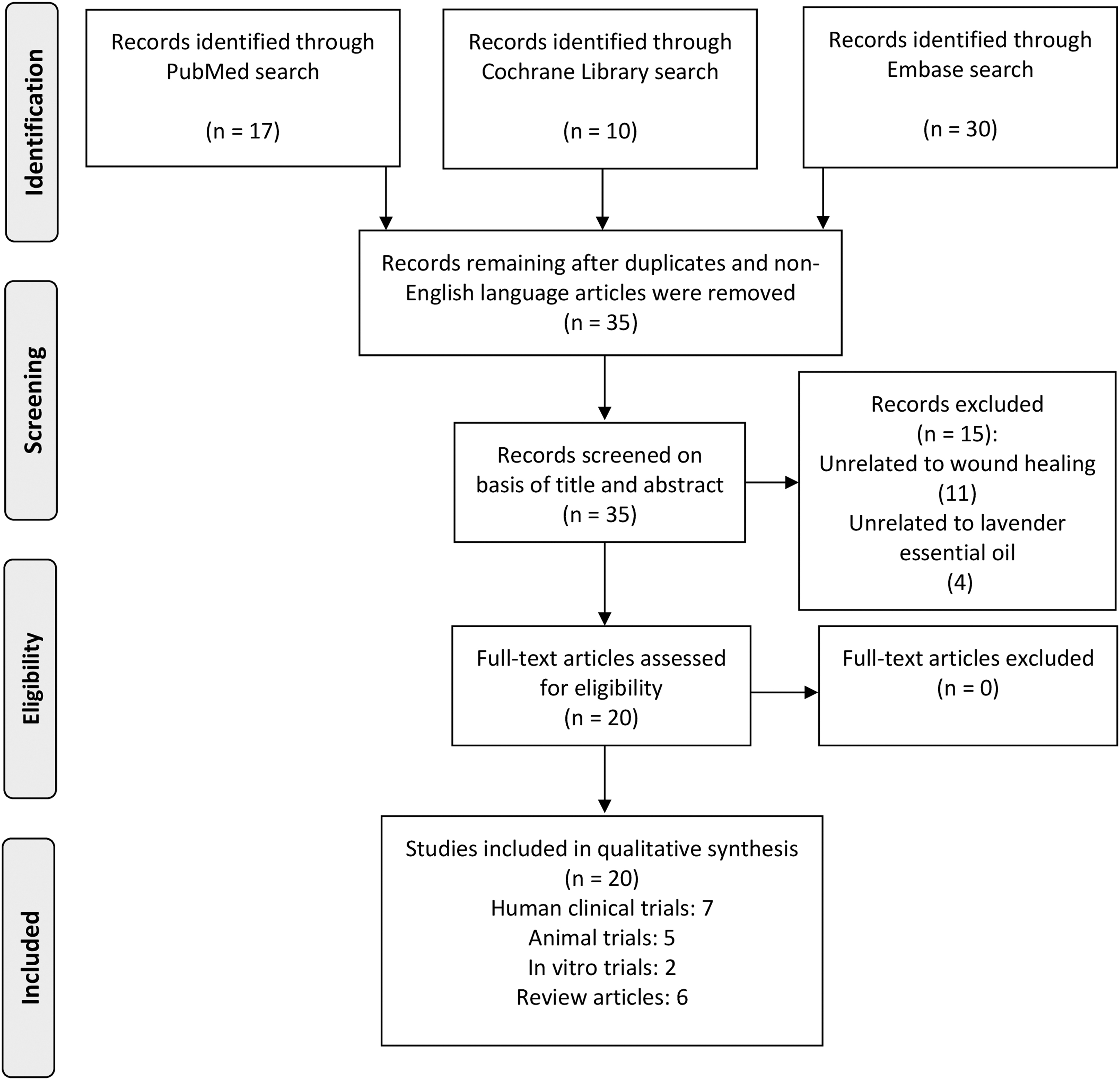
Flow diagram demonstrating the search methods, adapted from Preferred Reporting Items for Systematic Reviews and Meta-analyses: The PRISMA Statement. From: Moher et al. 43
Results
Study characteristics
From the 20 studies included in this review, 9 covered general skin wound healing, 3 related specifically to the healing of episiotomy wounds, 1 involved healing of aphthous ulcers, 1 detailed the cytotoxicity of lavender essential oil, and 6 were previously conducted reviews. The majority of studies were classified as level of evidence (LOE) II (12, 60%), whereas the remaining studies were classified as LOE I (4, 20%), LOE III (2, 10%), or were in vitro studies on human skin cells, considered here to be LOE IV (2, 10%). Studies were graded according to the Oxford Centre for Evidence-Based Medicine 2011 Levels of Evidence. Please see Table 1 for more detailed information about the included studies.
Studies Included in This Review
EGF, epidermal growth factor; FGF-2, fibroblast growth factor-2.
Previously conducted reviews
Three reviews conducted between 2007 and 2017 included a total of five studies relevant to lavender essential oil and wound healing; each of these studies is included in this review and described in detail in the next section. 14 –16 A review by Cavanagh and Wilkinson (2002, LOE II) investigated lavender essential oil's use in eczema and alopecia, although the literature showed little convincing evidence for using lavender essential oil for these conditions. 17 To inform midwives about the use of lavender essential oil in healing perineal skin trauma, Jones (2011, LOE I) conducted a literature review of studies (n = 6) that discussed the topical application of lavender essential oil. 18 Overall, these reviews had few studies to include with respect to lavender essential oil and wound healing, giving them limited ability to draw meaningful conclusions.
Pérez-Recalde et al. (2018, LOE I) conducted a literature review investigating the wound healing value of biopolymers (proteins such as collagen, and polysaccharides such as chitosan) enhanced with essential oils. The authors found only one study evaluating a lavender essential oil and biopolymer blend: an alginate film mixed with glycerol as a plasticizer, Igepal as a surfactant, and lavender essential oil at concentrations of 16%, 50%, or 66% of the film dry weight. The results of this study demonstrated the antimicrobial and antifungal properties of the 50% and 66% lavender essential oil-enhanced films as they inhibited the growth of the two microorganisms tested, Escherichia coli and Candida albicans.
The authors of the review suggested that, although most essential oils had not yet been adequately studied in combination with biopolymers, the results of the included studies and the previously described effects of essential oils and biopolymers in isolation could be useful in designing new antimicrobial wound dressings. 19
Human trials
Interventional human trials have been conducted over the past two decades to elucidate the role lavender essential oil might play in the healing of skin wounds. These studies used a variety of approaches to evaluate lavender essential oil's effects and determine its utility as a potential treatment. The risk of bias in each of the seven included trials was determined with results displayed in Figure 3. A limitation revealed by this assessment is the lack of blinded interventions found in many of the studies. Blinding of participants and personnel was likely forgone in several studies as essential oils are characteristically fragrant and difficult to mask, making it unlikely that any of the study participants would be truly blinded to their treatment.
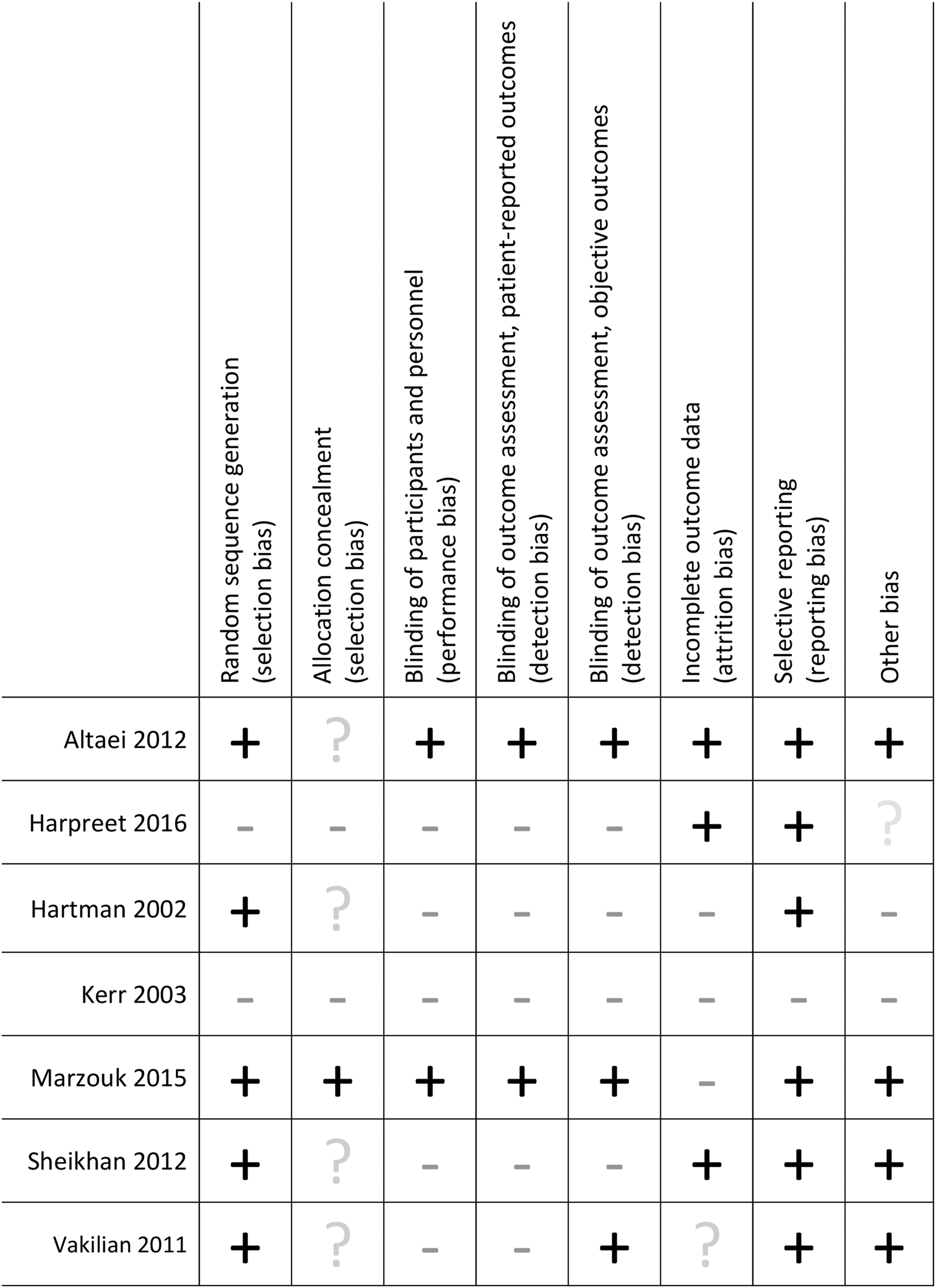
Risk of bias chart created to assess the validity of the included human clinical trials. Addition symbols indicate low risk of bias from a particular criterion, while subtraction symbols indicate high risk, and question marks indicate unclear risk.
A study by Hartman and Coetzee (2002, LOE III) evaluated the effect of a combination of lavender and chamomile essential oils (6% combined concentration) on chronic wound healing. The authors selected lavender essential oil for its reported skin-regenerative, antibacterial, and analgesic properties, and they included chamomile oil for its reported anti-inflammatory and analgesic properties. The study involved eight patients with chronic ulcers present for three or more months, five of whom were treated with the essential oil blend and three of whom were treated with conventional methods, such as Granulex or a boric acid and hydrogen peroxide regimen. Researchers found that wounds treated with the essential oils healed more quickly with four of five wounds treated with the essential oils healing completely by the conclusion of the study (420 days out), and none of the three control wounds healing completely over the same time period. Given the small sample size and variation among wound characteristics, meaningful statistical analyses were unable to be completed. 20
Kerr (2002, LOE III) created a blend of essential oils in Aloe vera gel, presumably selected as the base for its moisturizing effect, to be used as an aromatherapeutic topical application for the management of common wounds such as skin tears and cracks, pressure injuries, and puncture wounds. The efficacy of daily use of the blend was tested on the wounds of over 100 residents and staff at private nursing homes over the course of the 3-year study. After three trials of undisclosed length using five formulas of varying concentrations, the author determined the most efficacious formula to be a blend of lavender (Lavandula angustifolia), German chamomile, myrrh, and tea tree essential oils (12% concentration of combined oils) in Aloe vera gel. Overall, a 100% success rate was reported for the final formula with regard to infection control, corroborated by subjective observations of reductions in odor, redness/inflammation, and healing time (compared with what would be expected from typical treatments). However, the study was unable to perform statistical testing because the collected data were not quantified and there were no controls. 21
A randomized-controlled trial conducted by Altaei (2012, LOE II) evaluated lavender essential oil's utility in the healing of oral mucosal wounds. Half of the 115 subjects with recurrent aphthous ulceration (canker sores) were treated with 2% lavender essential oil (two 36 mg/drops, three times daily), and the other half received a glycerol product without active ingredients as a placebo. The subjects were evaluated by a dentist during the healing process. In the group treated with lavender, 100% of the ulcers were completely healed within 4 days and had no remaining symptoms such as edema or pain. The ulcers of the placebo group remained at the sixth day of treatment (p < 0.0001), and it was not reported how long the ulcers persisted thereafter. In addition, treatment with lavender essential oil significantly reduced erythema in 2.3 ± 0.3 days compared with the placebo group, which continued to have noticeable redness for 10.5 ± 1.2 days (p = 0.0003). 22
Recent clinical studies have demonstrated the anti-inflammatory and analgesic effects of lavender essential oil in gynecologic wound healing. Vakilian et al. (2011, LOE II) conducted a randomized-controlled trial with 120 women demonstrating that treatment with lavender essential oil significantly reduced erythema but had a nonsignificant effect on pain (p < 0.001 and p = 0.06, respectively) after episiotomy relative to control groups. 23 A subsequent randomized clinical trial conducted by Marzouk et al. (2015, LOE II) in status-postepisiotomy patients demonstrated similar results with lavender essential oil-treated groups achieving significant reductions in the REEDA (redness, edema, ecchymosis, discharge, and approximation) score in addition to the visual analog scale for pain relative to controls (p = 0.013 and p = 0.011, respectively). 24
A clinical trial performed by Sheikhan et al. (2012, LOE II) in an Iranian hospital corroborates these results. Researchers found that both pain intensity and REEDA scores were significantly lower (p < 0.001 and p < 0.001, respectively) at 5 days postepisiotomy for the group of women treated with 0.96% lavender essential oil compared with those treated with betadine. 25 Similarly, Harpreet et al. (2016, LOE II) compared the healing of episiotomy wounds in postnatal mothers who were treated with either lavender essential oil or betadine. Using the REEDA scale for comparison, researchers found that the application of lavender essential oil was more effective in wound healing for the first 3 days (p = 0.035), but the two treatments were equally effective by day 5 (p < 0.05). 26
Animal studies
Several experimental animal studies have been conducted to further investigate lavender essential oil's role in wound healing. In addition, some researchers propose mechanisms through which lavender essential oil may act by detailing its observed biomolecular effects on healing wounds.
Altaei (2012, LOE II) demonstrated that lavender essential oil aided in the healing of oral mucosal wounds in rabbits (n = 18). The author conducted a randomized placebo-controlled trial in which he found that oral wounds treated with 2% lavender essential oil twice daily for 5 days had an increased rate of mucosal repair (p = 0.001) when compared with a group treated with a glycerol product free of active ingredients. 22
Koca Kutlu et al. (2013, LOE II) compared the effects of various wound healing modalities using incision wounds in rats. Four groups of rats (n = 4 in each group) were wounded and then treated with transcutaneous electrical nerve stimulation (TENS), saline solution, povidone/iodine, or L. angustifolia essential oil. In addition, one group of rats was wounded with no treatment, and one healthy group was kept without incision wounds. After the 5-day treatment period, researchers excised the incision sites and surrounding skin for analysis of growth factor expression, including epidermal growth factor (EGF, predominantly seen during active wound contraction), platelet-derived growth factor-A (PDGF-A, seen in all stages of wound healing), and fibroblast growth factor-2 (FGF-2, predominantly seen during granulation tissue formation).
They found that expression of PDGF-A and EGF was highest in the group treated with TENS. Lavender essential oil had modest effects, thought to be exerted through significantly increased expression of EGF and FGF-2 (p < 0.05 and p < 0.05), compared with the untreated group. It was also reported to have anti-inflammatory and antimicrobial action as the wounds treated with lavender revealed no signs of edema, discharge, or local infection. Similar findings were not reported for any other group. 27
A study conducted by Ben Djemaa et al. (2016, LOE II) investigated the wound healing efficacy of 4% Lavandula aspic L. essential oil applied to excisional wounds in rats compared with untreated, vehicle-treated, and reference drug-treated (Cytolnat Centella cream) groups. The researchers followed macroscopic wound contraction and epithelialization. Over a span of 14 days, the rate of wound contraction in the group treated with 4% lavender essential oil demonstrated “almost total” closure, whereas the reference drug-treated wounds were completely closed by day 14. At that same point in time, the untreated and vehicle-treated wounds were incompletely closed.
Thus, the lavender-treated group, compared with the untreated control group, healed at a faster rate (p ≤ 0.05), produced thinner epidermal layers that more closely mimicked those of normal skin, and displayed better structural organization of the dermis and epidermis as evidenced by histopathologic examination of the scar tissue at autopsy. 10
Mori et al. (2016, LOE II) used L. angustifolia essential oil with specified concentrations of linalool (43.0%) and linalyl acetate (32.1%) to evaluate the efficacy of lavender essential oil in wound healing. The researchers produced circular full-thickness wounds in rats and applied either a control solution (containing the lipophilic substances dimethyl sulfoxide and Tween 20) or 1% L. angustifolia essential oil dissolved in the control solution to the wounds on alternating days for 14 days. The wound area of rats treated with lavender essential oil was significantly decreased compared with control rats at 4, 6, 8, and 10 days after wounding (at days 4, 6, 8: p < 0.01 vs. control; at day 10: p < 0.05 vs. control). No significant difference in wound size was seen at 12 and 14 days.
In the same study, protein levels of transforming growth factor (TGF)-β, a cytokine known to induce the proliferation of fibroblasts, significantly increased in lavender-treated groups compared with controls at both 4 and 7 days after wounding (at day 4: p < 0.05 vs. control; at day 7: p < 0.01 vs. control). In addition, at 4 days the lavender-treated group demonstrated increased expression of type I collagen (predominant in the scar tissue of a healed wound) and type III collagen (predominant in the granulation tissue of an actively healing wound). Levels reduced to control levels by day 7 for type III collagen, while expression of type I collagen remained elevated at day 7, suggesting that type III was more rapidly replaced with type I collagen in the lavender-treated group. 28
An animal trial designed by El Banna et al. (2018, LOE II) used excision wounds in rats to evaluate the efficacy of Grotto cream (a combination cream containing beeswax,
At several time points throughout the study, a significant reduction in wound area (p < 0.05) was seen in both normal and diabetic rats treated with either Grotto or Fucidin cream compared with their corresponding controls. In addition, the epithelialization period was shortened from 25 days in the control group to 17 and 19 days in the Grotto and Fucidin treatment groups, respectively (p < 0.05). The researchers concluded that Grotto cream was effective in promoting wound healing in both normal and diabetic rats, but they called for further investigation into the activities of the individual components of the cream. 29 As Grotto cream comprised six potentially active ingredients in addition to lavender essential oil, it is difficult to discern how much of the cream's effect can be attributed to lavender essential oil.
While lavender's essential oil is most thoroughly studied, the lavender flower also produces a honey. Lusby et al. (2006, LOE II) compared the wound healing effects of both the honey and essential oil of Lavandula x allardii with those of a standard therapeutic honey (Medihoney). Researchers created surgical wounds on rats and, after applying treatment twice a day for 4 days, analyzed the wounds for contraction and capillary volume. After a 12-day period, they found that none of the three topical treatments produced a statistically significant difference in wound contraction relative to the untreated control. However, there was a significant reduction (p < 0.001) in capillary volume at the wound site on day 12 in the groups treated with either of the two honeys. 30
In vitro trials
A study by Han et al. (2017, LOE IV) evaluated the biologic effects of essential oils on human dermal fibroblast cells undergoing simulated chronic inflammation. Inflammation was achieved by the addition of inflammatory molecular stimuli, including interleukin-1β, tumor necrosis factor-α, and interferon-γ. One of the essential oils tested was a commercial blend of lavender, frankincense, Hawaiian sandalwood, myrrh, Helichrysum, and rose essential oils. Each of the oils tested by the researchers, including the commercial blend, was found to have a significantly antiproliferative effect on fibroblast cells (p < 0.01). In addition, the commercial blend containing lavender was one of the few oils that inhibited collagen III (a major component of granulation tissue), plasminogen activator inhibitor (PAI)-1 (a protein that causes decreased degradation of extracellular matrix), and tissue remodeling-related proteins. 31
To elucidate the concentration at which lavender essential oil can safely be used as a topical application, Prashar et al. (2004, LOE IV) assessed its cytotoxicity to endothelial cells and fibroblasts in vitro. The researchers determined that at a concentration of 0.25%, L. angustifolia essential oil becomes cytotoxic to these human skin cells. The researchers propose that its major components, linalyl acetate (51%) and linalool (35%), cause membrane damage at and above this concentration, and the majority of cytotoxic activity is attributed to linalyl acetate. 32
Discussion
Wounds are a common medical problem that burdens the patients and practitioners who care for them. As wounds can result from any trauma to the skin, such as surgical procedures, childbirth, pressure injuries, and diabetic ulcers, they are pervasive in medical practice. However, despite the ubiquity of wounds, there are few accepted treatments known to enhance the wound healing process.
Current recommendations for basic wound care include initiation of antibiotic therapy for wounds with clinical infection, debridement of wounds with devitalized tissue or contaminants, and application of dressings that maintain a moist environment. 33 Pressure injuries require repositioning and offloading of pressure, and extremities with wounds caused by venous or lymphatic stasis require elevation and application of compressive dressings. In addition, topical therapies, such as growth factor preparations and antimicrobial agents, can be selectively utilized to stimulate healing and reduce the bacterial load of wounds. 33 Physicians and patients have been searching for potential alternative therapies that may improve wound healing. As lavender essential oil has been hypothesized to hasten wound contraction and to have antimicrobial activity, it has potential for use as a topical therapy that serves both these purposes. 10,22,28,34,35
The majority of studies identified in this review support the use of lavender essential oil in wound healing and suggest several unique mechanisms through which the oil may exert its effects on healing wounds. In one study, lavender essential oil was found to significantly increase levels of TGF-β and type I collagen. 28 As TGF-β is reported to induce the proliferation of fibroblasts and their subsequent differentiation into myofibroblasts, which play an essential role in wound contraction via tissue shrinkage, this finding corroborates the clinical finding of increased and faster wound contraction in the lavender-treated group compared with the control group.
Another study reported significant elevations of FGF-2 and EGF in wounds treated with lavender essential oil. 27 As its name suggests, a major role of FGF-2 is to induce the proliferation of fibroblasts. EGF is a signaling molecule responsible for wound contraction and epithelialization via stimulation of fibroblast and epithelial cell migration, and it is currently being investigated as a novel topical therapy for chronic wounds. 36
Further evidencing its role in wound maturation, lavender essential oil, as part of a blend, was found to inhibit PAI-1. 31 The inhibition of PAI-1 is known to lead to a more rapid degradation of fibrin, which accounts for lavender essential oil's demonstrated ability to avoid the excess formation of connective tissue in wound healing. It is believed that these effects on the tissue remodeling-related proteins may be due, in large part, to linalyl acetate and linalool, the major components of lavender essential oil. 37 It is important to note, however, a conflicting mechanism reported in this in vitro study that utilized a blend of essential oils containing lavender. The blend was found to have antiproliferative effects on fibroblasts, in direct contrast with the previously discussed in vivo observations of lavender essential oil in isolation inducing the proliferation and differentiation of fibroblasts. 31 This difference might be explained by other oils in the blend exerting predominating antiproliferative effects. The biologic activities of lavender essential oil reported in these studies provide several potential mechanisms of action to account for the faster rate of wound contraction and enhanced healing process seen in several studies included in this review.
Care for delivery-related perineal trauma typically focuses on control of pain and edema. This is classically achieved with topical cooling treatments, such as crushed ice or frozen menstrual pads, and oral analgesics. 38 As application of lavender essential oil to perineal wounds resulted in significantly reduced pain and improved REEDA scores in several studies, it could be considered for use alongside these common methods of wound care, either applied topically to the perineal area or added to a sitz bath.
A limitation of this review is found in the risk of bias of one of the included studies, Chemical composition analysis and in vitro biological activities of ten essential oils in human skin cells, by Han et al. The researchers report they are employees at dōTERRA, where the studied essential oils were manufactured. In addition, many studies utilized lavender essential oil compounded with other ingredients.
The chemical compositions of lavender essential oils vary widely, as ecologic conditions such as latitude, altitude, temperature, and rainfall affect the relative amounts of the chemicals in the oil depending on where and when the plant was grown and harvested. 39,40 The concentration of linalool, typically the predominant chemical component of the oil, has been found to vary substantially based on changes in these environmental factors.
For example, researchers identified one population of lavender grown in North Greece with linalool concentrations changing from 48.71% to 35.1% over the span of a few weeks due to fluctuations in temperature and time since the most recent rainfall. 40 Although two bottles of commercially available lavender essential oil may claim to be 100% lavender essential oil isolated from L. angustifolia populations grown in the same region, a difference in ecologic conditions between the two populations of plants may drastically affect the relative amounts of the active chemicals found in the bottle. Furthermore, Cavanagh and Wilkinson propose that the inconsistencies found in the literature on lavender essential oil may be due to the widespread lack of reporting the specific oil type used and the concentrations of its biologically active components. 17 While lavender essential oils on the market are frequently labeled as 100% pure, this claim is not validated by an overseeing body and the actual composition of the product is not regulated. Therefore, until the chemical composition of each bottle of lavender essential oil is verified, it will be impossible to provide a standard dilution of drops of essential oil in carrier that is safe for topical application by consumers.
Many commercial lavender essential oil distributors also label their products as “therapeutic grade,” although this distinction is equally meaningless. According to the U.S. Food and Drug Administration (FDA), essential oils are currently considered to be cosmetics and will not be established and regulated as drugs until they are proven to meet the requirements for safety and efficacy. As only drugs can legally be labeled for therapeutic use under the Federal Food, Drug, and Cosmetic Act, any essential oil claiming to be “therapeutic grade” is in violation of this act. Illustrating this point, the FDA has sent Warning Letters to multiple companies who were found to advertise their essential oil products “for use in the diagnosis, cure, mitigation, treatment, or prevention of disease.” 41,42
Lavender essential oil must be appropriately diluted before topical application due to its potential cytotoxicity. It is important to note that while Prashar et al. determined lavender essential oil causes membrane damage to human skin cells in vitro at and above concentrations of 0.25%, this value only applies to oils containing the same specific concentrations of the components linalyl acetate (51%) and linalool (35%) used by the researchers. 32 In this oil, the concentration of linalyl acetate (found to be the more cytotoxic component) was higher than that of linalool, which is not typical for lavender essential oils. Furthermore, the results of this in vitro study may not be generalizable to in vivo application of lavender essential oil, as many of the human clinical trials included in this review used lavender essential oil at higher concentrations without reported damage to the skin.
However, in light of the demonstrated cytotoxic effects of lavender essential oil on human skin cells, one should not presume in vivo benefits from activities seen at exclusively high concentrations in vitro. For example, although a safe upper limit is yet to be established, the antimicrobial activity seen at lavender essential oil concentrations greater than 50% would likely not be present in a safe topical preparation, as suggested by one in vitro study. 19
An additional limitation of this review is found in the search methodology. The authors chose to limit searches to three popular databases (PubMed, Cochrane Library, and Embase) and used few, specific search terms to avoid returning thousands of potentially irrelevant articles through a more extensive search utilizing all available databases. The methodology as described may have been improved with the use of more extensive search terms entered into a greater number of databases. However, the quantity and quality of articles uncovered through these searches yielded a high percentage of relevant material.
Although prior reviews related to this topic exist, they were conducted before many significant studies had been performed, and none focuses on lavender essential oil and wound healing specifically or covers it extensively. The aim of this review is to consolidate and describe what is known about lavender essential oil's potential therapeutic effect on wounds to guide future research and aid physicians in clinical discussions and decision-making. The authors felt this aim would be best accomplished by including study designs beyond human clinical trials, as clinical studies are currently limited in number and do not provide insight into potential mechanisms of action. In addition, studies were not excluded based on wound type (e.g., surgical skin excision, episiotomy, or mucosal) as the diversity of included investigations provides valuable information about the potential utility of lavender essential oil in healing wounds of many types.
Conclusions
The current body of literature suggests a potential therapeutic benefit of topical application of lavender essential oil in wound healing through mechanisms such as faster wound contraction, enhanced activity of the proteins involved in the tissue remodeling process, and increased expression of collagen. In addition, lavender essential oil was found to reduce pain and REEDA scores when used on episiotomy wounds.
Satisfactory work has been done to elucidate the mechanisms through which lavender essential oil exerts its therapeutic effects at the cellular level. However, further clinical studies are warranted to evaluate the safety and efficacy of lavender essential oil therapy before its acceptance into practice as an evidence-based therapy. In addition, significant work is needed to standardize the chemical concentration of commercially available lavender essential oils, importantly the components linalyl acetate and linalool, so that a standard dilution ratio that is consistently safe and effective can be provided to consumers. Physicians should make themselves familiar with this current body of evidence to best understand all treatment options for the large number of patients suffering from wounds and to counsel patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.