
Abstract
Introduction:
Herbal medicine (HM) is widely used in East Asia to treat idiopathic central precocious puberty (ICPP). However, no systematic reviews of the efficacy and safety of HM for treatment of ICPP have been reported. Thus, this systematic review assessed the efficacy and safety of HM for ICPP. Most available clinical trials that investigated HM for ICPP were included in this review.
Methods and analysis:
Eleven databases, including Asian databases, were searched from the date of inception until June 2018. We included randomized controlled trials (RCTs) that assessed HM for ICPP.
Results:
Nine RCTs including 650 participants with ICPP, were included in this review. As a result of meta-analysis, response rate of HM group was 1.14 times higher compared with control group, with moderate level of evidence. Also, serum estradiol (E2) level was significantly lower in HM group compared to control group with moderate level of evidence. Notably, serum luteinizing hormone (LH) level (IU/L) and E2 level were significantly lower in HM group than triptorelin injection group with moderate level of evidence. Bone age index and uterine volume were also significantly lower in HM group than control group with very low level of evidence. The incidence of adverse events was lower in the HM group than control group, but it was not statistically significant.
Conclusions:
According to the results of the meta-analysis, it seems that HM treatment has a significant effect on the treatment of ICPP and can effectively reduce serum LH, E2 level, and bone age. In particular, as gonadotropin-releasing hormone analog therapy has a negative effect on the growth rate and final height if bone age ≥13 years, this study suggests that HM treatment may be helpful. Additional higher quality RCTs are needed to demonstrate the efficacy and safety of HM for treatment of ICPP.
Introduction
Central precocious puberty (CPP, also known as gonadotropin-releasing hormone [GnRH]-dependent precocious puberty) is defined as premature activation of the hypothalamic-pituitary-gonadal axis and appearance of secondary sex characteristics before the age of 8 years in girls and 9 years in boys. 1 CPP without an identifiable cause is known as idiopathic central precocious puberty (ICPP). The prevalence of CPP is much higher in girls, comprising 90% of all reported cases of ICPP 2 ; the prevalence of CPP among Korean girls has increased markedly, from 3.3 per 100,000 girls in 2004 to 50.4 per 100,000 girls in 2010. 3 Early secretion of estradiol (E2) accelerates growth and bone age, resulting in shortening of the growth period and reduction of adult height. CPP can cause psychological problems and early menarche in girls, 4 and can increase the risk of metabolic and cardiovascular diseases in both boys and girls. 5,6
Currently, the most common treatment for CPP is GnRH analog therapy; such analogs inhibit the progression of puberty by blocking secretion of gonadotropin and the production of sex steroids. 7 However, there have been reports of side effects. If the bone age is ≥13 years, GnRH analog therapy may negatively impact growth velocity and final height, and may lead to weight gain and reduced bone mineral density during treatment. 8 Furthermore, adverse effects of GnRH analog therapy may include hypertriglyceridemia and increased low-density lipoprotein level, 9 hyperprolactinemia, 10 vaginal bleeding, 11 and skin reactions at the injection site. 12 In addition, many children with ICPP complain of fear and pain of injection treatment. 13
Recent studies have suggested that GnRH analog therapy may not result in these side effects and is safe for long-term use, 7,14,15 but considerable controversy remains regarding its safety and further research is needed. 9 In Korea, GnRH analog injection treatment, which is a typical treatment for ICPP, is not covered by health insurance in most cases, thus incurs a cost burden. 16 Furthermore, according to one study conducted in Korea, it was found that 43.4% of children treated with GnRH analog therapy for ICPP also used growth hormone to compensate for the decrease in the growth rate due to GnRH analog therapy, causing increase in treatment cost, which is about 3,000,000 to 30,000,000 won per year. 17 Because of concerns regarding safety and cost burden, the demand for complementary and alternative medicine approaches to treat ICPP has increased in East Asia. 18,19
Herbal medicine (HM) is widely used for the treatment of ICPP in Asian countries, 16,17 specifically to delay pubertal development and promote growth in affected patients. 20 In Traditional Chinese Medicine (TCM), ICPP is considered to be caused by the broken balance of yin and yang, and is treated by classifying it in to three main TCM patterns: hyperactivity of fire due to yin deficiency, liver-qi stagnation transforming into fire, and phlegm stagnation due to spleen deficiency. 21 In previous studies, HM suppressed the hypothalamic-pituitary-gonadal axis and inhibited the synthesis and release of GnRH in an animal model, 22 and has been reported to delay sexual development in animal studies. 23,24 In addition, several studies have reported that HM regulates the function of the hypothalamic-pituitary-ovarian axis and delays skeletal development and maturation in idiopathic precocious puberty patients. 25,26
Although several studies have been performed regarding the effects of HM for treatment of ICPP, there have been no systematic reviews of this therapeutic approach. Thus, this study aimed to assess the efficacy and safety of HM for the treatment of ICPP.
Methods
Study registration
The protocol for this systematic review has been registered in PROSPERO 2018 (No. CRD42018087988).
Data sources
The following databases were searched from their dates of inception until June 2018: MEDLINE, Embase, the Cochrane Central Register of Controlled Trials (CENTRAL), AMED, and CINAHL. We also searched six Korean medical databases (OASIS, the Korean Traditional Knowledge Portal, the Korean Studies Information Service System, KoreaMed, the Korean Medical Database, and DBPIA) and three Chinese databases: CNKI (containing data from the China Academic Journal, the China Doctoral Dissertations and Masters' Theses Full-text Database, the China Proceedings of Conference Full-Text Database, and the Century Journal Project), Wanfang, and VIP. In addition, we conducted nonelectronic searches of conference proceedings, our own article files, and nine traditional Korean medicine journals. Study selection was documented and summarized in a PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis)-compliant flow chart (Fig. 1). Additional search was conducted in March 2020, but no studies matching the criteria were found.

Flowchart depicting the results of the literature search.
Types of studies
Prospective randomized controlled trials (RCTs) and quasi-RCTs that evaluated the efficacy of HM for ICPP were included in this review. Both treatment with HM alone and concurrent treatment with HM and another therapy were considered acceptable if HM was administered solely to the intervention group and any other treatment was administered equally to both groups. Trials with any type of control intervention were included. There were no restrictions regarding publication language. Hard copies of all articles were obtained and read in full.
Types of participants
This study included patients who were diagnosed with ICPP. We excluded patients with CPP secondary to congenital hypothyroidism, germ cell tumors, various types of gonadal tumors, or organic diseases (e.g., congenital adrenal hyperplasia, adrenal tumors, various intracranial tumors, or central nervous system diseases). Due to the outcome determinations, only RCTs involving girls were included.
Types of interventions
Interventions involving any formulation (i.e., decoction, tablets, capsules, pills, powders, and extracts) of HM were included. This study included only previous studies using HM prescribed by traditional East Asian medicine doctors, and the compositions of all interventions were reviewed.
Data extraction and quality assessment
Hard copies of all articles were obtained and read in full. Two authors (J.A.L. and Y.B.L.) extracted the data and assessed the quality using a predefined data extraction form. The risk of bias was evaluated using the Cochrane risk of bias assessment tool, version 5.1.0, which considers random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, completeness of outcome data, selective reporting, and other sources of bias. 27 The results of such evaluations were presented by utilizing scores of “L,” “U,” and “H” to indicate a low risk of bias, an uncertain risk of bias, and a high risk of bias, respectively. Disagreements were resolved by discussion among all authors. When disagreements regarding selection could not be resolved through discussion, an arbiter (L.H.L.) made the final decision.
Data collection and synthesis
Outcome measures
Primary outcomes
Response rate
Hormone levels (follicle-stimulating hormone [FSH], luteinizing hormone [LH], and E2).
Secondary outcomes
Ovarian volume and uterine volume
Adverse events
Bone age
Data synthesis
Differences between the intervention and control groups were assessed. The mean difference (MD) and 95% confidence interval (CI) were used to measure the effects of treatment for continuous data. We converted other forms of data into the MD. For outcome variables with different scales, we used the standard MD and 95% CI. For dichotomous data, we presented treatment effects as the relative risk (RR) and 95% CI; other binary data were converted into the RR.
All statistical analyses were conducted using the Cochrane Collaboration's software program Review Manager (RevMan) version 5.3 for Windows (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark). When missing information was encountered in a study, we contacted the corresponding author for clarification whenever possible. As appropriate, we pooled data across studies to conduct a meta-analysis using fixed- or random-effects models. We used GRADEpro software (McMaster University/Evidence Prime, Inc., Hamilton, Canada) to create a summary of findings table.
Results
Study search results
A total of 268 studies were selected through electronic search; all were screened, and there were no duplicates. The literature search identified 48 potentially relevant studies, 9 of which were included (Fig. 1). The main characteristics of the nine included studies are summarized in Table 1. 28 –36 All included RCTs were performed in China and were published between 2001 and 2016.
Characteristics of Studies Included in the Meta-Analysis
BA, bone age; BAI, bone age index (ΔBA/ΔCA); BGP, osteocalcin; BMI, body mass index; CA, chronological age; CI, confidence interval; E2, estradiol; FSH, follicle-stimulating hormone; HM, herbal medicine; LH, luteinizing hormone; ICPP, idiopathic central precocious puberty; IPP, idiopathic precocious puberty; LHRH, luteinizing hormone releasing hormone; RR, risk ratio; TCM, Traditional Chinese Medicine; WM, Western medicine.
Risk of bias
Only two trials reported the use of a random sequence generation method. 29,33 Both trials used a randomized digital table method and were considered to exhibit a “low risk” of selection bias. The randomization procedure was not clearly stated in the other seven trials. No trials described allocation concealment or blinding of outcome assessment. In all trials, blinding of participants and personnel was incomplete. Because the control group did not receive placebo treatment, participants and researchers were able to identify the assigned intervention. There were no dropouts in any of the studies; thus, the risk of bias for incomplete outcome data was considered to be “low risk.” The risk of bias for selective reporting was “unclear” because none of the trials had published protocols. Three trials did not state whether baseline characteristics were comparable, so those studies were considered to have an “unclear” risk of other sources of bias (Supplementary Figure S1).
Effects of interventions
Images of meta-analysis results not shown in the text are shown in Supplementary Figure S2.
HM versus Megestrol
Two studies tested four different HM interventions compared with megestrol. 28,29 Both studies compared HM plus megestrol with megestrol alone.
Response rate
One study compared response rate between HM plus megestrol and megestrol alone, and reported response rate of HM plus megestrol was significantly higher (p < 0.05). 29 This study evaluated clinical efficacy in four stages; cured, significantly improved, improved, and ineffective. It was considered effective if breasts reduced to stage B1 or reduced after treatment, clinical symptoms disappeared or decreased, and laboratory indicators returned to normal or improved. Total response rate is defined as the proportion of participants who were cured, significantly improved, or improved after treatment.
Hormone levels (FSH, LH, and E2)
In one study, serum LH, FSH, and E2 level of HM plus megestrol and megestrol alone were compared, and all were significantly lower in HM plus megestrol group (p < 0.05). 29 In other study, only serum LH level (IU/L) after LH releasing hormone stimulating test was compared, but there was no significant difference between two groups (p > 0.05). 28
Uterine and ovarian volume
Both studies compared uterine and ovarian volume between HM plus megestrol and megestrol alone, 28,29 and one study compared according to Tanner stage. 28 Both studies showed no significant differences between two groups (p > 0.05). 19,20
Bone age index
Both studies compared bone age index (ΔBA/ΔCA) between HM plus megestrol and megestrol alone 28,29 ; meta-analysis revealed that bone age index (ΔBA/ΔCA) was significantly lower in HM plus megestrol group (n = 148, MD: −0.68, 95% CI: −0.86 to −0.51, p < 0.00001, I 2 = 73%). Bone age index is defined as bone age divided by chronological age.
Other
In one study, predicted final height of HM plus megestrol group was significantly higher than control group (p < 0.05). 28
HM versus triptorelin (GnRH analog) injection
Five studies tested four different HM interventions compared with triptorelin. 30 –34 Two studies compared HM plus triptorelin injection with triptorelin injection alone 32,33 ; another two studies compared HM alone with triptorelin injection alone. 31,34 One study compared HM plus acupoint sticking with triptorelin injection alone. 30
Response rate
Five studies compared response rate between HM group and triptorelin injection group 30 –34 ; meta-analysis revealed that the response rate of HM group was higher than triptorelin injection-treated group, but this finding was not statistically significant (n = 356, RR: 1.11, 95% CI: 0.99–1.24, p = 0.08, I 2 = 0%). Four studies evaluated clinical efficacy in three stages: cured or significantly improved, improved, and ineffective. 30,32 –34 And one study evaluated clinical efficacy in four stages: cured, significantly improved, improved, and ineffective. 31 Evaluation criteria varied among studies, but were generally considered to be effective when breast reduces, clinical symptoms disappeared or decreased, and laboratory indicators returned to normal or improved. Total response rate is defined as the proportion of participants who were cured, significantly improved, or improved after treatment.
Hormone levels (LH, FSH, and E2)
All of five studies compared serum LH level between HM group and triptorelin injection group 30 –34 ; meta-analysis revealed that the serum LH level (IU/L) of HM group was significantly lower than triptorelin injection group (n = 356, MD: −0.74, 95% CI: −1.22 to −0.27, p = 0.002, I 2 = 88%, Fig. 2).
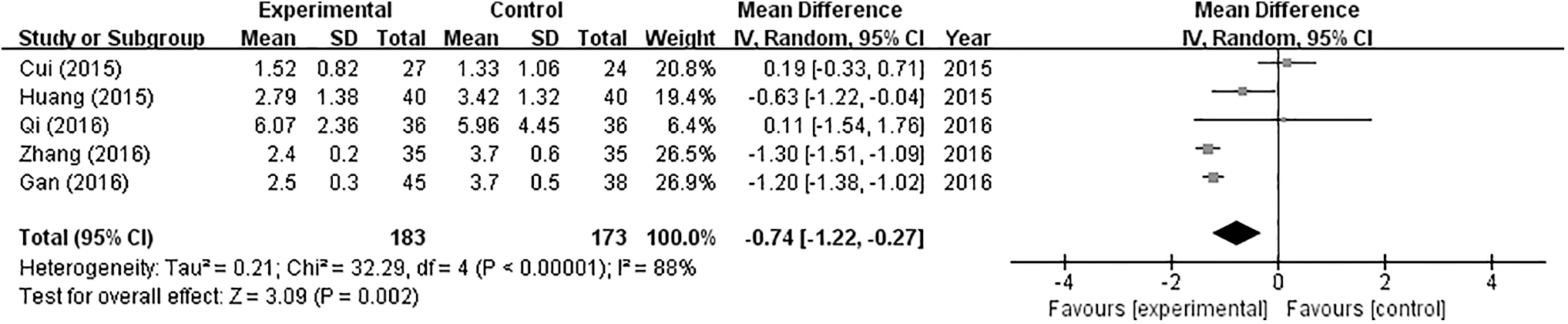
Forest plot comparing LH level (IU/L) between HM group and triptorelin-treated group. HM, herbal medicine; LH, luteinizing hormone.
Five studies compared serum E2 level (pg/mL) between HM group and triptorelin injection group 30 –34 ; meta-analysis showed that serum E2 level was also significantly lower in HM group (n = 356, MD: −4.21, 95% CI: −5.00 to −3.43, p < 0.00001, I 2 = 0%, Fig. 3).

Forest plot comparing E2 level (pg/mL) between HM group and triptorelin-treated group. E2, estradiol; HM, herbal medicine.
Five studies reported serum FSH level (IU/L) 30 –34 ; meta-analysis revealed that serum FSH level of HM group was lower than triptorelin injection group, but this finding was not statistically significant (n = 356, MD: −0.57, 95% CI: −1.26 to 0.12, p = 0.11, I 2 = 93%).
Uterine and ovarian volume
Five studies compared uterine volume (mL) between HM group and triptorelin injection group 30 –34 ; meta-analysis revealed that the uterine volume (mL) of HM group was lower than triptorelin injection group, but not statistically significant (n = 356, MD: −0.42, 95% CI: −0.92 to 0.08, p = 0.10, I 2 = 81%).
Five studies compared ovarian volume (mL) of HM group and triptorelin injection group 30 –34 ; meta-analysis showed that ovarian volume (mL) of HM group was higher than triptorelin injection group, but this finding was not statistically significant (n = 356, MD: 0.02, 95% CI: −0.25 to 0.29, p = 0.87, I 2 = 87%).
Bone age index
Four studies compared bone age index (ΔBA/ΔCA) between HM group and triptorelin injection group 31 –34 ; meta-analysis revealed that the bone age index (ΔBA/ΔCA) of HM group was lower than triptorelin injection group, but this finding was not statistically significant (n = 305, MD: −0.09, 95% CI: −0.25 to 0.08, p = 0.30, I 2 = 78%). Bone age index is defined as bone age divided by chronological age.
Other
In one study, body max index (BMI) was compared between HM and triptorelin injection, and BMI (kg/m3) of HM group was significantly lower than triptorelin injection group (p = 0.001). 31 Another study compared growth rate between HM plus triptorelin injection and triptorelin alone, and it was significantly lower in HM plus triptorelin injection group (p < 0.00001). 32 One study compared treatment cost between HM plus triptorelin injection and triptorelin injection alone, and it was significantly lower in HM plus triptorelin injection group (p < 0.00001). 33
HM versus leuprolide (GnRH analog) injection
Only one study compared HM with leuprolide injection. 35 This study compared serum E2 level (pg/mL), osteocalcin level (pmol/L), and bone age index (ΔBA/ΔCA) between HM and leuprolide injection, and there were no significant differences between two groups (p > 0.05).
HM versus no treatment
Two studies compared tested two different HM interventions compared with no treatment. 28,36 One study compared HM plus megestrol with no treatment, 28 and the other study compared HM alone with no treatment. 36
Response rate
Both studies did not report response rate.
Hormone levels (FSH, LH, and E2)
In one study, serum LH, FSH, and E2 level of HM alone and no treatment were compared, and all were significantly lower in HM group (p < 0.05). 36
Uterine and ovarian volume
Both studies compared uterine and ovarian volume between HM group and no treatment group, 28,36 and one study compared according to Tanner stage. 28 Both studies showed significantly smaller uterine and ovarian volume in HM group (p < 0.05). 28,36
Bone age index
Both studies compared bone age index (ΔBA/ΔCA) between HM alone and no treatment 28,36 ; meta-analysis revealed that bone age index (ΔBA/ΔCA) was significantly lower in HM group (n = 151, MD: −0.93, 95% CI: −1.02 to −0.85, p < 0.00001, I 2 = 0%, Fig. 4). Bone age index is defined as bone age divided by chronological age.

Forest plot comparing bone age index (ΔBA/ΔCA) between HM group and No treatment group. HM, herbal medicine.
Other
In one study, predicted final height of HM plus megestrol group was significantly higher than control group (p < 0.05). 28
HM versus control group
Overall, nine studies tested nine different HM interventions compared with control group. 28 –36
Response rate
Six studies reported response rate 29 –34 ; meta-analysis of these six studies showed that the response rate was significantly higher in the HM group (n = 418, RR: 1.14, 95% CI: 1.03–1.26, p = 0.01, I 2 = 2%, Fig. 5).
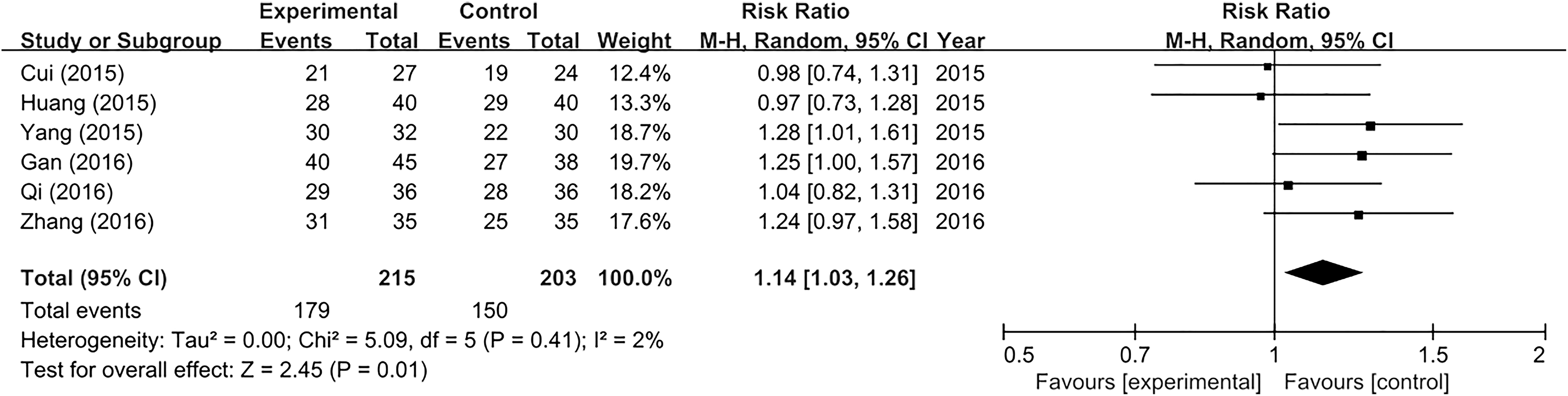
Forest plot comparing response rate between HM group and control group. HM, herbal medicine.
Hormone levels (LH, FSH, and E2)
Seven studies reported serum LH level (IU/L). 29 –34,36 ; meta-analysis showed that the LH level (IU/L) was lower in the HM group, but this result was not statistically significant (n = 498, MD: −2.09, 95% CI: −5.30 to 1.13, p = 0.20, I 2 = 100%).
Seven studies compared serum FSH level (IU/L) between HM group and control group 29 –34,36 ; meta-analysis showed that the serum FSH level was lower in the HM group, but this finding was not statistically significant (n = 498, MD: −1.39, 95% CI: −3.21 to 0.42, p = 0.13, I 2 = 99%).
Seven studies compared serum E2 level (pg/mL) between HM group and control group 29 –35 ; meta-analysis showed that the serum E2 level was significantly lower in the HM group (n = 464, MD: −4.22, 95% CI: −5.00 to −3.45, p < 0.00001, I 2 = 0%).
Uterine and ovarian volume
Seven studies reported uterine volume (mL) after treatment 29 –34,36 ; meta-analysis showed that the uterine volume was significantly smaller in the HM group (n = 498, MD: −0.70, 95% CI: −1.37 to −0.04, p = 0.04, I 2 = 92%).
Seven studies compared ovarian volume (mL) after treatment 29 –34,36 between HM group and control group; meta-analysis showed that the ovarian volume (mL) was smaller in HM group, but this finding was not statistically significant (n = 498, MD: −0.26, 95% CI: −0.74 to 0.22, p = 0.29, I 2 = 97%).
Bone age index (ΔBA/ΔCA)
Eight studies reported bone age index (ΔBA/ΔCA) 28,29,31 –36 ; meta-analysis showed that the bone age index (ΔBA/ΔCA) was significantly lower in the HM group (n = 579, MD: −0.35, 95% CI: −0.60 to −0.09, p = 0.007, I 2 = 98%). Bone age index is defined as bone age divided by chronological age.
Adverse events
Six studies reported adverse events. 29,31 –34,36 In one study comparing HM plus megestrol with megestrol alone, two cases of mild diarrhea and three cases of pain at the injection site were reported in the group receiving HM with oral megestrol acetate tablets; four cases of pain at the injection site were reported in the group taking oral megestrol acetate tablets alone. 29 The difference between groups was not statistically significant (n = 62, RR: 1.17, 95% CI: 0.35–3.96, p = 0.80, one trial). Among five studies that reported adverse events comparing HM group with triptorelin injection, four of these revealed that there were no side effects in both groups 31,32,34,36 ; and in one study, five cases of mild vaginal bleeding were reported in the group treated with triptorelin (GnRH analog) injection. 33 The difference between groups was not statistically significant (n = 72, RR: 0.09, 95% CI: 0.01–1.59, p = 0.10, one trial).
Details of HM approaches and formulations
Details regarding the HM approaches and formulations in the included studies are presented in Table 2. Only two studies reported TCM patterns. 29,35 In one study, participants were divided into three TCM patterns—hyperactivity of fire due to yin deficiency, liver-qi stagnation transforming into fire, and phlegm stagnation due to spleen deficiency—and were administered different HM interventions. 29 In another study, only people with liver depression and phlegm stagnation were recruited. 35 Regarding the preparation form, four studies used decoction, 28 –30,33 two studies used granules, 31,35 and three studies used pills. 32,34,36 In seven studies, a detailed composition of the HM was provided 28 –31,33,35 ; all seven studies reported different compositions. The Dabuyin pill was used in all three studies involving pill usage. 32,34,36 There were six studies describing the dose of HM, 28,31,33 –36 and one study applied different doses according to age. 35 In five studies, participants took HM twice a day, 28,30,31,33,35 in one study, participants took HM two to three times a day, 34 and in one study, participants took HM three times a day. 36 Duration of taking HM was provided in all nine studies, and it varied from 4 months to 3.5 years. 28 –36
Details of Herbal Medicine in the Included Studies
HM, herbal medicine; TCM, Traditional Chinese Medicine.
Level of evidence
The level of evidence for each outcome is presented in Tables 3 –6. When comparing HM group with megestrol, the evidence level for bone age index was “very low.” When comparing HM group with triptorelin injection, the evidence level for serum LH level (IU/L) and E2 level (pg/mL) was “moderate,” and evidence level for uterine volume, ovarian volume, and bone age index was “very low.” When comparing HM group with no treatment, there was a “moderate” level of evidence for bone age index. Overall, there were “moderate” level of evidences for response rate and serum E2 level in HM group compared to control group, and “very low” level of evidences for serum LH level, serum FSH level, uterine volume, ovarian volume, and bone age index in HM group compared to control group. The low level of evidence was largely due to a high risk of bias (especially due to incomplete blinding of participants and personnel), high heterogeneity, and overlap in the 95% CIs, leading to a lack of significant effects.
Summary of Findings: Herbal Medicine Group Compared to Megestrol for Idiopathic Central Precocious Puberty
GRADE Working Group grades of evidence:
High certainty: we are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: we are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.
Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect.
Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect.
The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
In all trials, blinding of participants and personnel was incomplete.
Heterogeneity is very high (I 2 = 73%).
BAI, bone age index; CI, confidence interval; GRADE, Grading of Recommendations Assessment, Development and Evaluation; HM, herbal medicine; ICPP, idiopathic central precocious puberty; MD, mean difference; RCT, randomized controlled trial.
Summary of Findings: Herbal Medicine Group Compared to Triptorelin Injection for Idiopathic Central Precocious Puberty
GRADE Working Group grades of evidence:
High certainty: we are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.
Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect.
Very low certainty: we have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect.
The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
In all trials, blinding of participants and personnel was incomplete.
Heterogeneity is very high (I 2 = 88%).
Heterogeneity is very high (I 2 = 93%).
p > 0.05.
Heterogeneity is very high (I 2 = 81%).
Heterogeneity is very high (I 2 = 87%).
Heterogeneity is very high (I 2 = 78%).
BAI, bone age index; CI, confidence interval; E2, estradiol; FSH, follicle-stimulating hormone; GRADE, Grading of Recommendations Assessment, Development and Evaluation; HM, herbal medicine; LH, luteinizing hormone; ICPP, idiopathic central precocious puberty; MD, mean difference; RCT, randomized controlled trial; RR, relative risk.
Summary of Findings: Herbal Medicine Group Compared to No Treatment for Idiopathic Central Precocious Puberty
GRADE Working Group grades of evidence:
High certainty: we are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.
Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect.
Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect.
The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
In all trials, blinding of participants and personnel was incomplete.
BAI, bone age index; CI, confidence interval; GRADE, Grading of Recommendations Assessment, Development and Evaluation; HM, herbal medicine; ICPP, idiopathic central precocious puberty; MD, mean difference; RCT, randomized controlled trial.
Summary of Findings: Herbal Medicine Group Compared to Control Group for Idiopathic Central Precocious Puberty
GRADE Working Group grades of evidence:
High certainty: we are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: we are moderately confident in the effect estimate: the true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.
Low certainty: our confidence in the effect estimate is limited: the true effect may be substantially different from the estimate of the effect.
Very low certainty: we have very little confidence in the effect estimate: the true effect is likely to be substantially different from the estimate of effect.
The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
In all trials, blinding of participants and personnel was incomplete.
Heterogeneity is very high (I 2 = 100%).
p > 0.05.
Heterogeneity is very high (I 2 = 99%).
Heterogeneity is very high (I 2 = 92%).
Heterogeneity is very high (I 2 = 97%).
Heterogeneity is very high (I 2 = 98%).
BAI, bone age index; CI, confidence interval; E2, estradiol; FSH, follicle-stimulating hormone; GRADE, Grading of Recommendations Assessment, Development and Evaluation; HM, herbal medicine; LH, luteinizing hormone; ICPP, idiopathic central precocious puberty; MD, mean difference; RCT, randomized controlled trial; RR, risk ratio.
Discussion
Summary of evidence
The results of this systematic review and meta-analysis showed that, for treatment of ICPP, HM is more effective than control group. Response rate of HM group was 1.14 times higher compared with control group with moderate level of evidence. Also, serum E2 level was significantly lower in HM group compared to control group with moderate level of evidence. Bone age index and uterine volume were also significantly lower in HM group than control group with very low level of evidence. According to the above results, it is considered that HM treatment is effective for ICPP. In particular, serum LH level (IU/L) and E2 level were significantly lower in HM group than triptorelin injection group with moderate level of evidence. Triptorelin is a GnRH analog, which is widely used as a treatment for ICPP. Since GnRH analog may have a negative effect on the final height if bone age is over 13 years, 8 combination with HM or HM alone might be effective for treating ICPP without affecting final height.
The incidence of adverse events was lower in the HM group than control group, but it was not statistically significant. Five cases of mild vaginal bleeding were reported in the group treated with triptorelin injection. 33 Two cases of mild diarrhea and three cases of pain at the injection site were reported in the group treated with HM combined with oral megestrol acetate tablets; four cases of pain at the injection site were reported in the group treated with oral megestrol acetate tablets alone. 29 Side effects of GnRH analog therapy, currently used as a standard treatment for ICPP, may include hypertriglyceridemia and increased low-density lipoprotein level, 9 hyperprolactinemia, 10 vaginal bleeding, 11 and skin reactions at the injection site. 12 In one study included in this review, vaginal bleeding was observed in triptorelin injection group, while no adverse events occurred in HM plus triptorelin injection group. 33 Therefore, it is thought that combination use of HM with GnRH analog may reduce side effects. Overall, since only mild adverse events were reported in HM group, and no adverse events were reported in the group treated with HM alone, it is considered relatively safe to use HM compared to triptorelin injection and megestrol acetate tablets, but there is a limit to judging the clinical significance.
The major TCM patterns of ICPP are known as hyperactivity of fire due to yin deficiency, liver-qi stagnation transforming into fire, and phlegm stagnation due to spleen deficiency. 22 In this systematic review, only two studies reported TCM patterns. 29,35 In one study, patients were divided into hyperactivity of fire due to yin deficiency, liver-qi stagnation transforming into fire, and phlegm stagnation due to spleen deficiency 29 ; in the other study, only patients with liver depression and phlegm stagnation types were recruited. 35
Research on the treatment cost was conducted in only one study, and it was reported that treatment cost of HM plus triptorelin injection group was significantly lower than triptorelin injection alone group (p < 0.00001). 33 Since many patients are feeling the burden of the cost treating ICPP, research on the treatment cost will be helpful for the further use of HM for treating ICPP.
Limitations
There are several limitations to this review. The first limitation of this review is that the studies included in the meta-analysis exhibited high heterogeneity. High heterogeneity among these studies was likely caused by various clinical factors (population, study duration, and herbal ingredients), as well as research design and the interventions used in treatment or control groups.
The second limitation of this review is that the included studies were of low quality. When assessing the risk of bias, all studies were considered to be “high risk” in more than one aspect; in particular, performance bias was considered to be “high risk” in all studies. Because there were no control groups using placebo, both participants and researchers were aware of the assigned interventions and blinding could not be performed.
The third limitation of this review is that the evaluation criteria are not standardized for assessing treatment outcomes of ICPP. Regarding the response rate, it was difficult to determine morbidity because the criteria were subjective and differed among studies; thus, the response rate reliability was poor.
The fourth limitation of this review is that all of the included studies were conducted in China; thus, the results cannot be readily generalized.
Conclusions
According to the results of the meta-analysis, it seems that HM treatment has a significant effect for treating ICPP and can effectively reduce serum LH, E2 level, and bone age. In particular, since serum LH, E2 level, and bone age index were significantly lower in HM group than triptorelin injection group, it seems that HM can supplement the limitations of the GnRH analog treatment, which is widely used for ICPP. In conclusion, HM treatment for treating ICPP is effective and safe. However, because of the limitations described above, more large-scale high-quality studies are needed to clarify the safety and efficacy of HM for treatment of ICPP. In addition, more accurate analysis, achieved through application of standardized and objective outcome variables, is needed. Because treatment of ICPP is performed in children and side effects have been reported when HM are used, further studies of these side effects are needed.
Footnotes
Authors' Contributions
Y.B.L. and L.H.L. conceived the study, developed the criteria, searched the literature, performed the data analysis, and wrote the protocol. Y.B.L. and J.A.L. conducted the preliminary search. J.A.L. and L.H.L. assisted in searching the Chinese literature and extracting the data. All authors have read and approved the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by the Daejeon University Research Grants (2019).
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.