
Abstract
Objectives:
Mindfulness-based interventions (MBIs) have been shown to reduce engagement in disordered eating behaviors, although how these interventions engender change remains unclear. The objective of this exploratory qualitative study was to describe the experiences and perceived attitudinal and behavioral changes of women participating in a mindful eating program.
Design:
Focus group discussions were held with women participating in a community-based mindful eating program for binge and emotional eating. A semistructured interview guide was used to explore participants' conceptualizations of mindfulness-based attitudinal and behavior change, as related to food, eating, and body image. The focus group discussions were audio-recorded, transcribed, and analyzed using thematic analysis to identify salient concepts.
Settings/Location:
Focus group discussions were held at the Center for Mindfulness at the University of Massachusetts Medical School (UMMS) (United States).
Participants:
A sample of nine women who were enrolled in the mindful eating program at UMMS for problems with self-reported binge and/or emotional eating participated in this study.
Results:
Four themes were constructed that described a process of mindfulness-based behavior change, including (1) Learning Through Self-Awareness, (2) Self-Empowerment, (3) Mindful Choice-Making, and (4) Resilient Self-Care. An overarching description of the participants' perceived attitudinal and behavior changes was developed: “unforced freedom of choice, emerging from embodied awareness.”
Conclusions:
These findings suggest that MBIs reduce may disordered eating behaviors through empowering women to make positive choices about food, eating, and coping, without focusing on weight control. Future research is needed to examine whether these findings replicate in larger and more diverse samples, and how they can be used to optimize and implement eating-specific MBIs in community-based settings.
Introduction
Disordered eating describes a range of problematic eating attitudes and behaviors that primarily affect women. 1,2 These issues are prevalent (32% of women report body dissatisfaction, 27% restrictive dieting, and 7% binge eating), 3 –6 and associated with health issues such as reproductive and metabolic dysfunction, depression, and anxiety. 6 –9 Relatedly, emotional eating has been defined as eating in response to emotional states rather than homeostatic hunger cues. 10 Although recent research challenges the concept of emotional eating, suggesting that high scores on emotional eating scales represent general eating-related concern and/or a tendency to attribute subjective overeating to negative emotions, 11 –14 women who self-report emotional eating often report associated psychological distress (likely related to the social stigma of emotional eating). 15,16
Despite the burden of disordered eating, there are limited community-based interventions to serve as a public health approach to treatment and prevention. 17 Interventions for binge and emotional eating are especially needed, given their prevalence and physical, psychological, and social consequences. 6,8,9,18,19 Furthermore, although etiologic models of these behaviors routinely include psychosocial factors (e.g., interpersonal/social stress), 20 –22 the dominant treatment paradigm narrowly focuses on reducing overeating through increasing self-control, with weight loss the ultimate goal. 23,24 This “weight-centric” approach has received critique for failing to achieve long-term weight loss, while simultaneously perpetuating weight stigma and further disordered eating, 25 –29 supporting interest in other approaches. 22,30
One such approach is mindfulness-based interventions (MBIs). 31 Mindfulness, a quality of consciousness defined as “the awareness that emerges through paying attention on purpose, in the present moment, and nonjudgmentally,” 32 has been adopted from Buddhist spiritual traditions into Western psychology to address a variety of behavioral and emotional health issues. 33 MBIs for eating-related issues range from general mindful eating programs to the standardized Mindfulness-Based Eating Awareness Training (MB-EAT), all of which focus on cultivating mindfulness around food and eating through systematic training (e.g., mindfulness meditation exercises). 34,35 The motivation for using MBIs to address disordered eating includes their hypothesized effects on emotion regulation, cognitive flexibility, reactivity to food cues, and body appreciation. 36 –39 In addition, recent research suggests that mindfulness and mindful eating may help promote embodiment, 40 defined as “the lived experience of engagement of the body with the world,” 41,42 which is increasingly recognized as a protective factor against disordered eating. 42,43 Indeed, MBIs are associated with improvements across a range of disordered eating behaviors, 44 –46 and may be readily implemented into community-based settings. 47
However, research on mindful eating among otherwise healthy women experiencing binge and/or emotional eating is limited. Extant research is largely quantitative investigations of mindful eating correlates with little insight into the underlying mechanisms of MBIs, precluding efforts to improve the impact of these interventions for large-scale implementation. 48 Conversely, qualitative methods can help identify the pertinent attitudinal and behavioral changes of complex interventions by directly exploring the lived experience of program participants. 49 Furthermore, centering participants' voices in the early stages of intervention development can help ensure interventions address issues important to participants and avoid perpetuating harm (e.g., weight stigma). Few studies have used qualitative methods in research on eating-specific MBIs, 50,51 and none to our knowledge has focused on women's perceptions of the mechanistic changes involved.
This study
To address these gaps, this exploratory qualitative study aimed to elucidate the attitudinal and behavioral changes of women participating in a community-based mindful eating program at the University of Massachusetts Medical School (UMMS) Center for Mindfulness. We were interested in describing participants' (1) conceptualization of mindful eating; (2) perceived attitudinal and behavioral changes; and (3) understandings of how these changes occurred.
Materials and Methods
Study design and procedures
We conducted focus group discussions with participants from the UMMS Center for Mindfulness mindful eating program. Program facilitators announced the opportunity for participation to program participants; those who were interested provided their name and e-mail address and were contacted by study personnel. Because of the small number of eligible participants (∼20 individuals were enrolled in the mindful eating program at the time of the study), information on general demographics of program participants was collected in place of individually identifying information to preserve anonymity. Nine women from the program participated in this study. Two 90-min focus group discussions (n = 5 and n = 4) were held at the Center for Mindfulness, facilitated by a graduate student experienced in qualitative interviewing. Participants provided informed consent before participation. The discussions were conducted using a semistructured interview guide developed by the study personnel, with input from program facilitators. Questions were based on salient program concepts (Table 1), and were asked in an open-ended format using additional probe questions as necessary. As the study posed minimal risk, did not collect personally identifying information, and was classified as nongeneralizable, educational setting research (discussions occurred within the context of the program and covered similar topics), the UMMS Institutional Review Board deemed it exempt from federal regulations.
Focus Group Discussion Questions and Associated Prompts
UMMS mindful eating program
The UMMS Center for Mindfulness in Worcester, MA, offers a community-based, rolling-admissions mindful eating program for individuals experiencing binge and emotional eating. The program focuses on mindfulness training, delivered through a weekly in-person class with support from the Eat Right Now ® app (Table 2). 52,53 The weekly in-person class is a “flipped-classroom” style discussion group led by a trained facilitator, in which participants share experiences and problem solve struggles. It is based on a three-stage model (termed the “Three Gears”) intended to guide participants from disordered to normalized eating. 53 –55 Briefly, “First Gear” focuses on increasing awareness of one's eating-related behaviors (including perceived triggers) without judgment or attempt at change. In “Second Gear,” the focus is on observing the outcomes (i.e., emotions and physical sensations) of one's behaviors, again without judgment or attempts at change. Finally, in “Third Gear,” the focus is on learning to exist with triggers rather than (always) acting upon them, with the goal of developing additional coping strategies for one's specific stressors.
Outline of the Eat Right Now App Video Modules
Data analysis
Focus group discussions were audio-recorded, transcribed, and analyzed using thematic analysis, a qualitative method used to identify and interpret patterns (i.e., “themes”) within the data. 56 We focused on participants' experiences with Third Gear, the stage at which we hypothesized change to occur. After familiarizing ourselves with the data through repeated readings of the transcripts, the first analytic cycle involved initial coding, when data were broken down into groups of words, sentences, and paragraphs representing major concepts. In the second cycle, we reassembled the initial codes hierarchically into codes and higher-order themes. These first two cycles were carried out independently by two researchers using Dedoose software version 7.0.23, 57 with differences discussed through discussion with a third investigator until reaching consensus. In the next cycle, all investigators worked to identify the “core category,” or the principle phenomena all other themes related to and how well the themes supported the data. Finally, diagramming techniques were used to name and define each theme and to visualize the relationships between them. 58
Results
The majority (>75%) of mindful eating program participants were middle-aged women (aged 40–70 years) who self-reported binge and/or emotional eating for at least 1 year. All participants lived in central Massachusetts, were middle to upper middle class and were employed or retired, and were predominantly (>75%) non-Hispanic White. The 9 women who participated in this study (who had been in the program for an average of 6 months [range: 3–12], participating in both the weekly in-person class and usage of the app) reflected these demographics. None of the women had a current eating disorder diagnosis.
Analysis of the focus group data generated 10 codes clustered under four themes that described participants' experiences with Third Gear: “Learning Through Self-Awareness,” “Self-Empowerment,” “Mindful Choice Making,” and “Resilient Self-Care” (Table 3).
Themes and Associated Codes from Qualitative Analysis
Theme 1: Learning through self-awareness
Under this theme, participants' comments highlighted the centrality of self-awareness in addressing disordered eating, characterized by an increased ability to observe one's thoughts, feelings, and behaviors around food and eating. Many participants described having an “awakening,” becoming cognizant of behaviors previously perceived to be “automatic.” For example, one woman explained that she used to “just wake up in the middle of eating.” However, she eventually became more observant of her behaviors, explaining “I'm seeing better when I open the cabinet … Sometimes I make a food choice, sometimes I don't, but it's the awareness that's different.” Overtime, this self-awareness cultivated a curiosity about the situational contexts in which their disordered eating thoughts and behaviors occurred, enabling women to ask questions such as, “What might have happened today that led to me feeling this urge to [binge] right now?”
Importantly, this self-awareness originated from and was enhanced by body awareness. Because much of the training in the program focuses on attending to sensory experiences, the women learned to discern bodily sensations (e.g., hunger and satiety, and how emotions “feel”). While all of the women described how this learning was a nonlinear process (reflecting challenges inherent to initiating and maintain a mindfulness practice), this ultimately enabled them to pay better attention to the act of eating, including the physical and emotional aspects, facilitating a deeper awareness and understanding.
Theme 2: Self-empowerment
The self-awareness cultivated during the early stages of the program enabled the women to explore the “function” of their disordered eating. For many, these behaviors were coping mechanisms, and they identified stressful or traumatic life events as triggers. As one woman stated, “I don't think we questioned our binges … Now I can go back and say, well, I just got devastating news!” Understanding the role that disordered eating played in their lives decreased feelings of shame or guilt (e.g., “There's less judgment … I'm just human, and this is what I'm feeling”), and this was often contrasted with previous attempts to “control” their eating, such as through dieting. For example, one woman explained, “That's the main thing about this program versus others … where it was either you lost weight or you didn't, meaning you're a good person or a bad person.”
Letting go of shame and guilt opened space for self-compassion and a desire to address the root causes of their emotional distress, rather than continuing to ignore or repress them. Compared to previous attempts at self-control through dieting, however, this self-compassion-based approach instilled in the women a sense of relative ease and eagerness (e.g., “This is very empowering for me because now that I know what's going on, I can make changes”), Many of the women explained how self-empowerment through self-discovery was a turning point for them, and thus was frequently cited as the beginning of the transition into Third Gear.
Theme 3: Mindful choice making
Almost all participants discussed how Third Gear was characterized by an increased perceived capacity to make positive choices about food and eating (e.g., “You can have awareness in any gear. But making the choice, that's what makes it Third Gear”). In general, the women described these choices in terms of adopting adaptive methods of coping with adverse experiences or emotions (e.g., calling a friend and going for a walk). For instance, one woman defined Third Gear as “[enabling] you to hold the pain without medicating the pain.” Other participants discussed how they could choose to “sit with” distressing emotions, rather than “numb themselves with food.”
The importance of body awareness was frequently emphasized when discussing choice making. One woman explained, “You can be stuck in your head, and you may see things clearly, but you're not feeling them, and feeling them in your body makes such a huge difference.” By tuning in to their bodies, the women were able to make choices that felt intuitive rather than forced. These mindfulness-based “embodied choices” were often described as reinforcing feelings of empowerment, as well as cultivating a sense of freedom around food and body concerns.
Theme 4: Resilient self-care
Finally, participants described how their increased capacity for choice making fostered meaningful, individualized behavior change centered around self-care and a deep respect for their physical, emotional, and social needs. One woman stated, “It just sort of clicks, it flips a switch in your brain and you think, oh … what do I need?” Another woman defined Third Gear as “consciously choosing to take care of yourself.” This translated into what many women called an “uncoupling” of previous triggers (e.g., a bad day at work and a fight with a significant other) from using food and eating as a coping mechanism.
This uncoupling was typically rooted in self-compassion, which allowed the women to re-frame “set-backs” as expected patterns and cycles of eating. Many participants rejected the idea of “perfect eating,” embracing flexibility instead. One woman stated, “It's like, wow, I'm capable of making awesome choices, and also knowing that sometimes, I'm not going to, and that's ok.” Another woman explained, “It's a process, in that you have those Third Gear moments, it's awesome, it's like ‘I can really do this’ … I also don't say that I'm cured, or something like that.” Such flexibility was perceived as a personal strength by many participants as it conferred resiliency. They discussed how they often encountered triggers or other psychosocial stressors in their social environment that made engaging in mindful eating more difficult, as well as challenges such as time constraints or family obligations. However, rather than embrace an “all-or-nothing” attitude, most participants were compassionate with themselves when they made what they previously would have called a “bad food choice” (i.e., a binge episode), recognizing that such a choice did not represent a moral failing and, in the case of eating in response to stress or other negative emotions, often was the best coping response they had in the moment. As one woman explained, “There's a tremendous amount of potential in Third Gear.”
Relationships between themes
These four themes are interrelated and describe the temporal process by which participants experienced mindfulness-based behavior change, which we present visually in Figure 1. The first phase involved the initiation of a mindfulness practice and the development of self-awareness. Specifically, the ability to observe one's thoughts and actions fostered an understanding of habitual behaviors surrounding food and eating and the external contexts that engendered them. As this self-awareness extended to include an understanding of the function served by one's disordered eating, previously entrenched shame and guilt were replaced by nonjudgmental acceptance and self-determination. This sense of empowerment represented the major turning point in the process, as it led to an increased perceived capacity for engaging in embodied self-care practices, the defining attitudinal and behavior change experienced by the women. From these theme interrelationships, we developed an overarching definition of participants' perceived changes in Third Gear: “unforced freedom of choice, emerging from embodied awareness.”
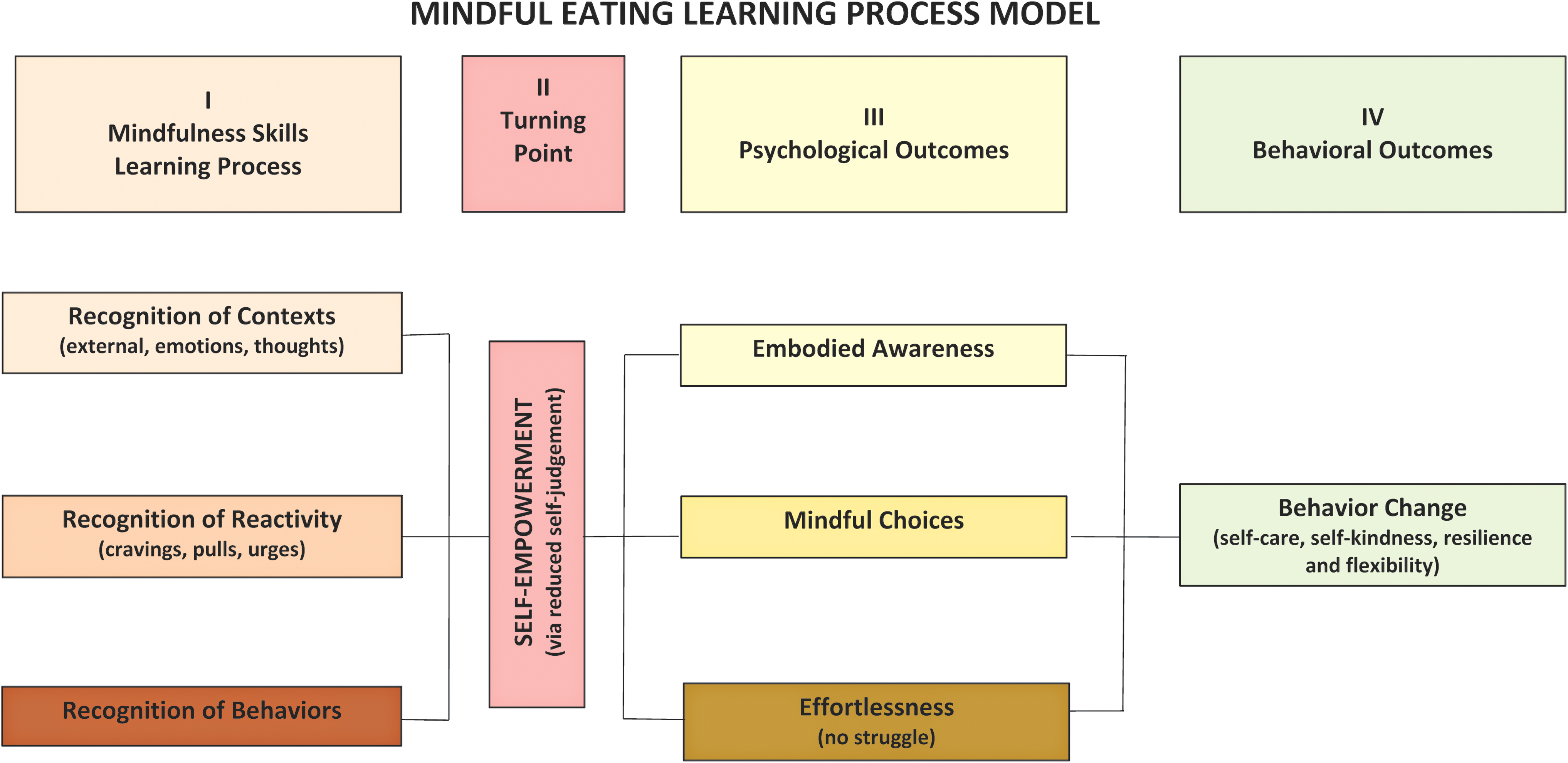
Conceptual model of mindfulness-based behavior change for disordered eating. The model presents a four-phase temporal process resulting in an “unforced freedom of choice, emerging from embodied awareness.” Color images are available online.
Discussion
MBIs are increasingly popular approaches for addressing disordered eating, although their underlying mechanisms remain unclear, precluding the refinement of these interventions for larger-scale implementation. This exploratory study aimed to help fill this gap by describing women's experiences with a community-based mindful eating program. From the qualitative analysis, four interrelated themes describing a four-phase process of mindfulness-based change were constructed, shedding light on how mindfulness training can alter the relationships that women have to food, eating, and their bodies.
The development of embodiment was central to the participants' experiences of change. Specifically, the women described a transition from what has been defined as “negative embodiment” (disrupted connection to one's body) to “positive embodiment” (adaptive connection to one's body). 59 Previous research has implicated factors related to negative embodiment such as low self-esteem and negative effect in the etiology of binge eating 60 ; this is consistent with findings that disturbances to embodiment are associated with eating-related issues more broadly. 42,61 –64 Piran's Development Theory of Embodiment posits that “embodied individuals” experience their bodies as valued aspects of their self-concept and well-being, and thus are likely to attend to their bodies' needs. 42,65 Mindfulness training may have facilitated this shift for the women in this study through practices designed to cultivate body awareness in a self-compassionate manner, suggesting that the development of positive embodiment is a key dimension of mindful eating's therapeutic effects. Notably, quantitative research on MBIs has identified increased embodiment as a plausible mechanism by which mindfulness training improves psychological health, 66,67 including eating-related outcomes. 68,69
The women described how this positive embodiment cultivated an increased perceived capacity for intuitive choice making; these choices, centered around self-care, represented an enhanced expression of agency regarding food and eating. Feminist theorists have long linked restricted agency with women's eating-related issues, articulating how these issues stem from social constructions of women's bodies and appetites. 65,70,71 Mindfulness training has been shown to increase self-confidence and perceived control over one's life, 72 –74 and as an embodied contemplative practice, may allow women to reflect upon and ultimately reject these constructions. This intellectual transformation could have contributed to the women's shift from negative to positive embodiment, consistent with how the women reframed their notions regarding the relationships between eating, weight, and self-worth (thereby promoting adaptive coping and self-care behaviors). As an important aside, MBIs are generally individual-level interventions that do not explicitly address the wider social contexts in which disparate health outcomes develop. 75 While individual-level therapeutic work is often necessary in addressing eating-related issues, future research should explore how mindfulness training can fit into multilevel community-based interventions that consider structural barriers women face pertaining to food- and body image-related concerns.
Overall, our findings are consistent with and build upon hypothesized models of mindfulness-based behavior change. First, our findings reflect a model of mindfulness-based behavior change focused on decoupling, or the modification of the relationship between internal and external experiences (e.g., thoughts/feelings vs. behavior). 36 Decoupling has been suggested to be a mechanism of action for mindful eating interventions, such that mindfulness training interrupts the relationship between disordered eating thoughts (e.g., self-worth as tied to eating patterns and body size) and subsequent disordered eating behaviors. 37,48,53 Our findings are also consistent with the Attuned Representational Model of Self, which posits that mindfulness-based positive embodiment fosters the ability to attend to one's physical and emotional needs through “health-promoting self-care behaviors.” 38 Notably, the aspects of mindful eating perceived as central to change by the women in this study relate entirely to developing adaptive methods of coping, rather than weight loss/management. This situates mindful eating within a “weight-neutral” (i.e., nonweight focused) approach to health, 76,77 and suggests that emphasizing weight control within eating-specific MBIs may mitigate intervention effects. Rather, these programs may be most impactful by focusing on factors deemed most helpful: positive embodiment, self-compassion, and self-empowerment.
Limitations and future directions
These findings should be considered in light of limitations. Given the exploratory nature of our study, our sample was small and relatively homogenous with respect to demographic factors; furthermore, participants who were overly satisfied with the program may have been more likely to participate. Therefore, the findings must be interpreted with caution and the understanding that they reflect the experiences that one group had with a specific mindful eating program. Future research should build upon this work by exploring the experiences had with mindful eating among larger, more diverse samples and with different MBIs. Future work should also consider mixed methods to investigate whether experience is empirically related to change in the hypothesized mediators (e.g., embodiment), and objective measures of disordered eating.
Conclusions
Disordered eating behaviors are prevalent among adult women and are associated with significant health risks and reduced quality of life. 1,2,10,15,16 This qualitative study of women's experiences with a mindful eating program elucidated a step-wise process of attitudinal and behavior change resulting in an increased capacity for intuitive choice making centered around self-care. Understanding these mechanisms is critical to the development and implementation of community-based MBIs for disordered eating, a critically underaddressed women's health issue.
Footnotes
Acknowledgments
The named authors thank Carol Bova PhD, RN, ANP, for her guidance in qualitative research methodology, Patti Holland MS, CRC, for her assistance in organizing the focus groups, and the focus group participants for their time, energy, and insight.
Author Disclosure Statement
J.A.B. owns stock in MindSciences, the company that produces the Eat Right Now® mobile app. All other authors declare that they have no conflicts of interest. Several members of the team have personal mindfulness practices, although the coding team included a balance of those with and without such a practice.
Funding Information
No funding was received for this article.