
Abstract
Background:
Centella asiatica, a medicinal plant, has been used traditionally to promote wound healing. Its efficacy on promoting postlaser resurfacing wound healing is lacking.
Methods:
Thirty individuals with facial acne scars underwent a treatment with 2940 nm Er:YAG laser. Half side of the face was randomized to receive 0.05% w/w ECa 233 gel, a standardized extract of C. asiatica, and the other half a placebo gel. The gels were applied four times daily for 7 days then twice daily for 3 months. Erythema, melanin, and texture index (TI) from Antera3D,® and skin biophysics were obtained at baseline, days 2, 4, and 7, then every 2 weeks for the first month, and every month for 3 months. Three blinded dermatologists assessed the photographs and provided a grading scale of wound appearances.
Results:
The ECa 233 treated side exhibited significantly less erythema index over total follow-up by 0.03 U (coefficient = −0.03 [95% CI −0.06 to −0.0006]; p = 0.046). In keeping with the physicians' assessment that showed significantly higher improvements in skin erythema at days 2, 4, and 7 (p = 0.009, 0.0061, 0.012), crusting at days 2 (p = 0.02), and general wound appearance at days 2, 4, and 7 (p = 0.008, 0.001, 0.044), TI showed a trend toward better outcome in the ECa 233 group. Skin biophysics did not differ between the two groups.
Conclusion:
ECa 233 might be an option for postlaser treatment to improve wound appearance.
Introduction
Treatments for facial scarring, that is, acne scar and photoaging, are increasingly popular. Among options available, laser skin resurfacing (LSR) is commonly used. Resurfacing lasers work by selective ablation of water-containing tissue and offer predictable and reproducible clinical outcomes. 1 Although the results are promising, post-treatment care remains challenging. These procedures come with complications, including prolonged erythema and edema, risk of infections, prolonged hyperpigmentation, and cicatrization. 2 Proper postprocedural care is necessary to optimize wound healing, reduce downtime and complications, and maximize beneficial outcomes of the laser treatment.
Centella asiatica (Linn.) Urban, also known as Bua-bok, Gotu Kola, Tiger Grass, or Indian Pennywort, is an herbaceous vine belonging to the Apiaceae (or Umbelliferae) family. 3 This medicinal plant is grown in tropical regions of Asia, Australia, Africa, and America. 4 It is used traditionally as an antimicrobial, antioxidative, and anticancer agent. 5,6 Importantly, it has been shown to enhance wound healing and was effective for tissue repair and regeneration in animal models. 7 –9 The beneficial effects of C. asiatica in promoting healing of small wounds, hypertrophic scars, and burns have also been described. 10
The authors were able to establish a standardized extract of C. asiatica, ECa 233, in which the fraction of triterpenoid glycosides is maintained. 11 Previous studies in animals have demonstrated the positive results of ECa 233 on second-degree burns with good tolerability. 12 However, a clinical study in humans to establish efficacy of postlaser resurfacing treatment is still lacking. In this present study, the authors aimed to evaluate the efficacy of topical 0.05% w/w ECa 233 gel for promoting postlaser wound healing and reducing complications after laser resurfacing on the face in participants with atrophic acne scars.
Materials and Methods
Ethical consideration
This current study is a prospective, randomized, split-face, double-blind, single-center clinical trial. The protocol was approved by the Institutional Review Board of Faculty of Medicine, Chulalongkorn University (IRB No. 586/61). The trial was conducted at King Chulalongkorn Memorial Hospital from December 2018 to March 2019 and was registered with Thai Clinical Trials Registry (TCTR20180927001). Written informed consent was obtained from each subject before the enrollment.
Inclusion and exclusion criteria
Adult subjects, aged 18 years or older, with bilateral atrophic facial acne scars for at least 6 months were eligible to participate in this study. Subjects were excluded if they were pregnant, lactating, smoking, had skin infections, inflamed acne, photosensitive dermatoses, or a propensity for keloid scarring, were receiving concomitant treatments on the involved skin areas or taking isotretinoin, or have received ablative/nonablative LSR procedures 3 months before the study period, and known allergy or sensitivity to lotions, moisturizers, or creams.
Preparation of topical formulation of ECa 233
ECa 233 as a raw material was provided by Siam Herbal Innovation Co., Ltd., Thailand. The extract contains madecassoside 51% and asiaticoside 38% as determined by LC-MS/MS analysis. Topical formulation of ECa 233 gel was developed by Pharma Neuva Co., Ltd., Thailand. The gel formulation had percent labelled amount in range of 90%–110%. All production procedures were complied with Good Manufacturing Practice. The concentration of the gel used in the study was 0.05% w/w based on the results of their previous study. 13 The placebo gel appeared identical to 0.05% w/w ECa 233 gel. Only the active ingredient, ECa 233, was removed.
Treatment protocol
The treatment area of the face was cleansed with mild cleanser. Then topical anesthetic cream (lidocaine and prilocaine-based cream, EMLA cream 5%, Karlskoga, Sweden) was applied under occlusion for 1 h before the laser procedure.
All participants were treated with erbium-doped yttrium aluminum garnet (Er:YAG) 2940 nm laser (SkinPlus Er:YAG device; Fotona Medical Lasers, Ljubljana, Slovenia) by the same dermatologist using a 7-mm spot sized handpiece at 1.8 J/cm2 for one session. The authors alternated short-pulsed and long-pulsed Er:YAG in a total of three passes, starting with short pulsed then long pulsed and the final step with short pulsed. Air cooling was provided during the procedure to minimize discomfort. No prophylactic antivirals or antibiotics were given to any subject.
Cooling with ice compression was done for 15–20 min after the laser treatment. During the first week, the participants were instructed to cleanse the treated area gently with tap water. Two different post-treatment care regimens were randomly assigned for each side of the face (block randomization, block size of 4) immediately after the laser. On one side, the patients were instructed to apply 0.05% w/w ECa 233 gel. On the other side, the placebo gel with identical appearance was applied. Both gels were used four times daily (morning, noon, evening, and bedtime). At nighttime, white petrolatum ointment was used after the gels on both sides. Subjects were instructed to use two different fingertips to apply the gels to avoid contamination. After the first week, the application frequency of the gels was reduced to twice daily (morning and bedtime). White petrolatum ointment was stopped, and broad-spectrum sunscreen (Anthelios XL dry touch, La Roche-Posay, France) was initiated every morning. The regimen was continued for 3 months. In addition, the participants were advised to avoid sun exposure, and the use of topical medications or products was prohibited throughout the study period.
Objective assessment
The participants were assessed at baseline, then on the second, fourth, seventh days after the laser treatment, then every 2 weeks for the first month, and every month for a total 3 months after the laser treatment. All objective measurements were performed in the same room with no daylight under controlled ambient conditions (room temperature 20°C and 40%–60% relative humidity). Each subject was required to clean the face and acclimatize to the environmental condition 30 min before the measurements. Erythema, melanin, and texture index (TI) were obtained by Antera 3D® (Miravex, Dublin, Ireland), and skin biophysics were taken with multiprobe system Cutometer® dual MPA580 (Courage+Khazaka, Köln, Germany). Similar skin positions were measured at every visit using photographic documentation.
Antera 3D® is a device containing camera for image acquisition and analysis of the skin. The acquired image was obtained by illuminating the skin with light-emitting diode of different wavelengths from different directions. Unlike traditional image techniques, which used only three-color channels (red, green, and blue), Antera 3D® uses reflectance mapping of seven different light wavelengths spanning the whole visible spectrum. This allows for more precise view and analysis of skin color by measuring the hemoglobin and melanin level. Moreover, texture of the skin can be evaluated. Therefore, skin color and texture can be assessed and represented as erythema, melanin, and TI. 14
Skin biophysics were evaluated by multiprobe system Cutometer® dual MPA580 (Corneometer® CM825; for skin moisture, Tewameter® TM300; for transepidermal water loss (TEWL), Skin-pH-Meter® PH905; for skin pH). The measurements were taken thrice from each side of the face, and average values of the triplicate readings were used.
Subjective evaluation
Photographic documentation using VISIA® Complexion Analysis System (Canfield Imaging Systems, Fairfield, NJ) was obtained at every visit. By the end of the study, three blinded dermatologists independently assessed the photographs to identify the clinical improvement of the wound compared with the baseline. The improvement of erythema, crusting/scabbing, epithelial confluence, and general wound appearance (overall appearance of the entire wound) was evaluated using a quartile grading system as follows: grade −4, 76%–100% worsening; grade −3, 51%–75% worsening; grade −2, 26%–50% worsening; grade −1, 1%–25%worsening; 0, no change; grade 1, 1%–25% improvement; grade 2, 26%–50% improvement; grade 3, 51%–75% improvement; and grade 4, 76%–100% improvement. Hyperpigmentation postlaser was also recorded according to its degree of intensity (0: no; 1 < 25%; 2: 25%–50%; 3: 51%–75%; 4: >75% darkening) and extension (0: no; 1 < 25%; 2: 25%–50%; 3: 51%–75%; 4: >75% of the treated area).
The participants were interviewed for subjective irritation parameters namely burning, itching, dryness, and pain using visual analog scales. In addition, adverse effects were recorded at each follow-up.
Statistical analysis
Participant demographics and skin characteristics were summarized by treatment group. Changes in erythema, melanin, and TI were summarized over follow-up, and formal comparisons in these parameters were compared over total follow-up in the ECa 233 treated versus the control side as a reference, using a generalized estimating equation to account for clustering and repeated measurements. Physician assessment scores were compared at different study weeks using a Wilcoxon rank sum test. Analyses were performed using Stata 15.1 (StataCorp, College Station, TX).
Results
Thirty patients, 25 females (83.3%) and 5 males (16.7%), with mild-to-moderate bilateral atrophic acne scar were enrolled and completed the study. The consort flow diagram showing the enrollment, allocation, follow-up, and analysis populations is shown in Figure 1. The mean age was 30.6 ± 5.6 years. The skin phototypes were III (n = 23, 76.7%) and IV (n = 7, 23.3%). The baseline demographic data and skin biophysical properties are shown in Table 1. Baseline skin biophysics were comparable between groups.

The consort flow diagram showing the enrollment, allocation, follow-up, and analysis.
Baseline Characteristics and Skin Biophysical Properties (n = 30)
Treatment, the standardized extract of Centella asiatica ECa 233; control, placebo.
SD, standard deviation; TEWL, transepidermal water loss.
In the ECa 233 treated side, mean (± standard deviation [SD]) Erythema Index (EI) reached the highest level on day 2 (1.3 ± 0.16) and was lower compared with the baseline on day 7 (1.14 ± 0.13) (Fig. 2a). While in the placebo side, the erythema also peaked on day 2 (1.38 ± 0.18) and was lower compared with the baseline on day 28 (1.12 ± 0.13). Importantly, the mean difference in EI on the ECa 233 treated side was significantly lower over the total follow-up period by 0.03 U (coefficient = −0.03 [95% CI −0.06 to −0.0006]; p = 0.046).
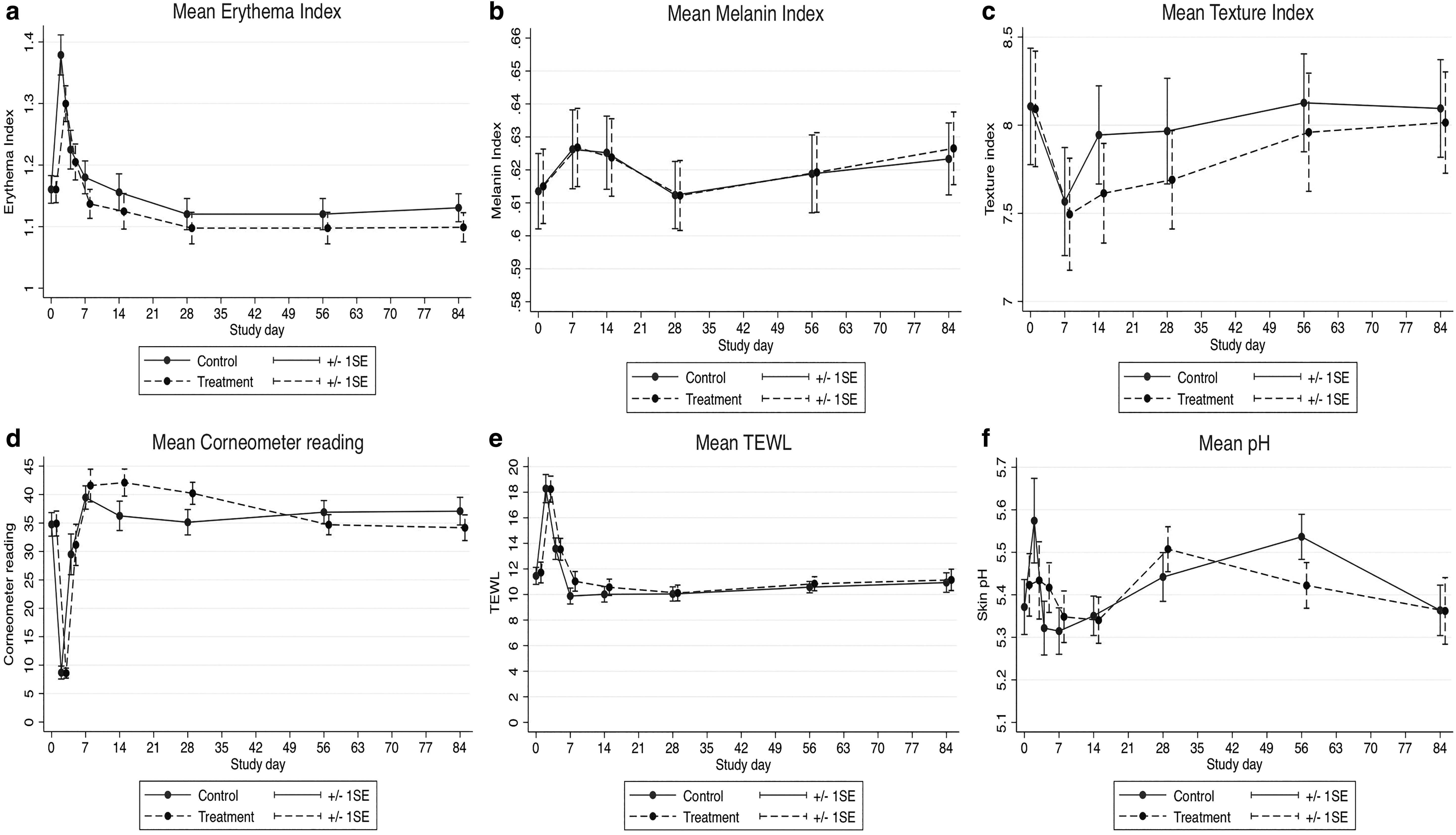
Objective measurement by Antera3D® and multiprobe system Cutometer® dual MPA580.
Melanin index (MI) at baseline and subsequent changes in both the ECa 233 treated and control sides largely paralleled each other (Fig. 2b), increasing from baseline on days 7 and 14, then falling to baseline levels by day 28, and then rising again at day 84. The changes were in a very narrow range, and the mean difference in MI over all follow-up in the ECa 233 treated side was not statistically different (coefficient = −0.0005 [95% CI −0.01 to 0.01]; p = 0.93).
Baseline mean (SD) TI was 8.09 ± 1.80 in the ECa 233 treated group and 8.11 ± 1.81 in the control group, and this decreased in both groups at day 7. Both groups gradually increased toward the baseline levels at day 84, but the treatment side had a maintained lower mean TI than the control arm over all follow-up, although the difference was just shy of statistical significance (coefficient = −0.16 [95% CI −0.34 to 0.03]; p = 0.09) (Fig. 2c).
The skin biophysics, including skin moisture, TEWL, and pH, did not differ between the groups over all follow-up. Skin biophysics of the treatment and control are shown in Figure 2d–f.
Physicians' assessment showed significantly higher improvements in the ECa 233 treated side. The skin erythema was better on days 2, 4, and 7 (p = 0.009, 0.0061, 0.012), crusting on day 2 (p = 0.02), and general wound appearance on days 2, 4, and 7 (p = 0.008, 0.001, 0.044). Physician assessment results are shown in Figure 3a–e. Postlaser hyperpigmentation returned to its baseline on day 7 in the ECa 233 treated side versus on day 14 in the placebo side. Interestingly both groups exhibited positive improvement in hyperpigmentation at the end of treatment (0.39 ± 0.49, 0.35 ± 0.48, respectively) (Fig. 3e). However, statistically significant improvements were not observed for postlaser hyperpigmentation and epithelial confluence. Subjective assessments of skin irritation demonstrated no significant differences in burning, itching, dryness, and pain between the two groups at any time points. Clinical photographs are shown in Figure 4.

Subjective measurement by three independent dermatologists in the improvement of
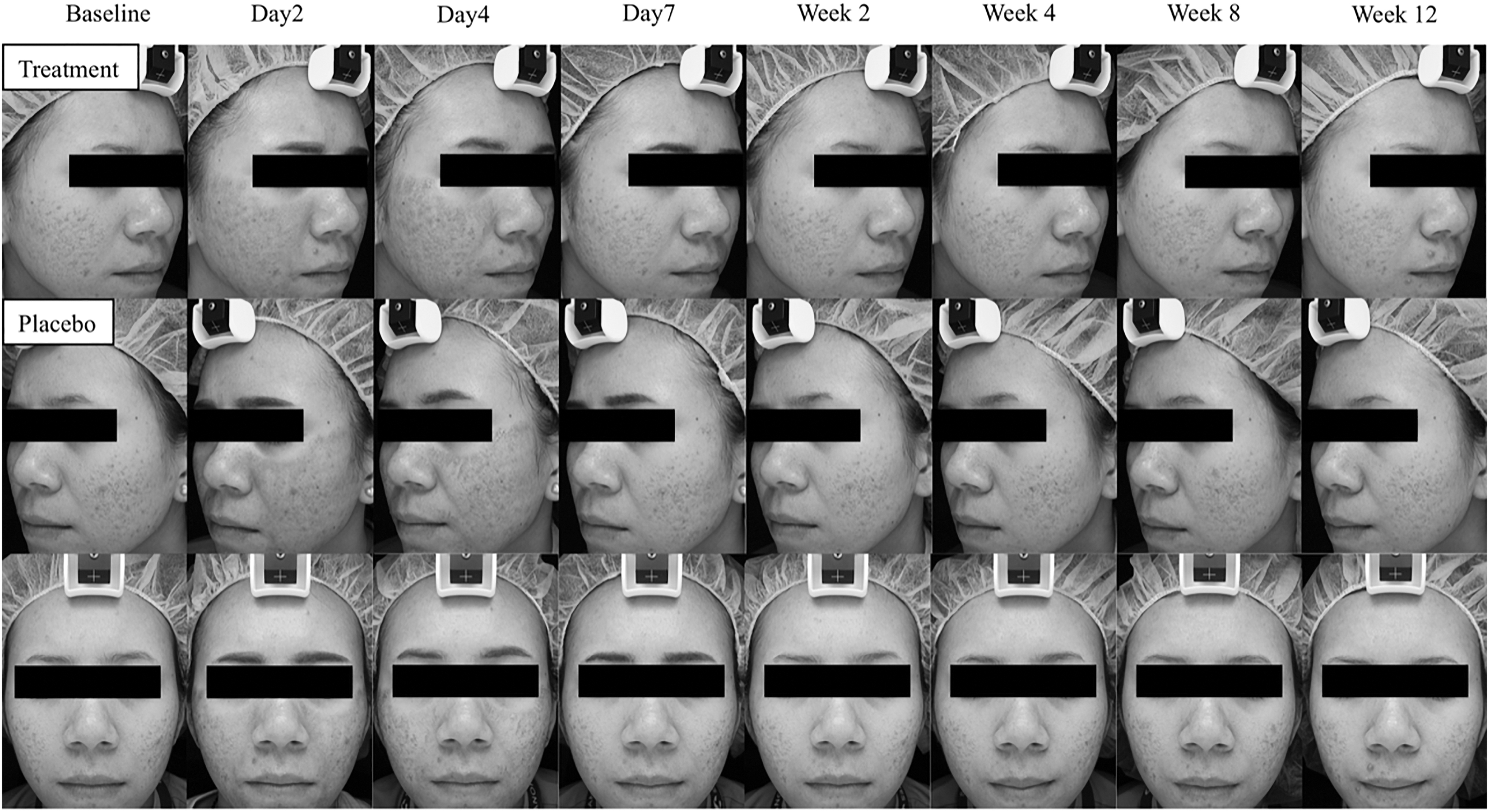
Photographic documentation using VISIA® postoperatively comparing the treated versus placebo sides.
Of 30 subjects treated, 2 (6.7%) developed dryness on the treated area on the second day postoperatively. The symptoms improved with the application of white petrolatum ointment on both sides for the first 7 days. No other adverse effects such as eczema, skin infections, hyper- or hypopigmentation, or scarring were observed.
Discussion
In this present study, the authors demonstrated that topical application of 0.05% w/w ECa 233 gel significantly reduced erythema post-LSR. This was confirmed by both objective and subjective assessments. Interestingly, erythema on the ECa 233 treated side subsided earlier compared with the placebo (day 7 vs. day 28). In addition, improvement in skin texture was observed in the treatment group. These results are in keeping with the physicians' assessments that showed significant improvements in erythema, crusting/scabbing, and general wound appearance in the treatment group within the first week after the LSR. These findings were consistent with the nature of wound healing that would be of greatest improvement within the first week.
C. asiatica has long been used in Dermatology to promote wound healing and as a treatment for leprosy and psoriasis. 15,16 The pharmacologic effects are thought to be exerted by its phyto-constituents. The most important ones are pentacyclic triterpenoid glycosides, known as centelloids, mainly: asiaticoside, madecassoside, asiatic acid, and madecassic acid. 10 Other constituents include flavonoids, fatty acids, tannins, essential oils, phytosterols, free amino acids, and alkaloids. 17 The standardized extract of C. asiatica, ECa 233, used in the study was established at the Faculty of Pharmaceutical Sciences, Chulalongkorn University. The extract was prepared to maintain the triterpenoid glycosides, and major active ingredients, at no less than 80%. The ratio between madecassoside and asiaticoside was maintained at 1.5 ± 0.5:1. 11,18
Asiaticoside and madecassoside have been reported to accelerate healing of superficial wounds and ulcers. This action is mediated by the activation of Malpighi cells of the epidermis, inhibition of the inflammatory process, and biostimulation of the formation of collagen. 19,20 The reepithelialization process involves differentiation, proliferation, and migration of epidermal keratinocytes. 21 Therefore, the increment of keratinocyte migration is mandatory to optimize wound healing process. 22 Intriguingly, ECa 233 has been reported to promote keratinocyte migration through activation of focal adhesion kinase, ATP-dependent tyrosine kinase and extracellular-signal-regulated kinase ½, and p38 mitogen-activated protein kinase signaling pathways. 23 At the dermal level, asiaticoside and madecassoside have been shown to enhance the synthesis of collagen type I, II, and III. 24 An in vitro study using cell proliferation assays demonstrated that asiaticoside increased the numbers of human dermal fibroblasts. 25 These mechanisms might explain the results from their study. ECa 233 may reduce erythema through its anti-inflammatory actions. Crusting/scabbing improvement may result from its positive effects on reepithelialization, and the overall texture improvement may be achieved by enhancing collagen production and optimizing wound healing.
LSR is an increasingly popular cosmetic procedure to reduce the signs of photoaging and improve facial scarring. The procedure induces skin damage in a targeted manner to stimulate the production of growth factors, collagen synthesis, and remodeling that ultimately results in skin restoration. 2 However, postprocedural complications may arise, especially in dark-skinned individuals. 26 To reduce complications from the procedures, post-treatment wound care is crucial. However, no standardized guideline is established, and there exists an unmet need for effective post-treatment regimens. One of the common complications of LSR is prolonged erythema. 2 The results from their study suggest that proper supplementary measures from a medicinal plant that is readily available in the region may reduce significant complications of LSR.
The limitations of the study included the fact that the participants were only Asians with skin phototype III–IV. Therefore, the results may not be generalizable to people with other skin phototypes. None of their participants experienced mid and late complications of LSR with the laser parameters used in the study. These complications are pigmentary changes (postinflammatory hypo- and hyperpigmentation) and cicatrization. Therefore, the effects of ECa 233 on these complications cannot be evaluated. Finally, the subjected evaluation on patient's acceptance was not obtained due to the design of the study (split-face). To their knowledge, this is the first clinical trial to evaluate the effects of ECa 233 after LSR. Moreover, the follow-up period (3 months) of the study is long enough to evaluate the wound healing process after the procedure.
Conclusion
Topical application of 0.05% w/w ECa 233 could improve skin erythema and wound appearance post Er:YAG 2940 nm laser resurfacing for acne scars. Therefore, this treatment regimen might be an option for postlaser resurfacing.
Footnotes
Acknowledgments
The authors heartfully thank the Skin and Allergy Research Unit, Chulalongkorn University for their supports.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was funded by the Department of Thai Traditional and Alternative Medicine, Ministry of Public Health, Thailand.