
Abstract
Objectives:
The purpose of this study was to investigate the immediate effects of self-Thai foot massages (STFMs) on the foot skin blood flow, the foot skin temperature, and range of motion (ROM) of the foot and ankle in type 2 diabetic patients with peripheral neuropathy.
Design:
A randomized crossover study.
Subjects:
Twenty five diabetic patients with peripheral neuropathy were recruited.
Interventions:
Participants were randomly assigned to either STFM or Thai foot massage (TFM) performed by a massage therapist; then, they were switched to the other group after a 1-week washout period. In both groups, the foot massage was performed in a seated position on the dominant lower leg and foot for 25 min.
Outcome measures:
Before and immediately after treatment, foot skin blood flow, foot skin temperature, and ROM of the foot and ankle were evaluated. Heart rate was measured throughout the treatment.
Results:
After a single treatment of the massage, foot skin blood flow and ROM of the foot and ankle significantly improved in both groups (p < 0.05). Foot skin temperature did not change in STFM, whereas it significantly increased in TFM. Heart rate significantly increased in STFM, whereas it tended to decrease in TFM.
Conclusions:
Both STFM and TFM by a massage therapist could improve foot skin blood flow and ROM of the foot and ankle in diabetic patients with peripheral neuropathy. An STFM could be a promising alternative treatment that patients can perform at home.
Introduction
Diabetic peripheral neuropathy (DPN), also called diabetic foot, is a metabolic disorder that causes impaired blood circulation in the feet of type 2 diabetic patients. 1 The symptoms of DPN include pain, loss of sensation, muscle weakness, and atrophy. The somatosensory deficit in DPN can include loss of muscle spindle function in the lower leg, loss of movement perception at the ankle joint, and loss of plantar cutaneous sensation. 2,3 Losing sensation in the foot can cause severe complications, including neuropathic ulcers. Prolonged infection of an ulcer may require amputation of the leg. 4 The sensory system in the foot also plays an important role in postural control. 5 Postural control during standing is associated with the sensitivity or neural components of the foot. 6 –9 This indicates that a loss of plantar cutaneous sensitivity in type 2 diabetic patients would be associated with a loss of postural stability. In addition, joint mobility in diabetic patients is often impaired due to increased stiffness of the articular capsule, ligaments, and tendons. 10 These dysfunctions of the leg and foot may lead to postural instability and an increased risk of falls in older people. 11
Treatments for feet in diabetic patients include the application of massage with acupressure by using the thumb, finger, palm, or elbow. 12 Massage is a method of performing mediated vasodilation 13 and helps to improve blood circulation and metabolic demands in patients with type 2 diabetes. 13 –18 Massage can decrease pain and improve impaired sensation in diabetic neuropathy patients, because it helps improve blood flow, skin sensation, and joint mobility. 13,19,20 Thai foot massage (TFM) is a form of deep massage using thumb pressure applied along the meridian lines of the foot and the leg, combined with distraction of the toe joints. 12 In diabetic patients, traditional TFM can improve balance and range of motion (ROM) of the ankle and toe joints. 12
Self-massage has also been shown to improve blood sugar levels in diabetic patients. 21 Because self-massage is a low-cost, practical treatment option, a home-based program of self-massage along with a clinic-based program supervised by massage therapists might provide confidence for type 2 diabetic patients to help manage DPN symptoms by themselves. However, there are no studies that have investigated whether a self-Thai foot massage (STFM) can improve the peripheral vascular condition of the foot in type 2 diabetic patients. Therefore, the purpose of this study was to investigate the immediate effects of STFMs on the foot skin blood flow, the foot skin temperature, and ROM of the foot and ankle in type 2 diabetic patients with peripheral neuropathy.
Materials and Methods
Study design
A randomized crossover study was conducted in diabetic patients with peripheral neuropathy. Participants were randomly assigned to a single treatment of massage consisting of either STFM or TFM performed by a massage therapist. They were then switched to the other group after a 1-week washout period.
Participants
Forty type 2 diabetic patients with peripheral neuropathy were recruited from Ban Non Muang and Sam Liam Health Promoting Hospitals in Khon Kaen Province, Thailand. They were assessed for initial eligibility with the Michigan Neuropathy Screening Instrument (MNSI). Data from their medical records were collected with permission from the hospital directors. Inclusion criteria were as follows: (1) an MNSI score higher than 2.5 out of 10 in the physical assessment section of the hospital medical records, (2) diagnosis of type 2 diabetes with well-controlled blood glucose based on three follow-up instances of medical assessments, and (3) ability to sit on the floor for 1 h without pain or discomfort in the lower extremities. Exclusion criteria were as follows: diagnoses of peripheral venous insufficiency; cardiac, renal, or hepatic insufficiency; uncontrolled hypertension; myopathic central nervous system dysfunction; limited ROM in the hip or knee when seated on the floor; loss of sensation; presence of foot ulcer(s); and contraindications of massage, such as fever, recent surgery, acute injuries, skin diseases, varicose veins, undiagnosed pain, and acute inflammation of muscle and joints.
After the screening, 25 patients with type 2 diabetes with DPN were eligible for the study. Figure 1 shows the flow diagram of participant recruitment. Before the start of the study, all participants were informed about the experimental procedures as well as the purpose of the study.
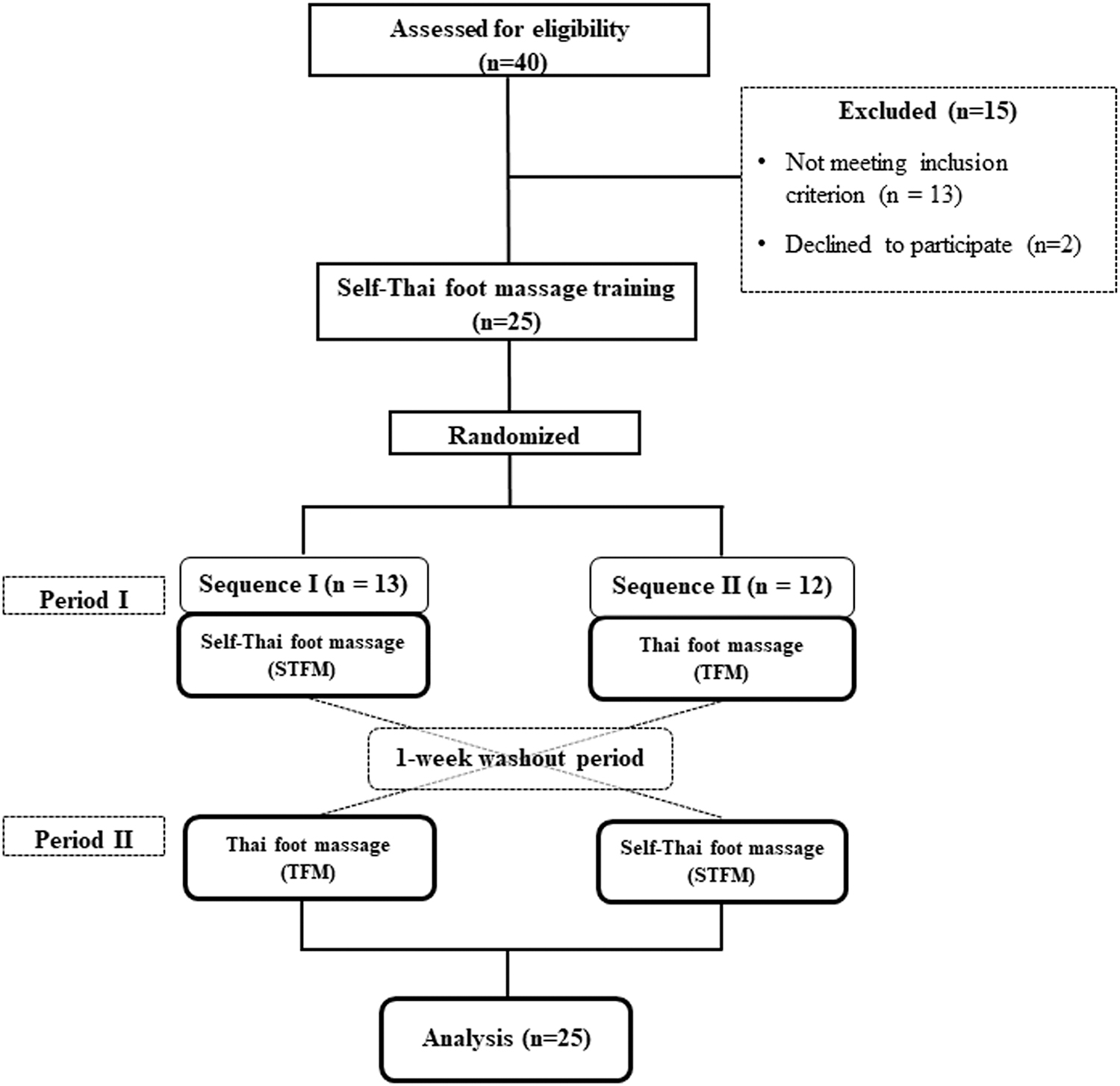
The flow diagram of participant recruitment.
The required sample size was estimated based on a previous study published in the Thai language. The study evaluated the efficacy of femoral artery temporary occlusion on skin blood flow of the foot in 10 healthy participants. 22 The sample size was calculated by using a formula for crossover trials with a standard deviation (SD) of 7 perfusion units (PU), to detect the difference of 4.4 PU in skin blood flow of the foot with 80% power of test and 5% significance. According to these, 25 participants were recruited and they volunteered for their generosity and willingness to participate in this study. Participants were paid for the inconvenience and time spent, and were reimbursed for expenses incurred, in connection with their participation in this study. Written informed consent was obtained from each participant. The protocol and consent forms were approved by the Ethics Committee for Human Research at Khon Kaen University.
Experimental procedure
After recruitment, all participants (n = 25) received three sessions of STFM training, and then they were assessed for their knowledge and skills in traditional TFM until they met satisfactory levels. One week after the STFM training, participants were randomly assigned (block size of 4) to one of two treatment sequences (Fig. 1). Participants in the first sequence performed STFM followed by a washout period of at least 1 week; then, they received TFM. Participants in the second sequence received TFM followed by a washout period of at least 1 week; then, they performed STFM. During the washout period, they were asked not to perform STFM. Foot massage was performed on the dominant lower leg and foot for a period of 25 min with the patient in a seated position. Before and immediately after treatment, heart rate, skin blood flow and skin temperature of the foot, and ROM of the foot and ankle were evaluated. In addition, 15 type 2 diabetic patients under the pretreatment condition were assessed by using the outcome measures in the foot skin blood flow, foot skin temperature, and ROM of the foot and ankle by a single rater at a different time (24 h of duration between two measurements) for the intra-rater reliability tests.
Experimental protocol
Figure 2 shows the experimental protocol consisting of pre- and post-measurements for TFM. Before and immediately after the treatment of TFM, the outcome measures were assessed by an experienced physical therapist with experience of 5 years; this therapist was blind to the treatment sequence of the participant. All outcome measures were performed in a quiet laboratory room, located next to the massage treatment room, in a thermoneutral environment of 23°C ± 2.0°C with an average humidity of 38% rh.
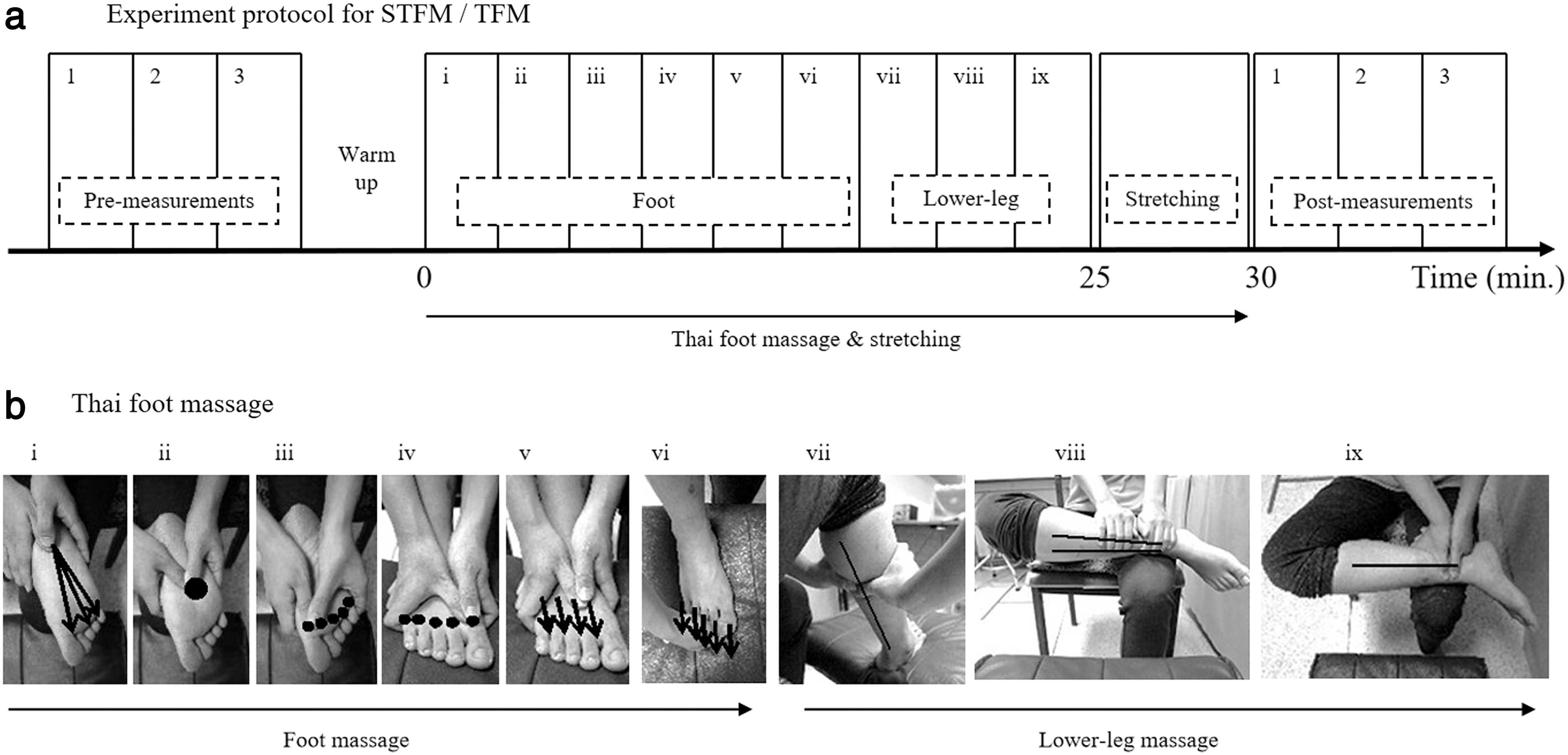
Experimental protocol. Measurements were assessed before and immediately after the treatment in order
Before the TFM treatment, the participants warmed up with 5 min of stretching of the lower back and leg muscles. Nine forms of TFM were performed on the meridian lines and pressure points of the dominant foot and lower leg for a total 25 min (Fig. 2). Thumb pressure was gently applied along the meridian lines and pressure points and repeated 3–5 times. 12 When participants started feeling discomfort below the pain threshold, pressure was maintained for 5–10 sec at each massage point. 12 A 5-min stretching of the calf and foot muscles was performed after a 25-min TFM was performed. For the STFM, the participants sat on a chair and performed this protocol of TFM on themselves.
For the TFM, one traditional Thai massage therapist was recruited at the physical therapy clinic in Khon Kaen University. Potential volunteers were attracted by advertising the project in the university, and they were tested for the TFM. The massage therapist had 5 years of experience and was certified in the 800-h massage training program conducted by the Ministry of Public Health. The massage therapist was paid for the inconvenience and time spent, and was reimbursed for expenses incurred, in connection with their participation in this study. The massage treatment room for both groups was maintained at a temperature of 25°C ± 5.0°C.
Outcome measurements
Four outcome measurements were assessed in the following order: (1) heart rate, (2) foot skin blood flow, (3) foot skin temperature, and (4) ROM of the foot and ankle.
Heart rate was continuously measured during the treatment by using a heart rate monitor (FT 4; Polar Electro Oy, Kempele).
Foot skin blood flow was measured by using laser Doppler flowmetry (Periflux 5010 system; Perimed, Jarfalla) with a 780-nm wavelength. The standard probe with a diameter of 6 mm was placed at the 1st distal phalanx of the big toe. 23 Special software (Perisoft; Perimed AB Sweden) was used for determining mean values, which were expressed in PU. Figure 3 shows raw data of the skin blood flow of the foot.
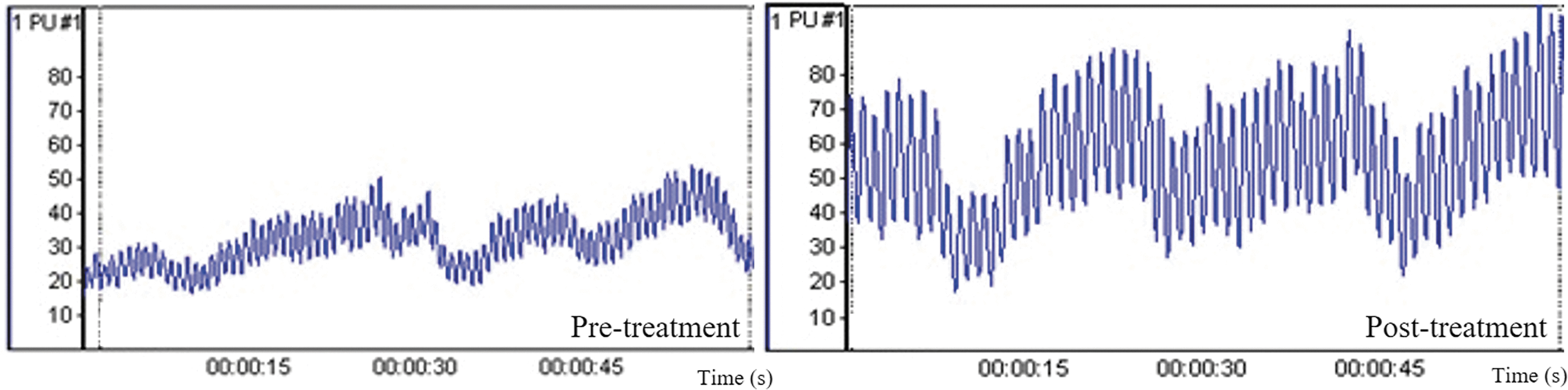
Raw data of skin blood flow of the foot before and after the self-Thai foot massages. Color images are available online.
Foot skin temperature was measured by using an infrared thermal imaging camera featuring in 320 × 240 pixels with an infrared spectral band of 7.5–14.0 μm (Ti10 Fluke Thermal Imaging Camera; Fluke Corporation, Washington). 24 The region of interest (ROI) used to obtain the skin temperature was the whole plantar surface (Fig. 4). The camera was set 80 cm away from the measuring foot in a supine position. 25

Measurement of the skin temperature of plantar surface. Set-up for the infrared thermal imaging camera (left). Square area shows the infrared thermal image with regions of interest in the plantar surface used to obtain the skin temperature (right). Color images are available online.
The maximum pain-free active and passive ROM of the first metatarsophalangeal (MTP) and the ankle joint were measured (Fig. 5). The ROM of the first MTP in the neutral position of the ankle joint was evaluated based on the difference between the neutral position and the maximum flexion/extension of the MTP joint without pain. The ROM of the ankle joint was evaluated based on the difference between the neutral position and maximum dorsiflexion/plantar flexion of the ankle joint without pain. ROM data were photographed and analyzed by using motion analysis software (Kinovea 0.8.15). 26
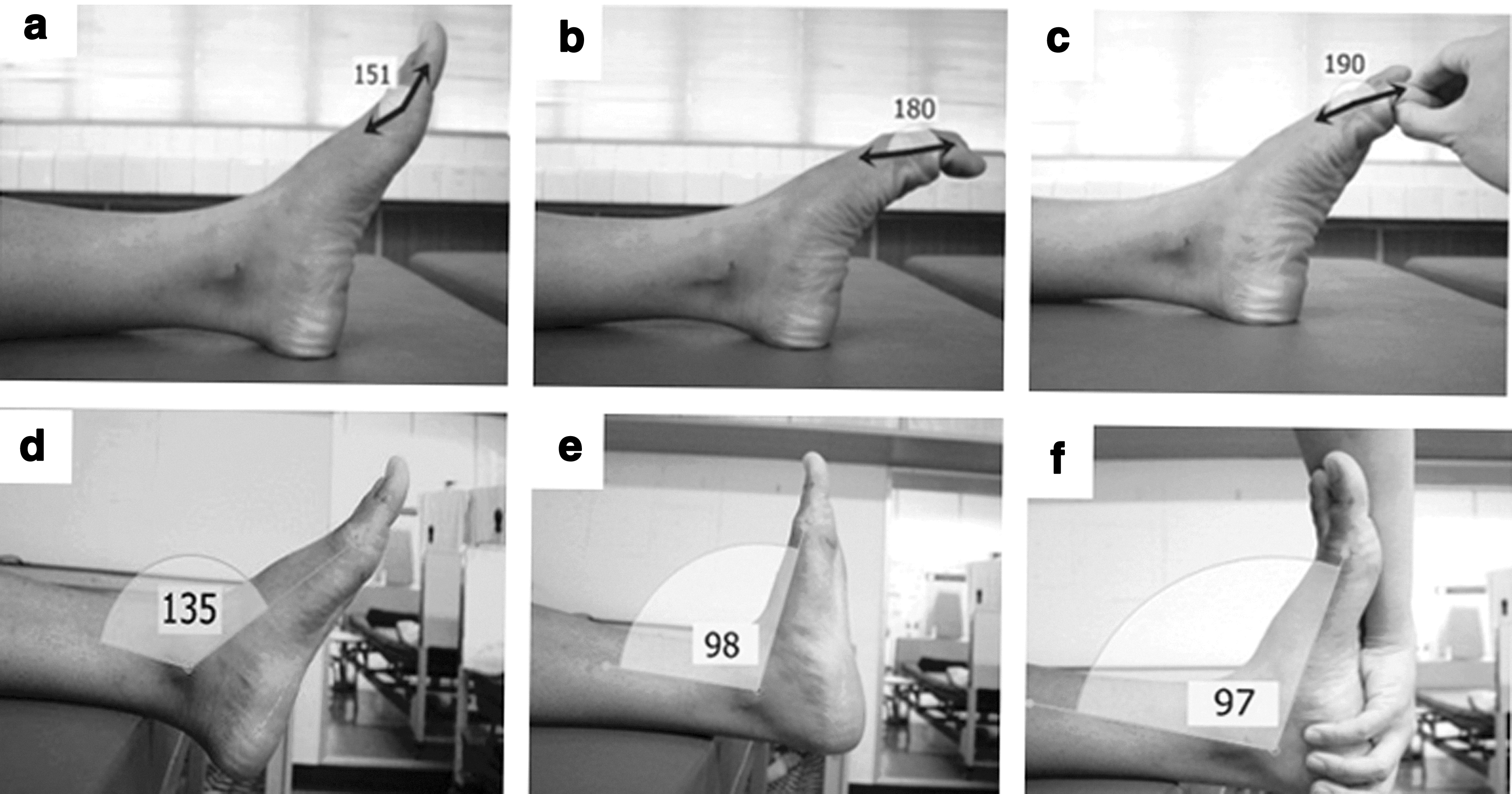
Measurement of the active and passive ROM in first metatarsophalangeal
Data analysis
Data were presented as mean ± SD continuous data and percentage for category data. The intra-rater reliability tests of the outcome measures in the foot skin blood flow, foot skin temperature, and ROM of the foot and ankle were analyzed by using the intra-class correlation coefficient (ICC) with model 3,1 (two-way mixed effect) and the standard error of measurement (SEM) with calculation from the error variance in the ICC formula.
27
A paired t-test was used to compare pre-test and post-test within each group to evaluate the immediate effect. All parameters in each group over two periods were checked for normal distribution. Data of all variables of this study were normally distributed (Shapiro–Wilk W test; p > 0.05). The paired t-test was used to compare before and after the intervention in each period (I or II) and each sequence (1st or 2nd). The period and period × treatment effect (interaction effects) were checked by two sample t-tests. The ordinary least-squares method was used to determine the first- and second-order carry-over effect.
28
If there were no carry-over effects, the pooled data (n = 25) from both sequences were analyzed to compare (pair t-test) the mean change in score (post
Results
The demographic characteristics of participants in both sequences are shown in Table 1. There were no significant differences between the sequences in terms of baseline characteristics (p > 0.05). Table 2 shows the ICC and SEM values for the foot skin blood flow, foot skin temperature, and ROM of the foot and ankle in all directions. The ICC of these outcome values were statistically significant (p < 0.05). Table 3 shows the immediate effects (ES) of the massage on heart rate, foot skin blood flow, foot skin temperature, and ROM of the foot and ankle. After both STFM and TFM treatments, the foot skin blood flow was significantly improved; these increases represent 81.68% ± 55.55% (p < 0.001) and 74.43% ± 63.30% (p < 0.001) of baseline values of STFM and TFM, respectively. Foot skin temperature did not change in STFM, whereas it significantly increased in TFM. Most of the active and passive ROM of the first MTP and ankle joints were improved after both treatments. Heart rate significantly increased in STFM, whereas it tended to decrease in TFM. Comparisons of the outcome measures between pre- and post-assessments in sequence 1 and sequence 2 are shown in Table 4. There were no significant carry-over effects or period effects between the two treatment periods (p > 0.05). Table 5 shows the treatment effects in differences between STFM and TFM. The two treatments had no significant differences in all outcome measures, except foot skin temperature and heart rate.
Demographic Features and Baseline Characteristics
Values are means ± SD. The table compares the demographic features and baseline characteristics of participants in the sequence 1 versus the sequence 2.
BMI, body mass index; MNSI, Michigan Neuropathy Screening Instrument; SD, standard deviation; STFM, self-Thai foot massage; TFM, Thai foot massage.
Intra-Class Correlation Coefficients and the Standard Error of Measurement for Outcome Measures in Pretreatment Measurements (n = 15)
CI, confidence interval; ICC, intra-class correlation coefficient; MTP, the first metatarsophalangeal joint; PU, perfusion units; ROM, range of motion; SEM, standard error of measurement.
Comparison of the Outcome Measures Between Pre- and Post-Assessments in Self-Thai Foot Massages and Thai Foot Massages Using the Pooled Data (n = 25)
Values are means ± SD.
bpm, beats per minute; ES, effect size; MTP, the first metatarsophalangeal joint; PU, perfusion units; ROM, range of motion; SD, standard deviation; STFM, self-Thai foot massage; TFM, Thai foot massage.
Comparison of the Outcome Measures Between Pre- and Post-Assessments in Sequence 1 and Sequence 2
Values are means ± SD.
Denotes a significant difference between pre and post at p < 0.05.
bpm, beats per minute; MTP, the first metatarsophalangeal joint; PU, perfusion units; ROM, range of motion; SD, standard deviation; STFM, self-Thai foot massages; TFM, Thai foot massages.
Comparison of the Average of Mean Change (Post
Values are means ± SD.
bpm, beats per minute; CI, confidence interval; MTP, the first metatarsophalangeal joint; PU, perfusion units; ROM, range of motion; SD, standard deviation; STFM, self-Thai foot massage; TFM, Thai foot massage.
Discussion
This study showed that TFM performed by the patients themselves or by a massage therapist improved foot skin blood flow and ROM of the first MTP and ankle joints in diabetic patients with peripheral neuropathy. Foot skin temperature did not change after STFM, whereas it significantly increased after TFM performed by a massage therapist. Heart rate significantly increased after STFM, whereas it tended to decrease after TFM performed by a massage therapist. These results suggest that both STFM and TFM by a massage therapist could be an effective way to improve foot skin blood flow and ROM of the foot and ankle in diabetic patients with peripheral neuropathy. In addition, STFM can be easy to perform on a daily basis and may have the added benefit of increasing clinical outcomes. Therefore, STFM could be a promising alternative treatment that patients can perform at home.
Foot skin blood flow of diabetic patients with peripheral neuropathy was significantly increased immediately after TFM when compared with the baseline in both treatment groups. Another study reported that foot skin blood flow of type 2 diabetic patients improved by ∼10% after they received massages for 30 min. 14 The mechanism underlying the effects of TFM on blood flow is commonly attributed to the effects of direct compression on the vasculature, localized release of vasodilators, and decrease in sympathetic tone as a response to mechanical pressure on tissue. 30 Accordingly, mechanical pressure from the massage may improve blood flow and thereby enhance skin sensation in the bottom of the foot. 13,20
Foot skin temperature did not change after STFM, whereas it significantly increased after TFM performed by a massage therapist. In accordance with the result of STFM in this study, a previous study shows no significant improvement in foot skin temperature after participants received massages for 30 min. 14 Contrarily, foot skin temperature significantly increased after TFM performed by a massage therapist. Mori et al. also show an increase in foot skin temperature after massage. 20 Foot skin temperature could be increased by the superficial skin friction, which causes local heating to increase within the massaged area. 13,20 Therefore, TFM performed by a massage therapist in this study might give higher skin friction at the bottom of the foot than STFM. These contradictory findings of foot skin temperature after the massage can be explained by the varying effects of different types of massage on the foot.
Traditional TFMs improved ROM of the first MTP and ankle joints when compared with baseline in both treatment groups. TFM improved ROM by about 1–2° in diabetic patients with peripheral neuropathy.
12
Increased range of joint motion may decrease the risk of falls in diabetic patients, because ROM of the foot and ankle could affect balance
11
and the force-generating capacity of the foot and lower leg.
31
The mechanical pressure on the muscle tissue from the massage and the stretching of the leg and foot may decrease tissue adhesion. Muscle-tendon compliance may be increased by mobilizing and elongating connective tissue. Improved muscle compliance results in a less stiff muscle
STFM could be one strategy to promote self-efficacy and self-awareness. A potential impact may be sustainable treatment application for diabetes self-management. 34,35 An STFM might be categorized as a light physical activity, because it significantly increases heart rate. During physical exercise, heart rate increases by the activation of sympathetic activity and inhibition of parasympathetic stimulation from the central command in the brain. 36 Therefore, an STFM may be used practically in acute metabolic regulation for diabetic patients. 37,38 On the other hand, 30 min of TFM and stretching performed by a massage therapist might result in promoting relaxation and not increasing metabolic demands, because it does not increase hear rate. Overall, the results of this study suggest that a home-based self-care massage regimen may promote physical fitness and quality of life while reducing cost of treatment for diabetic patients. Future study is needed to prove the fidelity of self-massage in home-based care.
There are some limitations to this study. Because crossover trials were used in this study, certain weaknesses arise due to carry-over effects. This study used multiple tests to evaluate, which may be the source of the Type I error. 39 This study did not measure plantar cutaneous sensation, which may influence balance in diabetic patients with peripheral neuropathy. Future research should investigate plantar cutaneous sensation with the balance system in diabetic patients. Local change of the foot skin temperature was not detected, because the ROI used to obtain the skin temperature was a whole area of the foot in this study. Further, a longer duration of treatment may be necessary to confirm the long-term effects and follow-up outcomes related to self-massage in diabetic patients with peripheral neuropathy.
Conclusions
Both STFM and TFM by a massage therapist could improve foot skin blood flow and ROM of the foot and ankle in diabetic patients with peripheral neuropathy.
Footnotes
Acknowledgments
The authors would like to express their sincere gratitude and appreciation to all the patients for their generosity and willingness to participate in this study. They gratefully acknowledge Ban Non Muang and Ban Sam Liam Community Primary Public Health Center, Khon Kaen Province, Thailand, for allowing the use of their facilities.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors are indebted to the Research Center in Back, Neck, Other Joint Pain and Human Performance (BNOJPH), Faculty of Associated Medical Sciences, Khon Kaen University, Khon Kaen, Thailand, for providing valuable research funding.