
Abstract
Objectives:
Fufang Banmao (FFBM) capsule, a type of Chinese medicinal formulation, has decades of history in treating hepatocellular carcinoma (HCC). This retrospective study aimed to observe the effect of FFBM capsules on the 6-month survival of patients with advanced HCC and Vp3–4 portal vein tumor thrombosis (PVTT) who received supportive therapy alone.
Design:
In total, 320 HCC/Vp3–4 PVTT patients underwent treatment with supportive therapy, of whom 95 took FFBM capsules and were treated with supportive therapy (FFBM group) and 225 received supportive therapy alone (control group). Comparisons of the 6-month overall survival (OS) rate of the two groups were performed. Propensity score matching (PSM) was used to match the characteristics between individuals in the two groups. A nomogram was built based on independent predictive factors for OS.
Results:
Cox multivariate analysis revealed that hepatic encephalopathy, aspartate transaminase (AST) and γ-glutamyl transpeptidase levels, Child–Pugh class, prothrombin time, α-fetoprotein level, largest tumor diameter, and use of FFBM capsules were independent predictive factors of OS. Variceal bleeding, alanine transaminase, AST, total bilirubin, and Barcelona Clinic for Liver Cancer stage were different at baseline in the FFBM and control groups. Analysis revealed no significant adverse effects or toxicities relevant to the medications. After PSM (1:1), 95 patient pairs were analyzed as FFBM versus control. The OS probability was remarkably higher for patients in the FFBM group than in those in the control group at 6 months (p < 0.0001). The median survival time was 4 months in the FFBM group and 2.2 months in the control group. Kaplan–Meier analysis showed significant statistical differences in the 6-month OS rates in the patients with total nomogram scores ≥84 (p < 0.0001).
Conclusions:
Given the satisfying survival outcomes, the results suggested that FFBM capsules should be administered to patients with HCC/Vp3–4 PVTT in the high-risk group (score ≥84). FFBM capsules have the potential for improving patient survival time in those with advanced HCC and Vp3–4 PVTT who receive supportive therapy alone, especially those in the high-risk group (score ≥84).
Introduction
Approximately 810,000
The Barcelona Clinic Liver Cancer (BCLC) classification system3 states that HCC patients with portal vein tumor thrombosis (PVTT) are, unfortunately, categorized in the advanced stage of disease (i.e., stage C). PVTT is a common complication associated with HCC, with a reported incidence of 34% to 50% in those with advanced HCC. Moreover, PVTT has been touted as a typical negative prognostic factor. 4,5 In settings lacking appropriate treatment modalities, patient survival is ∼3 months. 6 Recently, the Liver Cancer Study Group of Japan proposed a macroscopic classification for PVTT categories using the following five grades: Vp0, no PVTT; Vp1, PVTT distal to the portal vein (PV) second-order branches; Vp2, PVTT in the PV second-order branches; Vp3, PVTT in the first-order branches of the PV; and Vp4, PVTT based on the PV main trunk or a PV branch contralateral to the most major relevant lobe (or both). 7 The association between the extent of PVTT and median overall survival (OS) time was 35.7, 14.6, 9.4, and 5.8 months, respectively, with 4.8 months for Vp0–Vp4 (p < 0.001). 8
According to previous reports, hepatectomy, 9 percutaneous electrochemotherapy, 10 or thrombectomy 11 has been supported for Vp3–Vp4 PVTT treatment. However, none of these therapies can be performed in patients with ascites; those with severe liver function damage (higher than Child–Pugh class B-8) significantly decreased platelet count (platelet count <50,000/mm3), poor coagulation function (international normalized ratio >1.5), and high bilirubin levels (total bilirubin [TBIL] >1.5 mg/dL).
Traditional Chinese Medicine (TCM) has a long history for cancer treatment in China. To date, the Guidelines of Diagnosis and Therapy in Oncology based on TCM were put to use for international standards, which conformed to modern clinical practice. 12 Fufang Banmao (FFBM) capsule, which has been billed as a traditionally applied Chinese herbal formula, exerts an antitumor effect. It is likely to result in prolonged median survival time by improving OS in patients with HCC. 13 However, it is not clear whether FFBM can improve the prognosis of HCC patients with Vp3–4 PVTT. Accordingly, this retrospective clinical research study was conducted to evaluate the effect of FFBM capsules on the OS of patients with HCC and Vp3–4 PVTT.
Materials and Methods
Patients
Between October 2008 and May 2018, 386 patients with HCC were observed at the authors' hospital. Individuals who met the following criteria were included in the present study: individuals aged ≥18 years who received supportive therapy and had BCLC stage C with Vp3–Vp4 PVTT. Patients with current or previous malignancies in addition to HCC, Child–Pugh liver function class C, autoimmune-based liver disease, syphilis, hepatitis A, D, or E, or AIDS, patients for whom complete data were not available or those who were not available for follow-up, and those who had consumed other traditional Chinese herbal formula within 4 weeks before recruitment in the study were excluded.
Supportive therapy is recommended in patients with massive ascites, upper gastrointestinal bleeding due to esophageal varices, hepatic encephalopathy, Child–Pugh class C liver function, poor Eastern Cooperative Oncology Group (ECOG) performance status, and those not suitable for sorafenib treatment. HCC/PVTT patients undergoing supportive therapy did not receive local or systemic chemotherapy, radiotherapy, radiofrequency ablation, and/or surgical treatment involving resection. They were, instead, treated with symptomatic supportive care aimed at treating ascites, hypersplenism, upper gastrointestinal bleeding, and hepatorenal syndrome, as well as hepatic failure caused by portal hypertension. Patients in the two groups were administered supportive treatment according to standardized treatment principles in the follow-up period. Tenofovir, entecavir, lamivudine, telbivudine, or adefovir was used for patients based on the hepatitis B virus replication degree. Liver protection drugs, plasma, and human albumin were used for patients based on liver function, prothrombin activity, and plasma albumin level. The application of diuretics was based on the patient's ascites and edema, and the application of vitamins and glucose was based on the patient's food and water intake. Patients with bacterial infections were treated with antibiotics. In addition, complications such as hepatorenal syndrome, hepatic encephalopathy, and upper gastrointestinal bleeding were treated with appropriate treatment methods.
This research obtained approval from the Institutional Research Ethics Committee attached to the Beijing Ditan Hospital, Capital Medical University (Beijing, China). The study protocol adhered to the tenets of the Declaration of Helsinki, following the principles of “Good Clinical Practice.” All patients provided informed written consent to participate in the study.
Interventional medicines
FFBM refers to the herbal extraction, which comprises Banmou (Mylabris phalerata Pallas or Mylabris cichorii Linnaeus), Ginshen (Panax ginseng C. A. Mey), Huangqi (Radix astragali), Ciwujia (Radix et Caulis acanthopanacis senticosi), Sanleng (stem of Sparganium stoloniferum Buch.-Ham), Banzhilian (Herba scutellariae barbatae), Ezhu (Rhizoma curcumae), Shanzhuyu (Fructus corni), Nvzhenzi (Fructus ligustri lucidi), Xiongdanfen (Fel Ursi Powder), and Gancao (Radix glycyrrhizae) (Table 1). All ingredients of FFBM have been approved by the State Food and Drug Administration (SFDA) of China.
The Ingredients Contained in Fufang Banmao Capsules
From the above eleven herbs, Ginseng, Shanzhuyu, Nvzhenzi, and Banzhilian were crushed into powder and sieved; Banmou was soaked (in 95.2 mL chloroform for 72 h each time) and extracted thrice, which was further concentrated without chloroform. The other five herbs, namely, Huangqi, Ciwujia, Sanleng, Ezhu, and Gancao, were decocted with water thrice (the first time for 3 h, the second time for 1.5 h, and the third time for 1 h). The decoctions were combined, filtered, and concentrated to the relative density of about 1.20 (80°C). Thereafter, the Fel Ursi Powder was dissolved in water at 80°C, which was then mixed with the above extract and powder and allowed to dry below 80°C. It was then smashed into powder and put into capsules (0.25 g/capsule). The content of the capsule is a yellow green to brown powder, and the taste is slightly bitter and sweet. Z52020238 represents the approval number of national medicine permission number of FFBM capsule (Yibai Pharmaceutical Co., Ltd., Guizhou, China). The daily dose of FFBM is six capsules, administered orally twice per day. The suggested intake is after meals, given that some patients occasionally experienced abdominal discomfort after taking FFBM in a fasted state.
Follow-up treatment
Patients underwent clinical assessment at baseline and every 1 or 2 months thereafter. During each visit, investigational data, including heart rate, pill counts, and adverse events, were noted. In addition, blood samples were collected for hematologic measurements. All adverse events were recorded, regardless of the likely relevance to the illness or the research treatment. The duration of the clinical intervention period was 6 months. Follow-up treatment concluded at the endpoints. The primary endpoint was OS; the secondary endpoints represented disease progression.
Statistical analysis
The sample size was calculated by PASS software version 15.0.5 (NCSS, LLC, UT) by the log-rank test; the parameters were set as follows: α = 0.05 (two sided), β = 0.8, and FFBM group/control group = 1/3; median survival time was 2 months in the control group and 4 months in the FFBM group. Continuous variables are expressed as mean ± standard deviation. Pearson's χ 2 tests, based on Fisher's exact likeliness, were used to analyze the frequency distributions of the categorical variables in the two groups. One-way analysis of variance was used to compare differences in the means of continuous variables between the two groups. Furthermore, a one-to-one propensity score matching (PSM) was used to reduce bias in the analysis. The FFBM group was matched with the control group according to the generated propensity scores using a caliper width of 0.05, which was processed using SPSS 22.0 (SPSS, Inc., Chicago, IL). Nomogram was established by rms package of R software version 3.6.3 (R Foundation for Statistical Computing, Vienna, Austria). The Kaplan–Meier method was used to compare long-term survival rates. In addition, the log-rank test was performed to analyze survival curves; p < 0.05 was considered to be statistically significant.
Results
Prognostic factors of survival
According to the findings of univariate Cox regression analysis, ascites, hepatic encephalopathy, spontaneous bacterial infection, hepatic alanine transaminase (ALT) level, aspartate transaminase (AST) level, γ-glutamyl transferase (GGT) level, Child–Pugh class, neutrophil-to-lymphocyte ratio, creatinine level, prothrombin time (PT), α-fetoprotein (AFP) level, tumor number, largest tumor diameter, and FFBM capsule therapy were the survival factors. These variables were subsequently entered into the multivariate Cox regression analysis. Finally, hepatic encephalopathy, AST, GGT, Child–Pugh class, PT, AFP ≥400 ng/mL, largest tumor diameter ≥5 cm, and FFBM capsule therapy were found to be significant elements that affected the prognosis for OS using the forward selection procedure (Table 2).
Univariate and Multivariate Cox Regression Analyses for Overall Survival of Hepatocellular Carcinoma with Vp3–4 Portal Vein Tumor Thrombosis
AFP, α-fetoprotein; ALT, alanine transaminase; AST, aspartate transaminase; CI, confidence interval; Cr, creatinine; FFBM, Fufang Banmao; GGT, γ-glutamyl transferase; HBV, hepatitis B virus; HR, hazard ratios; NLR, neutrophil–lymphocyte ratio; PT, prothrombin time.
Baseline characteristics
Collectively, 320 patients diagnosed with HCC and Vp3–4 PVTT, undergoing FFBM capsule or supportive therapy, comprised the research cohort. Among these, 95 were treated with FFBM capsule therapy, and 225 underwent supportive therapy (Fig. 1). The FFBM group exhibited a clearly comparable difference from the control group for baseline characteristics before PSM. The FFBM group demonstrated a lower variceal bleeding rate than the control group (p = 0.007) and lower ALT, AST, and TBIL levels compared with the control group (p < 0.001; p = 0.005). There was a clear difference in BCLC stage between the FFBM and control groups (p = 0.038) (Table 3).

Flowchart of the treatments included in the study. FFBM, Fufang Banmao; HBV, hepatitis B virus; HCC, hepatocellular carcinoma; HCV, hepatitis C virus; PVTT, portal vein tumor thrombosis.
Baseline Characteristics of Patients Before and After Matching
Data are presented as median (interquartile range).
t-Test.
Chi-square test or Fisher's exact test.
Mann–Whitney U test.
ALT, alanine transaminase; AFP, α-fetoprotein; AST, aspartate transaminase; BCLC, Barcelona Clinic Liver Cancer; Cr, creatinine; FFBM, Fufang Banmao; GGT, γ-glutamyl transferase; HCC, hepatocellular carcinoma; NLR, neutrophil–lymphocyte ratio; PT, prothrombin time; TBIL, total bilirubin; TNM, Tumor, Node, Metastasis staging.
In the FFBM versus control group matched 1:1, the propensity score model was composed of variables, including variceal bleeding; ALT, AST, and TBIL levels; and BCLC stage. Following PSM, the crucial relevant characteristics demonstrated balanced performance (Table 3).
OS analysis
In the 6-month follow-up, 49 of 225 (21.8%) patients were in the control group, and 31 of 95 (32.6%) patients were in the FFBM survival group (Fig. 2a). The median survival period was 2.2 months in the control group and 4 months in the FFBM group. Before PSM, Kaplan–Meier analysis revealed that the FFBM and control groups demonstrated a significant difference in OS (p = 0.0004) (Fig. 2a). PSM was used to form 95 pairs of patients in the control versus FFBM group (i.e., 1-to-1 matched). OS demonstrated a dramatic value in the FFBM group compared with that in control group after 6 years (p < 0.0001) (Fig. 2b).
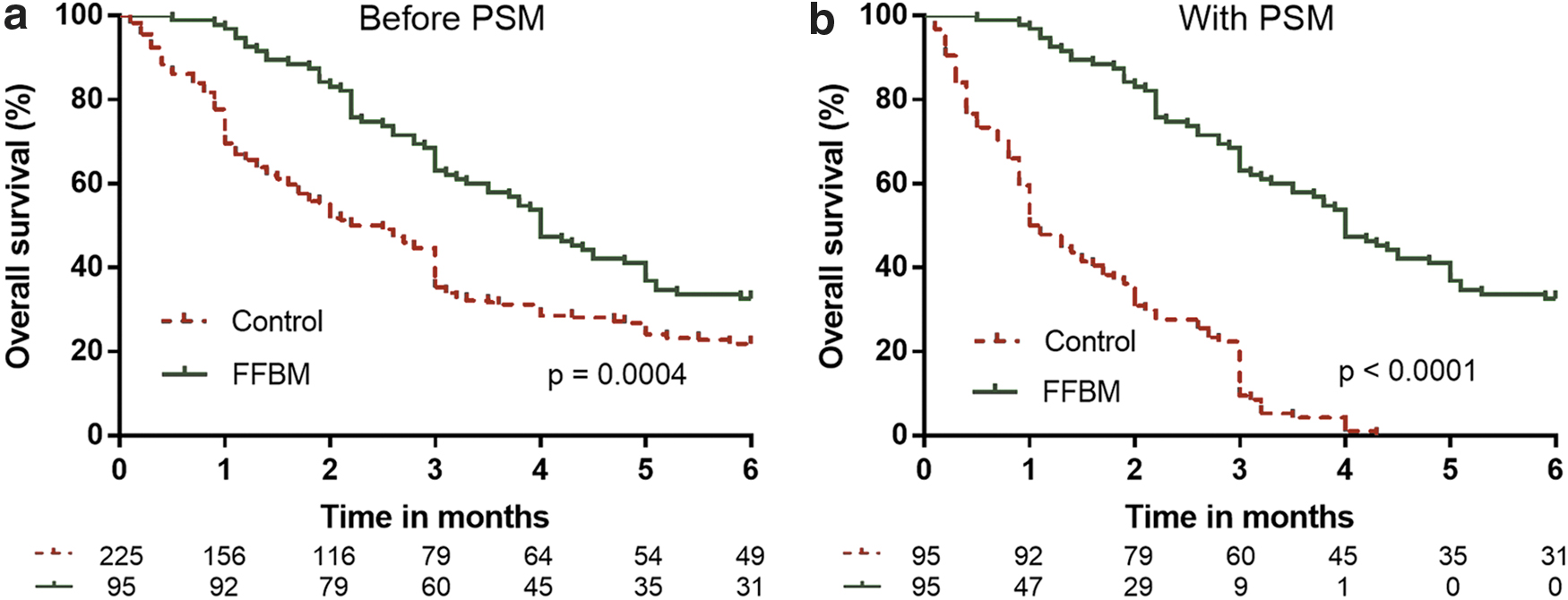
Kaplan–Meier curves of 6-month OS of patients with HCC and Vp3–4 PVTT in the FFBM group compared with those in the control group before
Subgroup analysis
Further analysis was performed on the 6-month OS of patients with HCC and Vp3–4 PVTT and in BCLC stage C or D, AFP <400 ng/mL or AFP ≥400 ng/mL, and tumor diameter <5 cm or tumor diameter ≥5 cm who underwent FFBM or supportive therapy. Results demonstrated that the 6-month OS was significantly higher in those with BCLC stage C (Fig. 3a) or D (Fig. 3b), AFP ≥400 ng/mL (Fig. 3d), and tumor diameter ≥5 cm (Fig. 3f) after FFBM capsule therapy (p = 0.0085, p = 0.0248, p = 0.0042, and p < 0.001, respectively). Six-month OS revealed similarity in AFP <400 ng/mL (Fig. 3c) and tumor diameter <5 cm (Fig. 3e) after FFBM or supportive therapy (p = 0.0564 and p = 0.9603, respectively).

OS in the FFBM group compared with those in the control group over the 6-month follow-up period for patients with BCLC C stage
Nomogram
A nomogram was constructed based on the abovementioned predictors, which was used to predict the 1-, 3-, and 6-month OS rates by adding the score corresponding to each factor and highlighting the overall score to the bottom scale (Fig. 4). Details concerning the point assignment from the nomograms and the prognostic score are shown in Table 4. The c-index of predicated OS was 0.687 (95% confidence interval 0.651–0.723). The patients were divided into two quartiles according to total scores: low risk, 0–83, and high risk, ≥84. There was no remarkable difference between the FFBM and control groups in terms of OS of the low-risk group (p = 0.9001) (Fig. 5a). Kaplan–Meier analysis revealed significant statistical differences in the OS rate in the FFBM and the control groups in the high-risk group (p < 0.0001) (Fig. 5b).

Nomogram predicting 1-, 3-, and 6-month OSs of patients with HCC and Vp3–4 PVTT. The total point was obtained by adding the scores of each variable corresponding to the point on the upper pointing axis. A line was then drawn to the probability axis of the graph at the bottom, which indicated the survival probability at 1-, 3-, and 6- months. AFP, α-fetoprotein; ALT, alanine transaminase; AST, aspartate transaminase; GGT, γ-glutamyl transferase; HCC, hepatocellular carcinoma; OS, overall survival; PT, prothrombin time; PVTT, portal vein tumor thrombosis.

Kaplan–Meier curves stratified according to risk scores:
Nomogram Scoring System
AFP, α-fetoprotein; AST, aspartate transaminase; GGT, γ-glutamyl transferase; PT, prothrombin time.
Discussion
Several technical treatments have been used to treat patients with HCC and PVTT, including surgical resection, 14 transcatheter arterial chemoembolization, 15 hepatic arterial infusion chemotherapy, 16 as well as systemic chemotherapy. 17 However, an effective adjuvant therapy is needed for patients with both Vp3–Vp4 PVTT and HCC with end-stage liver disease, including severely impaired liver function and/or severe complications, who cannot receive local or systemic chemotherapy, radiotherapy, radiofrequency ablation, and/or resection.
TCM is an advantageous option for patients with advanced cancer, older patients, or those deemed unsuitable for radiotherapy and/or chemotherapy. For example, with slight negative reactions, TCM helps consolidate the stability of tumor lesions, enhance symptoms, and improve quality of life, as well as lengthen survival time. 18 A strategically applicable approach to prevent tumor progression is control of HCC metastasis. It is reported that various TCM herbs have this property. In particular, SiniSan inhibits HCC cells from HBx-induced migration and invasiveness in virtue of inhibiting multiple signal transduction pathways, including ERK/phosphatidylinositol 3-kinase/Akt upstream of NF-κB and AP-1 in human HCC cells. 19 Huaier constrained SKHEP-1 cells from exerting metastatic capability by decreasing Lamin B1 levels and elevating NOV levels. 20
Paeonol, one of the ingredients of FFBM capsules, can reduce liver inflammation and improve immune function in rat models of HCC. 21 In addition, it is reported that cantharidin in FFBM capsule, a PP2A inhibitor, inhibits tumor cell growth by regulating the G2/M cell cycle. 22 Cantharidin analog helps stimulate proapoptotic signaling and caspase-3, -8, and -9 and p38-mediated apoptotic pathway in HCC cells. 23 Norcantharidin, a demethylated form of cantharidin, regulates the polarity of macrophages by increasing the expression of miR-214, thereby inhibiting the progression of HCC. 24
Palliative sorafenib chemotherapy is the standard treatment for advanced HCC, according to the BCLC staging system and treatment guidelines. 25 Casadei Gardini et al. identified the predictive indicators of sorafenib efficacy, and the results showed that immune-inflammation index ≥360 and neutrophil–lymphocyte ratio ≥3 were independent risk factors of OS for patients with HCC treated with sorafenib. 26 In addition, a study has reported that patients treated with a combination of sorafenib and metformin have worse progression-free survival (p = 0.029) and OS (p = 0.014) than those treated with sorafenib alone. 27 The present research demonstrated that FFBM capsules, a popularized TCM, can be used as an adjuvant treatment for patients with Vp3–Vp4 PVTT/HCC with end-stage liver disease, who cannot receive local or systemic chemotherapy, radiotherapy, radiofrequency ablation, and/or resection. Most patients had HBV-related disease, ≥3 tumors, and a tumor diameter ≥5 cm, TNM stage III, and BCLC stage C (Table 3). A significantly improved endpoint in OS rate with FFBM was demonstrated (32.6% in FFBM vs. 21.8% in the control group; p = 0.0004) (Fig. 2a).
Clinical and radiologic characteristics exhibited by HCC patients with Vp3–4 PVTT were incorporated into multivariate Cox regression analysis. The authors found that AST, GGT, PT, hepatic encephalopathy, AFP ≥400 ng/mL, tumor diameter ≥5 cm, and Child–Pugh class C were independent predictors of individual survival outcomes. Based on these seven parameters, an effective and easy-to-apply nomogram was constructed to estimate the individual survival prognosis of patients with HCC with Vp3–4 PVTT at 1, 3, and 6 months. Moreover, after stratifying the survival rates according to the cutoff value, the authors further identified the prognostic discrimination of the nomogram scores. The 6-month OS of the FFBM group was significantly longer than that in the control group of the high-risk group. Therefore, it is possible to consider FFBM therapy for patients in the high-risk group to achieve the goal of prolonging survival.
The present research had some limitations, including the design and data sources. First, it was a retrospective cohort study with unavoidable biases in clinical differences shared by the FFBM and control groups. Despite patient matching based on propensity score for the elimination of confounding factors, a significant difference remained in some biochemical indicators, including age and ALT level. As such, a rigorous prospective randomized controlled trial is needed to verify the curative effect of FFBM capsules on the survival of patients with HCC. Second, no positive control drugs were available (i.e., no drugs can effectively cure Vp3–4 PVTT). In addition, sorafenib should be the primary suggested first-line treatment for advanced-stage patients with Child–Pugh class A liver function. Patients enrolled in this study with severely impaired liver function and/or severe complications were not suitable for sorafenib therapy.
Conclusions
In summary, this retrospective cohort study demonstrated that adjuvant therapy based on FFBM capsule may lengthen the median survival time of patients with Vp3–4 PVTT/HCC and end-stage liver illness. After stratification according to nomogram score, the 6-month OS of the FFBM group was significantly longer than that in the control group of the high-risk group, which may help guide treatment decisions.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Capital's Funds for Health Improvement and Research (Grant No. 2018-1-2172) and the National Natural Science Foundation of China (NSFC) under Grant Nos. 81473641 and 81774234.