
Abstract

Introduction
Pain is a core complaint reported by patients electing orthopedic surgery to remediate joint problems. 1 Individual psychologic factors such as pain catastrophizing and distress can exacerbate the experience of pain and limit pain self-management before and after surgery. 2 Mindfulness training is used to foster heightened awareness of bodily experiences without cognitive elaboration and judgment and thus may help orthopedic patients better manage their pain through acceptance of discomfort and reduced catastraphizing. 3 This study assessed the feasibility of implementing a one-to-one telephone-based teacher-led mindfulness training before and after orthopedic surgery. In addition, the authors assessed changes in participant pain appraisals, physical disability, psychologic distress, and mindfulness levels during the perioperative period.
Methods
Patients were recruited from a Southern California orthopedic clinic in 2015. Adult patients who had been recommended for upper extremity joint surgery within 6 weeks from the date of recruitment were recruited for this feasibility trial. Participants completed self-reported assessments ∼2 weeks before surgery and at 2-, 5-, and 10-week postsurgery date. In addition, one phone call was made at the end of each of the four assessment periods to assess the amount of time participants practiced the mindfulness skills they learned during the training phone calls and from the audio-guided compact disc.
For the intervention, participants received two 45-min mindfulness training phone calls, one ∼2 weeks before and one 2 weeks after surgery, led by an experienced meditation instructor trained in Mindfulness-Based Stress Reduction (MBSR). The first call included an introduction to mindfulness, 15-min guided meditation, 10-min discussion of sensory experience during the call, and home mindfulness practice instructions. The second call began with reconnecting with the teacher and review of the purpose of the training, reflection of the surgical and practice experience, a 20-min guided mindfulness practice, and closing. Participants received an audio-guided meditation compact disc with instructor-recorded meditation modules ranging from 10 to 35 min for daily home practice. Participants received $20 for each survey returned and an extra $5 for reporting mindfulness practice days and times.
At all assessments, participants completed the Universal Pain Assessment Tool (UPAT) to quantify pain level, 4 Disability of the Arm, Shoulder and Hand Test (DASH) to quantify physical disability, 5 Depression, Anxiety, Stress Scale-21 (DASS) to quantify distress level, 6 and the Five Facet Mindfulness Questionnaire 24-item (FFMQ) to quantify mindfulness level. 7 Summary statistics at each assessment time point were analyzed to observe the mean changes of these measurements across the perioperative period.
Results
Eighty-five patients were interviewed, 20 met surgical eligibility, and 13 were enrolled after completing the signed informed consent process. Seven were not enrolled due to change in surgical date or decision not to participate. Of the 13 patients in the sample, nine patients (69.2%) had surgery at the shoulder, three patients had elbow surgery, and one wrist surgery. Participant mean age was 55.4 years (standard deviation = 13.9), 69.2% were male, and 84.6% were white. For comorbidities, 5 (38.5%) had hypertension, 3 (23.1%) had hyperlipidemia, and 6 were overweight/obese (body mass index ≥25.0) at the time of surgery. At baseline assessment, participants reported moderate pain (UPAT: M = 5.6 ± 2.5), moderate disability (DASH: M = 55.3 ± 15.4), and mild psychologic distress (depression: M = 5.3 ± 4.8; stress: M = 7.4 ± 5.0; and anxiety: M = 2.9 ± 2.7). Nine of the 13 participants completed week 2, and 7 participants completed weeks 5 and 10 assessments.
All 13 participants received the two 45-min mindfulness training telephone calls. Ten participants responded to the calls to assess their audio-guided meditation practice during the 10-week follow-up period. Median practice time was 5 days per week and 20 min per day between first intervention call and surgery date. Median practice time decreased to 3 days per week and 20 min per day at week 2, 2 days per week and 15 min per day at week 5, and 1 day per week and 13 min per day at week 10.
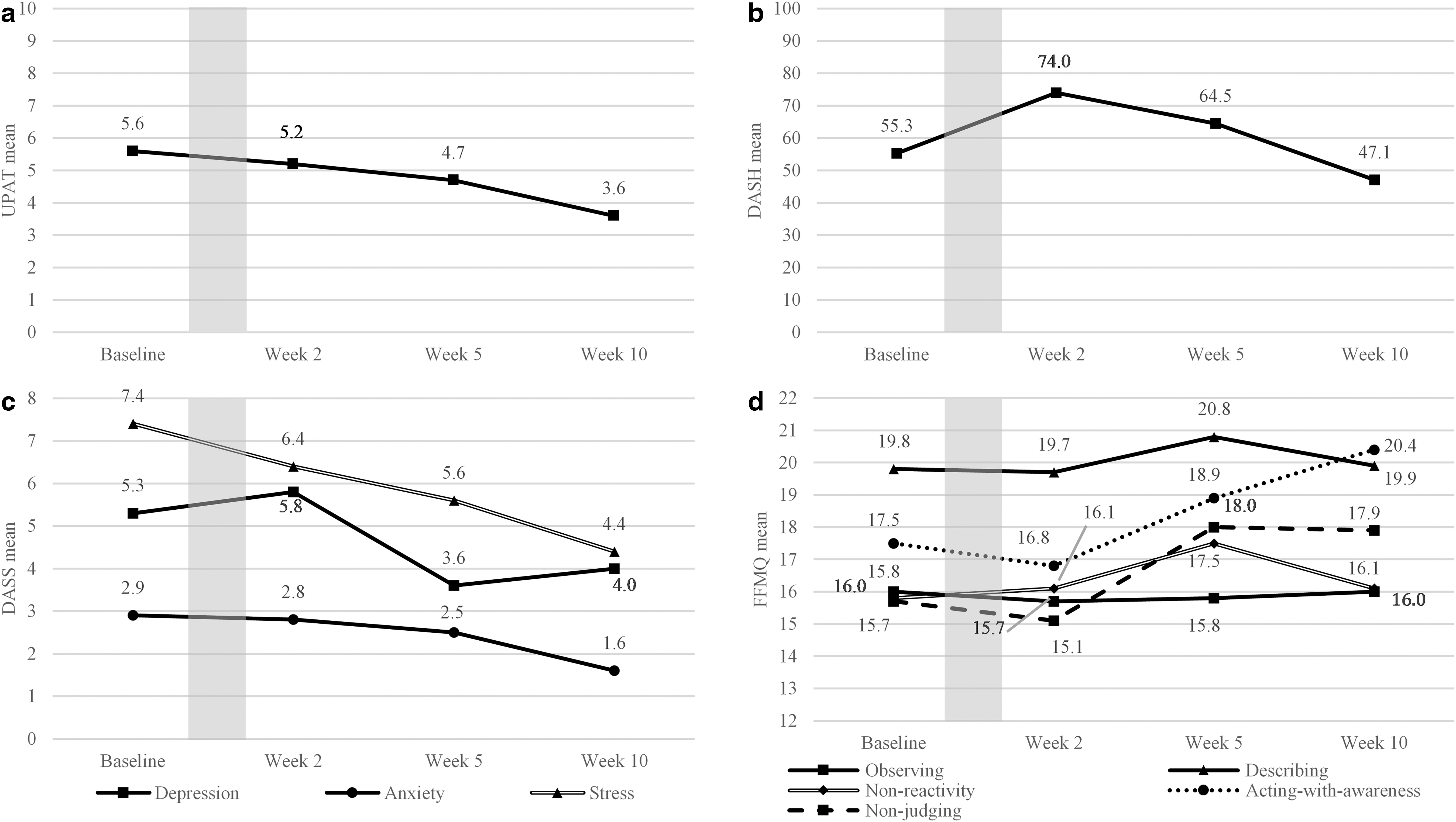
Figure 1 shows changes in measure scores from baseline to week 10. UPAT mean scores decreased by 2.0 (5.6–3.6). DASH mean scores increased at week 2 (55.3–74.0), then decreased by week 10 (74.0–47.1). DASS mean scores improved for depression (5.3–4.0), anxiety (2.9–1.6), and stress (7.4–4.4) from baseline to week 10. FFMQ mean scores improved for the acting-with-awareness (17.5–20.4) and non-judging (15.7–17.9) domains from baseline to week 10.
Discussion
This study tested the feasibility of a telephone-based mindfulness instruction before and after upper extremity orthopedic surgery. This is often a stressful period for patients as they anticipate surgery and voice concern over postsurgical recovery. The authors were able to successfully deliver the one-to-one teacher-led mindfulness training by phone, and participants reported using the prerecorded audio meditation multiple times per week, thus suggesting their willingness and motivation to comply with mindfulness skill-building activities. In addition, no adverse events were reported related to the mindfulness practice. However, practice effort declined over time, informing the need for cues to action and motivational incentives in future research. This trial was not designed to test treatment efficacy; however, the authors did observe within-subjects trends in improved pain, disability, distress, and mindfulness levels after surgery. The 2-point average decrease in pain (UPAT) achieved a clinically important 8 improvement in the sample. The decrease in disability (DASH) from weeks 2 to 10 also exceeded the 10-point clinically important improvement. 5 Change scores in DASS did not meet the clinical improvement cutoff. 9
Limitations of this feasibility study include loss to follow-up that resulted in missing data during the follow-up period. It is also difficult to disentangle any benefits between the two interventions, surgery, and mindfulness training. This study achieved its goal to demonstrate that mindfulness trainings could be administered to orthopedic patients by a trained MBSR teacher by telephone during the perioperative period. Next stage studies aiming to test the efficacy of mindfulness training on pain and pain-related symptoms among orthopedic patients in the perioperative period should attend to the characteristics of this population's potentially low intervention compliance, high levels of surgical rescheduling, therapeutic mechanism, 10 and probable need for incentives for follow-ups.
Footnotes
Author Disclosure Statement
All authors declare that there are no conflicts of interest.
Funding Information
Funding was provided by the University of Southern California Zumberge Interdisciplinary Grant to D.B. and G.S., and resource support was provided by the American Mindfulness Research Association.