
Abstract
Objectives:
Cancer treatment can present its own physical and mental challenges resulting in symptoms such as fatigue, stress, pain, nausea, and vomiting. Aurora Health Care is a large health system with 19 cancer centers. Integrative therapies such as acupuncture and massage have demonstrated success in reducing cancer-related symptoms and side effects to conventional cancer treatment and improving patient outcomes. In 2018, 15 of the 19 Aurora Cancer Clinics embedded a replicable Integrative Cancer Care closed model to provide adjuvant therapies for the best patient outcomes. This quality improvement study aimed to explore if the replicable integrative care model could demonstrate consistent outcomes for massage and acupuncture therapies aimed at symptom reduction across multiple oncology clinics.
Design:
Aurora Cancer Care and Aurora Integrative Medicine designed a reproducible integrative therapy service model to be embedded into the Aurora Cancer Centers. Integrative therapies within the cancer centers allow patients easy access to care before, during, or after their cancer treatment. In 2018, 15 of the 19 cancer clinics had integrative therapies available to patients with cancer. This model required unified operations, onboarding, training, competency, and clinical oversight to achieve consistent processes for consistent outcomes. Furthermore, these innovative models prioritized the following: patient access (easy and affordable); service delivery (consistent and operationalized); clinical outcomes (effective and meaningful); and caliber of clinician (competent and confident). Aurora Health Care employs massage therapists (Mts) and acupuncturists (Ats). This employment model allows for standards and program model adherence. To achieve competent and confident clinician's, MT or AT must complete a cancer treatment-focused competency training program relative to their respective profession and adherence to practice standards outlined. The training program is built on evidence-based practice, observation, direct demonstration, return demonstration, mentorship, and ongoing quality review by clinical leaders. Aurora's Integrative Cancer Care closed model of care is accessible to patients through philanthropic funds secured to underwrite the free service of MT provided during infusion treatments. Funds also provided three free AT sessions. Ongoing acupuncture therapies were provided at a low-cost group acupuncture fee at $25.00 per treatment. Acupuncture is available in group format and provided either before or after chemotherapy treatment. The free services were intended to introduce the concept of integrative therapies as a viable adjuvant option with conventional cancer care. As this model incorporates a mix of philanthropic funding and low-cost fees to offset the cost of the therapy provider, it is referred to as a “closed model” or accessible only to those patients under the care of an Aurora Cancer specialist. In 2018, 15 Aurora Cancer Clinics offered massage and 11 Aurora Cancer Clinics offered acupuncture. Patients who self-selected integrative therapies via system-employed Mts and Ats were surveyed pre/post acupuncture and MT treatments using a visual analog scale about their perceived levels of pain, stress, nausea, and neuropathy. The staff integrative clinicians collected data from patients, and post-treatment data were compiled by the Department of Integrative Medicine.
Settings/Location:
Aurora Cancer Centers are embedded within Aurora hospitals or free-standing clinics located throughout Wisconsin. In 2018, 15 cancer clinic locations embedded Mts, and 11 cancer clinic locations embedded Ats.
Subjects:
Oncology patients.
Interventions:
Clinical competencies were developed and applied to address indications, contraindications, and oncology-specific procedures to ensure that consistent quality of therapies was provided across sites. In 2018, Ats delivered 4367 Ats across 11 locations and Mts delivered 4197 Mts across 15 locations. During this study, the number of treatments provided was tracked versus episodic care.
Outcome Measures:
Pre/post AT and MT pain, stress, nausea, and neuropathy scores were recorded (0 [least] to 10 [worst]) and compared using paired t-tests.
Results:
Pre/post AT scores for pain, neuropathy, stress, and nausea were all significantly different (p < 0.001). For AT, there was a reported decrease in pain, stress, and neuropathy of 61.7%, 68.8%, and 47.9%, respectively. Pre/post MT scores for pain, neuropathy, nausea, and stress were also significantly different (p < 0.001). MT was greater at reducing stress and pain, 42.5% and 34.4%, respectively.
Conclusions:
Across 15 cancer clinics, both AT and MT treatments consistently and significantly reduced cancer-related side effects. These findings highlight the value of conducting a larger randomized-controlled trial to further assess the impact of Oncological Multisite Massage and Acupuncture Therapy on cancer-related symptoms across multiple oncologic clinics.
Introduction
Patients undergoing cancer treatment face physical side effects and symptoms associated with diagnosis, treatment, and the psychologic distress of a life-threatening illness. These side effects and symptoms may include fatigue, neuropathy, nausea, vomiting, gastrointestinal disorders, sleep disturbances, hot flashes, weight changes, sexual dysfunction, cognitive disorders, and/or mood disorders. 1
Aurora's Integrative Cancer Care considers patient quality of life (QoL) as paramount throughout treatment and survivorship. Treatment-related side effects are common, with up to 85% of cancer patients experiencing cancer-related pain at some point during cancer diagnosis, treatment, and survivorship. 2 The International Association of the Study of Pain defines pain as: “an unpleasant sensory and emotional experience associated with actual or potential tissue damage or described in terms of such damage”. 1,2 Cancer-related pain is difficult to treat and is a source of significant distress for patients. 3 Current pharmacologic options for pain management, such as opioids, have side effects such as fatigue, decreased cognitive function, constipation, and nausea. 3 In addition, opioids carry a risk of misuse and abuse. 3 The distress associated with these symptoms may interrupt treatment and negatively impact survival rates. 4
To provide the best care for patients, in 2018, 15 of the 19 Aurora Cancer Clinics embedded an Integrative Cancer Care closed model for patients to provide access to integrative oncology (IO) adjuvant therapies. IO uses acupuncture treatment (AT) and massage therapy (MT) to improve cancer-related symptoms such as pain and QoL. 3 Up to 60% of National Cancer Institute-designated comprehensive cancer centers use IO. 5 The following review explores the effectiveness of IO services, specifically the use of AT and MT, for reducing side effects and symptoms associated with cancer diagnosis, treatment, and survivorship.
Studies show AT is effective in improving side effects and symptoms throughout cancer diagnosis, treatment, and survivorship. AT involves the physical or electrical manipulation of needles that are inserted in particular points along the body. 3 According to the literature, AT improves physiologic factors such as pain, fatigue, weakness, and frail voice, psychologic factors such as QoL, coping strategies, and sense of personal and treatment control, emotional factors such as anxiety, depression, and relaxation, and cognitive factors such as memory loss and overall recovery. AT also improves functioning of the circulatory system (i.e., hot flashes), digestive system and excretory system (i.e., xerostomia, dysphagia, ileus, sweet and bad tastes in mouth, gas, diarrhea, and blood in the feces), endocrine system (i.e., hypoglycemia and appetite), exocrine system (i.e., excessive sweating), immune system (i.e., leukocytosis, neutropenia, allergies, and inflammation), lymphatic system (i.e., lymphedema), nervous system (i.e., neuropathy and insomnia), respiratory system (i.e., dyspnea), skeletal system (i.e., arthralgia), hematopoietic system (i.e., stem cell mobilization), and the vestibular system (labyrinthitis). Finally, studies show that AT is effective for tobacco cessation as well as for reducing use of opioids and opioid-related side effects (i.e., constipation, pruritus, nausea/vomiting, dizziness, sedation, and urinary retention). 1 –3,5 –8
In addition to AT, MT has been extensively studied in the context of IO and can be defined as an ancient technique that involves the deliberate movement of soft tissues. 9,10 According to the literature, MT improves physiologic factors such as pain, fatigue, discomfort, and scarring, psychologic factors such as QoL and well-being, emotional factors such as mood disorders and stress, and overall recovery. MT also improves functioning of the circulatory system (i.e., blood circulation and blood in tissues), digestive system and excretory system (i.e., elimination, nausea, and vomiting), immune system (i.e., immune system strength), lymphatic system (i.e., lymphedema, lymph clearance, and lymph circulation), nervous system (i.e., neuropathy and nervous system activation), and skeletal system (range of motion). 1,9
Given patient demand and program success, both “oncology acupuncture” and “oncology massage” are now considered specialty areas of practice that require providers to attend to the unique safety issues and psychosocial needs of their patients to improve cancer-related outcomes. 5 To address the impact of “oncology acupuncture” and “oncology massage” within their hospital system, the authors conducted a quality improvement study that aimed to explore whether AT and MT could demonstrate consistency in improving cancer-related symptoms across multiple oncology clinics.
Materials and Methods
In 2018, MTs and ATs employed by Aurora Health Care's Integrative Medicine Department treated patients who self-selected integrative cancer care services. Quality standards were established by requiring each clinical group (ATs and MTs) to: Complete a competency-focused training program. Adhere to a uniform data collection process utilizing visual analog scales (VAS). Participate in randomized chart audits by clinical leaders to assess quality of service provided.
A specific oncology competency-based training program was developed for each discipline. A centralized process within the integrative medicine department is in place to hire, orient, train, and oversee the quality of employed Ats and Mts. The competency focuses for acupuncture addressed a group model with delivery available within the infusion suite/bay. The massage model was limited to treatment provided in an infusion chair. Furthermore, the oncology massage competency encompassed skill training in Reiki levels I&II, aromatherapy, and guided relaxation exercises.
At the time of this study, foundation funds paid fully for Mts in the infusion setting. Foundation funds paid for the first three groups' Ats and subsequent Ats were offered at $25.00 per group session. During this study, the number of treatments versus episodic care was tracked. Overall, in 2018, Ats delivered 4367 Ats across 11 locations and Mts delivered 4197 Mts across 15 locations. Ats were employed part-time ranging from 8 to 20 h per week at 12 of the 15 locations. Mts were employed part-time ranging from 8 to 20 h per week at all 15 locations. Based on philanthropic funds, time and day to access integrative cancer care clinicians vary. Patients could self-select services on the same day as their infusion services.
Patients were surveyed about their perceived levels of pain, stress, nausea, and neuropathy before and after AT and MT. To measure pain, stress, nausea, and neuropathy, patients were asked to rate each on a scale from 0 [least] to 10 [worst]. Patients were provided with a VAS for reference. The integrative clinician collected data voluntarily reported by the patient before and after the integrative treatment. Responses were recorded on templates distributed and collected by Ats and Mts. Completed forms were then faxed to the integrative medicine department office, and recorded and deidentified outcomes were entered into a spreadsheet report to integrative medicine for analysis. To examine whether there were statistically significant differences between pre/post AT and MT scores, t-tests were conducted in STATA (StataCorp LLC, College Station, TX). A two-tailed p-value of <0.05 was considered statistically significant.
In 2018, smart chart data extraction was not available to integrative therapies. To track patient-reported outcomes across multiple site locations, integrative clinicians collected data from patients. Only encounter-related information was tracked and assessed to give us an initial idea about the consistency of the effectiveness of AT and MT for reducing pain, stress, nausea, and neuropathy across multiple oncology clinics. Future studies will focus on capturing both patient-related (e.g., Medical Record Number [MRN]) and encounter-related variables of interest to ensure the effectiveness of AT and MT for reducing side effects and symptoms throughout cancer diagnosis, treatment, and survivorship across multiple oncology clinics with respect to demographic variables and individual diagnosis, treatment, and survivorship information.
Evidence-based clinical competencies were developed by an interprofessional team in the IO department of the hospital system and applied to examine the quality of therapies provided across multiple cancer care clinics within one large, integrated, eastern Wisconsin hospital system. Ats and Mts would further develop and provide individualized treatment plans based on type of cancer, patient conditions, and patients' complaints and goals. Generally, AT consisted of patients receiving treatment fully clothed, in recliners, and in a group setting. ATs used distal acupuncture points placed in patients' arms/hands, legs/feet, and/or head/ears. Points that were chosen were based on specific patient complaints (e.g., pain, neuropathy, stress, nausea). Generally, MT consisted of the MT kneading the patient's feet, hands, and neck. Patients were fully clothed, in recliners, and in a group setting.
Results
Comparing symptoms before and after AT revealed mean pre/post scores for pain 2.99 (pre) versus 1.42 (post), neuropathy 2.75 versus 1.66, stress 3.02 versus 1.18, and nausea 0.45 versus 0.31; all were significantly different (p < 0.001) (Fig. 1). The majority of ATs reported resulted in a decrease in pain, stress, and neuropathy of 61.7%, 68.8%, and 47.9%, respectively. Comparing symptoms before and after MT revealed mean pre/post scores for pain 1.61 (pre) versus 0.84 (post), neuropathy 1.17 versus 0.77, nausea 0.26 versus 0.16, and stress 1.94 versus 0.93; all were significantly different (p < 0.001) (Fig. 2). The impact of MT was greater on reducing stress and pain, 42.5% and 34.4%, respectively.

Massage therapy change in severity, n = 4197. Black shade indicates pre-AT score, gray shade indicates post-AT score, *p < 0.001. AT, acupuncture treatment.
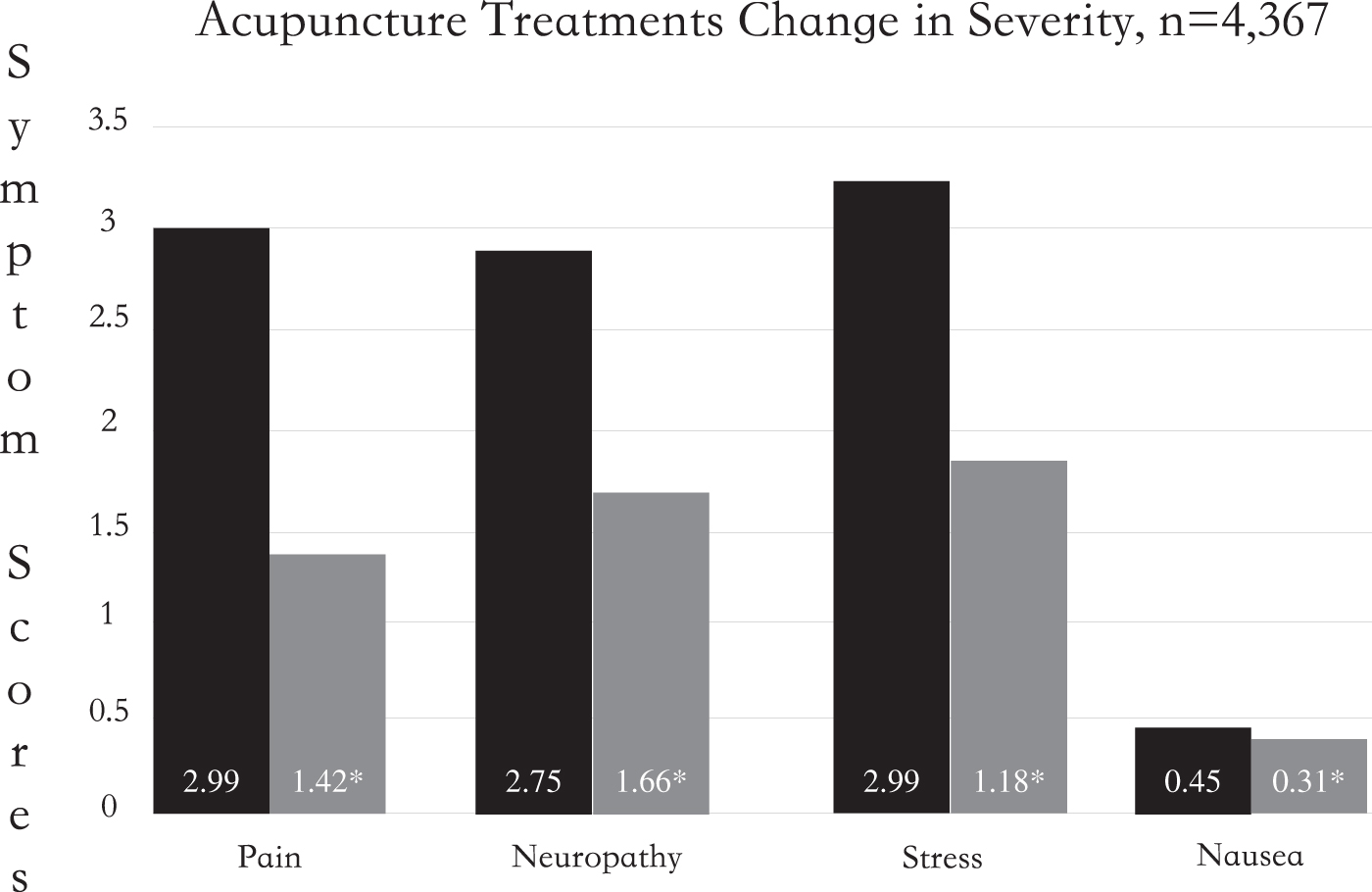
Acupuncture treatment change in severity, n = 4367. Black shade indicates pre-MT score, gray shade indicates post-MT score, *p < 0.001. MT, massage therapist.
Conclusions
To date, most studies that have explored the effectiveness of AT and MT in IO for improving cancer-related outcomes are of poor methodological quality. 2 The strengths of this study include its multisite design and large encounter size. However, this study also has several limitations. First, the authors relied on self-reported pre/post AT and MT scores. Self-reported data are often biased, given each individual's threshold for pain, neuropathy, nausea, and stress. Furthermore, patients' beliefs about the effectiveness of acupuncture and MT in addition to their experiences with individual therapists may influence their reports. Beyond this, the pre/post outcome measures were collected by providers, which may produce bias in the results.
The authors were unable to analyze the effectiveness of AT and MT for reducing pain, neuropathy, nausea, and stress across multiple oncology clinics with respect to demographic variables and individual diagnosis, treatment, and survivorship information. Therefore, there may be an over- and underrepresentation of the level of improvement in symptoms because patients vary in the severity and number of symptoms and side effects they experience, and the authors could not control for these factors. Lastly, this study was not a randomized trial; therefore, there is inherent and unavoidable selection bias because participants were patients who voluntarily participated in the Ats and Mts.
This study found that AT and MT significantly decreased cancer-related symptom severity across multiple oncology clinics. The results show that AT was effective at decreasing both pain and stress, closely followed by neuropathy. MT was effective at decreasing stress more than any other symptom. Furthermore, the current state of Aurora's 19 Cancer Care locations, 18 clinics with IO therapies, and since the Oncological Multisite Massage and Acupuncture Therapy (OMMAT) study, integrative medicine team members now utilize smart chart templates within the electronic medical record. This allows clinicians to follow patients who receive medical treatment from multiple providers and locations. Similarly, the patient's primary medical team can access information regarding the patient's integrative therapy treatments. Given these findings from the OMMAT study, the continued expansion of the Integrative Cancer Care services at Aurora Cancer Centers, and increased data collection operations, the authors see the value of conducting a larger randomized-controlled trial. In doing so, they further assess the effectiveness of Integrative Cancer Care's OMMAT study for reducing side effects and symptoms throughout cancer diagnosis, treatment, and survivorship across multiple oncology clinics with respect to demographic variables and individual diagnosis, treatment, and survivorship information. Finally, these results demonstrate it is possible to create a multisite program utilizing employed Ats and Mts from Aurora's Integrative Medicine Department. Therefore, the results of this study support the continuation and growth of the integrative cancer care program.
Footnotes
Acknowledgments
The authors acknowledge clinical leaders Scott Feist, Manager of Aurora Integrative Medicine, and Andrea Dinauer, Supervisor of Massage Therapy. They also acknowledge Sajid Masoud for data collection oversight, as well as all of the dedicated massage therapists, acupuncturists, oncology supervisors, nurses, and department/clinic support staff.
Author Disclosure Statement
All authors listed on this quality brief have no conflicts of interest to disclose. In addition, this research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. All authors wish to report no financial disclosures.
Funding Information
No funding was received for this article.