
Abstract
Objectives:
Traditional Chinese medicine (TCM) has been shown to reduce insulin resistance and improve beta cell function in previous studies. The aim of this study was to assess whether the use of TCM can delay the need for insulin therapy in patients with type 2 diabetes.
Design:
Data on patients with type 2 diabetes who received medical treatment for the first time between 2000 and 2003 were obtained from National Health Insurance Research Database (NHIRD) in Taiwan. Among these patients, those with a cumulative use of TCM of more than 28 days were defined as TCM users, and the others as non-users. Kaplan-Meier analysis was used to evaluate the cumulative risk of initiating insulin therapy. Cox proportional hazards models with and without competing risk events were used to evaluate the association between the use of TCM and insulin therapy.
Settings/Location:
Data were obtained from National Health Insurance Research Database (NHIRD) in Taiwan.
Subjects:
Patients with type 2 diabetes who received medical treatment for the first time between 2000 and 2003.
Interventions:
Among these patients, those with a cumulative use of TCM of more than 28 days were defined as TCM users, and the others as non-users.
Outcome measures:
After 1:1 propensity score matching, both groups were tracked until the initiation of insulin therapy, death, or the end of 2013.
Results:
We identified 6524 TCM users and 6524 non-users. The TCM users had a significantly lower risk of insulin initiation in a dose-dependent manner (log-rank test p < 0.001). This effect was consistent across subgroups with different severities of diabetes, and remained significant in competing risk analysis (for TCM users with 28 to 83 days cumulative use, HR 0.78 [0.70–0.87], p < 0.0001; for TCM users with ≥ 84 days cumulative use, HR 0.47 [0.42–0.53], p < 0.0001).
Conclusions:
The use of TCM in addition to standard diabetes treatment may delay the need for insulin treatment in patients who received medical treatment for type 2 diabetes for the first time. This benefit was strongly dose-dependent and applicable in patients with different severities of diabetes.
Introduction
Diabetes mellitus is an important public health issue. According to the International Diabetes Federation, the number of people with diabetes worldwide was 425 million in 2017 and will increase to 629 million in 2045. 1 Because of the pathophysiology, namely insulin resistance and eventually β cell failure, patients with type 2 diabetes inevitably need insulin replacement as the disease progresses. In a prior Swedish cohort study, 25% of patients with type 2 diabetes were prescribed with insulin within 6 years and 42% within 10 years of study enrollment. 2
Despite the safety and effectiveness of insulin treatment, patients may be concerned over injections and weight gain. Fortunately, newly developed oral antidiabetic drugs (OADs) such as dipeptidyl peptidase-4 (DPP-4) inhibitors 3 and sodium-glucose cotransporter-2 inhibitors 4 have been demonstrated to preserve β cell function and reduce insulin resistance in rodent models without weight gain 3 or even with weight loss. 4 In addition, second-line treatment after metformin, including thiazolidinediones 5 and DPP-4 inhibitors, 6 has also been associated with less insulin initiation compared with sulfonylurea in several cohort studies. Moreover, thiazolidinedione has been shown to reduce visceral fat 7 and DPP-4 inhibitors have been shown to be weight neutral in patients with type 2 diabetes. 8
In Traditional Chinese Medicine (TCM), diabetes mellitus is described as Xiaoke, which means increased thirst. In the Yellow Emperor's Internal Classics, which is classic TCM literature written 2000 years ago, Xiaoke was linked to an unhealthy diet, obesity, emotional disorders, and weakness in the five organs. 9 The main concept of diabetes treatment in TCM is nourishment, and that it should be individualized based on the symptoms and body constitution. More recent research has revealed the underlying mechanisms of the glucose-lowering effect of several TCM ingredients. For example, Radix Astragali can alleviate glucose toxicity and increase insulin sensitivity, 10 and Salvia miltiorrhiza can reduce oxidative stress and attenuate insulin resistance. 11 In addition, previous observational cohort studies have also shown long-term benefits of TCM use in reducing diabetic complications 12 and the risk of kidney failure among patients with type 2 diabetes. 13 However, no research has investigated the use of TCM and the timing of insulin initiation.
Therefore, the aim of this study was to investigate whether the use of TCM in addition to standard diabetes treatment can delay the initiation of insulin therapy. In addition, associated risk factors of insulin initiation were also analyzed.
Materials and Methods
Data resources
The data used in this population-based cohort study were obtained from the National Health Insurance Research Database (NHIRD), Taiwan. The National Health Insurance (NHI) program was launched in Taiwan on March 1, 1995. The NHI program is a single payer insurance program that covered 99.9% of the population in Taiwan by the end of 2014. 14 The NHIRD contains original claims data and registration files from the NHI program, and is maintained by the National Health Insurance Administration, Ministry of Health and Welfare, Taiwan, for the purpose of scientific research. 14 It has been used in previous studies of TCM. 12,13 The Institutional Review Board (IRB) of Chang Gung Medical Foundation approved this study (IRB No. 201801469B0C501).
Study cohort and case subjects
The study cohort was obtained from the Longitudinal Health Insurance Database 2005 (LHID 2005), a subset database of the NHIRD. The LHID 2005 contains all original claims data from 1 million randomly sampled individuals from ∼25.68 million beneficiaries in 2005. There is no significant difference in sex distribution between individuals in the LHID 2005 and NHIRD. 14 Patients with type 2 diabetes mellitus were selected who initiated medical treatment between 2000 and 2003 as the study cohort. The initiation of medical treatment was defined as the cumulative use of OADs (Anatomical Therapeutic Chemical, ATC code: A10B) ≥28 defined daily dose (DDD). The ATC/DDD system was established by the World Health Organization and serves as a useful tool to monitor drug use and for research. 15 The DDD is the supposed average daily maintenance dose for a drug used for its main indication in adults. Subjects <18 years or with end-stage renal disease (International Classification of Diseases 9th Revision, Clinical Modification [ICD-9-CM] code 585.6) were excluded.
Information of TCM prescriptions was acquired from outpatient and inpatient department claims data in the NHIRD. Subjects in the study cohort with ≥28 days cumulative use of TCM before insulin initiation were defined as TCM users, and the remaining patients were defined as TCM nonusers. The characteristics of the TCM users and nonusers were documented, including age, sex, urbanization level of residency, income, adapted diabetes complication severity index (aDCSI), comorbidities, and classes of OADs used. The DCSI consists of selected laboratory data and diagnosed diabetic complications including macrovascular and microvascular diseases, and metabolic parameters. It has been shown to perform better than complication count in predicting mortality and the risk of hospitalization. 16 The aDCSI, which excludes laboratory data, has been validated in claims data and has been reported to be a similarly good measure of the severity of diabetes as the DCSI. 17 Comorbidities that could possibly limit the use of OADs, including chronic liver disease and cirrhosis (ICD-9-CM 571) and chronic kidney disease (ICD-9-CM 585), were recorded. Classes of OADs available in Taiwan included metformin (ATC code: A10BA), sulfonylureas (ATC code: A10BB), α-glucosidase inhibitors (ATC code: A10BF), thiazolidinediones (ATC code: A10BG), DPP-4 inhibitors (ATC code: A10BH), and meglitinides (ATC code: A10BX02, A10BX03, and A10BX08). Fixed-dose combinations (ATC code: A10BD) were categorized into the aforementioned classes according to their components. Propensity score matching of the TCM users and nonusers was done, used 1:1 matching of each cohort by sex, age, urbanization level, income, aDCSI, comorbidity, and antidiabetic agents. The flowchart of study population selection and matching by propensity score is shown in Figure 1.
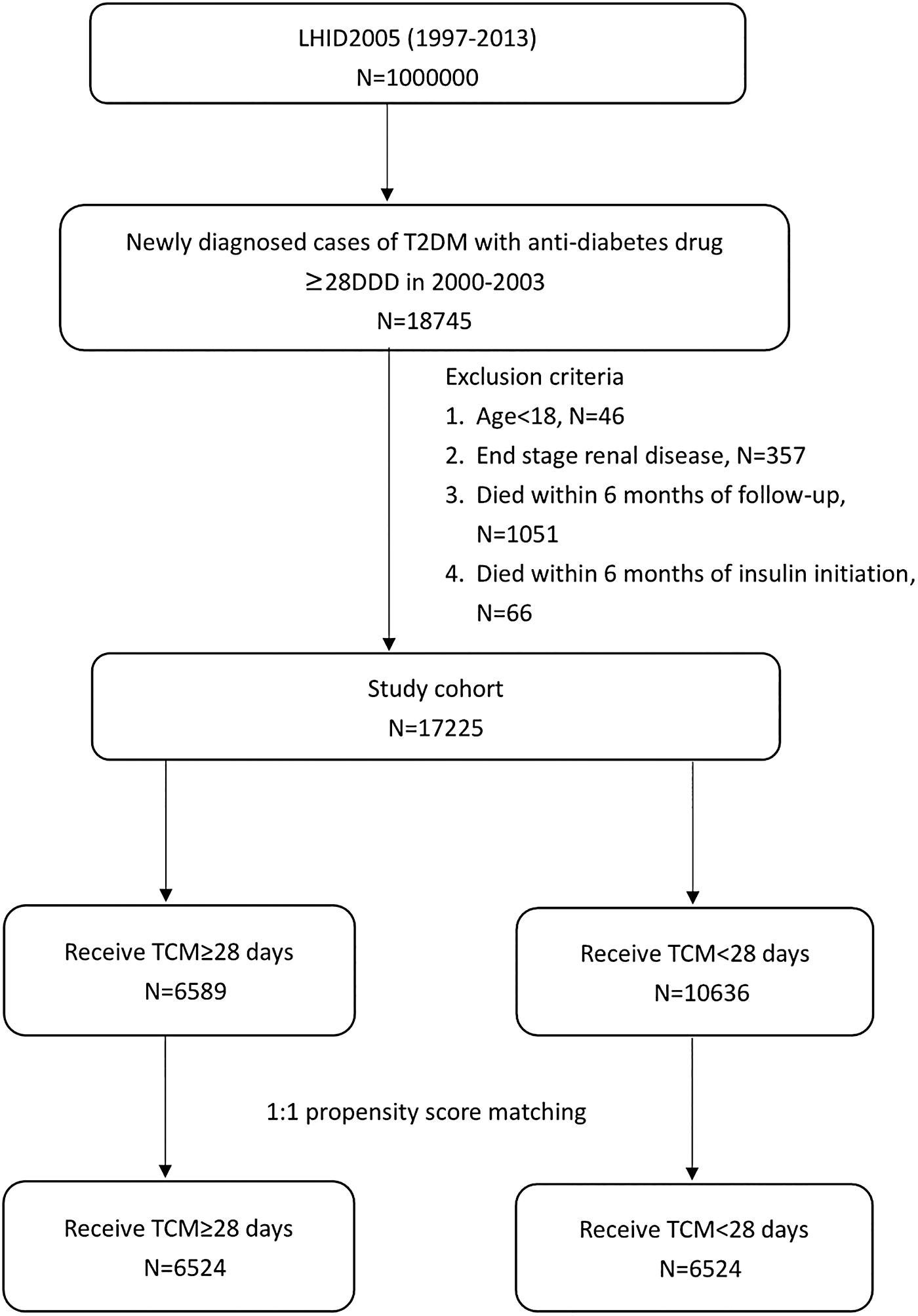
Flowchart of study population selection and matching by propensity score. LHID, Longitudinal Health Insurance Database; T2DM, type 2 diabetes mellitus; TCM, Traditional Chinese Medicine.
Endpoints
The endpoint of this study, insulin initiation, was tracked from the first prescription of a TCM (TCM users) or OAD (TCM nonusers) until the end of 2013 or death. Insulin initiation was defined as insulin prescriptions (ATC code: A10A) for cumulative ≥84 DDD to exclude the patients who needed temporary insulin rescue therapy for hyperglycemic crisis due to acute illness or poor adherence to OADs. Because of the progressive nature of type 2 diabetes mellitus, insulin secretory function decreases over time. 18 Thus, long-term insulin replacement therapy represents β cell failure as well as oral antidiabetic treatment failure. Although early intensive insulin treatment has been reported to preserve β cell function, most studies have had a short duration (14–21 days) and were conducted after 2004, a few years after study enrollment. 19 Patients who died within 6 months of follow-up and within 6 months of insulin initiation were also excluded because these cases were probably associated with critical illnesses.
Statistical analysis
The distribution of demographic factors and the proportions of comorbidities between the TCM users and nonusers were compared. Cox proportional hazards models were used to compute hazard ratios (HRs) with confidence intervals (95% CIs). Since insulin therapy could also be confounded by the competing risk of mortality, Cox proportional hazards analysis was also performed with competing risk events to examine whether the outcomes were consistent. Subgroup analyses stratified by aDCSI were also performed to test the outcomes with different severities of diabetes. All analyses were conducted using SAS statistical software (version 9.4; SAS Institute, Cary, NC).
Results
Characteristics of the TCM users and nonusers
A total of 17,225 patients with type 2 diabetes mellitus who initiated medical treatment between 2000 and 2003 were identified, among whom there were 6589 TCM users (Table 1). After 1:1 propensity score matching, 6524 TCM users and 6524 nonusers were included in final analysis (Fig. 1). There were no significant between-group differences in sex, age, urbanization level, income, aDCSI, comorbidity, and antidiabetic agents use. In addition, the TCM users had a lower mortality rate before insulin initiation (7.76% vs. 9.47%, p = 0.0005) (Table 1).
Characteristics of the Traditional Chinese Medicine Users and Nonusers
aDCSI, adapted diabetes complication severity index; CLD, chronic liver disease; DPP-4, dipeptidyl peptidase-4; NTD, new Taiwan dollars; TCM, Traditional Chinese Medicine.
Time to insulin initiation analysis
Kaplan–Meier analysis showed that the TCM users had a lower incidence of insulin initiation than the nonusers during the follow-up period (log-rank test p < 0.001) (Fig. 2A). The 5- and 10-year rates of insulin initiation in the two groups were 6.24% versus 13.75% and 11.64% versus 20.80%, respectively. The TCM users with a higher cumulative use of TCM (≥84 days) had a lower incidence of insulin initiation than the TCM users with 28–83 cumulative days (log-rank test p < 0.001) (Fig. 2B).
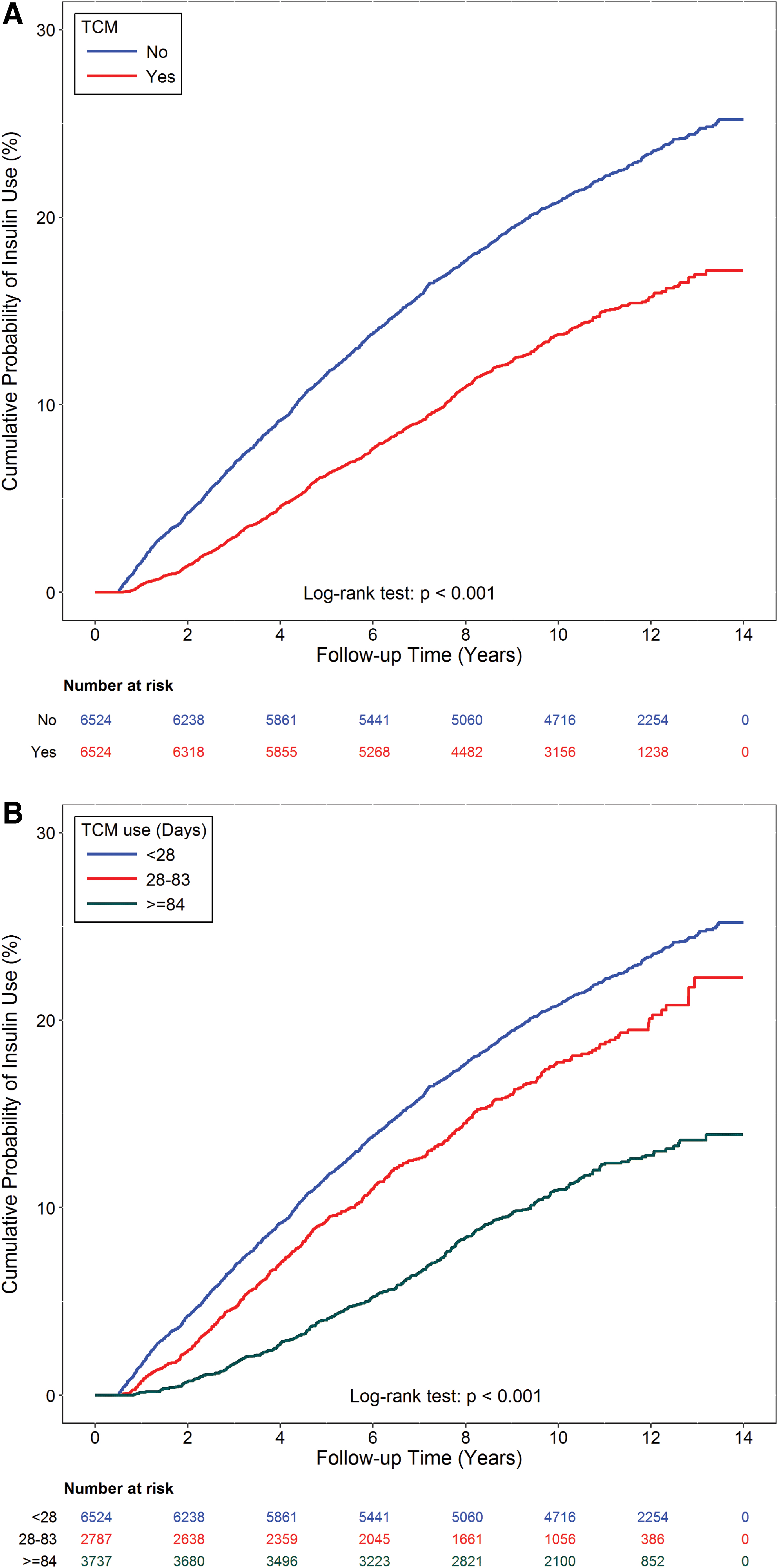
Kaplan–Meier curves with differences in cumulative incidence of insulin initiation between TCM users and non-TCM users
Risk of insulin initiation in subgroups of different severities of diabetes
Across subgroups of different severities of diabetes (aDCSI: 0, 1, and ≥2), the use of TCM between 28 and 83 days was associated with a lower risk of insulin initiation except for the aDCSI ≥2 group. However, a higher cumulative use (≥84 days) was consistently associated with an even lower risk of insulin initiation in all subgroups (all p < 0.05) (Table 2).
Risk of Insulin Initiation in Subgroups of Different Severities of Diabetes
The models were adjusted for all covariates (sex, age, urbanization, income, comorbidities, and antidiabetic agent).
aDCSI, adapted diabetes complication severity index; CI, confidence interval; HR, hazard ratio; TCM, Traditional Chinese Medicine.
Competing risk analysis
Competing risk analysis of different TCM exposure subgroups showed that a higher cumulative number of days of TCM use remained inversely proportional to insulin initiation before and after adjusting for all covariates (all p < 0.0001) (Table 3).
Competing Risk Analysis of Subgroups with Different Cumulative Days of Traditional Chinese Medicine Use
Adjusted for all covariates (sex, age, urbanization, income, aDCSI, comorbidities, and antidiabetic agent).
aDCSI, adapted diabetes complication severity index; CI, confidence interval; HR, hazard ratio; TCM, Traditional Chinese Medicine.
Most commonly used TCM in all TCM users
The five most commonly used single-herb products were Dan shen, Yan hu suo, Ge gen, Bei mu, and Tian hua fen, and the five most commonly used multiherb products were Shu jing huo xue tang, Liu wei di huang wan, Shao yao gan cao tang, Ping wei san, and Jia wei xiao yao san (Table 4).
Most Commonly Used Traditional Chinese Medicine in All Traditional Chinese Medicine Users (N = 6589)
TCM, Traditional Chinese Medicine.
Discussion
To the best of the authors' knowledge, this nationwide population-based cohort study is the first study to demonstrate that the use of TCM could significantly delay the time to insulin initiation in a dose-dependent manner in patients who receive medical treatment for the first time for type 2 diabetes. This effect was also consistent in patients with different severities of diabetes and remained significant in competing risk analysis.
In a retrospective cohort study, sitagliptin, a DPP-4 inhibitor, was shown to reduce the risk of insulin initiation compared with sulfonylureas as a second-line therapy after metformin, and that this benefit of DPP-4 inhibitors resulted from the preservation of β cell function. 6 Another similar study also showed that thiazolidinediones, an insulin sensitizer, could delay the need for insulin treatment compared with sulfonylureas after metformin use. 5 An increasing amount of research has been conducted on the antidiabetic mechanisms of several TCM ingredients. For example, berberine of Rhizoma coptidis has been shown to activate the adenosine monophosphate-activated protein kinase (AMPK) pathway and enhance insulin receptor expression in a manner similar to metformin. 20 In addition, Astragalus polysaccharides have been shown to alleviate glucose toxicity and restore glucose homeostasis in animal models by increasing insulin sensitivity. 10 Moreover, the combination of Rehmanniae radix, Ginseng radix, and Scutellariae radix has been shown to promote β cell proliferation through the induction of insulin receptor substrate 2. 21 Even if these ingredients have been shown to possess possible mechanisms of delaying insulin initiation and are commonly used to treat diabetes in Taiwan 22 and China, 23 the prescription patterns vary widely. Moreover, these ingredients are not only used to treat diabetes, but also other ailments in daily practice.
TCM views the human body in a holistic way, and looks at patterns of disharmony instead of seeking causative factors for a particular disease as in Western medicine. The essence of TCM is to differentiate symptoms through history taking, observation of the tongue and face, smelling of the breath and body, and palpation of pulse. The signs and symptoms of patients are categorized according to the concept of dualism and the eight principles of diagnosis—yin or yang, interior or exterior, cold or heat, and deficiency or excess. 24 In traditional TCM, the core pathogenesis of Xiaoke (diabetes mellitus) includes yin deficiency and dryness heat, which induces excess thirst, hunger, urination, and weight loss. Thus, classical treatment includes qi invigoration, yin nourishment, heat clearance, and stasis reduction. 23 However, a recent study reported that most patients with type 2 diabetes mellitus do not have these typical symptoms at presentation, and that the syndrome changes with the clinical stage of diabetes, from qi stagnation initially to excess heat in the stomach and intestine, and finally dual deficiency of qi and yin. 25 Hence, the prescription should be adjusted according to the clinical presentations, thus resulting in the great diversity in the prescription pattern. Even the patients came for diseases other than diabetes; the syndrome differentiation would guide the prescription, not the diseases. Thus, TCM was regarded as a whole rather than analyzing the effect of specific formulae of TCM.
It was found that the TCM users had a significantly lower mortality rate before insulin initiation than the nonusers, even though the TCM users were followed from the first prescription of TCM, which probably indicates a later stage of diabetes. This finding could also support that the lower insulin initiation rate in the TCM users was not due to a reluctance to receive insulin injections, which may have worsened blood glucose control. Although the NHIRD does not include laboratory data, a previous study revealed that higher glycated hemoglobin, meaning poorer control of diabetes, was associated with a higher mortality rate. 26 Moreover, some commonly used antidiabetic TCM ingredients have been reported to benefit metabolic syndrome. In a meta-analysis, berberine was shown to reduce the level of low-density lipoprotein cholesterol, raise the level of high-density lipoprotein cholesterol, and lower blood pressure. 27 Rehmanniae radix has also been reported to have anti-inflammatory and antihypertensive effects in Korean studies. 28 These benefits could have led to a lower risk of cardiovascular diseases and hence the lower risk of mortality in the TCM users in this study.
Because of the retrospective database design, this study had some limitations. First, the NHIRD does not contain biochemistry data or the medical histories of the patients, including personal history, family history, clinical symptoms, the duration of diabetes, and glycated hemoglobin data. Clinical physicians may initiate insulin replacement therapy according to different criteria. In addition, the patients may have initiated insulin therapy earlier because of intolerance to certain classes of OADs or due to their willingness. However, the incidence of these conditions was expected to be similar in both groups, and HRs were used to eliminate these possible biases. Second, data on the drug adherence rate in the TCM group were unavailable. It is unlikely that every patient in the TCM group took all prescribed TCM without loss. Thus, the benefits of TCM in this study were probably underestimated. Third, complementary and alternative medicine users tend to be more aware of their health. 29 Although it is well known that lifestyle modifications and weight reduction are the basis of glycemic control, 30 neither data on body mass index or changes in diet and physical activity are available in the NHIRD. From this point of view, the advantages of TCM may have been overestimated. Fourth, in the NHI claims data, it could not be excluded that patients may have taken self-paid TCM or antidiabetic agents by themselves. Nevertheless, the copayment of each clinic visit is relatively cheap under the NHI program (∼1.5 to 5 U.S. dollars), and, therefore, it is unlikely that patients would purchase TCM without prescriptions. Finally, there were still some residual confounders that could affect insulin initiation in patients with type 2 diabetes, such as baseline β cell function and insulin sensitivity. Further well-controlled prospective human studies are needed to clarify this issue. Despite these limitations, the strengths of this study include its large nationwide cohort and long follow-up period.
Conclusions
In conclusion, the use of TCM in addition to standard diabetes care may delay the need for insulin therapy in the patients who started medical treatment for type 2 diabetes. This benefit was strongly dose dependent and applicable in patients with different severities of diabetes. Further studies are needed to clarify the possible survival benefits of TCM.
Footnotes
Acknowledgment
The authors thank the Health Information and Epidemiology Laboratory of Chang Gung Memorial Hospital, Chiayi Branch (CLRPG6G0042), for its comments and assistance in data analysis.
Author Disclosure Statement
No competing financial interests exist
Funding Information
This study was supported by a grant from Chang Gung Memorial Hospital, Chiayi Branch, and based on the National Health Insurance Research Database provided by the Central Bureau of National Health Insurance, the Department of Health, and managed by the National Health Research Institutes. The interpretation and conclusions contained herein do not represent those of the Bureau of National Health Insurance, Department of Health, or National Health Research Institutes.