
Abstract
Background:
Fire needle therapy is a method of quickly piercing into acupoints with red-hot needles to treat diseases. Recently, multiple studies have reported that fire needle therapy is effective in the treatment of psoriasis; however, there are few articles systematically evaluating the effect of this therapy. Therefore, this systematic and meta-analysis study is conducted to estimate the efficacy and safety of fire needle therapy for psoriasis.
Methods:
PubMed, Embase, CNKI, VIP, CBM, CENTRAL, and Wan Fang databases were systematically searched from the dates of construction of these databases to August 24, 2019, and randomized controlled trials assessing patients with psoriasis who were treated with fire needle therapy alone or in combination with other drugs were also evaluated.
Results:
Fire needle therapy was effective in treating psoriasis (p = 0.0002; risk ratio [RR], 1.20; 95% confidence interval [CI], 1.09–1.33) with a lower recurrence rate (p = 0.005; RR, 0.48; 95% CI, 0.29–0.80). Adverse events after fire needle treatment were similar to those without fire needle treatment (p = 0.38; RR, 0.67; 95% CI, 0.28–1.63). After fire needle treatment, the number of cluster of differentiation (CD)8+T cells, type 1 helper cells, interleukin (IL)-2, and interferon (IFN)-γ decreased, whereas the number of CD4+T cells, type 2 helper cells, IL-4, IL-10, and the proportion of CD4+T cells and CD8+T cells increased.
Conclusions:
Fire needle therapy, specifically in combination with oral medicines, is effective in treating patients with psoriasis with low recurrence rates.
Introduction
Psoriasis is a chronic inflammatory skin disease, which results from the interaction between genetics and the environment, and is mediated by immunity. There are five types of psoriasis, including plaque psoriasis, guttate (droplet) or eruptive psoriasis, inverse psoriasis, pustular psoriasis, and erythrodermic psoriasis. 1 The main clinical manifestations of psoriasis are red papules or plaques, covered with multiple layers of silvery-white scales. 2
Psoriasis is observed in people of all ages. A World Health Organization global report 3 indicated that the prevalence of psoriasis ranged from 0.09% in the United Republic of Tanzania 4 to 11.4% in Norway, 5 making psoriasis a global problem that plagues ∼100 million people worldwide. In China, the prevalence of psoriasis increased from 0.123% in 19846 to 0.47% in 2012. 7 The Global Burden of Disease Study in 2010 demonstrated the high burden of psoriasis, 8 comprising disease severity, skin symptoms, physical and psychological complications, quality of life, and medical expenses. 9 Among them, psoriasis-related complications include coronary heart disease, metabolic syndrome, 10 chronic obstructive pulmonary disease, 11 cardiovascular disease, 12 hyperuricemia, 13 and so on.
The American Academy of Dermatology recommends five options for treating psoriasis, including classic systemic therapy, biologics, topical therapy, phototherapy, and photochemotherapy. 14 However, considering the evident toxicities, side effects, and high economic costs of these treatments, patients with psoriasis are discouraged to receive these types of treatments. Although phototherapy is cost-effective, the lack of equipment in some medical institutions limits its application. Hence, several clinicians and researchers have been searching for better treatment options, including fish oil, 15 and moving cupping therapy. 16
Fire acupuncture has a long history in the treatment of psoriasis and is widely used in clinics. Fire needle therapy is considered as a characteristic Chinese medicine therapy, according to the Chinese guidelines for diagnosis and treatment of psoriasis (2018 simplified version). 17 Different from ordinary acupuncture, fire needle therapy is a method of quickly piercing into acupoints with red-hot needles to treat diseases. Attention should be paid to disinfection before acupuncture, and the depth of acupuncture should be determined according to the condition of the disease, patients' physique and age, and muscle thickness and vascular depth of acupuncture points. In fire needle therapy, pulling out quickly after inserting the needle, and pressing the pinhole with cotton balls to reduce pain should be considered. Analogous to other acupuncture schemes, when a patient is hungry, in pain, unwell, or nervous during fire needle treatment, it can lead to a loss of consciousness and mobility for a short period of time. This is known as fainting during acupuncture treatment. 18 The operator should pay close attention to the patient's status. If discomfort or even syncope is observed, the operator should immediately stop the treatment and take the necessary treatment measures. At present, some medical institutions are investigating the use of topical anesthesia followed by fire needle therapy to relieve pain and improve treatment compliance, including compound lidocaine cream and capsaicin ointment. 19 –21 The fire needle needs to be heated using the alcohol lamp and subsequently penetrates into the skin lesion. Thus, a microscald reaction is observed. Microscalding reactions will easily cause infection if not handled properly. Therefore, patients should avoid scratching and bathing immediately after treatment.
At present, fire needle therapy is used to treat moderate-severe acne 22 and nodular prurigo. 23 Several literatures also show that fire needle therapy has beneficial effects in the treatment of psoriasis with less side effects and a low recurrence rate, 24 and some articles pay attention to the immune mechanism of fire needle therapy in the treatment of diseases. 25 –27 Considering that there is no systematic evaluation of fire needle therapy for psoriasis, a systematic review and meta-analysis is conducted to evaluate the effectiveness and safety of acupuncture treatment for psoriasis.
Experimental Section
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISM) statement (Supplementary Table S1). 28 Furthermore, this title has been registered in the Joanna Briggs Institute (JBI).
Data sources and search strategy
Seven databases, including PubMed, Embase, CNKI, VIP, CBM, CENTRAL, and Wan Fang, were searched for literature published from the dates of construction of these databases to August 24, 2019. In the computer-based retrieval, the combination of subject words and free words was used for search. These terms mainly included “psoriasis,” “fire needle,” “fire needle therapy,” and “randomized controlled trial.” After removing duplications, two reviewers independently (X.C. and Y.L.) screened titles and abstracts of all literatures based on the inclusion criteria. The Chinese Clinical Trial Registry (
Study selection and eligibility criteria
Randomized controlled trials (RCT) were eligible in this meta-analysis, and were used to assess the effects of fire needle therapy alone, as well as of a combination of fire needle therapy and other medications for the intervention group, such as fire needle therapy and fire needle therapy plus oral/external Chinese medicine or plus oral/external western medicine. For the control group, characteristic therapy of Traditional Chinese Medicine (TCM) and oral/external Chinese medicine or oral/external western medicine was included. In addition, articles using Psoriasis Area and Severity Index (PASI) as the main outcome indicators were included. Patients' age ranged between 18 and 70 years, regardless of sex, except for pregnant and lactating women. The inclusion criteria were as follows: patients without heart, brain, kidney, liver, gallbladder, gastrointestinal, or other biomedical diseases, patients who did not receive systematic treatment of psoriasis in the past month, and patients who voluntarily participated and provided informed consent.
Outcomes
PASI is a commonly used tool for measuring the area and severity of skin lesions in patients with psoriasis. The evaluation of the efficacy of fire acupuncture treatment of psoriasis was mainly based on the cured and markedly effective and improved rate of PASI. In addition, TCM syndrome scores, the incidence of adverse events, quality of life score, Hamilton Anxiety Rating Scale (HAM-A) score, and recurrence rate were used as the secondary outcome indicators of this study. Finally, the changes of inflammatory cells and cytokines were summarized and analyzed to provide evidence for the mechanism research.
Data extraction and risk-of-bias assessment
Two authors (X.C. and Y.L.) separately screened the title, abstract, and full text in each study. First author, publication date, sample size, psoriasis type, TCM syndrome, course of disease, interventions, outcomes, and untoward effects were extracted. If the opinions were not uniform, the authors reached a consensus through consultation.
Two reviewers (M.X. and J-K. S.) assessed the quality of studies independently. If the two reviewers disagreed on the results, another person (Y.R.) participated in the evaluation to reach an agreement. The Cochrane risk-of-bias tool 29 was applied to assess the risk of bias of all involved trials.
Statistical analysis
Revman 5.3 analyses were performed to calculate the risk ratio (RR), continuous outcomes, and mean differences (MDs) with 95% confidence intervals (CIs). For the dichotomous variables, RRs with 95% CI were determined to describe findings. I 2 was used to indicate heterogeneity. If p was >0.1 and I 2 was <50%, there was homogeneity, and a fixed model was applied. Otherwise, it was heterogeneous, and a randomized model was used. At this time, subgroup analysis was applied.
Results
Study identification and selection
Eighty-nine relevant citations were identified. After removing duplicate studies, 45 literatures were selected from those initially identified. Subsequently, the titles and abstracts of each study were screened, and 33 articles remained for detailed evaluation. Of those, one was a duplicate of a previous study, and the other was a systematic review. Seven were nonrandomized controlled trials, and the other eight were not relevant to our study. Ultimately, 16 trials 30 –45 met the criteria and were included in this review. The comprehensive details of these trials are presented in Figure 1.
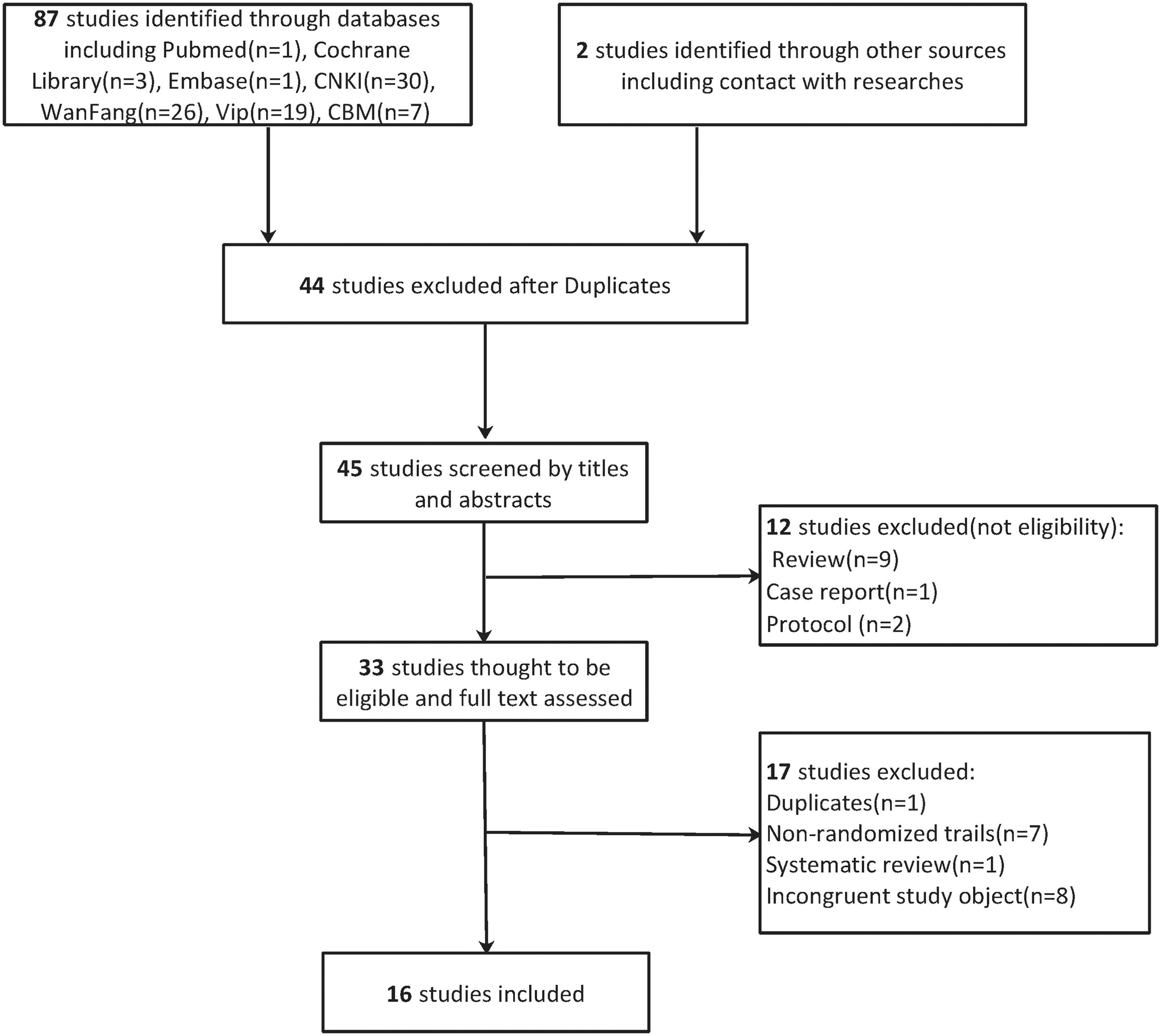
Flow chart of search strategy and study selection, according to PRISMA guidelines. PRISM, Preferred Reporting Items for Systematic Reviews and Meta-analyses.
Characteristics of included studies
Sixteen trials involving 1267 participants were included in the analysis. Nine clinical studies 30,31,36,38 –41,43,44 used fire needles to treat psoriasis vulgaris, six 32,34,35,37,42,45 used fire needles to treat plaque psoriasis, and one 33 used fire needles to treat erythrodermic psoriasis. Of the trials selected that used Chinese medicine syndrome concepts, one used fire needles to treat blood dryness, 32 one to treat blood heat, 40 and nine to treat blood stasis syndrome. 30,32,35 –39,42,44 Currently, there is no clear definition to completely match the biomedical categories with Chinese medicine categories. However, fire needle therapy is commonly used to treat blood stasis syndrome of psoriasis vulgaris (including drip psoriasis and plaque psoriasis) in clinical practice. Two trials 37,45 were multicenter clinical trials conducted in three hospitals in China.
Four types of treatments, including treatment with fire needle only, 30 –32,34 fire needle plus oral medication, 33,36,41,43,44 such as acitretin capsule and compound glycyrrhizin tablets; fire needle plus oral and topical medication, 35,37 –39,42,45 such as calcipotriol cream and tazarotene cream; and fire needle plus Chinese herbal medicine and Chinese patent medicine, 40 the efficacy of which was mainly based on clear heat used to remove toxicity and activate blood and resolve stasis, were used in the included trials. Notably, except for one study 33 using fire needles combined with western medicine, other oral medicines were Chinese herbal medicines. 36,41,43,44
Eleven studies 30,31,35 –37,39–42,45 reported the primary outcome and PASI scores, and the other five 32 –34,38,44 studies described only comprehensive efficacy calculated based on the PASI scores, as PASI scores after treatment were not reported. In addition, Dermatology Life Quality Index (DLQI) score, HAM-A score, TCM syndrome score, T cells, and inflammatory cytokines were reported in some studies. Full details are presented in Table 1.
Characteristic of Encountered Trials
AE, adverse events; BDS, blood dryness syndrome; BHS, blood heat syndrome; BSS, blood stasis syndrome; C, control; CHM, Chinese herbal medicine; CPD, Chinese patent drug; DLQI, Dermatology Life Quality Index; HAM-A, Hamilton Anxiety Rating Scale; I, interventions; IFN, interferon; IL, interleukin; OM, oral medication; PASI, Psoriasis Area and Severity Index; RER, recurrence rate; SD, standard deviation; SF-36, 36-item Short Form Health Survey; TCM, Traditional Chinese Medicine; TCMSS, TCM syndrome score; TO, topical ointment; VEGF, vascular endothelial growth factor.
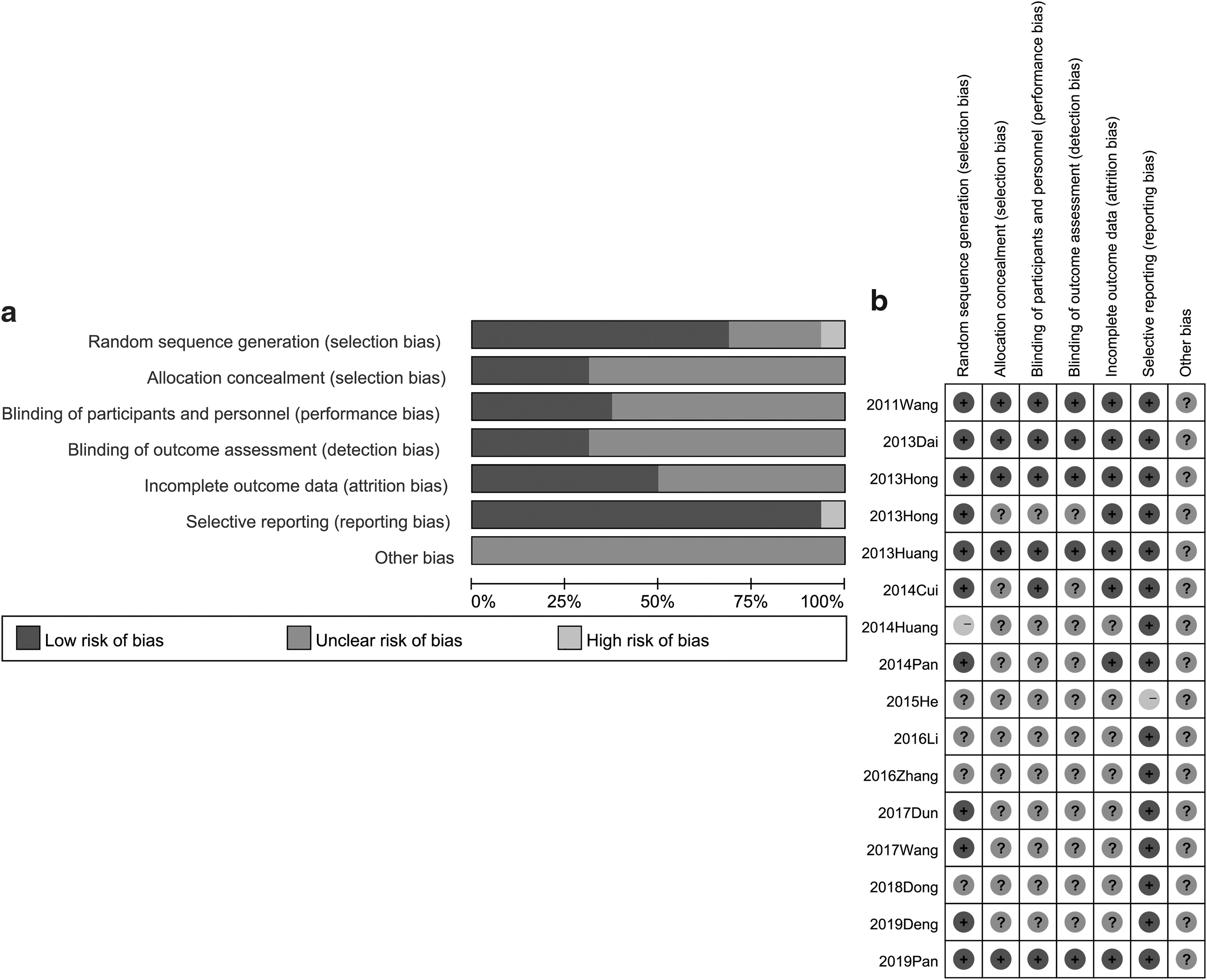
Risk-of-bias assessment
Nine articles 30 –32,34,35,41,42,44,45 used computer-generated random numbers to generate random assignments. Two studies used segmental randomization 33 and block randomization, 37 separately. One article 36 was randomly grouped according to the order of patients' visits. The rest of the studies only mentioned the word “randomization.” Five trials 30 –32,34,45 mentioned the method of assigning concealment, including the envelope method and application central randomization system. Due to the particularity of fire needle treatment, six studies 30 –32,34,35,45 were not blinded, and in four of these studies, 30 –32,34 clinical researchers, clinical data collectors, and data statisticians worked independently. The remaining studies did not describe whether blinded methods were used. There were no cases of loss in the three studies. 30,31,33 Six studies 32,34,35,37,39,45 reported cases of loss and causes of loss, of which one described how to deal with missing values, 32 and another used Intention-To-Treat (ITT) analysis. 37 Other studies did not describe specific analysis methods for shedding cases. The remaining trials did not describe whether there were missing cases. DLQI and HAM-A evaluation was planned in the design of one study, 38 but these two indicators have not been reported in the subsequent analysis of results. Details are shown in Figure 2a and b.
Primary outcomes
In this article, each included study applied a PASI score to evaluate efficacy after treatment with fire needle therapy. Only one article reported using fire acupuncture to treat erythrodermic psoriasis so it was excluded in the meta-analysis, which suggested that all patients with psoriasis in the clinical trials included in the analysis had psoriasis vulgaris. In addition, one of the pooled trials only described PASI scores after fire needle therapy, and no comprehensive efficacy was reported. Another study evaluated the efficacy of fire needle therapy combined with Chinese herbal medicine. Therefore, these two studies were excluded from the analysis.
A total of 13 trials were included in the analysis (Table 2 and Supplementary Fig. S1). In general, fire needle therapy was effective in treating psoriasis (p = 0.0002; RR, 1.20; 95% CI, 1.09–1.33). On comparing fire needle therapy with topical treatments of skin lesions (p = 0.11; RR, 1.15; 95% CI, 0.97–1.36) and with the combination of oral and topical medications plus fire needle treatment (p = 0.44; RR, 1.14; 95% CI, 0.82–1.59), the effects were similar with no significant differences. The most effective treatment was fire needle therapy plus oral medications, which was 1.35 times better than treatment with oral medications without fire needle therapy (p = 0.0001; RR, 1.35; 95% CI, 1.16–1.57). The efficacy of the combination of fire needle therapy and Chinese herbal medicine reported by Zhang et al. was also better than that of Chinese patent medicine alone (p < 0.05). Fire needle therapy combined with oral medication for erythrodermic psoriasis was also shown to achieve satisfactory results. 40
Meta-Analysis of the Overall Effect of Fire Needle Therapy on Psoriasis Patients
CI, confidence interval.
Considering that 10 trials reported PASI scores, the clinical efficacy of fire needle therapy in the treatment of psoriasis was also analyzed from the perspective of the PASI score (Table 3 and Supplementary Fig. S2). Similar to the results of the cured and markedly effective rate analysis, the clinical effects of fire needle therapy were better than those of other interventions (p = 0.003; MD, −1.32; 95% CI, −2.19 to −0.44). However, the risk of increased PASI scores was lower after fire needle therapy was used in combination with internal and external medications to treat patients with psoriasis (p < 0.00001; MD, −0.53; 95% CI, −0.72 to −0.33).
Meta-Analysis of Psoriasis Area and Severity Index Scores After Fire Needle Therapy on Psoriasis Patients
Secondary outcomes
TCM syndrome scores
Six trials 35,37 –39,42,45 used TCM syndrome scores to assess the improvement of TCM syndromes in patients with psoriasis. A meta-analysis assessed whether the color of the skin lesions (p = 0.03; MD, −1.20; 95% CI, −2.32 to −0.09), the degree of skin lesion infiltration (p = 0.002; MD, −0.38; 95% CI, −0.62 to −0.13), or the condition of scaly dry skin (p < 0.00001; MD, −0.70; 95% CI, −0.96 to −0.44) was improved after treatment with fire needle therapy (Table 4 and Supplementary Fig. S3). He et al. 38 evaluated the comprehensive scores of TCM syndrome in patients with psoriasis after fire needle treatment, and found that the effective rate after treatment with fire needle therapy (81.5%) was significantly higher than that of the control group (66.6%, p < 0.05), which was the same as the results of Pan et al. 45
Traditional Chinese Medicine Syndrome Scores of Clinical Efficiency of Fire Needle Therapy in the Treatment of Psoriasis
Adverse events
Ten trials 30 –37,39,45 estimated the adverse events of fire needle therapy when treating individuals with psoriasis. Two studies 33,36 found no adverse events in either the experimental or the control group. Li 39 only described one case of adverse reactions in the control group but did not indicate the specific type of adverse event. In the remaining studies describing adverse events, a meta-analysis showed that, overall, the incidence of side effects after fire needle treatment was similar to that without fire needle treatment (p = 0.38; RR, 0.67; 95% CI, 0.28–1.63) (Table 5 and Supplementary Fig. S4). Regarding anaphylaxis, the control group had increased incidence of anaphylaxis (p = 0.04; RR, 0.21; 95% CI, 0.05–0.95).
Meta-Analysis of Adverse Events of Fire Needle Therapy
Quality of life
Four trials 35,37,39,45 evaluated the quality of life after treatment with fire needle therapy. One of the studies used the 36-item Short Form Health Survey Index, and the other studies used DLQI. A meta-analysis showed that the use of fire needle treatment did not significantly ameliorate the quality of life (p = 0.21; MD, −0.44; 95% CI, −1.11 to 0.24) (Table 6 and Supplementary Fig. S5).
Quality of Life and Anxiety of Psoriasis Patients After Fire Needle Treatment
Hamilton Anxiety Rating Scale
Four trials 35,37,39,45 assessed HAM-A after treatment with fire needle therapy. A meta-analysis presented that fire needle treatment did not significantly reduce the anxiety of patients with psoriasis (p = 0.71; MD, −0.16; 95% CI, −0.98 to 0.67) (Table 6 and Supplementary Fig. S6).
Recurrence rate
Two studies 32,34 reported the recurrence rate, and found that patients with psoriasis treated with fire needles had a significantly lower probability of recurrence after the symptoms had improved than those with psoriasis not treated with fire needles (p = 0.005; RR, 0.48; 95% CI, 0.29–0.80) (Table 7 and Supplementary Fig. S7).
Recurrence Rates of Fire Needle Therapy in the Treatment of Psoriasis
Inflammatory cells and cytokines
Four trials 40,41,43,44 examined the subtype of T cells, and two trials 40,44 assessed inflammatory cytokines after treatment with fire needle therapy. It was found that there was no significant difference between the experimental group and the control group as a whole. However, for each subgroup, the number of cluster of differentiation (CD)8+T cells decreased (p < 0.00001; MD, −4.30; 95% CI, −5.70 to −2.90), and the number of CD4+T cells (p < 0.00001; MD, 8.90; 95% CI, 6.41 to 11.39) and the proportion of CD4+T cells and CD8+T cells (p < 0.00001; MD, 0.52; 95% CI, 0.43 to 0.61) increased after fire needle treatment. There were two subgroups of CD4+T cells, namely type 1 helper (Th1) cells and type 2 helper (Th2) cells. After fire needle treatment, the decrease in the number of Th1 cells (p < 0.00001; MD, −0.98; 95% CI, −1.12 to −0.84) was accompanied by a decrease in the number of interleukin (IL)-2 (p < 0.00001; MD, −9.19; 95% CI, −10.46 to −7.74) and interferon (IFN)-γ (p < 0.00001; MD, −21.52; 95% CI, −24.26 to −18.78), which were secreted by Th1 cells and could mediate the inflammatory response. On the contrary, an increase in the number of Th2 cells (p < 0.00001; MD, 0.39; 95% CI, 0.32 to 0.46) was accompanied by an increase in the number of IL-4 (p < 0.00001; MD, 5.13; 95% CI, 3.33 to 6.93) and IL-10 (p < 0.00001; MD, 6.31; 95% CI, 4.43 to 8.19) secreted by Th2 cells, which inhibits the inflammatory response. Vascular endothelial growth factor (VEGF) level decreased after treatment with fire needle therapy (p < 0.00001; MD, −20.78; 95% CI, −26.22 to −15.34). Full details are shown in Table 8 and Supplementary Figures S8 and S9.
T Cell Subsets and Inflammatory Cytokines of Fire Needle Therapy in the Treatment of Psoriasis
CD, cluster of differentiation; Th1, type 1 helper; Th2, type 2 helper.
Discussion
In this analysis, fire needle treatment of psoriasis, specifically in patients with psoriasis vulgaris, improved skin lesions with a low recurrence rate. The conclusions were different when analyzing the cured and markedly effective rate and the PASI score. However, it is certain that the effects of fire needles and external medicines were comparable, and the skin lesions of patients with psoriasis significantly improved after treatment with fire needle therapy plus oral medications. Therefore, a combination of fire needle therapy with oral medications is recommended. However, fire needle therapy does not improve quality of life and anxiety in patients with psoriasis as expected.
Any treatment has side effects, and fire needle therapy is no exception. Fainting during acupuncture treatment is one of the most noteworthy side effects of fire needle therapy for psoriasis. Fortunately, a significant majority of patients in this study did not experience fainting during acupuncture treatment, except for one patient who experienced fainting during the second fire needle treatment, because of significantly little food intake and excessive stress. In this lone case, the doctor immediately stopped the treatment and laid the patient on the treatment bed, and the patient subsequently received moxa-moxibustion therapy on the BaiHui acupoint (GV20) for 2 min. After the patient felt that the fainting subsided, the doctor provided him with boiled sugar water. After the doctor confirmed a normal pulse and blood pressure, the patient agreed to continue treatment. 30 In this meta-analysis, causalgia was observed in the skin lesions of two patients, and infection was observed in four patients after fire needle treatment. These symptoms disappeared after treatment, and these patients consented to continue treatment.
In all involved trials, most researchers applied fire needle therapy to treat blood stasis syndrome of psoriasis and observed positive effects. From the perspective of TCM, the distribution pattern of psoriasis syndrome is based on blood. Among them, blood heat syndrome, blood stasis syndrome, and blood dryness syndrome are the three basic syndrome types. 46 In addition, the pathologic factor, blood stasis, remains through the whole process of psoriasis. 47,48 The formation of blood stasis syndrome is considered to be an abnormality of the blood in the veins, such that the body tissues and organs may not receive sufficient blood perfusion. It is also possible to form systemic or local blood stasis, thereby causing systemic or local metabolic disorders and dysfunction. 47 Currently, a large number of studies 49 have indicated that blood stasis syndrome is closely associated with microcirculatory disorders, hemodynamic abnormalities, platelet activation, vascular endothelial injury, and inflammatory response, which is similar to the pathogenesis of psoriasis. 50 Acupuncture has a positive effect on psoriasis, which can improve blood rheology and microcirculation. 51 Fire needle therapy combines the effects of acupuncture in stimulating meridian qi and moxibustion in warming yang and dispelling cold, which produces a better effect on blood heat syndrome and blood stasis syndrome. 32,36,40 Therefore, in addition to the above effects, it can regulate immunity, sterilize with high temperature, and ameliorate the body's internal environment. 52 These may be the reasons for the low recurrence rate of fire needle treatment of psoriasis.
In all studies reporting the immune response after fire needle therapy, three described the treatment mechanism of fire needle therapy combined with oral medication, which is consistent with conclusions from the analysis of the cured and marked effective rate. In the pathogenesis of psoriasis, CD4+T cells exert an enormous function. They differentiate into several types through stimulation by diverse inflammatory cytokines, involving Th1, Th2, Th17, Th9, Th22, follicular Th cells, peripheral Tregs, and T regulatory type 1, 53 in which Th1, Th2, Th17, and Treg cells participate in the entire process of psoriasis. The pathogenesis of psoriasis includes three cycles (Fig. 3). (1) Keratinocytes (KCs)/dendritic cells (DCs)/T-cell loop 54 : at an early stage of psoriasis, with the injured epidermis, KCs produce high-level CCL20, a chemokine cysteine motif chemokine ligand 20. 55 CCL20 has the ability to migrate myeloid DCs and CCR6+IL-17-producing T cells into focal skin regions. 54,56,57 Subsequently, DCs are activated by diverse stimuli, and release IL-23 and tumor necrosis factor (TNF)-α. IL-23 induces Th17 cells, which overexpress IL-17 and IL-22. Subsequently, IL-23, IL-17, and TNF-α act on KCs, resulting in epidermal hyperplasia. 58 (2) Th17/Treg balance 59 : Tregs, which mainly secrete Foxp3, tumor growth factor-β, and IL-10, are responsible for maintaining their own tolerance to inhibit autoimmunity. Proinflammatory Th17 cells, excreting IL-17, IL-12, IL-22, and IL-9, contribute to the induction and spread of inflammation. 60 In psoriatic lesions, IL-6 is released by epidermal cells, resulting in the increase of Th17 cells and the Th17/Treg ratio, which is an impaired function of Treg cells. 61,62 This plays a key role in maintaining the balance of Th17 and Treg cells. 59,63 (3) Th1/Th2 proportion 64 : CD4+T cells are differentiated into Th1 and Th2 cells by IL-1265 and IL-4 stimulation, 66 respectively. Th1 cells secrete cytokines such as IFN-γ, IL-2, and TNF-α and migrate to the psoriatic lesions by chemokines, showing proinflammatory effects. 54 However, Th2 cells appear to secrete poor cytokines, including IL-4 and IL-10. 67 Our previous study reported that IFN-γ, IL-17, IL-23, IL-6, and TNF-α levels significantly increased, whereas IL-4 and IL-10 levels were significantly decreased in the serum of patients with psoriasis. 68,69
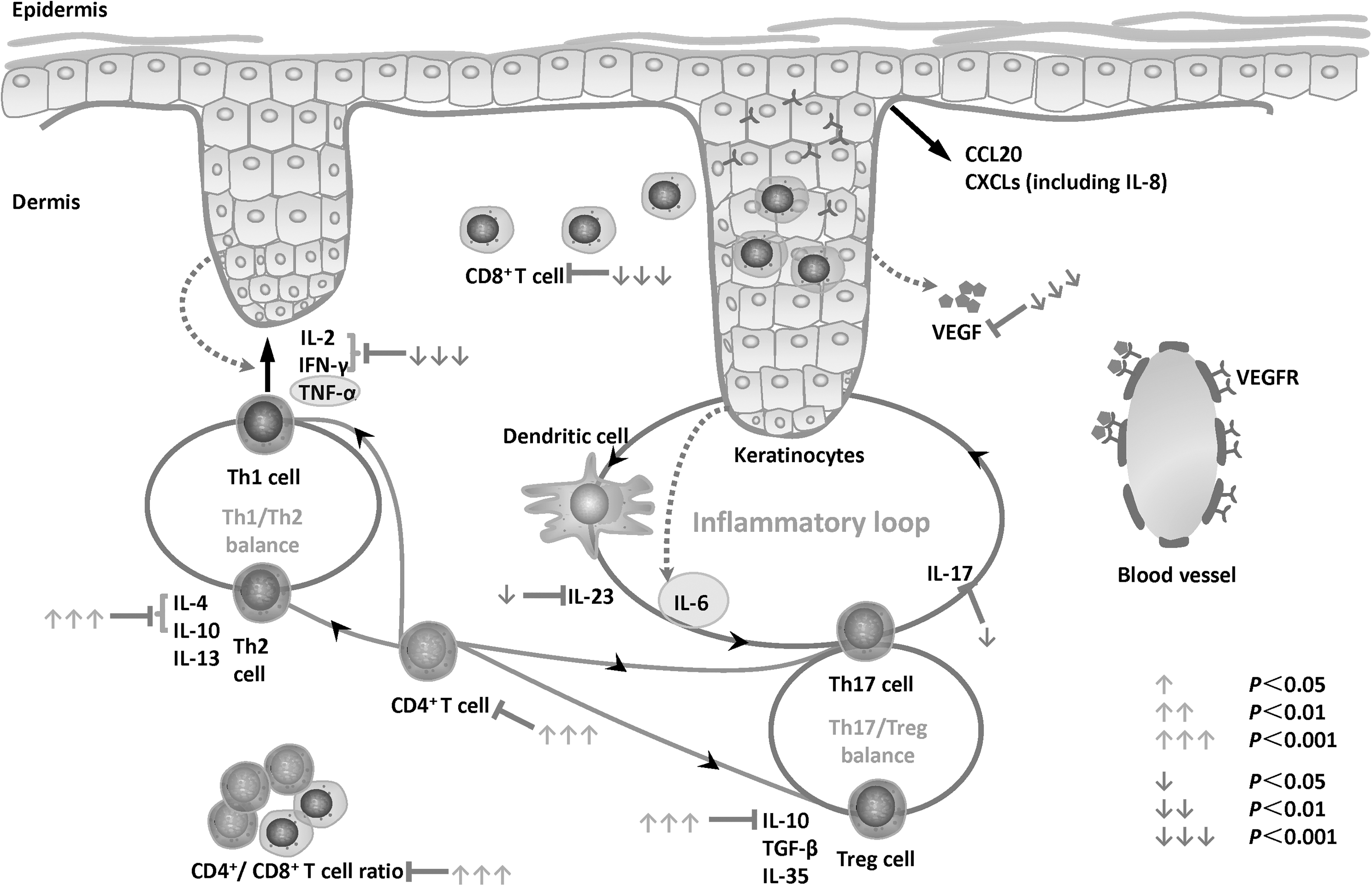
Immune responses of fire needle therapy plus oral medicines when treating psoriasis. Th1/Th2 proportion, Th17/Treg balance, and KC/DC/T cell loops are considered to play an essential part in pathogenesis of psoriasis. The onset of psoriasis begins with the release of IL-23 from DCs, characteristically by TNF-associated systemic inflammation. Activation of Th17 cells by IL-23 results in IL-17-mediated keratinocyte responses. After fire needle therapy, CD4+T cells are increased due to the increase in the number of Th2 cells, and cytokines secreted by them, such as IL-4 and IL-10. The proinflammatory CD8+T cells, Th1 cells, and cytokines are released by Th1 cells involving IL-2, but IFN-γ is reduced. Similarly, the decrease of IL-23 and IL-17 restores the inflammatory loop and maintains balance of Th1 and Th17. CD, cluster of differentiation; DC, dendritic cell; IFN, interferon; IL, interleukin; KC, keratinocyte; Th1, type 1 helper; Th2, type 2 helper; TNF, tumor necrosis factor.
After fire needle therapy, the number of CD4+T cells is increased. However, Th2 cells and cytokines secreted by these cells, such as IL-4 and IL-10, that exert an inhibitory effect are also increased. Meanwhile, the proinflammatory Th1 cells and cytokines released by these cells, including IL-2 and IFN-γ, decrease. CD8+T cells are increasingly believed to produce proinflammatory factors similar to those produced by CD4+T cells, which plays a key role in psoriasis. 70 Different from CD4+T cells, which are enriched and act in the dermis, CD8+ cells mainly migrate to the epidermis, aggravating the inflammatory response in skin lesions. 71 When treated with fire needle therapy, the number of CD8+T cells decreases, and the ratio of CD4+T cells/CD8+T cells is increased. Therefore, it has been suggested that the changes in CD4+T cells may be mainly due to the increase in the number of Th2 cells. Recently, a study on imiquimod-induced psoriasis-like mice manifested that fire needle therapy ameliorated skin lesions by thinning the epidermis, inhibiting KC proliferation, reducing CD3+T cell infiltration, and secreting inflammatory cytokines including IL-1β, IL-17A, and IL-23p40. 72 Since Treg cells also secrete IL-10, increased IL-10 level after fire needle treatment was shown to partially restore the function of Tregs. Similarly, a decreased IL-17 level represents a partial inhibition of Th17 function. This indicates that fire needle therapy restores the dynamic balance between Treg and Th17.
The formation of new blood vessels is also an important pathogenesis of psoriasis, in which VEGFs are considered to be an essential angiogenic factor. It is reported that VEGFs act on psoriatic lesions in two ways: one is in an indirect way, in which VEGFs derived from KCs are capable of inducing angiogenesis to produce essential nutrients to preserve the hyperproliferation of epidermis in a paracrine manner. 67 The other way is by means of VEGF receptors, which are expressed by the epidermis and are found in both the lesioned and nonlesioned areas of patients with psoriasis 73 that directly promote KC proliferation. 73 Hence, the amount of VEGF in peripheral blood circulation is associated with the degree of psoriasis activity. 74 In this study, fire needle therapy was found to relieve psoriasis primarily through the indirect manner, which inhibits the role of VEGFs in psoriasis. Fire needle therapy was able to reduce the number of VEGFs in the serum and, subsequently, control the development of psoriasis.
This study has the following limitations. First, this study does not include the types of experiments outside the RCT. If a more extensive research type is included, the research results will be more comprehensive and representative. Second, the current clinical research related to fire needle therapy cannot be designed as double-blind trial, which may lead to a bias in the results. Third, the randomization scheme and allocation concealment scheme in some studies are unclear, resulting in the limitations of the interpretation of outcomes. None of the included clinical trials claim to be designed, implemented, or reported in accordance with the Consolidated Standards of Reporting Trials (CONSORT) statement. Furthermore, there are few multicenter studies, and the sample size needs to be expanded. In addition, a PASI improvement rate of >60% (PASI60) is ideally found as a therapeutic evaluation index, but due to the low quality of the included literature, the PASI improvement rate is not uniform, including PASI60 and PASI70. Therefore, the efficacy evaluation indicator was defined as the cured and markedly effective rate, which includes the abovementioned two improvement rates. To address this issue, a multicenter randomized controlled trial of fire acupuncture for plaque psoriasis is also conducted, which is currently registered on
Conclusions
This meta-analysis of randomized controlled trials indicates that fire needle therapy is effective in treating psoriasis vulgaris patients with a low recurrence rate, and fire needle therapy may regulate the inflammatory loop of KCs/DCs/T cells, maintain Th17/Treg balance, and preserve Th1/Th2 proportions in psoriasis. However, due to the lack of rigorously designed research, the results should be interpreted with caution. To further clarify the effectiveness and related mechanisms of fire needle therapy on psoriasis, a more rigorous design, higher quality, and larger sample size trials are required.
Ethics Approval and Consent to Participate
This study was based on previously published studies; therefore, ethical approval and patient consent are not relevant.
Authors' Contributions
This study was proposed and designed by Dr. Xin Li and Prof. Bin Li. Prof. Bin Li obtained funding. Data acquisition and extraction were conducted by X.C., Y.L., M.X., J-K. S., Y.R., S-T. C., and X-Y. S., H-J. L, Y.L., and L.L. performed the statistical analysis of all data. L.L. and X.S. drafted the article, and Dr. Xin Li critically revised it.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by the National Key Research and Development Program of China (No. 2018YFC1705303), the National Natural Science Foundation of China (grant nos. 81874470, 81973860).
Supplementary Material
Supplementary Data
Supplementary Table S1
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Figure S6
Supplementary Figure S7
Supplementary Figure S8
Supplementary Figure S9
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.