
Abstract
Objective:
The development of pseudoaldosteronism is shown to be mainly associated with four factors: daily dose of glycyrrhiza (licorice), duration of glycyrrhiza use, body size, and age. Recently, direct bilirubinemia and hypoalbuminemia are newly reported as possible factors that trigger pseudoaldosteronism due to glycyrrhiza ingestion. Pseudoaldosteronism occurs in the presence of combinations of these factors; therefore, the importance of each factor on the tolerance to glycyrrhiza loading is still unclear.
Methods:
In seven patients (63–78 years old, six women) who developed pseudoaldosteronism due to ingestion of glycyrrhiza-containing Kampo extract in their clinic, serum albumin and direct bilirubin (D-bil) levels were investigated. In six women, the authors evaluated the correlations between daily dose of glycyrrhiza ingested and each factor: age, height, weight, body mass index, body surface area (BSA), and duration of ingestion (Pearson's correlation coefficient).
Results:
No patients had abnormal levels of serum albumin or D-bil around the time of the onset. In six women, the highest correlation coefficient was observed between BSA and the glycyrrhiza dose in Kampo extract at the onset of pseudoaldosteronism.
Conclusions:
The findings suggested that in elderly women, BSA should be considered first as a factor for predicting the development of pseudoaldosteronism.
Introduction
Pseudoaldosteronism is a well-known adverse drug event caused by Glycyrrhizin (GL)-containing medicines. GL is a major component of licorice root (Glycyrrhizae Radix), and numerous Kampo (Japanese herbal) medicines contain glycyrrhiza as a component herb.
As documented in the Manuals for Management of Adverse Drug Reactions (Ministry of Health, Labor and Welfare of Japan, 2006), 1 the development of pseudoaldosteronism is mainly associated with four factors: daily dose of glycyrrhiza, duration of glycyrrhiza use, body size, and age. 1,2 However, in actual clinical practice, pseudoaldosteronism occurs in the presence of combinations of these factors; therefore, it is difficult to identify the correlation between pseudoaldosteronism onset and each of the factors. In some cases the importance of glycyrrhiza dose even seems to be uncertain. For that reason, a former literature suggested that pseudoaldosteronism occurs independent of glycyrrhiza dose. 3 In a recent report, 4 authors also suggested that the known four factors might be even “confounding factors.”
The authors of this paper have reported that the incidence of pseudoaldosteronism is dependent on the daily dose of glycyrrhiza ingestion 5 and have reported two patients who recovered from pseudoaldosteronism by simply reducing the daily dose of glycyrrhiza-containing Kampo medicines. 6 These reports demonstrated that pseudoaldosteronism occurs in a dose-dependent manner.
The daily dose of glycyrrhiza that can be tolerated varies according to the individual person. Such a phenomenon is referred to as “dose dependency with individual differences.” 2 The Ministry of Health, Labor and Welfare Manual comments that individuals with a small body surface area (BSA), such as short and/or low-weight individuals, and the elderly are more likely to develop pseudoaldosteronism. 1 In their clinic most of the onsets of pseudoaldosteronism have been seen in elderly individuals with a small body size.
Honma et al. reported that with Shakuyakukanzoto extract granules (contains 6 g of crude drug glycyrrhiza, nearly equivalent to 240 mg of GL), the longer the duration of use and the more elderly the patient, the lower the potassium (K) level becomes; however, this trend is not seen with Shosaikoto extract granules (2 g of glycyrrhiza). 7 The authors of this paper also reported that the incidence of pseudoaldosteronism was notably affected by the daily dose of glycyrrhiza in Kampo extract (1, 2, 4, and 6 g of glycyrrhiza) rather than duration of ingestion. 5 These reports suggested that the daily dose of glycyrrhiza takes precedence over the duration of ingestion and elderly status. 2 However, importance of age, body size, and duration of ingestion (three factors) on the onset of pseudoaldosteronism is still unclear.
Furthermore, an elevated direct bilirubin (D-bil) level 4,8 and hypoalbuminemia 4,9 have been also pointed out as risk factors for pseudoaldosteronism.
For this study, the authors collected patients with pseudoaldosteronism from the department of Kampo medicine (Japanese herbal medicine) in their clinic to determine the level of importance that the three factors, as well as D-bil and albumin levels, have on the onset of pseudoaldosteronism.
Subject and Methods
The medical charts of patients registered as having developed pseudoaldosteronism due to glycyrrhiza-containing Kampo medicines and whose final clinic visit was between January 2014 and March 2019 were examined (from the whole medical records stored in their clinic as of April 2019). Those who fulfilled the diagnostic criteria proposed in the Manuals for Management of Individual Serious Adverse Drug Reactions 1 were enrolled in this study. In other words, diagnoses were made on the basis of the presence of hyporeninemic hypoaldosteronemia, increased blood pressure (BP), and decreased serum K levels due to administration of glycyrrhiza that normalized when glycyrrhiza was discontinued. If the clinical course seemed to be consistent with the expected course of pseudoaldosteronism, the patient was diagnosed as having pseudoaldosteronism even if the plasma renin activity (PRA) and plasma aldosterone concentration (PAC) were relatively low (PRA <0.5 ng/mL/h and PAC <8 ng/dL) but within the standard values. Patients in whom PRA and PAC were not measured at the time of onset were excluded.
Age, height, weight, body mass index (BMI), BSA (DuBois method), daily dose of glycyrrhiza, duration of ingestion, PRA, PAC, K value, and increase level in systolic BP at onset were recorded for each patient. The authors estimated daily glycyrrhiza dosage according to the licorice content in each Kampo medicine administered to each patient.
How easily pseudoaldosteronism develops in each individual depends on the tolerance to glycyrrhiza loading of each; therefore, using correlation coefficient, the authors examined relationship between glycyrrhiza dose in Kampo medicine and other factors: patient's age, height, weight, BMI, BSA, and duration of Kampo medicine ingestion. Regression analysis was performed between BSA and daily dose of glycyrrhiza in Kampo medicines.
The serum albumin and D-bil level could not be measured at the time of onset in this study. For patients attending the Kampo clinic with a history of pseudoaldosteronism, bilirubin levels were measured when blood sampling had to be performed for any reason. The serum albumin values were obtained in tests performed within 6 months from the time of disorder onset. When multiple data were available, the measurement value closest to the time of onset was used. The standard value was ≥4.0 g/dL for albumin and ≤0.4 mg/dL for D-bil (vanadic acid method).
Results
The authors enrolled seven patients (one man and six women) with pseudoaldosteronism, and the age was 63–78 (mean 71.6) years (Table 1). All patients had taken glycyrrhiza-containing Kampo extract granules (Tsumura & Co, Tokyo, Japan) at the onset of pseudoaldosteronism (Table 2). Components of each Kampo extract are shown in Table 3. All Kampo preparations contain glycyrrhiza that is defined and regulated by the Japanese Pharmacopoeia (JP). Glycyrrhiza JP contains ∼4.0% of glycyrrhizic acid.
Patient Background
BMI, body mass index; BSA, body surface area; F, female; M, male; RA, rheumatoid arthritis.
Kampo Medicine, Dose, and Duration of Glycyrrhiza Intake
Components of Kampo Extracts Taken by Patients
These constituent herbs are defined and regulated by the JP. Glycyrrhiza JP contains ∼4.0% of glycyrrhizic acid.
ALR, Atractylodes lancea rhizome; JP, Japanese Pharmacopoeia; TSGS, Tokishigyakukagoshuyushokyoto.
None of them was on an aldosterone receptor blocker, angiotensin-converting enzyme inhibitor, angiotensin II receptor blocker, diuretics, or corticosteroids. At the time of onset, BP was elevated in all patients; however, hypokalemia (standard 3.5–5.0 mEq/L) was seen in only three (Table 4), and edema was observed in only one patient. All patients recovered from the increased BP, edema, and abnormal K value by discontinuing glycyrrhiza-containing Kampo medicine or decreasing its dose.
Patient Data
N/A, not available; sBP, systolic blood pressure.
None of the patients had hepatic dysfunction or elevated D-bil values. In case 3, D-bil levels measured twice were 0.1 mg/dL at both times. In case 6, D-bil levels measured for three times were 0.3–0.4 mg/dL, which were within normal limit (Table 4).
The albumin level could be confirmed in three patients, in whom severe diseases were absent. None of the three patients had hypoalbuminemia (Table 4).
Of the seven patients, five were slim with a BMI below 20 kg/m2, and the sole man had BMI of 19.8 kg/m2. For four of the six women, the weight was ≤42 kg, and three patients had a height of 140–145 cm. The BSA of five patients was ≤1.37 m2 (mean value for Japanese adult women was ∼1.43 m2), showing that most patients with pseudoaldosteronism onset had a small body size (Table 1).
The 68-year-old woman (case 2), whose BSA was 1.5 m2 (first among the women), did not have onset after ingesting 2.3 g of glycyrrhiza in Kampo extract but showed onset after ingesting 3.5 g, which was the largest daily dose among the six women. The 70-year-old women (case 3), with BSA of 1.37 m2 (ranked second), did not have an onset when ingested 2 g of glycyrrhiza in Kampo extract; however, she had onset when she ingested 2.7 g (second largest) for 24 weeks. In these cases, the onset occurred when ingested for 4–24 weeks with a glycyrrhiza daily dose of 2.3–3.5 g and, with 1.0–2.3 g, onset occurred in 3–6 years.
In the six women, correlation coefficients were calculated between the daily dose of glycyrrhiza in Kampo extract and each factor: age, body size, and duration of ingestion. The correlation coefficient for age was −0.25 (Fig. 1); height, 0.71; weight, 0.85; BMI, 0.38; BSA, 0.97 (Fig. 2); and duration of ingestion, −0.72 (Fig. 3). The strongest correlation coefficient was seen between BSA and daily dose of glycyrrhiza in Kampo medicines. The regression formula for analyzing BSA (x) and daily dose of glycyrrhiza (y) was y = 5.725x − 5.195 (R 2 = 0.932).

Correlation between age and glycyrrhiza dose.
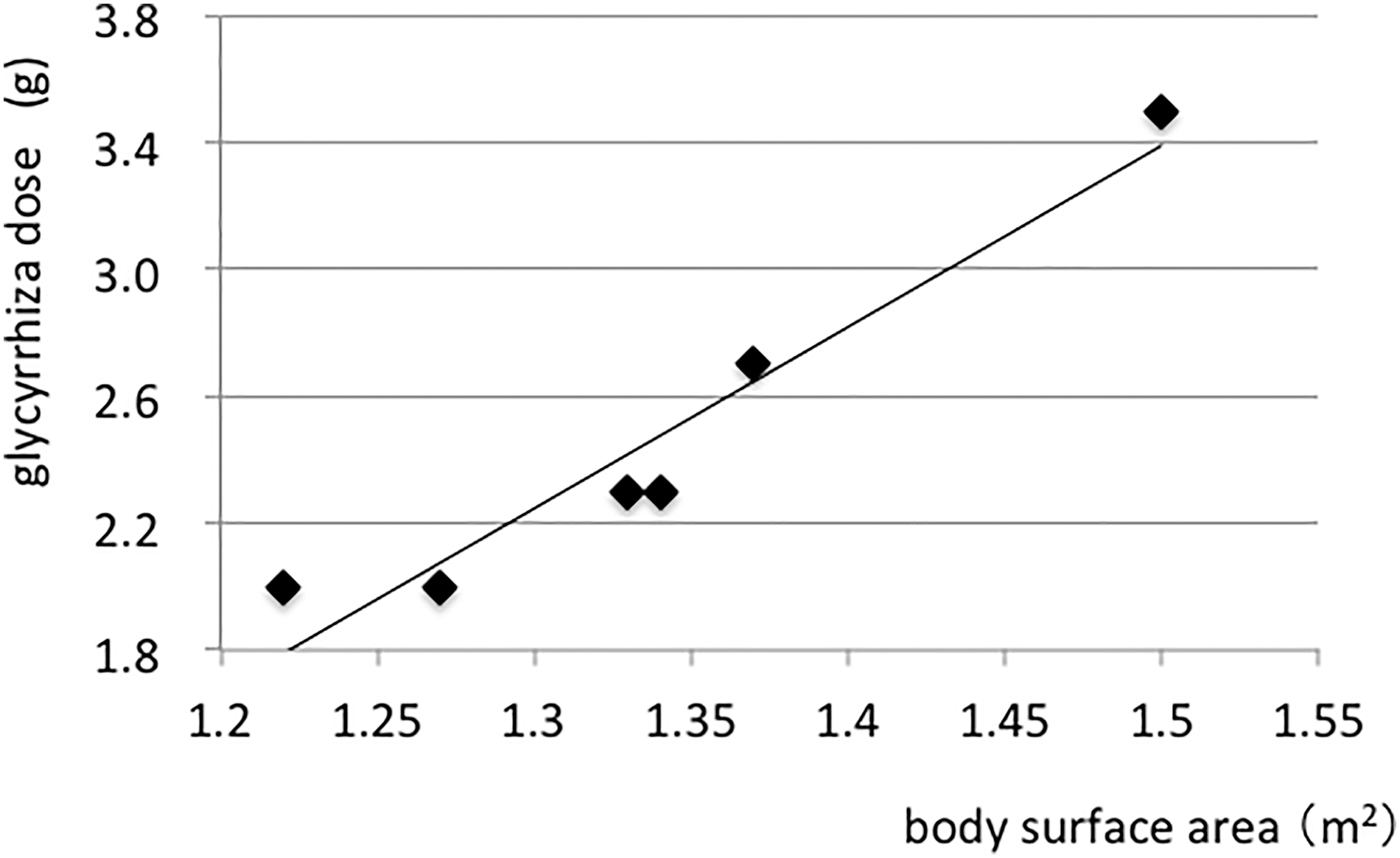
Correlation between body surface area and glycyrrhiza dose.

Correlation between ingestion period and glycyrrhiza dose.
Discussion
At their clinic, the standard values are PRA 0.2–3.9 ng/mL/h (while seated) and PAC 3.6–24.0 ng/dL (any time). Morimoto and Nakajima reported PRA and PAC of 63 pseudoaldosteronism patients. 3 Their data demonstrated that most patients had suppressed PRA and PAC, although in some patients, PRA and PAC were not fully suppressed (PRA 0.31–0.5 ng/mL/h, PAC 5.0–7.0 ng/dL). The authors of this paper have also experienced early-stage patients in whom PRA and PAC remained within normal limit. Thus, the criteria for enrollment in this study were determined as follows: both PRA below 0.5 ng/mL/h and PAC below 8 ng/dL.
Shimada et al. compared a hypokalemia group and nonhypokalemia group comprising 184 outpatients and 205 inpatients (PRA and PAC were not measured). The patients were treated with Yokukansan (Kampo medicine) for behavioral and psychologic symptoms of dementia or mental symptoms. They reported that decreased albumin levels, use of the full amount of Kampo medicines, and coadministration with LPIDs (lower potassium inducing drugs) were risk factors for hypokalemia. 9 Their patient groups registered at a university hospital might include a certain number of patients with severe diseases and fragile patients.
Meanwhile, Makino et al. have pointed out the importance of multidrug resistance protein 2 (MRP2; which eliminates bilirubin into the bile) dysfunction as a causal factor of pseudoaldosteronism. 10,11 Yoshino et al. reported high levels of D-bil in two terminal cancer patients (one patient died 2 months after starting Kampo medication) found to have low K levels after taking glycyrrhiza (PRA and PAC were not measured). 8
Furthermore, Komatsu et al. reported that high levels of D-bil and low levels of albumin are predictive factors for pseudoaldosteronism in a group of chronic hepatic disease patients (including cirrhosis) treated with GL formulations at a university hospital (PRA and PAC were not measured). 4 The authors have remarked that high levels of D-bil reflect MRP2 dysfunction.
In this study (both PRA and PAC were measured), the D-bil values of all subjects were within normal limit (≤0.4 mg/dL, vanadic acid method), and serum albumin levels in three patients were normal. The subjects of their investigation were relatively healthy patients. None of the seven patients had a severe disease, and none was on LPIDs. Serious conditions were relatively few in the patient of their clinic compared with the patients of university hospitals.
The low albumin levels seen in the articles by Shimada et al. 9 and Komatsu et al. 4 likely reflect anorexia due to cirrhosis or a severe disease. In such patients, there is also the possibility that pooled K in the body is constantly decreased. Moreover, the high D-bil levels in chronic hepatic disease suggest liver cirrhosis, which causes hypoalbuminemia. These studies 4,8,9 demonstrate the possibility of pseudoaldosteronism occurring in patients with severe diseases and/or cirrhosis. Low albumin levels and high D-bil levels might be predictive factors for pseudoaldosteronism in such a high-risk group.
In contrast, among the 243 Kampo clinic patients in the study by Yoshino et al., only 2 patients (0.9%) showed high D-bil levels. The D-bil levels of the remaining 241 patients were within normal ranges. 8 As such, the percentage of patients with high D-bil levels is very small among Kampo clinic patients. Although the results of this study cannot rule out the possibility that a high D-bil level and a low albumin level are factors affecting pseudoaldosteronism, the importance of high D-bil level and low albumin level on the onset may be small among Kampo clinic patients, especially when there are no complications from severe diseases or cirrhosis. Furthermore, no reports stating that pseudoaldosteronism was triggered in patients with Dubin–Johnson syndrome (MRP2 disorder) were found by their literature search.
In Table 1, “small body size” stands out among the causal factors. A 68-year-old woman (case 2), who was not thin (BMI 22.1) and had the largest BSA (1.5 m2) among women, did not develop the disorder when she ingested Kampo extract containing 2.3 g of glycyrrhiza, but developed with 3.5 g (maximum dose) for 4 weeks (shortest duration). This demonstrated that even if the body size is not small, ingestion of Kampo extract containing 3.5 g of glycyrrhiza can trigger the onset in a short period. Case 2 with BMI 22 and BSA 1.5 m2 developed with 3.5 g, and the patients (including the man) with BMI <20 developed with 1.0–2.3 g of glycyrrhiza contained in Kampo extract. These data suggest that body size and the daily dose of glycyrrhiza in Kampo extract are closely related.
How easily pseudoaldosteronism develops in each patient depends on the tolerance to glycyrrhiza loading of each. Individuals, who can tolerate only a small dose of glycyrrhiza, easily develop pseudoaldosteronism with a small dose. Thus, the factors closely correlated to the daily dose of glycyrrhiza at the onset can be used as predictive factors. The patients with “small BSA, such as being short, low weight, 1 are likely to develop pseudoaldosteronism; however, it has not been clear which indices of height, weight, BMI, and BSA are most appropriate to use. Therefore, the authors have analyzed the correlation between various factors and the daily dose of glycyrrhiza contained in Kampo extract in six women with onset of pseudoaldosteronism.
Among the factors related to body size, the strongest correlation coefficient was seen between BSA and daily dose of glycyrrhiza in Kampo extract (correlation coefficient of 0.97). As with anticancer drugs, BSA is probably appropriate to predict the daily dose of glycyrrhiza that can be tolerated.
It is noteworthy that, for example, case 3 with onset following the ingestion of Kampo extract containing 2.7 g of glycyrrhiza may likely show onset with even 2 g. The threshold cannot be strictly confirmed from an observation study performed in a clinical setting. The authors confirmed that case 4 and 5 had no onset with a smaller daily dose. Comprehensively, the authors presumed that BSA affects the deepest the daily dose of glycyrrhiza in Kampo extract at time of onset.
Next is a discussion of the factors concerning the duration of ingestion. Case 2 experienced pseudoaldosteronism onset in a short time of 4 weeks after ingesting Kampo extract containing 3 g of glycyrrhiza. Case 3 who ingested 2.7 g (ranked second) experienced the onset in 24 weeks. In the seven patients, the duration of ingestion was 4–24 weeks when the daily dose of glycyrrhiza in Kampo extract was 2.3–3.5 g, and the onset occurred in 3–6 years when the daily dose was 1.0–2.3 g.
The duration of ingestion seems to be subordinate factor that was regulated mainly on the basis of the daily dose of glycyrrhiza. Basically, the aim of searching for factors clinically related to onset is to be able to predict patients who are prone to develop. The duration of Kampo medicine administration cannot be determined at the time of the prescription and therefore cannot be considered a predictive factor of inclination to onset.
In contrast, as the statement by Honma et al. “the longer the duration of ingestion, the lower the K level in the Shakuyakukanzoto group,” 7 the duration of ingestion is a factor of increasing severity. General practitioners and pharmacists must engage in early detecting of pseudoaldosteronism by instructing patients to routinely perform BP measurements.
The correlation coefficient between age and daily dose of glycyrrhiza in Kampo extract was 0.2. The authors suppose that the reason is that, among the elderly aged 67–78 years, individual characteristics were likely more significant rather than age. This result showed that the simplification of “the higher the age, the easier the onset” cannot be established. Although young patients were also administered with glycyrrhiza in their clinic, pseudoaldosteronism occurred only in elderly patients, showing that the age factor is still important. Ito et al. also reported that the age of patients with onset of pseudoaldosteronism was significantly high (p < 0.01) compared with the overall age. 12
Among the seven patients in this study, four had onset after 3–6 years of ingesting glycyrrhiza-containing Kampo extract. In such cases, rather than the number of years of ingestion, “aging” within the 3–6 year period is probably the determining factor for the onset. One cannot suggest that it takes 6 years for GL metabolite to inhibit the activity of 11β-HSD2. In addition, the activity of 11β-HSD2 that converts cortisol to cortisone is known to decrease with age. 13,14 Furthermore, there are also individuals who experience weight loss due to aging. These factors likely make the conditions where the onset readily occurs.
The patients attending their clinic also include those with advanced cancer, collagen diseases, and patients on LPIDs. However, none of them were included among the seven patients in this study. The findings in this study were presumed to reflect the simple appearance of pseudoaldosteronism among the patients with no specific diseases that readily trigger pseudoaldosteronism or with no LPIDs. Pseudoaldosteronism also occurred when a slim man with BMI of 19.8 ingested only 1 g of glycyrrhiza contained in Kampo extract, showing that one cannot generally say that the disorder occurs exclusively in women.
Based on the former articles 5,7 and the results of this study, the authors consider that the importance of each predictive factor probably lines up in the following order: daily dose of glycyrrhiza ingested > body size (BSA) > age. “The tolerance to glycyrrhiza loading”, at least in part, depends on body size and age. The daily dose of glycyrrhiza in Kampo medicines affects the duration until onset of the disorder. It is preferable to be aware of the following: (1) for high doses, a small body or an elderly, caution should be taken, and (2) for elderly patients with a small body, there are cases where the onset occurs after administration of a small amount (1–2 g) over several years.
The daily dose of glycyrrhiza is certainly not “a confounding factor” of the onset of pseudoaldosteronism. 1,2,5 –7,9 This study also suggested that the four known factors are important. In addition, it may be preferable to measure D-bil and albumin values at least once for each patient.
Their clinic has six Kampo experts and, as such, Kampo medicines are prescribed for a relatively high number of patients. In this study period, ∼5000 patients newly visited to the department of Kampo medicine in their clinic. Nevertheless, only seven cases with the onset were observed. All of the cases were detected in the mild stage, and they could recover by discontinuing glycyrrhiza-containing Kampo extract or decreasing its dose. If glycyrrhiza is prescribed with caution, pseudoaldosteronism due to glycyrrhiza is not an adverse drug reaction that one should fear.
Conclusions
When the correlation coefficients between daily dose of glycyrrhiza in Kampo extract ingested at the time of onset and each factor (age, height, weight, BMI, BSA, and duration of ingestion) were examined in the six elderly women with onset of pseudoaldosteronism, BSA showed the highest correlation. Although age and duration of ingestion are also important, BSA may be the most superior as the predictive factor of the onset of pseudoaldosteronism. None of seven cases showed low albumin values or high D-bil values, suggesting that the impact of such factors on pseudoaldosteronism may be relatively small.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.