
Abstract
Objective:
The aim of this study was to evaluate the effects of Ayurvedic treatment on deceleration of the disease progress of nondialysis patients with stage IV or V chronic renal failure (CRF).
Materials and Methods:
A complex oral and proctocolonic Ayurvedic multiherbal medication was administered daily for 1 month to inpatients. Thereafter, patients were treated as outpatients with oral medication for additional 5 months. Four renal function tests (RFTs) were evaluated at various time points (TPs): (1) 6 months before baseline (TP −6), (2) at baseline (TP 0), and (3) after completion of 6 months of treatment (TP +6). Repeated-measures analysis of variance (ANOVA) with Greenhouse–Geisser correction and Friedman's ANOVA by ranks were used to analyze the RFTs. For post hoc tests, the Bonferroni correction was applied. Bias-corrected effect sizes (Hedges) for the treatment were calculated.
Results:
Sixty-four nondialysis CRF patients with laboratory investigations of the preceding 6 months were included; 12 patients discontinued the treatment. Fifty-two patients with stage IV or V at baseline completed the study. Mean concentrations of estimated glomerular filtration rate (eGFR), serum creatinine, and hemoglobin differed significantly between TPs (eGFR: F = 15.3, p < 0.001; serum creatinine: F = 29.3, p < 0.001; blood urea: F = 2.0, p = 0.159; hemoglobin: F = 53.9, p < 0.001). Pairwise comparisons of the mean differences between TPs are significant for eGFR, creatinine, and hemoglobin. For blood urea, a significant decrease was observed for the treatment period [15.9(↓) mg/dL, standard error 4.0; n = 52], but a nonsignificant increase was observed for the pretreatment period [16.2(↑) mg/dL, standard error 9.8] due to insufficient data for TP −6 (n = 26). The effect sizes for eGFR, creatinine, blood urea, and hemoglobin were medium (0.45, 0.53, 0.44, and 0.30).
Conclusions:
After 6 months of treatment, statistically and clinically significant improvements of eGFR, creatinine, blood urea, and hemoglobin and a significant shift to better CRF stages were observed. Several cardinal symptoms were also significantly reduced. Randomized controlled trials are warranted to evaluate the effects in comparison to usual care.
Introduction
Chronic renal failure (CRF) usually develops into end-stage renal disease (ESRD) within a course of only a few years. The incidence of ESRD—worldwide as well as in India—is increasing day by day. 1,2 Globally, more than 100 countries (with a combined population of >1 billion) have no provisions for chronic maintenance dialysis or kidney transplantation, and thus, more than 1 million people die annually from ESRD on a global scale. 3 –5 Data suggest that about 220,000–275,000 new patients need a renal replacement therapy (RRT) every year in India and Pakistan. 6 It is estimated that there are about 55,000 dialysis patients in India, and this population is growing at the rate of 10%–20% annually. 6 Because of the increasing incidence (increase nearly doubled from 2003 to 2013), 6 –8 nearly 10% of patients all over India are getting dialysis due to problems of accessibility and affordability. 8 Hemodialysis costs in India are also high in comparison to income levels. 9 Hence, efforts are needed to develop strategies to decelerate the progression of CRF. A 10% or 20% improvement in the estimated glomerular filtration rate (eGFR) of stage IV or V patients decreases the need of RRT, and estimated cumulative savings may be of 25% and 55%, respectively. Studies suggest that the cumulative economic impact of slowing the progression of CRF, even by as little as 10%, would be staggering from a health economic perspective. 10
The acceleration of disease progression of CRF can be judged by observing changes in eGFR within a 6-month period. According to the clinical observations of the authors during routine Ayurvedic hospital practice in CRF patients, it usually takes less time to develop ESRD from stage IV than the development of stage III from stage II.
Some preliminary scientific evidence exists, suggesting beneficial effects of Ayurvedic treatments in signs and symptoms as well as in renal function tests (RFTs) of CRF patients. 11 –14 Such treatments are being implemented in the P. D. Patel Ayurveda Hospital, Nadiad, India, with satisfactory clinical outcomes in CRF patients since improvements in eGFR as well as RFTs in stage II or stage III were commonly observed in our hospital.
The main aim of this study was to evaluate the effects of Ayurvedic treatment on the deceleration of the disease progress of nondialysis stage IV–V patients with CRF by comparing the mean changes of eGFR and RFTs at different time points (TPs): (1) 6 months before the beginning of the Ayurvedic treatment (TP −6), (2) at baseline (TP 0), and (3) 6 months after baseline (TP +6).
Materials and Methods
Study design
This is a quasi-experimental pilot study with a one group pre- and postdesign and two premeasurements defining a 6-month period for the Ayurvedic treatment and a 6-month pretreatment period reflecting the counterfactual. Permission was obtained from the Institutional Ethics Committee for Human Research of the J. S. Ayurveda College, Nadiad. A written consent of all patients was obtained before the start of this study.
Participants
During the period between January 2016 and June 2016, all CRF patients meeting the inclusion criteria listed below were selected from both the outpatient department and the inpatient department of the P. D. Patel Ayurveda Hospital, Nadiad, India (Teaching Hospital of the J. S. Ayurveda College). Also, a laboratory investigation record (RFTs and hemoglobin level) of the preceding 6 months was necessary for an inclusion into the study. Patients were enrolled one by one without specific recruitment procedures except informed patient consent.
Participants of both genders aged 18–60 years with a confirmed diagnosis of stage IV–V CRF (eGFR <30 mL/min/1.73 m2), not having undergone RRT, were included.
Patients who had received renal transplantation and patients with other serious chronic comorbidities, which could interfere with the outcomes or with a completion of the study, that is, severe cardiovascular diseases, severe mental disorders, and severe liver or metabolic disorders were excluded from the study. Serious acute conditions as well as pregnancy, breastfeeding, and postdelivery period were also exclusion criteria.
Study protocol and treatment
Enrolled patients were hospitalized for a period of 1 month. They were assessed clinically and through laboratory investigations (RFTs and a hemogram) on the first day of hospitalization. The clinical record of this assessment was considered as TP 0 (baseline). The laboratory investigations of 6 months preceding the hospitalization date (±5 days) were also recorded and considered as TP −6. Table 1 depicts the oral Ayurvedic medication administered daily to all patients.
Oral Ayurvedic Medication
Together with these orally administered medications, each patient was treated with Ayurvedic enemas (nirūha-basti) containing 40 mL Punarnavādi-kvātha (decoction) daily in the morning 1 h before lunch.
All these Ayurvedic preparations were solely prepared by Sundar Ayurveda Pharmacy (teaching pharmacy of the J. S. Ayurveda College) under continuous expert supervision.
Antihypertensive, antihyperglycemic, and/or diuretic drugs prescribed by conventional physicians before baseline were continued initially, but dosages were modified or the drugs completely discontinued in the course of treatment if blood and urine sugar levels, blood pressure, and electrolytes were continuously low and/or reduction in edema as well as an increase in urine output were observed. Vitamin D, calcium preparations, or erythropoietin prescribed before baseline was continued due to the fact that the kidneys were not able to produce sufficient amounts of vitamin D and erythropoietin, to prevent osteodystrophy and anemia.
All patients were strictly instructed to follow a specific Ayurvedic diet. Boiled mung (green gram), mung bean soup, boiled vegetables, and rice were given for lunch, whereas mung bean soup, rice or khichaḍī (Indian recipe containing equal quantities of boiled mung beans and white basmati rice), and boiled vegetables were given for dinner. Patients were allowed to eat papaya, sweet apples, puffed rice, and dates as snacks if they felt hungry during the day. Additionally, to the breakfast milk (described in Table 1), patients could take up to 150 mL boiled cow's milk during the day, but keeping a minimum break of 1 h before and after the above-mentioned food items. Salty and/or sour-tasting food was strictly forbidden. In a few cases, small quantities of saindhava-lavaṇa (pink rock salt) and spices except chili were permitted on strong patient demand.
After 1 month of this treatment, the patients were discharged from our hospital and instructed to continue the intake of all medications (except the enema), and to adhere to the Ayurvedic food regimen. Monthly checkups at our hospital were performed for the following 5 months. Hence, the total active treatment period lasted for 6 months.
Outcomes and measurements
RFTs (eGFR, serum creatinine, blood urea, serum electrolytes, serum calcium) and the hemoglobin level were recorded 6 months before baseline (±5 days) (TP −6). The same investigations were performed in the laboratory of the study institute at the date of starting the Ayurvedic treatment (TP 0, baseline). The final assessment with laboratory investigations was performed 6 months after completion of our treatment in the same laboratory (TP +6).
CRF-specific signs and symptoms were assessed by using a grade score (Table 2), which was adopted from a previously published research article. 14 Changes in signs and symptoms, eGFR, albuminuria, serum creatinine, blood urea, serum electrolytes, serum calcium, and hemoglobin level were observed. For the calculation of eGFR, the DaVita Glomerular Filtration Rate calculator was used, which applies the 2009 CKD-EPI creatinine equation, recommended by the KDIGO Clinical Practice Guidelines for Management of Chronic Kidney Disease. 15
Grade Score of Signs and Symptoms
Statistical analysis
This is a quasi-experimental clinical pilot study with one group pre- and postdesign and two premeasurements defining a 6-month period for the Ayurvedic treatment and a 6-month pretreatment period reflecting the counterfactual. Quasi-experimental designs test causal hypotheses but, in lieu of a randomized assignment of the intervention, seek to define a comparison group or time period that reflects the counterfactual (i.e., outcomes if the intervention had not been implemented). 16 Categorical data are presented as numbers and percentages. Continuous data are presented as mean and standard deviation, and median and range. Normality of the variables was tested by Kolmogorov–Smirnov test. The null hypothesis of normal distribution was rejected if p < 0.05. A repeated-measures analysis of variance (ANOVA) with Greenhouse–Geisser correction to analyze the four RFTs for the various TPs and in particular the treatment effects was used. Mauchly's test of sphericity, an important assumption of a repeated-measures ANOVA, was calculated. Greenhouse–Geisser correction was applied. This correction alters the degrees of freedom and produces an F-ratio where the type I error rate is reduced. The tests of “Within-Subjects Effects” describe if there was an overall significant difference between the means at the different TPs. In addition, we used related-samples Friedman's two-way ANOVA by ranks with the Bonferroni correction for multiple tests. The bias-corrected effect sizes (Hedges) with 95% confidence intervals (CIs) were calculated. For various post hoc tests, the Bonferroni correction was applied. A two-sided p-value of <0.05 was considered to indicate statistical significance. Statistical analysis was performed using R version 3.5 (R Foundation) and IBM SPSS Statistics, version 26.0 (IBM Corp., Armonk, NY).
Results
In total, 64 patients were enrolled during the period between January 2016 and June 2016. Seven patients discontinued the treatment due to personal (nonmedical) reasons. Five patients were withdrawn from the study by the investigator within the first 10 days of their treatment due to the need of RRT on the basis of continued breathlessness, strong accumulation of body fluid, and other features of severe uremia. Overall, 52 patients completed the study protocol.
Basic characteristics
The median age of the patients was 51 years (range 18–60 years), 57.7% male and 42.3% female. Forty-six patients (87%) suffered from CRF since 5 years or longer. More than 70% of the patients reported a sedentary life style and high stress levels. Hypertension was found in 57% of the patients and chronic nephritis in 25% of the patients. In only 21% of the patients, diabetes mellitus was found to be the main cause of CRF.
Renal function tests
Six months before starting the Ayurvedic treatment (TP −6), the mean values ± standard deviation of eGFR, serum creatinine, blood urea, and hemoglobin were 19.96 ± 11.84 mL/min/1.73 m2, 5.94 ± 2.34 mg/dL, 81.85 ± 52.72 mg/dL, and 11.48 ± 1.75 g%, respectively. At the time of first consultation (before starting the Ayurvedic treatment), the same parameters ranged at 11.36 ± 5.87 mL/min/1.73 m2, 5.94 ± 2.34 mg/dL, 97.73 ± 37.42 mg/dL, and 9.71 ± 1.69 g%, respectively. After 6 months of Ayurvedic treatment (TP +6), the mean values of eGFR, serum creatinine, blood urea, and hemoglobin were 15.98 ± 13.23 mL/min/1.73 m2, 4.80 ± 1.95 mg/dL, 81.87 ± 34.52 mg/dL, and 10.21 ± 1.58 g%, respectively (Table 3). Profile plots for eGFR, serum creatinine, blood urea, and hemoglobin (Figs. 1–4) facilitate the understanding of the results mentioned in Table 3.

Profile plots of the mean values with 95% CI of hemoglobin at the time points −6, 0, and +6. CI, confidence interval.
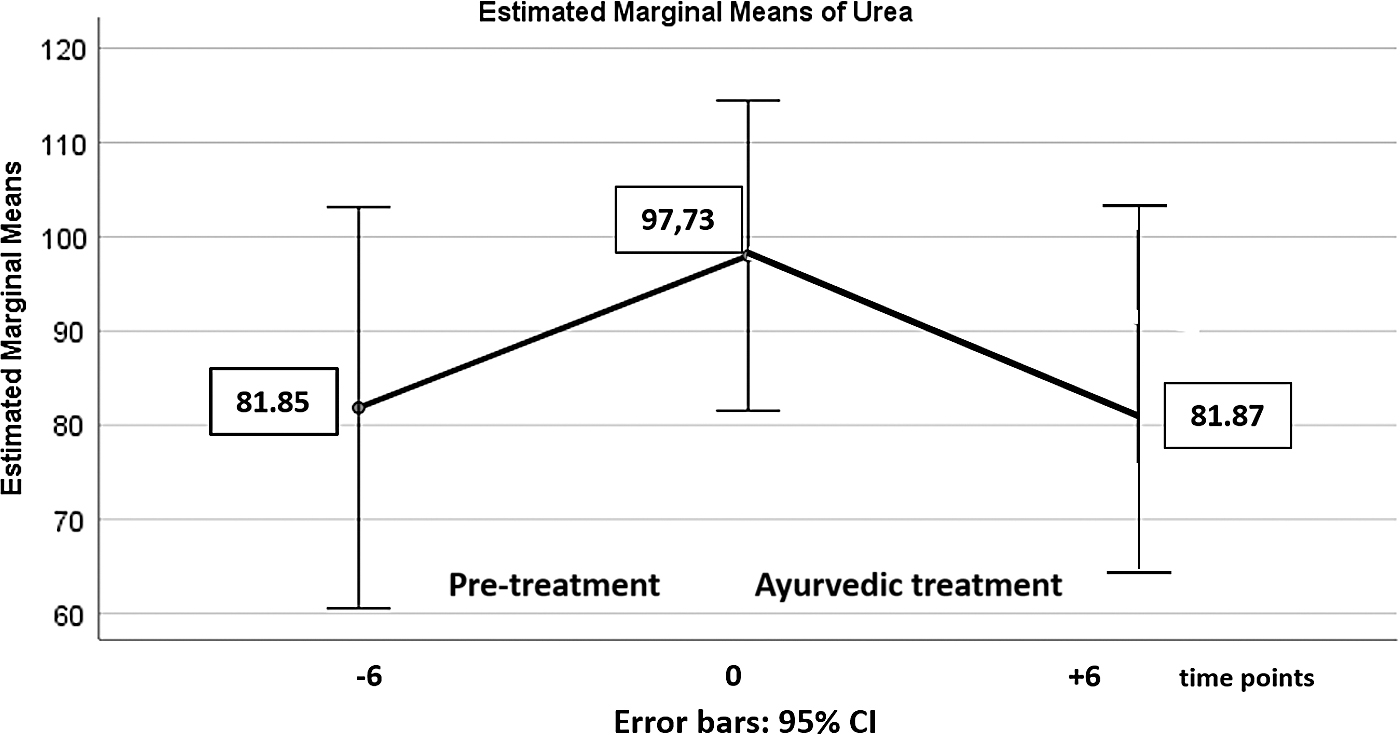
Profile plots of the mean values with 95% CI of blood urea at the time points −6, 0, and +6. CI, confidence interval.
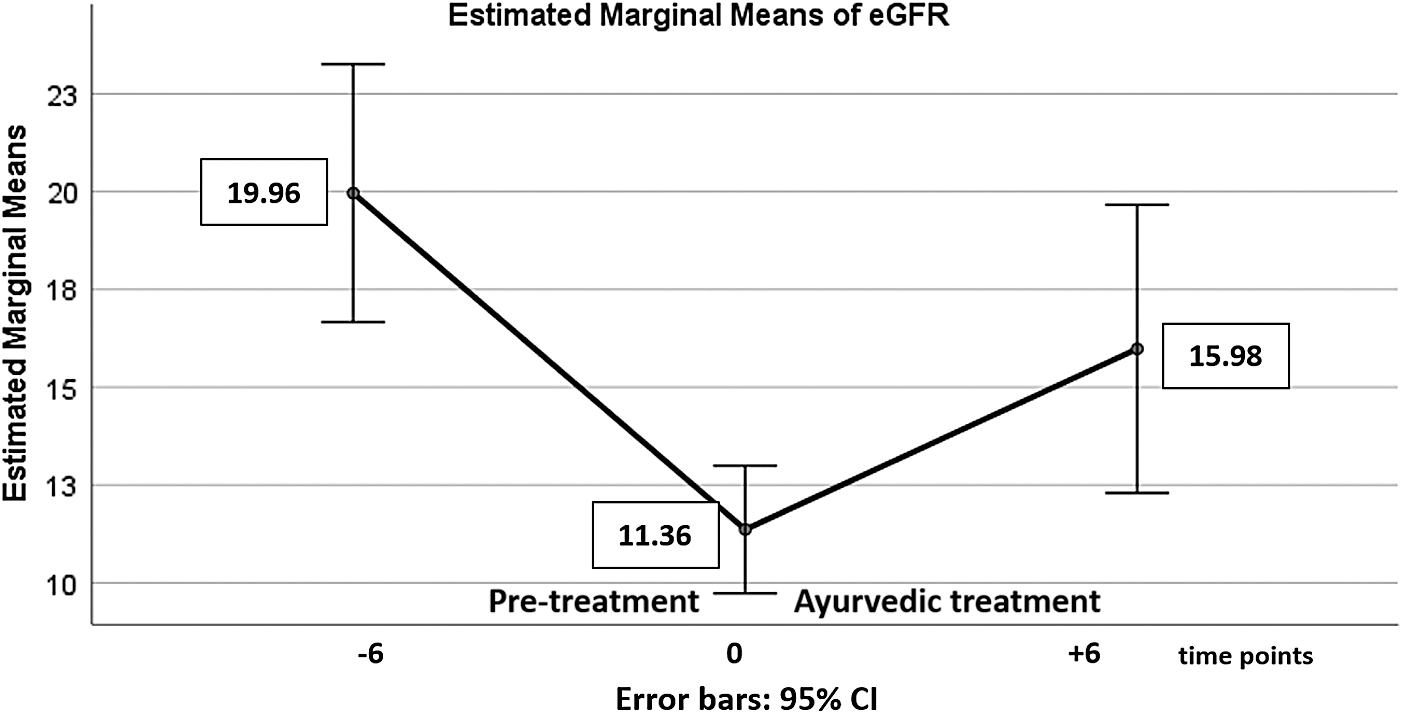
Profile plots of the mean values with 95% CI of eGFR at the time points −6, 0, and +6. CI, confidence interval; eGFR, estimated glomerular filtration rate.
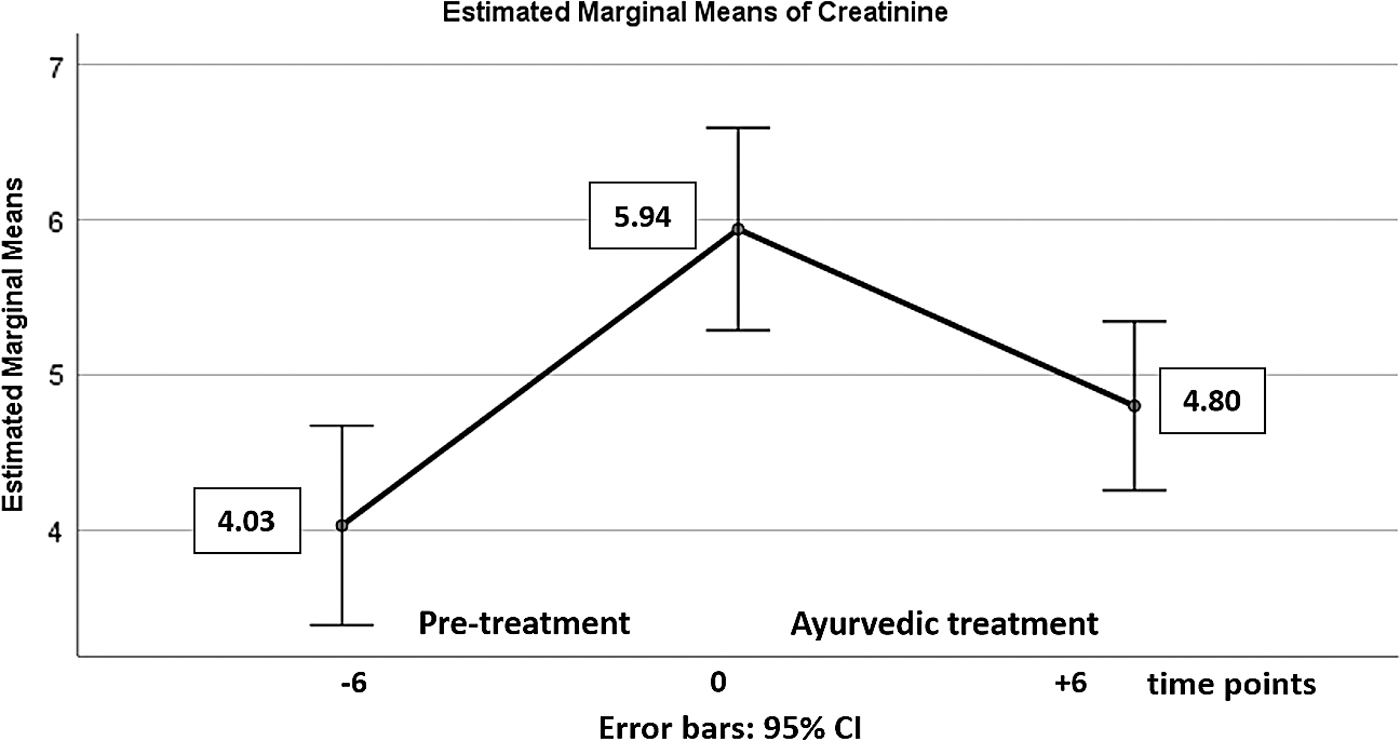
Profile plots of the mean values with 95% CI of serum creatinine at the time points −6, 0, and +6. CI, confidence interval.
The Means and Medians of Renal Function Tests at the Three Defined Time Points
eGFR, estimated glomerular filtration rate; RFT, renal function test.
The repeated-measures ANOVA with a Greenhouse–Geisser correction determined that the mean RFT concentrations differed statistically significantly between the three TPs, except for blood urea [eGFR: F(df = 1.5, error:df = 76.5) = 15.3, p < 0.001; serum creatinine: F(df = 1.5, error:df = 77.3) = 29.3, p < 0.001; blood urea: F(df = 1.5, error:df = 37.5) = 2.0, p = 0.159; and hemoglobin: F(df = 1.7, error:df = 85.1) = 53.9, p < 0.001].
Pairwise comparisons of the mean differences for the pretreatment period and for the Ayurvedic treatment period showed that all mean differences are significant (Table 4), except the pretreatment difference for blood urea due to insufficient data for TP −6. Please note that for TP −6 only from 26 patients, the blood urea values could be procured. This explains why the above results for blood urea did not differ significantly between the three TPs.
The Disease Progress During the Pretreatment Period and the Effect of the Ayurvedic Treatment on the Disease Process
Pairwise comparisons of the mean differences for the pretreatment period (TP 0 and −6) and for the Ayurvedic treatment period (TP 0 and +6).
Time 0 = baseline (TP 0 = starting point of the Ayurvedic treatment).
Time −6 (TP −6 = 6 months before starting the Ayurvedic treatment) and time +6 (TP +6 = after 6 months of Ayurvedic treatment).
eGFR, estimated glomerular filtration rate; TP, time point.
The related-samples Friedman's two-way ANOVA by ranks with the Bonferroni correction for multiple tests showed that all above pairwise comparisons of the distributions of the various RFTs are significantly different. This includes blood urea.
The effects of the Ayurvedic treatment on signs and symptoms are shown in Table 5. The medians for swelling, nausea/vomiting, weakness, and breathlessness improved significantly during 6 months of Ayurvedic treatment.
Effects of the Ayurvedic Treatment on Signs and Symptoms in Chronic Renal Failure Patients
TP, time point.
The number of patients for each CRF stage for the three TPs (asymptotic significance p < 0.001) are depicted in Table 6. Ten patients with stage V at baseline shifted to lower stages. After 6 months of Ayurvedic treatment, five patients reached stage III and one patient even stage II.
Number of Patients with Various Chronic Renal Failure Stages at Various Time Points
CRF, chronic renal failure; TP, time point.
The bias-corrected effect sizes with 95% CI after 6 months of Ayurvedic treatment are as follows: eGFR: 0.45 (95% CI 0.06–0.84); serum creatinine: 0.53 (95% CI 0.13–0.92); blood urea: 0.44 (95% CI 0.05–0.83); and hemoglobin: 0.30 (95% CI −0.08 to 0.69). These effect sizes are interpreted as medium effects.
Discussion
This quasi-experimental pilot study with one group pre- and postdesign and two premeasurements reports clinical correlates and outcomes of a complex oral and proctocolonic Ayurvedic multiherbal regimen in 52 confirmed stages IV–V patients with CRF. The main findings of this study are as follows: A significant progress of CRF could be observed in all patients within the 6-month pretreatment period despite taking antihypertensive, antihyperglycemic, and/or diuretic conventional therapy, prescribed by nephrologists. On average, 8.6% less blood was “cleaned” by the kidneys at the end of this period. In 48% of the patients, the CRF staging also worsened during this period. After 6 months of Ayurvedic treatment, the progress of the disease could not only be stopped, but a statistically significant improvement of the mean values of eGFR, serum creatinine, blood urea, and hemoglobin was observed. On average, 4.1% more blood was “cleaned” by the kidneys, a result which was again statistically and clinically significant. The medians of swelling, nausea/vomiting, weakness, and breathlessness improved significantly after 6 months of Ayurvedic treatment. In 31% of the patients, the CRF stage improved after 6 months of Ayurvedic treatment. Only 1 of the 52 patients changed to a worse stage.
On the ground of these findings, it may be inferred that Ayurvedic treatment seems to decelerate the CRF disease progress.
According to Ayurvedic rationales, CRF can be considered as a disease of mūtra-vaha-srotas (urine forming channels). Although all the three doṣas (three Ayurvedic functional principles, i.e., vāta, pitta, and kapha that govern all bodily functions) as well as all the dūṣyas (pathologic bodily formations) are involved in the disease, vāta and kapha doṣas are more dominant in creating pathologies in the kidneys by their rūkṣa (dry), khara (rough), guru (heavy), and kaṭhina (hard) properties. Kapha may be considered to be responsible for blocking microvessels and developing microangiopathy, whereas vāta governs degeneration processes and hardening of kidney structures.
In CRF, multiple dhātus (primary body components), upadhātus (secondary body components), and malas (nonessential components and waste products) are involved as dūṣyas (pathologic bodily formations). Hence, all CRF patients suffer from avara-sāra (lower quality of body components). Initially, minor damages in the kidneys can be compensated by the remaining healthy nephrons. However, a continuous burden damages the nephrons further and progresses dysfunctions of the kidneys, which finally may lead to ESRD. According to Ayurvedic principles of the management of this disease, tissue damages can be prevented and repaired by rasāyana (tissue regeneration) measures. 17 Rasāyana medicines have the capability to improve the qualities of tissues and hence increase their resistance toward the disease. 18 Specific rasāyanas for the mūtra-vaha-srotas (channels or system related to the formation and transportation of urine) were chosen to improve the functional capacity of the remaining healthy nephrons and also to prevent their further damage. Especially, Rasāyana-cūrṇa is a preparation, which acts as a rasāyana for mūtra-vaha-srotas.
Nirūha-basti (proctocolonic administration of Ayurvedic medicine) was administered with the intention to eliminate accumulated mala (waste products) from the body. 19 From the Ayurvedic perspective, nirūha-basti is not only capable of removing mala (waste products) from the intestines but also supports the elimination of other malas and also the doṣas from all over the body. 20 The term mala used in the mentioned reference implies both the stool and morbid body components. 21 Thus, waste products, which are not eliminated by the diseased kidneys, may be eliminated through this therapeutic process.
Furthermore, if tubular structures are hampered in their functions, according to Ayurveda, existing blockages can be removed by lekhana (scraping) medication, which exerts a “scraping” effect on blocked channels. Gokṣurādi-guggulu (classical Ayurvedic compound) is considered to be a rasāyana for mūtra-vaha-srotas and also displays lekhana (scraping) effect, which primarily can be related to Guggulu (Commiphoramukul). 22 Varuṇādi-kvātha relieves both kapha and meda, 23 which are mainly responsible for the pathogenesis of CRF according to Ayurveda.
In conventional medicine, diabetes mellitus is considered to be the main cause of CRF. However, hypertension and chronic nephritis were found as major causes in this study. Weight loss, uncontrolled blood pressure, and low hemoglobin levels were present in most of the study patients. These factors may be the reason, why the disease progress was faster than commonly expected.
Limitations
This study has the limitations inherent to a quasi-experimental pilot study with a one group pre- and postdesign. In general, it could be inappropriate to ascribe the improvements in the outcome measures solely to the study interventions since there might be other possible explanations, such as maturation or the regression to the mean phenomenon. However, the probability of other reasons than the effects of the Ayurvedic therapy for the improvements seems to be low. In our study, we have the pretreatment period that is as similar as possible to the Ayurvedic treatment period in terms of baseline characteristics. For the 6-month pretreatment period, we had a progress of the disease, whereas in the 6-month Ayurvedic treatment period, we observed significant improvements.
Regular follow-ups during the outdoor treatment period would have been desirable to better contextualize the results of this study and for planning future randomized trials in other hospital settings. However, many of the research participants lived very far from our hospital and were thus not able to return for long-term follow-up assessments on fixed intervals.
Although parameters related to the individuality of the patient (e.g., the physical and mental constitution = prakṛti) are useful for a detailed understanding of a patient case from the Ayurvedic point of view, in this study, such assessments were not documented. In severe disease conditions, these factors are overshadowed by the intense symptomatology of the disease ( = vikṛti). Therefore, an assessment of these patient-related parameters would not have been accurate and also would have to be considered as clinically much less important than the symptoms.
Another limitation of the study might be seen in the age-related inclusion criteria. Patients older than 60 years were excluded from the study since age-related factors can strongly interfere in the disease process of CRF and therefore could have influenced the results of this pilot study.
Conclusions
The Ayurvedic treatment used in this study seems to have positively influenced renal functions by improving eGFR as well as by reducing serum creatinine values in comparison to the values before the Ayurvedic treatment. Quality of life also improved, facilitated by a significant reduction in signs and symptoms. Hence, the Ayurvedic treatment analyzed in this study may reduce the disease progress of CRF and may postpone renal transplant as well as the need of dialysis. Ayurvedic treatment may be a valuable addition to conventional medicine. However, larger and confirmatory randomized controlled trials are warranted to support the preliminary findings from this study.
Footnotes
Acknowledgments
The authors are thankful to the management of the J. S. Ayurveda College and P. D. Patel Ayurveda Hospital, Nadiad, for providing the permission and the facilities for this study. The authors are also grateful to all medical officers and the deputy superintendent of the hospital for their support in the clinical management of the patients.
Disclaimer
The institutes, which performed this study, belong to a charitable organization engaged in health and education services in the region. The medications used in this study are common classical Ayurvedic recipes (open access); they are not branded products of any company.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.