
Abstract
Objectives:
This pilot study aimed to compare the efficacy of manual pressure release (MPR), strain counterstrain (SCS), and integrated neuromuscular inhibition technique (INIT) in the management of chronic nonspecific low back pain (LBP).
Design:
Single-blind, randomized, controlled pilot trial.
Setting:
Neurosurgery clinic.
Subjects:
Forty-eight patients (46 women; mean age, 35.47 ± 10.58 years) diagnosed chronic nonspecific LBP and who had at least one active myofascial trigger point (MTrP) in the quadratus lumborum, iliocostalis lumborum, gluteus maximus, gluteus medius, and gluteus minimus muscles were included.
Interventions:
Patients received a standard home exercise program in addition to the MPR technique (MPR group), SCS technique (SCS group), and INIT (INIT group) for 12 sessions (2 days/week for 6 weeks).
Outcome measures:
The primary outcome was the visual analog scale (VAS). The secondary outcomes were MTrP examination, pressure pain threshold, lumbar active range of motion, Oswestry Disability Index (ODI), Beck depression inventory, and state-trait anxiety inventory.
Results:
There is no significant difference in terms of the percentage of deactivated MTrPs after 1st session and 12th session between groups (p > 0.05), but the percentage of deactivated MTrPs was less in MPR group than other groups. The overall group-by-time interaction for the repeated measures analysis of variance was not significant for primary and secondary outcomes (p > 0.05), but the improvement in the VAS-activity and the ODI was slightly better in the SCS group compared with other groups.
Conclusions:
These preliminary findings, which might help provide a glimpse into the clinical effectiveness of three manual therapy techniques (MPR, SCS, and INIT) rather than statistical significance, indicated that SCS or INIT might provide slightly better improvement in pain during activity, deactivation of MTrPs, and disability related to pain in chronic nonspecific LBP.
Introduction
Nonspecific low back pain (LBP) is usually defined as pain, muscle tension, or stiffness localized below the costal margin and above the inferior gluteal folds. 1 Recurrent episodes (lasting more than 3 months) are common presentations of nonspecific LBP usually accompanied by limitation of movement, long-term disability, and decreased quality of life. 2 Besides, the presence and experience of nonspecific LBP could be affected by psychosocial factors, including anxiety and depression. These factors strongly influence the pain intensity during activity and degree of disability in patients with chronic nonspecific LBP. 1 –3
The recognition of soft tissue as a pain generator in chronic LBP is not a new concept, and recently, a paradigm shift in the evaluation and treatment of LBP toward a greater focus on soft tissue causes of pain was called for. 4 A myofascial trigger point (MTrP), which defined as a hypersensitive spot in a taut band of a skeletal muscle that is painful on contraction, stretching, or stimulation of the muscle and elicits a referred distant pain, is one mechanism responsible for the clinical presentation of nonspecific LBP. 5 However, understanding the specific etiology of chronic nonspecific LBP remains elusive because it results from a variety of factors that can interact with each other.
Few studies have examined the role of MTrPs in the etiology and maintenance of LBP. A recent study pointed out that MTrPs in quadratus lumborum and gluteus medius muscles were identified in 48 (85.7%) patients. 6 Besides, Iglesias-González et al. indicated that active MTrPs in the quadratus lumborum, iliocostalis lumborum, and gluteus medius muscles were the most prevalent in patients with nonspecific LBP, and also a greater number of active MTrPs was associated with higher pain intensity. 7
Manual therapy is a nonpharmacologic intervention implemented to reduce pain and address the consequences of long-term nonspecific LBP caused by MTrPs. Manual pressure release (MPR), strain counterstrain (SCS) or positional release technique, muscle energy technique (MET), and integrated neuromuscular inhibition technique (INIT) are utilized for the treatment of nonspecific LBP in addition to patient education, graded physical activity, and exercise. 8 –10
There is some evidence demonstrating that the treatment of active MTrPs with the abovementioned manual therapy techniques was effective for reducing symptoms in patients with LBP. 11 –13 However, most of these treatment methods lack evidence regarding their efficacies for deactivating MTrPs, reducing pain, and increasing mobility. Therefore, there is a need to develop that which are more effective interventions for nonspecific LBP caused by MTrPs. This pilot study aimed to compare these three manual therapy techniques (MPR, SCS, and INIT) and to determine the efficacy of each therapy for treating chronic nonspecific LBP resulting from the active MTrPs.
Methods
Participants
This study was a single-blind, randomized, controlled pilot trial with a parallel design in which patients diagnosed with chronic nonspecific LBP at the Ministry of Health Haseki Training and Research Hospital were recruited between February 2017 and February 2018 (Supplementary Table S1). The protocol was approved by the Clinical Research Ethics Committee of Istanbul Training and Research Hospital (Approval Number: 893). Before being included in the study, patients gave written informed consent to participate. The protocol conformed to the standards for human experiments set by the Declaration of Helsinki.
Inclusion requirements were subjects who were aged between 18 and 65 years, presenting chronic nonspecific LBP between bottom of ribs and buttock creases, having LBP problem that has persisted at least 3 months and has resulted in pain on at least half the days in the past 6 months, and diagnosed with at least one active MTrP in quadratus lumborum, iliocostalis lumborum, gluteus maximus, gluteus medius, and gluteus minimus.
Exclusion criteria were having LBP with a specific underlying pathology such as a malignancy, vertebral fracture, infections, disc herniation, spinal stenosis on magnetic resonance imaging, presence of any rheumatologic conditions or systemic conditions, signs consistent with nerve root compression, having indications for referral for low back surgery, advanced osteoporosis, and psychiatric disorders, cognitive impairment, or dementia. Subjects that were treated for myofascial pain at the time of the study and received anti-inflammatory, pain relief, or medication for arthritic were also excluded.
A total of 48 participants were recruited into this exploratory pilot study because it has been previously indicated that obtaining ∼10 participants per group could be sufficient to specify meaningful group differences in pilot studies. 14 Participants were randomly assigned to one of three parallel groups to receive MPR or SCS or INIT (ratio 1:1:1). “Research Randomizer,” which is an online randomization web service, was used to allocate the participants. The simple randomization procedure was used to randomize eligible participants.
An investigator had administered the list without clinical involvement in the study. The participants were allocated to study groups based on a selected sealed opaque envelope by each participant. The initial examination was performed by neurosurgery specialist (M.A.A.), and outcome assessments were made by a physiotherapist (E.K.M.). The interventions were applied by another physiotherapist (I.O.D.), while all data analyses were performed by an investigator (T.B.) who was blind to allocation.
Outcome measures
The primary outcome was pain intensity during activity. The secondary outcomes were MTrP examination, pressure pain threshold (PPT), lumbar active range of motion (AROM), disability-related to pain, and presence of the depression and anxiety symptoms. MTrP assessment was performed at baseline, after 1st session, and 12th session. Other outcome measures were assessed at baseline and repeated after the 6-week intervention.
Participants were initially examined by a neurosurgery specialist to determine if the participants had exclusion criteria that prevent a person from participating. Ten years experienced physiotherapist has performed MTrP assessment bilaterally to localize MTrPs in the quadratus lumborum, iliocostalis lumborum, gluteus maximus, gluteus medius, and gluteus minimus muscles. During the examination, MTrPs were considered as active when the following criteria were met: (1) presence of a palpable taut band in the muscle, (2) presence of a hyperirritable spot in the taut band, (3) local twitch response elicited by the snapping palpation of the taut band, and (4) reproduction of participants' pain upon palpation with patient recognition of the symptom as familiar. These criteria, when applied by a trained assessor, have shown excellent interexaminer reliability ranging from 0.84 to 0.88. 15
Pain intensity was measured using the visual analog scale (VAS). The participants were asked to indicate their perceived pain at rest, during activity, and at night on the 10 cm line between no pain and terrible pain. 16 The minimal clinically important difference (MCID) value was proposed as 1.5–2.0 cm for VAS in patients with LBP. 17
The PPT of every active MTrP was measured using an electronic digital algometer (Baseline Push-Pull Force Gauge®; Fabrication Enterprises, Inc.), and pressure measurements were expressed in a kilogram-force per centimeter square (kg/cm2). Three repetitions were performed in each active MTrP site, and then the mean of the three trials was calculated for analysis. A 30-sec resting period was allowed between each test. Several studies have indicated that PPT assessment has high intraexaminer and interexaminer reliability (intraclass correlation coefficient [ICC] = 0.80–0.97). 15,18
The AROM, including lumbar flexion, extension, and right and left lateral flexion, was measured with BROM II device, which has ICCs in the range of 0.67–0.94 (Performance Attainment Associates, Roseville, MN). Three repetitions were performed in each direction and the average value recorded for analysis. 19,20 It was found that the 95% confidence limits of agreement between the first and the second measurements were greater than 5° for lumbar flexion and extension and less than 5° for right and left lateral flexion and rotation. 20
Disability related to pain was assessed using the Oswestry Disability Index (ODI), which is divided into 10 sections to assess the level of pain and interference with several physical activities, including sleeping, self-care, sex life, social life, and traveling. Each question is scored on a six-point scale. Ratings are summed to yield a score ranging from 0 to 50 where the higher scores indicate an increased degree of disability related to pain. 21,22 The MCID value was found as 12.88 points (sensitivity 88% and specificity 85%) for ODI. 23
Depression symptoms were measured by the Beck Depression Inventory (BDI). It comprises 21 items, each of which is rated between 0 and 3 on a 4-point Likert scale. The total score ranges from 0 to 63 points, with higher scores indicating greater depression. 24,25 The MCID value was found as a 29.64% reduction in scores from baseline for BDI in chronic pain population. 26
Anxiety symptoms were assessed by the State-Trait Anxiety Inventory, which has two subscales: The State Anxiety Scale (S-Anxiety) which evaluates the current state of anxiety and The Trait Anxiety Scale (T-Anxiety). It comprises 40 items, each of which is rated between 1 and 4 on a 4-point Likert scale. The sum of the item scores produces the subscale total scores ranging from 20 to 80 points, with higher scores indicating greater anxiety. 27,28
Interventions
All participants received a standard home exercise program in addition to the MPR technique (MPR group), SCS technique (SCS group), and INIT (INIT group) in the order dictated by their treatment group (Fig. 1). The participants attended their treatment programs, consisting of one of the three manual therapy techniques, 2 days/week for 6 weeks at the clinical setting.
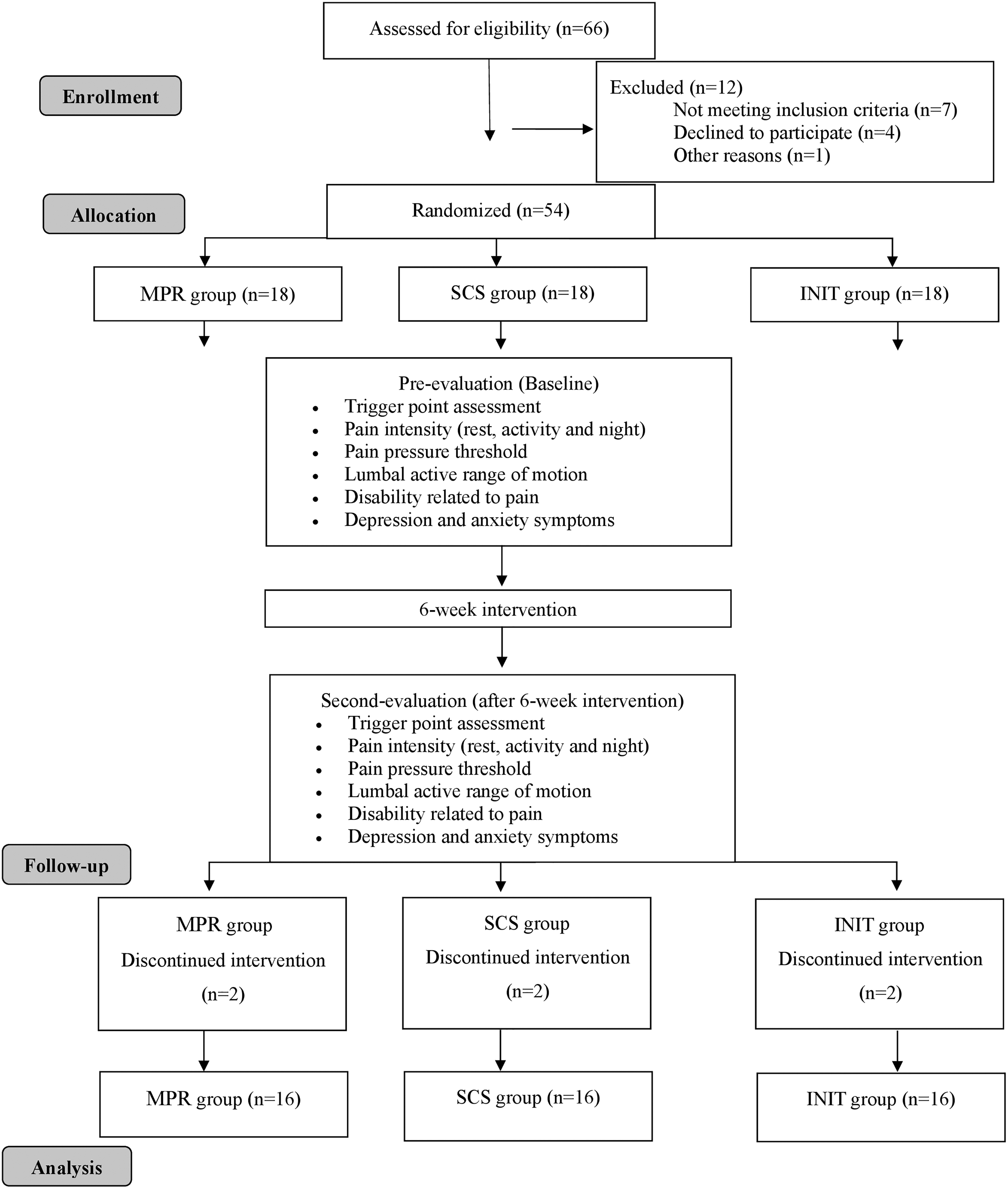
Design of the study (CONSORT flow diagram).
For the MPR intervention, the therapist utilized a slow pressure directly over a specific MTrP using flat palpation. The pressure was maintained until a release of the tissue barrier was felt and the pain was reduced. At that time, the pressure was again applied until a new barrier was felt. This procedure was performed for 90 sec and repeated three to five times per treatment session with a rest interval of 30-sec duration in between. 29
For the SCS intervention, the therapist asked participants to consider that their initial MTrP tenderness was “10” on a verbal scale where “0” represented no tenderness after MTrP was localized. Then, the therapist applied gradually increasing pressure to the MTrP until the sensation of pressure became one of pressure and pain. At that moment, the position of ease, which was defined as the point with a reduction in pain of at least 70%, was produced.
The position of ease was often produced by positioning the muscle in a shortened/relaxed position. Both perceived tissue tension and the patients' reported tissue tenderness upon intermittent probing were used to guide the therapist to the appropriate relieving position at MTrP before being slowly and passively returned to a neutral position. This position was maintained passively for 90 sec. The same maneuver was repeated three to five times per treatment session with a rest interval of 30-sec duration in between. 18
For the INIT intervention, multiple techniques were performed in the following sequence: (1) MPR, (2) SCS, and (3) MET. Once the MTrP was identified, MPR was started and followed by SCS. MET began after finishing SCS. The MPR and SCS were applied, as mentioned above. The MET was directed toward the involved muscle, and the isometric contraction of affected muscle was held for 7–10 sec. Following the contraction, the therapist applied the stretching to initiate a local tissue stretch in the tissues in which the TrP was located. Each stretch was held for 30-sec and was repeated three to five times per treatment session. 30
All participants received a standard home exercise program as recommended by clinical practice guidelines. 31 The home program consisted of straight leg raise, bridge exercise, lying down bicycle exercise, prone hip extension exercise, and abdominal curl exercise. All participants were encouraged to exercise at least five times a week, two times a day with 10 repetitions, and they were questioned about the adherence to the prescribed home exercise program within the previous week.
Statistical analyses
The Statistical Package for the Social Sciences 21.0 (SPSS, Inc., Chicago, IL) for Windows software was used for all statistical analyses. Before the statistical analyses, the Kolmogorov–Smirnov test was used to assess the distribution of data. Demographic data and clinical baseline variables were compared among the three groups by one-way analysis of variance for continuous variables and Chi-squared test for categorical variables. The percentage of deactivated MTrPs (absent or present) from baseline to 1st session and baseline to 12th session was compared among the three groups (MPR, SCS, and INIT) by the Chi-squared test. The effect of the interventions on PPT was analyzed on the most painful MTrP in the right or left quadratus lumborum, iliocostalis lumborum, gluteus maximus, gluteus medius, and gluteus minimus muscles.
Repeated measures analysis of variance (rANOVA) was conducted with time (baseline and after the 6-week intervention) as a within-subject variable and group (MPR, SCS, and INIT) as a between-subject variable to analyze the effect of the interventions on the primary and secondary outcomes. Partial eta squared was used as an indicator of effect size, which is elucidated as small 0.01; medium 0.06; and large 0.14. 32 The significance level was set at p < 0.05. The least significant difference post hoc test was used with a Bonferroni correction if differences among the means were determined.
Results
Sixty-six patients were screened for possible inclusion. A total of 18 patients were excluded due to various reasons; a total of 16 patients were randomized to the MPR group, while 16 patients were randomized to the SCS group with 16 randomized to the INIT group. All participants regularly attended their treatment programs 2 days/week for 6 weeks at the clinical setting. All participants have indicated that they performed a home exercise program exactly as prescribed at least five times a week, two times a day with 10 repetitions; please see the CONSORT diagram (Fig. 1). The average time between randomization and initiation of the intervention was 3–5 days for each participant. None of the participants reported an adverse effect during the 6-week intervention.
The demographic and clinical baseline variables of the participants are presented in Table 1. At baseline, there were no significant differences between groups for any sociodemographic and clinical variables of the participants (p > 0.05). The total percentage of active MTrPs at baseline and the percentage of deactivated MTrPs after 1st session and the 12th session are shown in Table 2. There is no statistically significant difference in terms of the percentage of deactivated MTrPs after 1st session and 12th session between groups (p > 0.05). The percentage of deactivated MTrPs in both after the 1st session and 12th session was less in the MPR group than in other groups. The overall group-by-time interaction for rANOVA was not significant for pain intensity, pain pressure threshold, AROM, ODI, and psychologic factors (p > 0.05) (Tables 3 and 4).
Sociodemographic and Clinical Variables of the Participants
The variables are expressed as mean ± standard deviation.
One-way ANOVA; significance level set at <0.05.
Chi-squared test; significance level set at <0.05.
ANOVA, analysis of variance; BDI, beck depression inventory; BMI, body mass index; INIT, integrated neuromuscular inhibition technique; LBP, low back pain; MPR, manuel pressure release; ODI, Oswestry disability index; SCS, strain counterstrain; STAI, state-trait anxiety inventory; VAS, visual analog scale.
The Percentage of Active Myofascial Trigger Points at Baseline and the Percentage of Deactivated Myofascial Trigger Points After 1st Session and 12th Session
The variables are expressed as number (percentage).
Chi-squared test; significance level set at <0.05.
INIT, integrated neuromuscular inhibition technique; MPR, manuel pressure release; SCS, strain counterstrain.
Comparison of Pain Intensity and Pain Pressure Threshold Between Groups
rANOVA; significance was accepted as p = 0.05/2 = 0.025 after Bonferroni correction.
CI, confidence interval; INIT, integrated neuromuscular inhibition technique; MPR, manuel pressure release; PPT, pressure pain threshold; rANOVA, repeated measures analysis of variance; SCS, strain counterstrain; SD, standard deviation; VAS, visual analog scale.
Comparison of Active Range of Motion, Oswestry Disability Index, and Psychological Factors Between Groups
rANOVA; significance was accepted as p = 0.05/2 = 0.025 after Bonferroni correction.
BDI, beck depression inventory; CI, confidence interval; INIT, integrated neuromuscular inhibition technique; MPR, manuel pressure release; ODI, Oswestry disability index; SCS, strain counterstrain; SD, standard deviation; STAI, state-trait anxiety inventory; VAS, visual analog scale.
After the 6-week intervention, improvement in the mean VAS-activity score was slightly better in the SCS group (4.50 ± 1.78) compared with the MPR group (3.00 ± 1.67) and INIT group (3.00 ± 1.67) (p = 0.26). In addition, the SCS group (25.0 ± 12.08) has a slightly better improvement in the mean ODI score compared with the MPR group (19.25 ± 9.32) and INIT group (22.25 ± 10.24) (p = 0.36) (Tables 3 and 4).
Discussion
The preliminary findings of this pilot study, which might help provide a glimpse into the clinical effectiveness of three manual therapy techniques (MPR, SCS, and INIT) rather than statistical significance, showed that improvement in pain intensity, PPT, AROM, disability related to pain, depression, and anxiety was similar between groups after 6-week intervention. However, the improvement in the pain intensity during activity and the disability related to pain was slightly better in the SCS group compared with other groups. In addition, the percentage of deactivated MTrPs was less in the MPR group than in other groups after the 1st session and 12th session.
Takamoto et al. found that compression at MTrPs is effective in treating acute LBP in terms of VAS score for pain intensity, PPT, and range of motion compared to compression at non-MTrPs and superficial massage. 12 Similarly, their findings showed that the magnitude of improvement in pain intensity during activity was clinically important in all groups after a 6-week intervention, as noted by within-group differences in VAS, which were greater than the MCID of 2 cm. 17 In addition, the magnitude of improvement in disability related to pain and depression symptoms was clinically important in all groups after a 6-week intervention, as noted by within-group differences in ODI and BDI, which were greater than the MCID of 12.88 points and a 29.64% reduction, respectively. 23,26
Several studies investigating SCS indicated that it appears effective in reducing palpation tenderness and clinical pain for trapezius and masseter MTrPs, but disability might not be improved. 33 In the present study, the SCS group showed relatively better improvement of pain intensity during activity and disability related to pain with a small effect size compared to the other groups. However, it should be noted that SCS was not superior to MPR or INIT in terms of overall improvements in chronic nonspecific LBP.
A randomized controlled study examining the short-term effects of SCS treatment on quantitative sensory measures at digitally tender points in the low back found that SCS intervention elicited an increase in PPT (reduction in MTrP tenderness), which is consistent with their findings. 34 The possible physiologic mechanisms explaining the effect of SCS include abnormal neuromuscular activity mediated by muscle spindles and local circulation or inflammatory reactions influenced by the sympathetic nervous system, but how SCS affects the body remains unclear. 35 In contrast, the evidence about performing SCS with exercise or alone is conflicting. Lewis et al. pointed out that the SCS combined with exercise is not more effective than exercise alone on pain and disability in patients with acute LBP. 36
All participants have indicated that they performed a home exercise program exactly as prescribed at least five times a week, two times a day with 10 repetitions in their study. Therefore, the home exercise intervention in this clinical trial might have a strong independent treatment effect. Since the independent treatment effect of the home exercise program might have masked the primary treatment effect of three manual therapy techniques (MPR, SCS, and INIT) on chronic nonspecific LBP, their findings should be considered within the context of the limitations of the study design.
Surprisingly, INIT intervention consisting of MPR, SCS, and MET application in the order was not found more effective than MPR and SCS interventions in the present study. The result of a recent study indicated that INIT applied to upper trapezius MTrP led to significantly greater improvements in pain and neck disability and lateral cervical flexion AROM than MET in patients with nonspecific neck pain. 37 MET, which is a commonly utilized method for decreasing tonus in a muscle before stretching, was a major difference between the interventions used in the present study because it has been hypothesized that the sequence of mechanoreceptor activation arouses firing of local somatic efferent.
Thanks to the stimulation of mechanoreceptors, simultaneous gating of the nociceptive impulses occurs in the dorsal horn of the spinal cord, which plays a role in the descending pain modulation. 38 Besides, a systematic review investigating the effect of MET in reducing pain and improving function in patients with LBP found minimal evidence that MET reduces pain and disability scores in individuals with acute LBP consistent with their findings. 13
The percentage of deactivated MTrPs after 1st session and the 12th session was higher in patients who received SCS or INIT than those that received MPR. Because an active MTrP in the quadratus lumborum, iliocostalis lumborum, and gluteus medius muscles might be implicated in the genesis and maintenance of nonspecific LBP, it is legitimate to an association between a greater number of active MTrPs and higher pain intensity. 6,7 Thus, the percentage of deactivated MTrPs is a clinically significant outcome. Wong emphasized that SCS is useful for preparing tissues for other techniques such as joint manipulation, soft tissue mobilization, stretching, or strengthening exercises. 35 In their opinion, exercise or functional training should be combined with SCS or INIT to deactivate the MTrPs, thereby providing pain relief and preventing disability related to pain.
To their knowledge, this is the first study to compare the effect of three manual therapy techniques on pain intensity, PPT, AROM, disability, depression, and anxiety in patients with chronic nonspecific LBP. Besides, most of the studies conducted at chronic nonspecific pain resulting from MTrP have included the patient with latent MTrPs, but the present study has included patients with active MTrPs. However, this study has some limitations that should be highlighted.
First, assessment of outcome measures was performed at baseline and after the 6-week intervention, but there is no follow-up period. Second, this study was intended to be a pilot for a future study, so its sample size is relatively small, which might lead to Type II errors; therefore, its findings should be interpreted with caution. Third, different results could be obtained if the authors have used any outcome measures, which are reliable in the evaluation of adherence to home exercises, but the authors have to believe their declaration of compliance. Finally, 100% compliance with the home exercise program might have caused the confounding treatment effect of the MPR technique, SCS technique, or INIT.
Conclusions
This randomized controlled pilot trial demonstrates that the three manual therapy techniques (MPR, SCS, and INIT) as MTrP therapy have a similar effect on pain intensity, PPT, AROM, disability related to pain, depression, and anxiety in patients with chronic nonspecific LBP. Beyond statistical significance, clinical interpretation of these findings supports that SCS or INIT might provide slightly better improvement in pain during activity, deactivation of MTrPs, and disability in chronic nonspecific LBP. In addition, it should be taken into consideration that all three techniques, which are low-cost methods, could be used in patients with nonspecific LBP induced by an active MTrP. Further studies with a larger sample size are required to investigate the primary treatment effect of these three manual therapy techniques in patients with chronic nonspecific LBP induced by an active MTrP.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The present work was supported by the Scientific Research Projects Coordination Unit of Istanbul University (Project No.: 24209).
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.