
Abstract
Background:
Blood pressure (BP) after a stroke is affected by autonomic regulation, the Cushing reaction, and basal history of hypertensive, arteriosclerotic conditions. To prevent recurrent stroke attack and its complications, BP must be regulated to within the normal range through monitoring, rest, and medication. Previous studies have reported that acupuncture may be effective in lowering BP in patients with hypertension.
Objectives:
This study was aimed at evaluating the efficacy of acupuncture in regulating BP in stroke patients, including both cerebral infarction and hemorrhage.
Methods:
A review was conducted of articles published in English, Korean, Chinese, and Japanese across 16 electronic databases (Pubmed, EMBASE, Cochrane Central Resister of Controlled Trials, AMED, CINAHL, CNKI, Wanfang, VIP, CiNii, and seven Korean databases) up to April 2020. Only randomized controlled trials that evaluated the efficacy of acupuncture for stroke patients were included and meta-analyzed, and BP data and risk of bias were extracted by scanning the full texts. Data analysis was performed by using RevMan 5.3.
Results:
From the 16 electronic databases, 7623 relevant articles were identified, and 847 stroke patients of 10 trials met the inclusion criteria. Two trials reported that BP was lowered more in the group who had received acupuncture treatment than the group who were treated with conventional medication. Two trials reported that BP was lowered after auricular acupuncture treatment more than those observed in the group receiving conventional medical treatment. Six trials reported that BP in cerebral infarction patients was lower than in the control group. None of the trials reported any adverse events.
Conclusions:
It was concluded that acupuncture may be a suitable treatment option for regulating BP after stroke. However, the trials are not free from bias. Further reviews would yield positive results if well-designed trials are conducted.
Introduction
Stroke, or cerebrovascular accident, is defined as the condition caused by interruption of the blood supply to the brain tissue, such as by a burst blood vessel or blockage by a clot 1 Since the mortality and neurological deficits caused by such lesions are tremendous, primary supportive care and patient monitoring, including blood pressure (BP) assessment, is crucial in the medical treatment of stroke patients. Hypertension is a major risk factor for stroke, and elevated BP is observed in up to 75% of acute stroke patients due to multiple reasons. It is known to be mediated by prior hypertension, neuroendocrine stimulation via the renin-angiotensin-aldosterone system, the autonomic nervous-corticotrophin-cortisol system, the Cushing reflex due to increased intracranial pressure, and stress responses to other medical conditions such as pain or emotion. 2 Whether or not BP control after acute stroke attack would be beneficial to the patient's prognosis has been the subject of debate. A fall in BP below the normal range is associated with the recurrence of ischemic stroke and acceleration of perihematomal ischemic damage. However, epidemiological reviews have shown that higher BP is associated with increased death rate and likelihood of functional dependency in stroke patients. 3
Conventional antihypertensive medications comprise oral or intravenous antihypertensive agents, including α-2 adrenergic receptor agonists, angiotensin-converting enzyme inhibitors, angiotensin II receptor antagonists, β-blockers, calcium channel antagonists, diuretics, magnesium, and nitric oxide. According to current clinical guidelines, the BP of acute ischemic stroke patients should be managed at below 220/120 mmHg: In cases of in acute kidney injury, aortic dissection, cardiac ischemia, hypertensive encephalopathy, and pulmonary edema, it should be regulated to 200/100 mmHg; in patients who have undergone thrombolytic therapy, it should be regulated to 185/110 mmHg. In hemorrhagic stroke patients, systolic BP (SBP) should be managed at below 140 mmHg. 1
Systematic reviews of acupuncture in patients with hypertension have been conducted in the past. Zhao et al. concluded that acupuncture is beneficial as adjunctive therapy with medication, but its efficacy as the sole mode of treatment remains doubtful. 4 There is insufficient evidence owing to the shortcomings of the methodology applied. 5,6 However, there has been no review evaluating the efficacy of acupuncture in regulating BP in stroke patients.
This review aims at evaluating the effectiveness of acupuncture for the regulation of stroke patients' BP, including patients who have suffered infarction or hemorrhage.
Methods
Criteria for considering studies for this review
The protocol of this review was registered in PROSPERO ID CRD42018092054 on April 3, 2018 (Archived at
Search methods for identification of studies
The following databases were searched: Pubmed, EMBASE, the Cochrane Central Resister of Controlled Trials (CENTRAL), AMED, CINAHL, CNKI, Wanfang, VIP, CiNii, and seven Korean medical databases (Koreantk, Oasis, RISS, DBpia, KISS, KISTI, NDSL), and all the searches ended in April 2020. The search terms included “Hypertension,” “Blood pressure,” “Stroke,” and “Acupuncture,” and others (Appendices A1–A5). We used search strategies to find related studies, and applied modified search formulae tailored to each database's characteristics.
Study selection
The studies were selected based on their eligibility and checked against the inclusion criteria. All randomized controlled trials (RCTs) were included in this review without restriction with regard to date of publication or language.
Inclusion criteria
Only RCTs that evaluated the effectiveness of acupuncture treatment by measuring BP in stroke patients were included. The patients had been diagnosed with stroke based on neurological deficit and brain imaging, and they were included irrespective of sex, age, race, country, or onset of stroke symptoms. All acupuncture types were included, such as conventional acupuncture, electroacupuncture, pharmacoacupuncture, auricular acupuncture, and acupressure, without any limitations on the number of acupoints, methods used, or duration of treatment. We determined that the control treatment would be any type of conventional therapy, placebo therapy, including sham acupuncture, conventional acupoints, and no treatment. Primary outcomes included SBP and diastolic BP (DBP), mean arterial pressure, change of BP, or a number of patients with significantly lowered BP after treatment. Secondary outcomes included adverse events and impact on quality of life. We excluded trials that were case reports, crossover designs, nonrandomized, noncontrolled, nonacupuncture therapy, such as moxibustion, herbal medication, negative cupping, or venesection.
Data extraction and management
The data were extracted by using a standard data extraction form that contains methodology, participants, intervention, and duration of treatment, outcomes, and conclusions.
Assessment of risk of bias in included studies
The risk of bias, as described in the Cochrane Handbook for Systematic Reviews of Interventions, was independently assessed. In terms of quality, the studies were categorized into low, unclear, or high risk of bias, according to the risk associated with each important outcome within the included studies, including adequacy of generation of the allocation sequence, allocation concealment, blinding, whether there were incomplete outcome data, and selective reporting of the results. Studies that met all criteria were categorized as having a low risk of bias, studies that met none of the criteria were categorized as having a high risk of bias, and studies that had insufficient information to make a judgment were categorized as unclear with regard to risk of bias.
Data analysis
Data analysis was performed by using RevMan 5.3 (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2016) software. Binary outcomes were summarized by using risk ratio (RR) with 95% confidence intervals (CI) for relative effect, and risk difference with 95% CI for absolute effect. The continuous outcomes were summarized by using mean difference (MD) with 95% CI. When there were sufficient data (with similar clinical characteristics, such as study design, participants, interventions, control, and outcome measures) and acceptable statistical heterogeneity, then the data were pooled and a meta-analysis using a random-effect model was performed, since it was supposed that the patients' BP levels would not be homogeneous across all trials.
Statistical heterogeneity was detected by I 2 test. Where an I 2 was between 50% and 75%, it indicated the possibility of statistical heterogeneity across the studies. Where I 2 was larger than 75%, clearly indicating statistical heterogeneity across the studies, the results from each individual study were presented, rather than pooled. Funnel plot analysis was planned for the detection of publication bias.
Results
Results of the search
From the 16 electronic databases, 7623 articles were identified (Fig. 1). After excluding duplicate studies and articles that did not meet the inclusion criteria, the full texts of 45 articles were retrieved and evaluated on the basis of the title and abstract. After browsing through these 45 articles, 35 articles were excluded (18 were not RCT, 17 did not discuss acupuncture). As a result, 10 trials were included for this review process and data analysis 7 –16 (Table 1).

PRISMA flow chart.
General Characteristics of Included Trials
Located above 2.5 cm from sternoclavicular joint, lateral 1.5cm from midline, T6 spinal transverse process.
C, control group; T, treatment group; DBP, diastolic blood pressure; HTN, hypertension; SBP, systolic blood pressure.
Characteristics of the included studies
A total of 847 stroke patients were included, of whom 15 patients had dropped out. Four trials included stroke patients without classification in terms of hemorrhage or infarction, stage or duration. Of the others, six trials included ischemic stroke patients, and one trial included hemorrhagic stroke patients. The mean sample size was ∼84 patients, but no trial reported the calculation sequence of the sample size. The duration of treatment ranged from 10 to 90 days.
Regarding the intervention type, eight trials applied acupuncture treatment by using conventional acupoints, whereas two trials applied auricular acupuncture treatment.
None of the trials used sham or placebo treatment for the control group. Six trials compared the acupuncture outcomes with those of conventional medication and care, whereas four trials compared them with treatment using other acupoints.
Outcome assessment
Regarding the outcome assessment, eight trials measured and reported BP at baseline and post-treatment. Two trials reported the response rates, without BP data. Five trials reported there were no adverse events, whereas the other five trials did not mention them at all.
Risk of bias of included studies
According to our predefined methodological quality criteria, all 10 trials were evaluated.
All 10 trials mentioned randomization, but three trials did not report generation of sequence, blinding, and seven trials did not report any drop-outs. All studies are suggested to have high risk of bias, because there was lack of blinding both patients and operators. None of the trials used placebo treatment, such as sham acupuncture or sham acupoints. This can result in the reporting of more positive data of practitioners or patients.
One trial mentioned drop-outs, but they excluded all data pertaining to dropped-out patients from the report. This trial was considered to have a high risk of attrition bias by not implementing the intention-to-treat analysis.
Publication bias is possibly present, since all trials were published in China, where the enrolled patients or practitioners are more favorably disposed toward acupuncture (Fig. 2A, B).

Risk of bias.
Meta-analysis: Therapeutic effects of the interventions
Acupuncture versus conventional medication
Patients who received acupuncture in the experimental groups showed lower BP, both systolic and diastolic, after treatment than those in the control group using conventional treatment (SBP: MD −6.14, 95% CI [−14.84 to 2.56], I 2 = 7%; DBP: MD −6.11, 95% CI [−12.21 to −0.01], I 2 = 0%) (Fig. 3A).
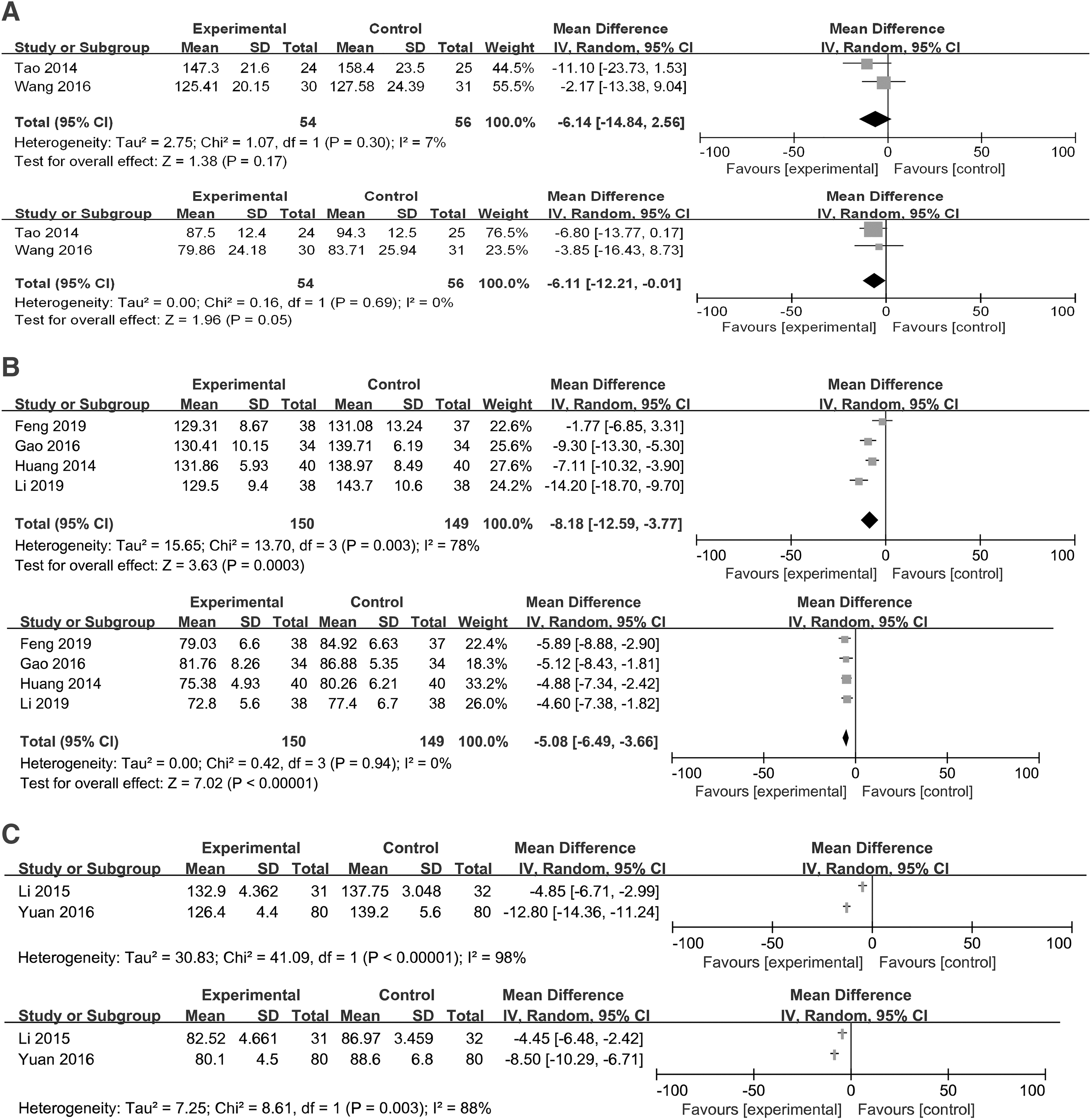
Forest plot of systolic and diastolic blood pressure with type of treatment.
Patients who received acupuncture in the experimental group exhibited more positive results in terms of their response rate, including lower BP, than those in the control group using conventional treatment (response rate: RR 1.15, 95% CI [1.05–1.26], I 2 = 0%).
Acupuncture versus conventional acupoints
Patients who received acupuncture in the experimental group exhibited lower BP, both systolic and diastolic, after treatment than those in the control group using conventional acupoints (SBP: MD −8.18, 95% CI [−12.59 to −3.77], I 2 = 78%; DBP: MD −5.08, 95% CI [−6.49 to −3.66], I 2 = 0%) (Fig. 3B).
Auricular acupuncture versus conventional medication
Patients who received auricular acupuncture in the experimental group exhibited lower BP, both systolic and diastolic, after treatment than those in the control group using conventional treatment.
Two trials showed statistical heterogeneity in their results, so meta-analysis and data synthesis were skipped (SBP: I 2 = 98%, DBP: I 2 = 88%) (Fig. 3C).
Meta-analysis: Type of stroke
Ischemic stroke
Ischemic stroke patients who received acupuncture in the experimental group exhibited lower BP, both systolic and diastolic, after treatment than those in the control group (SBP: MD −7.04, 95% CI [−10.29 to −3.80], I 2 = 75%; DBP: MD −4.86, 95% CI [−6.02 to −3.71], I 2 = 0%) (Fig. 4).

Forest plot of systolic and diastolic blood pressure of ischemic stroke patients.
Hemorrhagic stroke
Hemorrhagic stroke patients who received acupuncture in the experimental group exhibited lower BP, both systolic and diastolic, after treatment than those in the control group (SBP: MD −11.10, 95% CI [−23.73 to 1.53]; DBP: MD −6.80, 95% CI [−13.77 to 0.17]).
Only one trial by Tao treated hemorrhagic stroke patients. One hundred sixteen patients of small amount hematoma were included and received acupuncture for treatment group and conventional care for control group. After 12 h from the onset, the mean BP of patients who received acupuncture was lowered from 151.1/85.5 to 147.3/87.5 mmHg, whereas the mean BP of patients who received conventional treatment was raised from 152.7/83.6 to 158/94.3 mmHg. It suggests that BP, which can be significantly raised from baseline despite conventional treatment, would be maintained or regulated in the group who received adjuvant acupuncture treatment.
Heterogeneity
This review included 847 patients from 10 trials, but there was a degree of heterogeneity to the interventions (conventional acupuncture, auricular acupuncture), control treatment (conventional medication, other acupoints), and outcome measurements (BP, response rate). Therefore, a single conclusion based on all 10 trials could not be reached, but rather the conclusions were drawn for each treatment and outcome. This will undermine the reliability of the evidence that acupuncture is effective in regulating BP in stroke patients. By the statistical evaluation, SBP outcomes on the acupuncture trials and both BP outcomes on the auricular acupuncture trials showed clear statistical heterogeneity (I 2 > 75%) in their results.
Impaired data reporting
Seven trials reported only the mean BP of the final stage, and only one trial reported changes in BP, comparing both before and after treatment. Therefore, the extent to which BP was lowered by acupuncture treatment cannot be concluded by data synthesis on overall trials.
Two trials reported using their own scale-like response rate, but skipped reporting BP data, therefore providing only weak evidence of the effectiveness of acupuncture in lowering BP.
Adverse events
Five trials reported no adverse events resulting from acupuncture treatment, whereas the other five trials did not mention adverse events at all.
Discussion
The administration of acupuncture to stroke patients revealed similar or greater benefits in terms of antihypertensive effect and increased response rate with regard to BP, compared with conventional treatment. Therefore, we supposed that acupuncture would be a suitable treatment option for regulating BP in stroke patients, but owing to the following limitations, there is only relatively weak evidence to support this statement. As shown in the Figures, the effectiveness of acupuncture was not significantly remarkable compared with conventional medication. There were no trials that compared acupuncture's efficacy with a no-treatment control group, and therefore there is only relatively weak evidence to support the recommendation of acupuncture for regulating BP. However, when analyzed by stroke type, ischemic stroke patients showed significantly lower BP than did the control group, whereas hemorrhagic stroke patients did not.
From the perspective of traditional Korean medicine, BP is often associated with excessive syndrome of wind and heat (風證, 熱證) from the liver, heart, or kidneys (肝·心·腎). 17 The acupoints that are usually selected for hypertensive patients in previous RCTs were chosen with the aim of alleviating this pathology, by considering acupoints such as LR3(太衝), LI11(曲池), GB20(風池), ST36(足三里), LI4(合谷), SP6(三陰交), CV4(關元), and PC6(內關). 18 These acupoints were also selected for stroke patients in the trials included in this review, from the same aspect. Auricular acupuncture, which is administered based on the principle that the ears represent a microsystem of the entire body, is applied for various diseases based on the evidence of its efficacy. 19 The included trials selected auricular acupoints, such as depression (降壓點), shenmen (神門), heart (心), subcortex-cardiovascular system (皮質下-心血管系), liver (肝), adrenal gland (副腎), endocrine (內分泌), and sympathetic points (交感神經). These auricular acupoints are also associated with reducing excessive syndrome of wind and heat from the liver, heart, and kidneys.
Most of the trials did not report the changes in BP from baseline, but they rather reported the mean BP before and after treatment. Therefore, it was impossible to determine the degree to which BP dropped in response to acupuncture treatment, but it could only be concluded that BP after treatment was lower than among the control groups treated with conventional medication. In the interest of clinical application, further research should consider including data such as changes in BP during treatment.
Leem suggested that further research should measure patients' precise BP by using methods such as 24-h ambulatory blood pressure monitoring (ABPM). 18 As mentioned, the trials included in this review mostly measured morning BP, whereas only two studies 8,16 used ABPM. Since the BP of stroke patients is easily affected by their medical condition and treatment during the course of the day, measuring BP within a limited time zone may omit the data that reveal significant change.
Recently, several systematic reviews of acupuncture were conducted on patients with hypertension, but not on stroke patients. The reviews conducted by Leem 18 and Zhao et al. 4 suggested that the administration of acupuncture in combination with conventional medication revealed an additive effect in treating hypertension. They included a greater number of trials, but they could offer only limited conclusions because of biases. Auricular acupuncture, also termed ear acupuncture, is usually included in systematic reviews as a subtype of acupuncture that uses the auricular acupoints only. Zhao et al. included one trial of auricular acupuncture that reported no superior effects to those observed in the sham control group, despite the significant change in DBP. 4
We included 847 patients in 10 trials, but heterogeneity was present between the studies, in terms of design, interventions, control treatment, outcome, and statistical values. The number of patients prevent a single, holistic conclusion, but rather separate conclusions were reached for each treatment and outcome, undermining the reliable conclusion of acupuncture's effectiveness. We found clear heterogeneity (I 2 > 75%) on SBP outcomes of the acupuncture trials. It could be caused by out-liar, such as Feng's study, which treated with single additional acupoint (ST9) compared with the control group. Also, in the auricular acupuncture trials, there was obvious heterogeneity (I 2 > 75%) in their results, which could not form a single conclusion by meta-analysis.
None of the trials included placebo treatments, such as sham acupuncture or sham acupoints. This can lead to the reporting more positive data for practitioners or favorable reactions from patients. Publication bias is possibly present, since all the trials were published in China, where the enrolled patients or practitioners tend to be more favorable for acupuncture treatment.
The included trials mostly reported only the mean BP at the final stage, not changes in BP comparing both before and after treatment. The result was in a lack of conclusion regarding the extent to which BP will be lowered by acupuncture treatment. Two trials reported using their own scale-like response rates, but skipped reporting BP, therefore providing only weak and vague evidence of acupuncture's efficacy in lowering BP. Two trials reported using their own scale “response rate (臨床療效),” but they skipped reporting data of BP; therefore, they provide weak evidence to verify the effect of lowering BP.
Conclusion
The administration of acupuncture for regulating BP in stroke patients may be effective, compared with conventional medication, for both systolic and DBP, without the report of any adverse events.
No firm conclusions could be drawn, but rather the conclusion is vague, owing to limitations, such as the control treatment design and partial, insignificant results.
Further research is recommended to yield firm evidence for the efficacy of acupuncture in regulating BP in stroke patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research received no special grant from any funding agency in the public, commercial, or not-for-profit sectors.