
Abstract
Objectives:
To evaluate (1) the effect of a salivary substitute prepared using chamomile (Matricaria chamomilla L.) flower and flax (Linum usitatissimum L.) seed to relieve Primary burning mouth syndrome (BMS) symptoms, (2) their effect on the inhibition of matrix metallopeptidase 2 (MMP2) and MMP9 metalloproteinases, and (3) their potential cellular cytotoxic effect.
Subjects:
40 women aging >40 years with diagnosis of primary BMS.
Settings/Location:
Center of Diagnosis of Diseases of the Mouth, Federal University of Pelotas, Brazil.
Design:
This was an open clinical trial where primary BMS patients used the homemade salivary. At the first appointment, after 30 and 60 days, the authors evaluated the pattern and intensity of BMS and xerostomia symptoms, and then determined and compared the unstimulated salivary flow rate (SFR), viscosity, and salivary pH. MMP2 and MMP9 activities in saliva and cytotoxicity were assessed using different concentrations of chamomile flower and flax seed separately.
Interventions:
Subjects used the homemade salivary substitute for 3 months and were instructed to rinse their mouth three to four times daily for 1 min.
Outcome measures:
A numeric rating scale to evaluate the intensity of burning sensation and xerostomia symptoms, salivary flow rate (SFR) to determine salivary volume, dynamic rheology technique for viscosity and a digital meter for salivary pH. MMP2 and MMP9 activities in saliva and cytotoxicity were assessed by zymography and cell viability assay respectively.
Results:
After treatment, severity of BMS symptoms decreased, the SFR increased, salivary viscosity decreased, and severity of xerostomia sensation (in patients who reported having this symptom) improved (p < 0.05). Chamomile flower and flax seed had no effect on inhibiting MMP2 and MMP9 activities, and neither showed cellular cytotoxic effects.
Conclusion:
This homemade salivary substitute is an economical, viable, easily manipulated, noncytotoxic, and a practical alternative to relieve BMS symptoms.
Introduction
Primary burning mouth syndrome (BMS) is a chronic oral condition that significantly affects the patient's quality of life and is characterized by burning, dryness, and uncomfortable sensations in the mouth, without clinical alterations, or laboratory findings that justify these symptoms. 1 –4 Primary BMS must be differentiated from secondary BMS, which is caused by several etiological factors, ranging from local causes within the oral cavity to certain systemic diseases. 5 This condition predominantly affects middle-age women. Some associated symptoms are irritability, depression, and decreased sociability. 6 Clinical trials have reported that drug therapy with capsaicin, alpha-lipoic acid, clonazepam, and antidepressants and psychotherapy could help decrease burning mouth sensation, and could provide relief from oral burning or pain symptoms 4,7,8 ; however, there is no effective protocol for all patients.
BMS is notably often comorbid with xerostomia, nutritional deficiencies, and/or psychologic disorders. 7 Due to the association with xerostomia, treatments aiming to improve this symptom can also be used to improve the burning sensation in the mouth. One study conducted in 2015 evaluated the efficacy of a salivary substitute prepared using chamomile flower and flax seed to alleviate xerostomia and associated symptoms. 9 That study demonstrated, for the first time, that a homemade salivary substitute can be more effective in relieving burning tongue sensation (a symptom associated with xerostomia) than a conventional salivary substitute. The effectiveness of this substitute is attributed to the lubricating and wetting properties of the flax seed extract and the anti-inflammatory, antispasmodic, and sedative properties of chamomile flower. In contrast, it has been reported that patients with BMS can have neuropathic impairment, and that could be associated with the burning sensation reported by these patients. 10,11 Studies have demonstrated that inhibition of metalloproteinase activity, especially matrix metallopeptidase 2 (MMP2) and MMP9, may be reflected in the relief of neuropathic pain. 12,13 Considering a possible neuropathic origin of the burning sensation in patients with primary BMS, it is also highly interesting to evaluate whether a homemade salivary substitute would have any effect on inhibiting the activity of such metalloproteinases.
The objective of this study was to evaluate the effect of a salivary substitute prepared using chamomile flower (Matricaria chamomilla L.) flower and flax (Linum usitatissimum L.) seed to relieve BMS symptoms and inhibit MMP2 and MMP9 activities, and its effect on some salivary characteristics such as salivary flow and viscosity. Considering that chamomile flower and flax seed are easily available and highly economical, the authors evaluated their effectiveness in using them as a homemade formula prepared by the patient. In addition, it is important to evaluate whether it has any cytotoxic effect due to its potential permanent use in BMS.
Materials and Methods
This study was approved by the research ethics committee of the School of Dentistry at the Federal University of Pelotas, Pelotas, Brazil (UFPel) (Approval code: No. 2,078,409) and is registered with code RBR-774xbd in the Brazilian Registry of Clinical Trials (ReBEC). This was an open clinical trial, in which the authors recruited women aging >40 years with primary BMS who were referred to the Center for Diagnosis of Mouth Diseases at the School of Dentistry of UFPel (CDDB) from 2016 to 2018. Before starting the study, all participants signed an informed consent, according to the principles of the Declaration of Helsinki. 14
Determining the severity of primary BMS and xerostomia symptoms
The criteria to establish a diagnosis of primary BMS are as follows: (1) moderate-to-severe, daily, and bilateral burning sensation in the oral mucosa, (2) burning sensation with a duration of at least 4–6 months, (3) burning sensation can be constant or increasing in intensity during the day, (4) burning sensation can improve with food or liquid intake or interfere with sleep, and (5) absence of local and systemic factors that justify the burning sensation. 4,5,15 Patients were evaluated at the first appointment and after 30 and 60 days. In addition, a questionnaire was applied to determine the intensity of xerostomia symptoms. 16 For each protocol, the authors used a visual analog scale with scores ranging from 1 to 10, wherein 1 represented the absence of symptoms, and 10 the maximum symptomatic perception experienced by the patient. To evaluate relief of sleep disturbance, it was also used a visual analog scale with scores ranging from 1 to 10, being 1 minimum disturbance and 10 maximum disturbance of sleep.
All volunteers were evaluated by a dentist specialized in oral pathology to exclude local variables that could be associated with BMS. A medical history, including information related to current systemic diseases, ongoing medications was obtained for all patients. Patients also underwent laboratory tests (complete blood cell counts and glycated hemoglobin). Exclusion criteria included the presence of any of the following: previous history of head and neck malignancy, chronic thyroid disease, known Sjogren's disease, any alteration in blood cell counts, rheumatoid arthritis, contact allergies, pregnant women, history of herpes zoster, with signs and symptoms of buccal lichen planus and patients treated symptomatically or who showed relief after the use of corticosteroids or antifungals in relation to burning sensation. Patients with type 2 diabetes mellitus, only those with a glycated hemoglobin (hemoglobin A1C) level <7%, which is considered as adequate glycemic control, were recruited in the study. 17 Patients who underwent prior treatment for BMS were included only if the treatment was ineffective and discontinued for a minimum of 2 months before being included in this study.
Determining unstimulated salivary flow rate
Samples of nonstimulated saliva were collected at the beginning of the study and after 30 and 60 days. The saliva samples were collected under resting conditions in a quiet room between 9:00
Salivary pH measurement
The pH of the saliva samples was determined at the beginning of the study and after 30 and 60 days using saliva from the same tube, for which the SFR was measured. A digital pH meter (PL-600 EZDO-OMEGA model according to the ISO-9001 regulation) automatically provided the pH value to two decimal ranges. 19
Preparation and use of the homemade salivary substitute
The patients were instructed to purchase the components (whole flax seeds and dry chamomile flower flowers) at the same shop to ensure comparable product composition and quality and to avoid risk of bias. To prepare the homemade salivary substitute, the patients mixed 200 mL water with two tablespoons of flax seeds (10 g) and boiled the mixture to prepare a mucilage. The mixture was allowed to soak until cool after which the seeds were strained out by filtration. At the same time, a tea infusion was prepared by pouring 200 mL freshly boiled water over one tablespoon (1 g) of chamomile flowers, and allowing to steep for 10 min before straining. The flax seeds mucilage and the chamomile flowers tea infusion were mixed in equal proportions to prepare the homemade salivary substitute, which was then refrigerated at 4°C for 3 days. The patients were instructed to rinse their mouth with the substitute three to four times daily for 1 min. Patients were trained individually to prepare the homemade salivary substitute and a step-by-step instruction sheet was provided. It was recommended to buy German chamomile flower (M. chamomilla L.) and not Roman chamomile flower [Chamaemelum nobile (L.) All.].
Substrate gel electrophoresis (zymography): Determining MMP activity by zymography
The proteolytic activity of MMP2 and MMP9 was examined on 10% polyacrylamide gel containing 0.05% gelatin. The medium conditioned by the MMPs was obtained through a human saliva sample obtaining the signed consent to participate in the research. 20 The volunteer had been healthy, with no report of any oral disease or pathology, for which he was evaluated by an oral pathology specialist. The subject bit a sterile gauze for 30 sec, which was then placed in a sterile syringe to remove saliva from the gauze and deposit in a plastic sterile centrifuge tube. The saliva was mixed with the sample buffer (2% SDS, 125 mM Tris-HCl [pH 6.8], 10% glycerol, and 0.001% bromophenol blue), and then electrophoresis was conducted. The gel was incubated in a developing buffer containing the materials used in the study. The positive control was 0.5% N-ethylmaleimide (NEM) that does not inhibit metalloproteinase activity, and 0.5% EDTA was used as the negative control, which is a known metalloproteinase inhibitor. In addition, another control containing only the buffer solution (Tris-CaCl2) was used without any test group. After electrophoresis, the gel was washed twice in Triton X-100 (2%) for 60 min at room temperature, and incubated at 37°C for 24 h in 50 mM Tris-HCl buffer (after incubation, the gels were stained with 0.05% Coomassie Blue G-250 (Bio Rad, Richmond, CA). Gelatinolytic activity was detected as unstained bands on the blue-stained gel, and then a qualitative analysis of the bands was performed to quantify the inhibition of MMP2 and MMP9 activity by different concentrations of chamomile flower, and flax seed tested separately at different concentrations (100%, 50%, and 10%), where 100% was the indicated concentration for patients (200 mL of boiling water with 10 g of flax seeds and 200 mL boiling water with 1 g of chamomile flower).
Cell viability assay
Cell viability assay was performed according to ISO 10993:2009. Mouse fibroblasts L929 (2 × 104/well) were maintained in DMEM in 96-well plates for 24 h. Each material was previously incubated in 1 mL of DMEM at 37°C, pH 7.2 for 24 h, under static conditions to obtain the eluates (n = 3). The positive control used was the untreated group (only fibroblast cells in DMEM, without eluate addition). The eluates from the specimens were applied in each well of 96-well plates previously prepared with mouse fibroblasts. The cytotoxicity produced by each different group was assessed with 24 h cell exposure time using different concentrations of flax seed (50%, 25%, and 10%) and chamomile flower (50%, 25%, and 10%) according to the concentration indicated to the patients. After removing the eluates, 180 μL of DMEM was added to 20 μL of MTT solution, and placed in each well. After 4 h of incubation at 37°C in darkness, the blue formazan precipitate was extracted from the mitochondria using 200 μL/well of dimethyl sulfoxide (DMSO). The absorption was determined using a spectrophotometer at a wavelength of 540 nm.
Salivary substitute viscosity
The values of the viscosity of salivary samples from BMS patients at times 1 and after 3 months (M3) and of chamomile flower and flax seed at the same concentration indicated for patients were evaluated and recorded for 150 sec of continuous monitoring using the dynamic rheology technique with a HAAKE CaBER-1 extensional rheometer (Thermo-Fisher Scientific, MA). Samples were vortexed and loaded onto 6 mm diameter plates set within an initial 2 mm range. All measurements were performed at 37°C using 1 mL of each sample. The rheometer plates were cleaned with ethanol and then with distilled water and air-dried between each sample evaluated. Three measurements were taken per sample and the mean of each was used for statistical analysis. 21
Statistical analysis
Kruskal–Wallis one-way analysis of variance followed by SNK post hoc test was used to analyze cell viability (absorbance). Kruskal–Wallis one way was used to compare values of unstimulated SFR, pH, and severity of BMS, and xerostomia symptoms, according to the visual analog scale between M1, M2, and M3. T-test was used to compare salivary viscosity before and after therapy. SigmaPlot 12 (Systat, Inc., San Jose, CA) program was used and p < 0.05 was considered statistically significant.
Results
The authors enrolled 40 female patients (age 45–81 years, mean age 60.7 years). Most patients were receiving treatment for hypertension, depression, or anxiety, and most of them did not smoke or drink alcohol. Table 1 summarizes the frequency and percentage of systemic diseases, associated factors, and medication consumption.
Frequency and Percentage of Systemic Diseases, Consumption of Drugs, and Habits in Women with Burning Mouth Syndrome
The average unstimulated SFRs at the beginning of the study (M1) and after 30 (M2) and 60 (M3) days of treatment with the homemade salivary substitute were 0.375, 0.461, and 0.447 mL/min, respectively, with the differences being statistically significant (p < 0.05). The average pH values observed at M1, M2, and M3 were 7.23, 7.55, and 7.40, respectively, with no statistically significant differences (p > 0.05). Salivary characterization data are summarized in Table 2 and Figure 1.
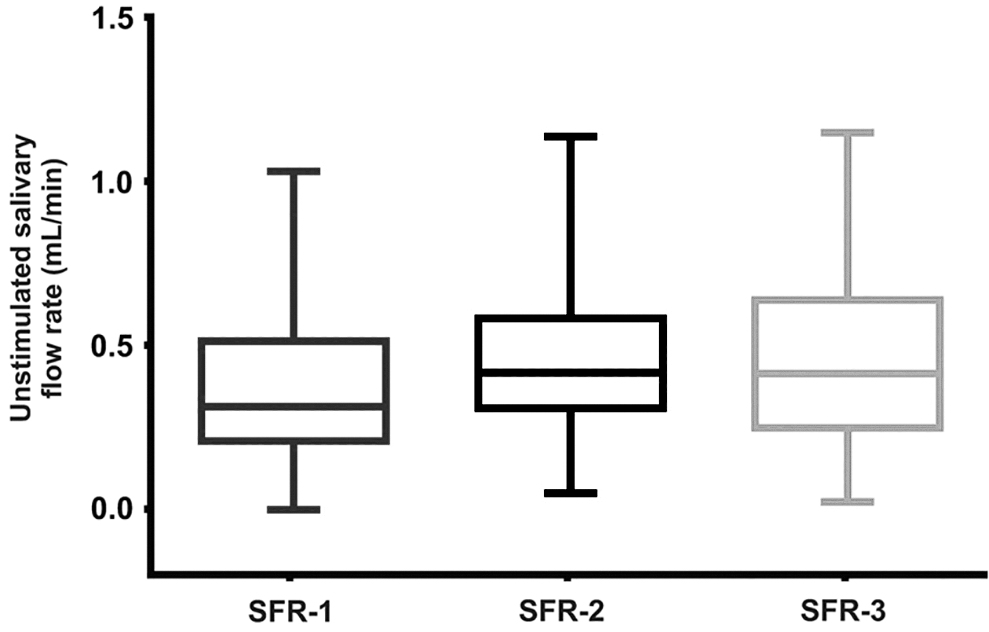
Unstimulated SFR at the beginning of the study (SFR-1) and after 30 (SFR-2) and 60 days (SFR-3) in women with BMS. BMS, burning mouth syndrome; SFR, salivary flow rate.
Salivary Characterization in Women with Burning Mouth Syndrome
M1, at the beginning of the study; M2, after 30 days; M3, after 60 days; SD, standard deviation.
Relief scores from the burning sensation associated with BMS (measured according to the decrease in the severity of symptoms reported by the patient using the visual analog scale scores ranging from 1 to 10) at M1, M2, and M3 were 7.74, 3.76, and 2.95, respectively, with the differences being statistically significant (Fig. 2). Seven (17.5%) patients reported sleep disturbances due to BMS, and these symptoms significantly improved with the use of the homemade salivary substitute. The average scores of improvement in sleep symptoms associated with BMS (which was also measured using the visual analog scale scores ranging from 1 to 10) in patients at M1, M2, and M3 were 3.38, 1.00, and 0.95, respectively. Table 3 summarizes the results of the average relief in oral mucosa burning sensation symptoms and the average improvement in sleep symptoms associated with BMS.
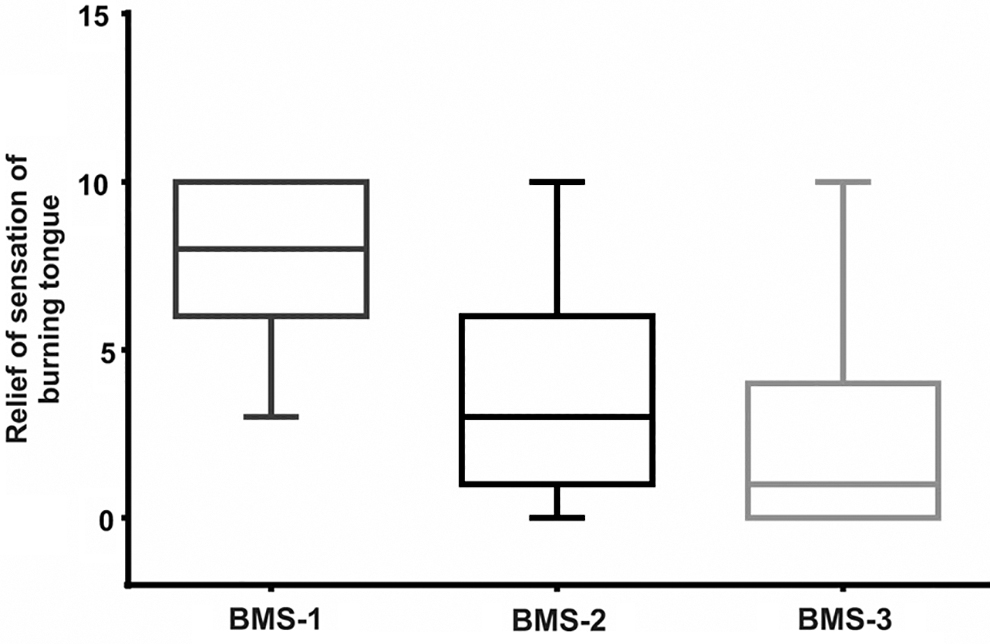
Burning tongue relief sensation at the beginning of the study (BMS-1) and after 30 (BMS-2) and 60 days (BMS-3) in women with BMS. BMS, burning mouth syndrome.
Average of Burning Tongue Relief Sensation and Sleep Disturbance
Values determined by visual analog scale with scores ranging from 1 to 10.
M1, at the beginning of the study; M2, after 30 days; M3, after 60 days.
Xerostomia was present in 26 (65%) women. Scores of the average intensity of xerostomia in these patients (which was also measured using the visual analog scale scores ranging from 1 to 10) were 4.90 (SD 2.29), 2.62 (SD 2.12), and 0.43 (SD 2.27) at the beginning of the study and after 30 and 60 days of treatment, respectively, with the differences being statistically significant (p < 0.05).
Results of qualitative zymography analysis showed that the different concentrations of flax seed and chamomile flower (100%, 50%, and 10%) did not inhibit the activities of MMP2 and MMP9 in the human saliva samples (Fig. 3).
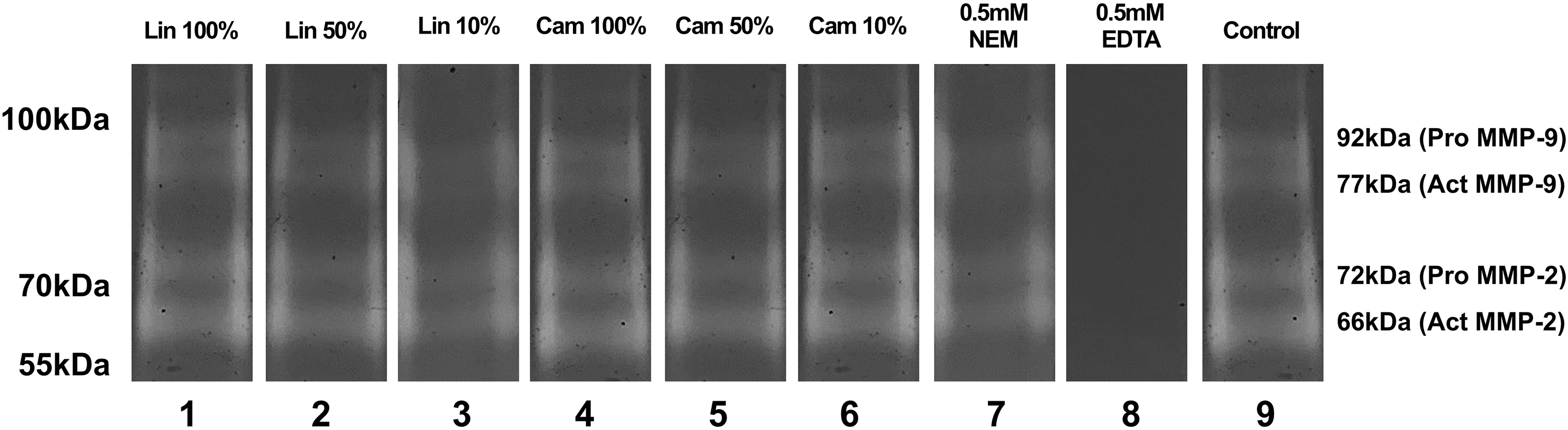
Effect of chamomile flower (Matricaria chamomilla) and flax seed (Linum usitatissimum) on the activities of MMP2 and MMP9. Normal human saliva samples were homogenized and prepared for qualitative zymography analysis using different concentrations of loaded protein. The different concentrations of flax seed (columns 1 [Lin 100%], 2 [Lin 50%], and 3 [Lin 10%]) and chamomile flower (columns 4 [Cam 100%], 5 [Cam 50%], and 6 [Cam 10%]) tested separately did inhibit the activities of MMP2 and MMP9. As observed in columns 7 (positive control containing 0.5% NEM) and 9 (containing only the buffer solution [Tris-CaCl2]), the solutions did not inhibit MMP2 and MMP9 activities. The negative control was 0.5% EDTA (column 8), which inhibited the activities of MMP2 and MMP9. MMP, matrix metallopeptidase; NEM, N-ethylmaleimide.
The average percentage of cell viability assessed after 24 h according to the different concentrations of chamomile flower and flax seed (100%, 50%, and 10%) were as follows: 108.86 (SD 13.37), 142.88 (SD 6.65), and 143.75 (SD 5.54) for chamomile flower and 109.40 (SD 17.23), 138.50 (SD 10.10), and 132.77 (SD 11.54) for flax seed without differences being statistically significant (p > 0.05). Chamomile flower (M. chamomilla) and flax seed (L. usitatissimum) were not cytotoxic to mouse fibroblasts (Fig. 4).

Effect of chamomile flower (Matricaria chamomilla) and flax seed (Linum usitatissimum) on cell viability. The percentage of cell viability evaluated after 24 h for the different concentrations of chamomile flower and flax seed (columns 1 [LIN 50%], 2 [LIN 25%] and 3 [LIN 10%]) and chamomile flower (columns 4 [Cam 50%], 5 [Cam 25%] and 6 [Cam 10%]). The average percentage of cell viability was 108.6 ± 13.37%, 142.88 ± 6.65%, 143.75 ± 5, 54, 109.40 ± 17.23, 138.50 ± 10.10, 132.77 ± 11.54 for columns 1, 2, 3, 4, 5, and 6, respectively, without statistically significant differences.
The average values of the viscosity of BMS patient's saliva samples pre- and post-therapy and from chamomile flower and flax seed after 150 sec of continuous monitoring and measures in millipascal seconds were 45.01 (SD 0.65), 41.87 (SD 2.73), 31.01 (SD 1.02), 29.60 (SD 0.29), and 26.38 (SD 0.34), respectively, showing statistically significant differences (p < 0.05) (Fig. 5).
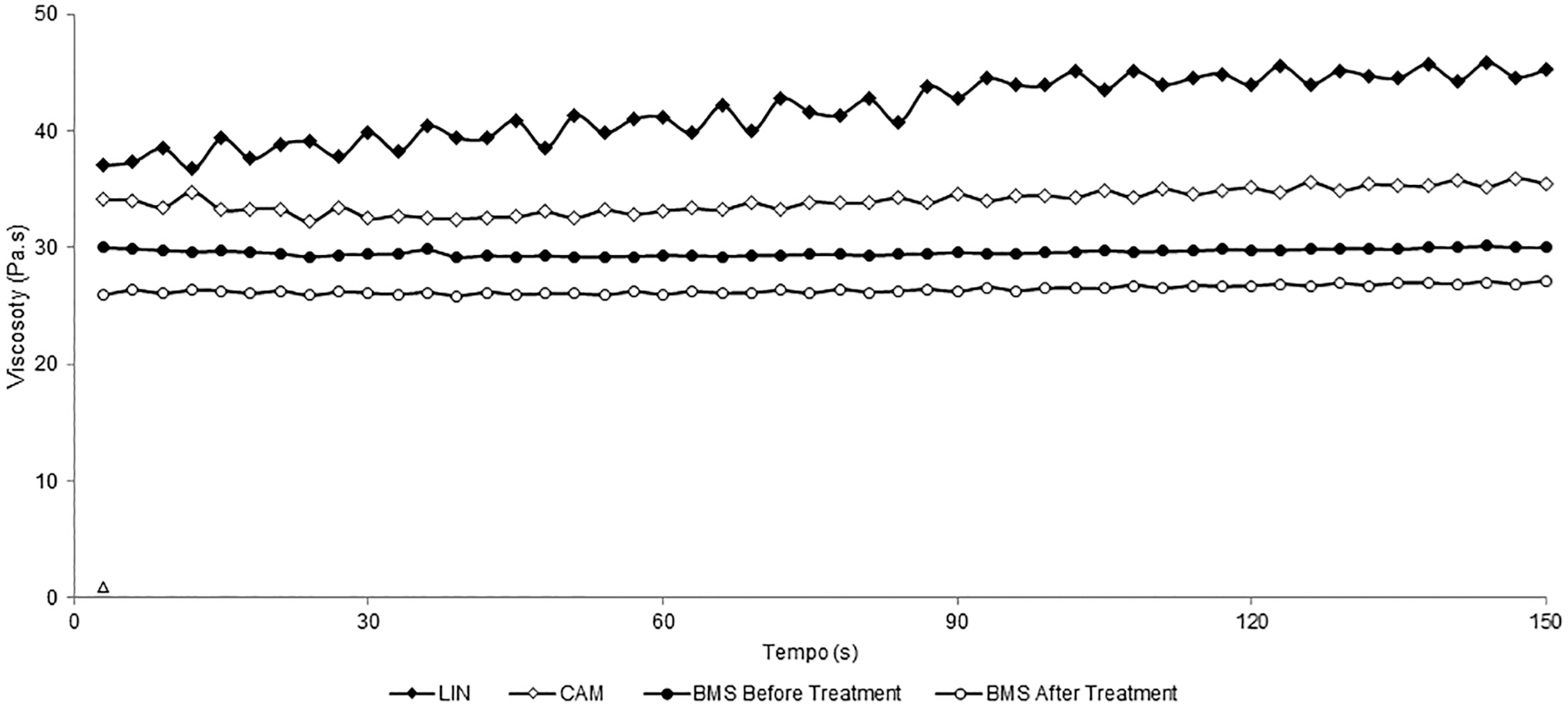
Viscosity measurements for chamomile flower and flax seed and whole saliva of BMS patients before and after treatment. The average viscosity after 150 sec of continuous monitoring in the group of women with BMS before and after 3 months of treatment showed statistically significant differences (p = 0.001). BMS, burning mouth syndrome.
Discussion
Regarding systemic diseases and associated treatments, in the sample, 50% reported that they were under treatment for arterial hypertension, which was the most common comorbidity associated with BMS, as reported in a previous study. 22 Although the use of antihypertensives may reduce salivary flow, which may be a risk factor for the development of BMS, 23,24 in the sample there were no differences in salivary flow or the severity of burning sensation in patients with hypertension compared with those who did not have this comorbidity. There were also no differences in the parameters evaluated in patients with or without diabetes mellitus and depression who were also being treated pharmacologically, which were the second and third most frequent systemic diseases in the sample.
Evidence indicates that the neuropathic pain could be determined by the activity of metalloproteinases, especially MMP9 and MMP2. In cases of diseases where the sensitivity problem has a neuropathic origin, the activity of metalloproteinases would be responsible for hypersensitizing the peripheral nerves causing this type of change in perception. 25 The results suggest that the origin of the burning sensation in BMS patients might not have a neuropathic origin and that the effect of chamomile flower and flax seed on BMS symptom improvement could be explained by other factors rather than by inhibiting MMP2 and MMP9 activities.
Regarding the salivary flow, differences were observed in SFR between M1 and M2. The improvement in BMS symptoms could be partly related to the increase in salivary flow observed 1 month after the treatment. These results are consistent with those of studies that reported an association between the decrease in salivary flow and BMS. 13,26 The decrease in SFR that can be present in BMS can promote the lack of chemical and physical protection of the oral mucosa, facilitating the establishment of BMS 27 and could influence the reception of stimuli and alter the perception in patients with BMS. 28 This would be one of the reasons why the increase in SFR could be associated with a relief of symptoms of BMS. The properties of chamomile flower and flax seed could also explain the relief of BMS symptoms. Flax seed contains molecules similar to mucins, such as polysaccharides, proteins, and glycoproteins, which have lubricating and moisturizing properties similar to those of mixed saliva. 29 Chamomile flower possesses anti-inflammatory properties and has been used to reduce oral mucositis symptoms. 30 The association between BMS and the alterations in SFR may be due to the simultaneity of systemic diseases, medication use, aging, and even associated glandular damage, which supports the hypothesis of a multifactorial etiology of BMS. 24
Previous studies have demonstrated that patients with BMS have more poor sleep quality than people without BMS. 2,31,32 In this study, seven (17.5%) patients reported having sleep disturbances due to BMS, which were significantly improved after the use of chamomile flower and flax seed. Emerging data indicate that several patients with BMS suffer from poor sleep quality and this phenomenon should be considered in the etiology of BMS.
It was important in view of its potential permanent therapeutic use to make sure that the substitute would not have a cytotoxic effect. Evidence indicates that 72 h fermented chamomile flower has an important cytotoxic effect of ∼95% against cancer cells, suggesting its promising role in cancer therapy. 33 Because of this background it was important to assess whether that cytotoxic potential could also affect normal cells that could even contraindicate chamomile flower's use permanently and several times a day. According to the results neither chamomile flower nor flax seed has cellular cytotoxic effect, which further underlines their safe use and no adverse effects.
Although an author indicates that viscosity may be a determining factor in BMS, evidence is insufficient to establish an association between salivary viscoelasticity and BMS in the literature. 28 Moreover, the little evidence that exists is contradictory. One study established an increase in salivary viscosity associated with xerostomia relief (symptom associated with BMS) in capsaicin-treated patients. 34 In contrast, it is suggested that patients with BMS have higher salivary viscosity than patients without the syndrome, which could induce the feeling of discomfort they report having. 35 The decrease in salivary viscosity observed in this study after therapy with the substitute could be related to the relief they reported having. However, the results may also be contradictory in this respect, because both chamomile flower and flax seed have higher viscosity than saliva of patients with the syndrome. If the beneficial effect of the substitute is based on decreased salivary viscosity and because this salivary characteristic can remain stable for 12 h, 28 the relief may be due to the instruction to use the substitute at least four times, which would maintain salivary viscosity stability throughout the day.
This substitute fits the definition of alternative or complementary medicine because even though it demonstrates an enormous potential clinical use, using elements of the nature of recognized efficacy by the scientific community, it had not been previously evaluated and a protocol to their use must be improved. 36 One limitation of this study may be the lack of total control over the composition, quality, purity, and strength of the botanical products purchased by the volunteers at the store indicated by the researchers. For this reason, these promising results presented must be accompanied by a controlled study, in which botanical materials are delivered in packages along with the written instructions step by step for the preparation and administration of the substitute in addition to a class with a demonstration to volunteers on how to make the preparation uniformly at home. In conclusion, this study has demonstrated that the homemade salivary substitute prepared using chamomile flower and flax seed is an economical, viable, easy-to-handle, noncytotoxic, and effective alternative to relieve the symptoms of BMS. Also, the results corroborate the hypothesis of multifactorial etiology of the syndrome. It is important to improve and increase studies that use affordable home remedies, especially for poor and low-income communities.
Footnotes
Acknowledgment
Fellowship OAS-GCUB.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.