
Abstract





Despite ongoing recommendations and guidelines published by national and international societies 1 (National Academy of Medicine and American College of Physicians), the inclusion of integrative medicine practices and practitioners into the systems of reimbursement continues to be slow and uneven. For more effective inclusion, we suggest that integrative medicine might lead the evolution of measurement-guided care as a driver for health care systems development. The purpose of this commentary is to explore the pattern of uptake to identify strategies where such activity might best support more appropriate inclusion.
The reasons for this uneven inclusion are many. Some are related to general patterns of health care change, and others specific to the field of integrative medicine. In the broader category, the rising cost of health care is itself a disincentive to include additional approaches. 2 The design of reimbursement systems, such as tiered products, 3 adds additional resistance. In addition, Ref. 4 found that any integration of new services that crosses lines between specialities 5 encounters barriers due to protective guild interests. Resistance preserves old practice patterns, anchoring the inertia of the existing system to complex procedures, which are part of the conventional care strategy and economics. An example is the use or overuse of cardiac stents. 6 Established cardiology practitioners have slow momentum to include new practice patterns due to present reimbursement and training platforms. However, with examples that specifically involve integrative practices—through a combination of mind–body approaches, diet, and exercise in a group format—strategies that reduce the need for stents may be slow in uptake.
Other challenges for coverage inclusion are specific to integrative medicine's philosophy and practices. A central component in integrative medicine is the freedom to choose treatment approaches between the practitioner and the patient. Many practitioners value this freedom and argue that the application of clinical experience must remain in the clinical setting without any measurement-guided care. In addition, the plethora of methods and procedures and the variability in integrative medicine practices makes it difficult to establish explicit principles for the sharing of clinical decision-making. Thus, reimbursement based on procedures would in many cases be difficult given that the procedures often carry a low grade of definition and thereby a low grade of evidence. Consequently, it makes it difficult to establish shareable principles for best practices between integrative medicine modalities.
Another challenge within integrative medicine is the lack of common diagnostic classifications for diagnosis, for example, International Classification of Diseases-11th Revision, 7 and varied descriptions of symptoms and divergent taxonomies. An even further challenge lies within the multiple variations of practices within a modality (e.g., massage therapy). 8 Some of these variations have a limited effect on outcome but marked effect in treatment intensity and thereby in cost. 9
Opportunities in the Shift to Focus on Outcomes
One way the inertia of the reimbursement systems is being challenged is through the focus on outcomes rather than on practice content. 10 This trend toward outcome-based reimbursement regimens, sometimes referenced as “from volume to value,” is global. 11 The importance of outcome measure for policy making was very well illustrated by the U.K. National Health Service (NHS) example called “Increased access to psychological treatment” (IAPT). Over the course of a few years, the NHS developed a nationally available program where access to psychological treatment was allowed to expand and in which transparent measures of outcomes for all patients was part of the treatment program. 8 Outcome measures are also part of the accountable care strategies supported by the 2010 Affordable Care Act in the United States. However, the transition in the payment systems is slow as the forms for quality-based payment models are only partially developed. 12
The trend toward value-based reimbursement is potentially a golden opportunity for integrative medicine. Likely, an increased focus on patient outcomes would favor integrative medicine. Reimbursement based on outcomes and achieved health has a great potential as such schemes are neutral toward process content. The value-based strategy of bundled payment may also be particularly appropriate for integrative medicine. The utility of this approach is evident in both integrative medicine's evidence deficiencies and its strengths. A survey of academically based integrative medicine practitioners indicates a stronger sense of alignment in these emerging strategies than with fee-for-service models. 13 Several trials in integrative medicine have demonstrated cost-effectiveness. 14,15 These appear to be linked to the integrative focus on prevention 16 and well-being, and patient centeredness combined with the reduction of morbidity through limiting the use of excessive technology and pharmacotherapy. 17 A retrospective study on health care utilization found a 43% reduction of services in patients that engaged with mind–body medicine services.
Notably, these studies demonstrate the value in promoting a more holistic view of health than the current health care system.
However, to achieve this integration requires that integrative medicine meet an important real-world evidence bar. A key for the migration of different integrative medicine measures to enter into reimbursement systems lies in the real-time availability and utilization of systematic health data. Built-in gathering of patient-reported outcome measures (PROMs) can potentially support the claims that integrative medicine provides additional value to promote the healing and well-being of patients. Variability in health care practices is a major reason for variability in health outcomes and in delivered quality. Hence, clinical practice often does not reflect evidence-based best practice—conventional and integrative medicine practices share this problem. This is the fundamental argument for sharing knowledge through a common process, especially for common health problems. At the same time, this type of knowledge sharing creates an opportunity for improvements in health care services The organized use of shared cumulatively built knowledge 18 in a properly determined clinical process expounds the basis for the different available clinical choices. Once established, such a process description can provide a very good basis for bundled care payments where quality ( = patient value) also is a part of the reimbursement.
Early data from an integrative patient-centered medical health care suggests positive outcomes. Such an approach should ideally include data on participating patients, their trajectory through health care, and their health outcomes. 19 For the obvious reason of comparability, these outcome measures should be consistent across types of practices in capturing achieved quality of life, psychological well-being, self-fulfillment, and physical ability. Ideally the same measures should be used irrespective of practice, and there are several initiatives that promote the use of standard outcomes measures. 20,21 Long-term outcome follow-up is also essential since integrative practices have shown persisting health benefits a year after the end of the treatments. 22
The current evidence base for medical practices ideally rests on the idea of a full description of mechanisms and procedures and supporting empirical data. Any model of reimbursement requires the ability to describe the basis for the payment, be it fee-for-service, availability, process quality, or achieved health.
The Long Road
The illustration of the decision space in the practice of integrative medicine (Fig. 1) demonstrates the long road toward unification of practices with common taxonomies and outcome measures. Such a unification is a prerequisite for the ability to assess the complexity and disease burden that patients present to health care. This is the core principle that will enable the move from fee-for-service toward newer forms of bundled payment, including outcome-based payments. For the latter, it is imperative with a properly described pretreatment assessment. The payer needs information on the achieved health as compared with when the patient entered into care. The quality measurement system needs to be robust and reflect the desired values for patient care. Otherwise, gaming of the payment systems, access to care for those who need it the most, and so on cannot be guaranteed.
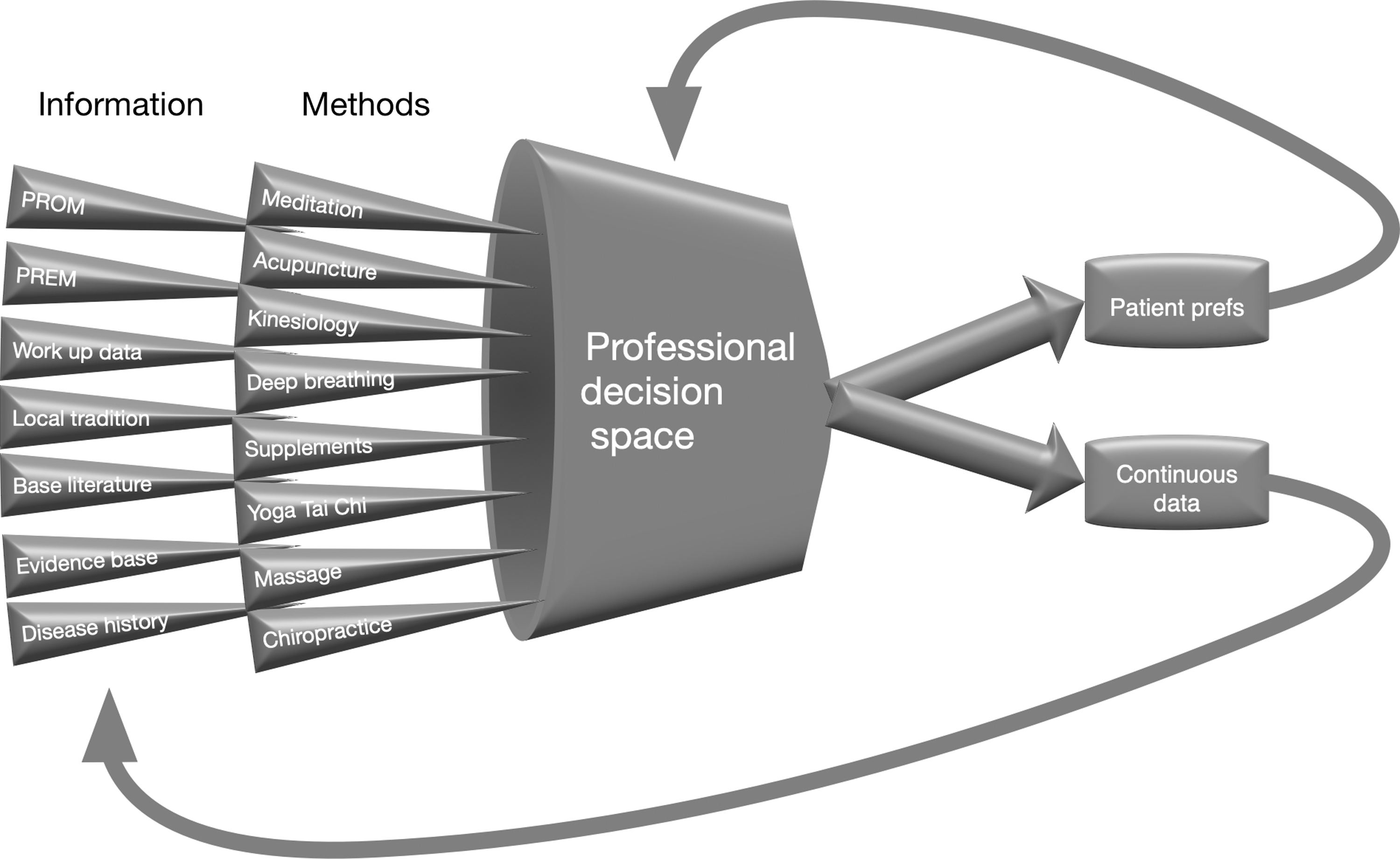
Decisions in clinical practice always rest on many dimensions and depend on both explicit and implicit knowledge and rules. The even more complex decision space in integrative medicine is a direct effect of the multitude of treatment paradigms and differences in terminologies and diagnose descriptions between practices. The building of a systematic evidence base as a result of continuous data collection is very difficult in such a diverse knowledge environment. PREM, patient-reported experience measure; PROM, patient-reported outcome measure.
The times have ended when health care professionals could simply ask for a blank check based on the professional knowledge as was common in what is referred to as eminence-based medicine (Cochrane Consumer Network 2019). In the era to come, those who provide data on quality, PROMs and patient-reported experience measures, care efficiency, and effectiveness will forge the path to the future. If integrative medicine can use this framework to invite its diverse branches into the common language of outcomes that represent healing and improved health experience, it will unequivocally reshape the way medicine is practiced, and reimbursed. 23