
Abstract
Objective:
This feasibility study examined the effects of a particular Traditional Chinese Medicine (TCM) herbal formula on attention-deficit/hyperactivity disorder (ADHD) and related problem behaviors.
Design:
A total of 79 participants aging 6–12 years consumed a granulated TCM herbal formula twice daily over a period of 3 months and underwent assessments at months 0, 3, and 6. Changes in ADHD symptoms and related behaviors were measured using the ADHD rating scale-IV (ADHD-RS-IV), child behavior checklist (CBCL), children's global sssessment scale (CGAS), as well as the clinical global impressions-severity (CGI-S) and improvement (CGI-I) scales.
Results:
Repeated measures mixed model analyses revealed significant differences in scores across time on all ADHD-RS-IV and CBCL subscales as well as on the CGAS, CGI-S, and CGI-I scales. Pairwise comparisons between months 0 and 3 as well as months 0 and 6 indicated significant improvements in scores. Scores also did not differ significantly between months 3 and 6. The results may suggest that this particular TCM formula possesses potential therapeutic qualities in the treatment of ADHD. Furthermore, changes in ADHD symptoms generally appear to be stable 3 months after discontinuation. However, these findings could also be attributed to placebo effects as well as reporting biases.
Conclusion:
This particular TCM formula may prove to be a useful adjunctive treatment for children with ADHD, and randomized controlled trials need to be conducted to evaluate its efficacy.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is one of the most diagnosed and researched illnesses among children and adolescents, interfering with many aspects of daily functioning, which include learning, productivity, and social relationships. 1 A chronic condition affecting millions worldwide, ADHD often requires treatment to enable affected individuals to cope and manage their symptoms. 2 Western medications, particularly methylphenidate (MPH) and atomoxetine, remain extensively used for the treatment of ADHD and has been rigorously reviewed to be efficacious, 3 –5 promoting favorable long-term outcomes and behavior. 6 –8
Numerous studies have attributed a myriad of adversities associated with MPH, the drug of choice for ADHD. These include common side effects such as reduced appetite, headaches, abdominal pain, and insomnia. 9,10 For atomoxetine, a nonstimulant, the common side effects include initial somnolence, gastrointestinal disturbances, and decreased appetite. 9 Thus, it is unsurprising that clinicians and caregivers of children with ADHD have increasingly advocated for alternative, effective, and well-tolerated treatments. 11
Research has shown a rising trend of complementary and alternative medicine (CAM) usage among children with ADHD across various populations. Results of the 2012 National Health Interview Survey revealed that >1 in every 10 children had used some form of complementary therapy for a multitude of common ailments, including ADHD in the preceding year, whereas another study reported up to 12% of 822 children having used CAM for ADHD. 12 –14 CAM forms part of holistic integrative medicine, which offers an alternative or adjunct to conventional pharmacological and cognitive behavioral treatments of ADHD. Together with other mind–body therapies (e.g., mindfulness, biofeedback, and yoga), CAM aims to bring about positive effects on psychosocial, emotional, and neurobiological functioning, and overall better treatment outcomes. 15,16
Traditional Chinese Medicine (TCM) is one frequently used CAM and according to its ideology, human health is characterized by “yin” and “yang” as well as five organ systems. 17 “Yin” denotes gentle quietness, whereas “yang” symbolizes impatience. Equilibrium of these two forces and the organ systems is required for sound physical and mental health, whereas imbalances result in conditions such as ADHD. Depending on the source of imbalance, different TCM preparations can be formulated to address deficiencies and restore harmony. 18
A review of CAM that examined 16 randomized controlled trials (RCTs) on herbal and nutritional remedies for ADHD had indicated promising results for zinc, iron, Pinus Marinus, as well as Ningdong, a TCM formula. 19 An interesting finding was that although Ningdong has shown its efficacy through improvements in scores on Teacher and Parent ADHD rating scales, side effects such as hypersomnia were associated with its use. 20 Studies with other TCM preparations have also documented adverse effects such as loss of appetite, insomnia, and mild abdominal pain, although limited when they were used appropriately. 21,22 These findings are contrary to the popular notion that TCM herbal formulations have few or no side effects. 23,24 Hence, more research on the safety and effectiveness of TCM, especially on children, would be prudent before TCM is to be considered a potential alternative treatment for ADHD.
Investigators have advocated that TCM is reliable, effective, and generally well tolerated, with low occurrence of addiction or side effects for the treatment of ADHD. 23,25,26 A review by Lan and associates systematically evaluated the effectiveness of 34 TCM remedies and found that a variety of TCM formulae were equally or more effective than MPH in treating children with ADHD as reflected by improvements in scores on various validated instruments, including the clinical global impressions (CGI) scale, child behavior checklist (CBCL), and ADHD rating scale-IV (ADHD-RS-IV). 22
It is also pertinent to note that most studies examined the short-term effects of TCM medication, but only few have attempted to evaluate the longer-term effects after cessation. 27,28 Another limitation in this literature is that most of the TCM studies were conducted primarily in China and published in Chinese TCM journals, obscuring the validity and replication of findings to other populations. 17,22 This emphasizes the need for replication of past studies and validation of findings in other populations.
Singapore is a cosmopolitan country with a population approaching 6 million people, comprising Chinese (74.3%), Malays (13.4%), Indians (9.0%), as well as individuals of other ethnicities (3.2%). 29 Local studies have indicated that a large proportion of the community have engaged in CAM, 30 with TCM being the most utilized. 31 Koh et al. conducted a local survey on knowledge, attitudes, and utilization of CAM (including TCM), and found that among 814 participants, a vast majority (96%) were either extremely or moderately satisfied with CAM and 80.9% agreed that CAM was safe and effective. 32 However, no local investigations currently exist with regard to the effectiveness, safety, as well as the satisfaction of TCM treatment for neurodevelopmental disorders such as ADHD.
This feasibility study aims to examine the short- and long-term effects of a particular TCM formula on Singapore children with ADHD over a period of 6 months using validated western instruments as well as to provide additional data on the safety and user satisfaction of TCM. It is hypothesized that the TCM formula will be well tolerated and reductions in ADHD symptoms and related problem behaviors will be observed. It is also hypothesized that changes in ADHD symptoms are stable over a period of 3 months after treatment cessation. This study serves to provide preliminary data to evaluate whether it is viable to conduct RCTs to examine the efficacy of the TCM formula.
Materials and Methods
Participants
A total of 130 children who presented at a local TCM clinic between 2013 and 2015 with complaints of ADHD symptoms were screened. Children with a primary diagnosis of ADHD as assessed by TCM physicians according to the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) 33 were referred to a member of the study team. Individuals who assented to initiate TCM treatment along with the consent of their respective parents were then recruited into the study, regardless of their level of symptom severity or functioning. Individuals with any prior diagnosis of pervasive developmental disorders, psychotic and mood disorders, substance abuse, intellectual disabilities, or a history of serious head trauma were not accepted into the study. Also excluded were individuals who were consuming any form of medications or herbal remedies for ADHD during or within 1 month of being screened. The study was approved by the National Healthcare Group Domain Specific Review Board, which is the institutional review board.
TCM formula
A standardized formula named “Mind-anchoring Granules,” which was developed by Nanjing Chinese Medicine University of China in collaboration with Science Arts Co. Pte. Ltd. (Singapore), was used for the study. This TCM preparation has been approved as a Chinese Proprietary Medicine in Singapore by the Health Sciences Authority. The formula was manufactured by Science Arts Co. Pte. Ltd. and sealed into 4 g sachets containing granulized extracts equivalent to the following raw herbs: Poriacocos 3.8 g, Rhizoma Acori Tatarinowii 3.8 g, Alpiniaeoxyphyllae Fructus 3.8 g, Polygalae Radix 3.8 g, Glycyrrhizae Radix et Rhizome 1.9 g, Radix Codonopsis 3.82 g, Triticum Aestivum 5.8 g, and Fructus Jujubae 1.8 g. Five Chinese herbs in the formula were frequently prescribed for ADHD in TCM, whereas other herbs have been used in previous TCM investigations. 20,34 –36 The contents of each sachet were dissolved in lukewarm water and consumed twice daily.
Instruments
Changes in ADHD symptoms and related behaviors were measured by the ADHD-RS-IV, CBCL, children's global assessment scale (CGAS), clinical global impressions-severity (CGI-S) and improvement (CGI-I) scales. The ADHD-RS-IV 37 consists of 18 items that examine the frequency of ADHD symptoms as specified in the DSM-IV. 33 It has been widely used and has displayed good psychometric properties. 38,39 Parents completed the questionnaire based on a scale that ranges from zero (never or rarely) to three (very often). Inattention, hyperactivity/impulsivity, and total raw scores were subsequently calculated, with larger values signifying more persistent ADHD symptoms. The CBCL is a comprehensive parent questionnaire comprising 112 three-point Likert scale items that examines a child's behavior across 10 domains. 40 Higher scores indicate increased presence of problematic behaviors. The CBCL has demonstrated strong reliability and validity among children of different ethnicities and populations. 40 –42
The TCM physicians consulting the participants completed the CGAS by rating the child's level of general functioning from 0 to 100, which corresponds to requiring constant supervision and superior functioning, respectively. 43 The CGAS is an extensively used and reliable instrument in clinical practice. 44,45 In addition, TCM physicians also rated the participant's severity and changes of symptoms by using the CGI-S and CGI-I, both 7-point scales indicating the degree of illness severity and the level of improvement of an individual's condition from baseline, respectively. 46 The CGI-S and CGI-I were reviewed to be practical and easily grasped instruments that demonstrated good psychometric properties. 47,48 The TCM physicians underwent training on the DSM-IV, CGAS, CGI-S, and CGI-I conducted by two of the study authors who are both licensed psychiatrists.
Finally, parental satisfaction on the use of TCM treatment for ADHD was elicited using a simple self-developed questionnaire scored on a 5-point scale that ranged from “Very poor” to “Very good.”
Procedure
Potential participants who sought treatment at the TCM clinic were approached by study team members and briefed about the research study. After obtaining assent and consent, participants were screened and suitable participants underwent a full physical examination. Sociodemographic data, medical, and surgical histories were collected using self-constructed checklists before the baseline (T1) assessment comprising the CGAS, CGI-S, CBCL, and ADHD-RS-IV was administered. After completing the assessment, participants were advised to take the “Mind-anchoring Granules” twice daily for a period of 3 months. Participants were instructed to return to the clinic at the end of first and second month to surrender empty sachets in exchange for additional supply of TCM granules to monitor and encourage compliance. Any potential adverse events or side effects were tracked by a study team member during follow-up phone calls to participants' parents at the first and second month.
At the end of the third month (T2), participants and their respective parents returned for a second assessment to examine the short-term effects of the TCM formula. In addition to the instruments given during the T1 assessment, the CGI-I and parent satisfaction questionnaire were administered. Any reported side effects were recorded using a self-constructed 21-item checklist that encompassed common adverse reactions such as constipation and lethargy. Participants were then advised not to take any form of ADHD medication or herbal supplements for the subsequent 3 months and to return to the clinic at the end of the sixth month (T3).
During the final assessment, participants and their parents repeated all measurements of the T2 assessment. Additional details of the sample flow and study procedure are illustrated in Figure 1. All participants received a small monetary remuneration after each assessment.
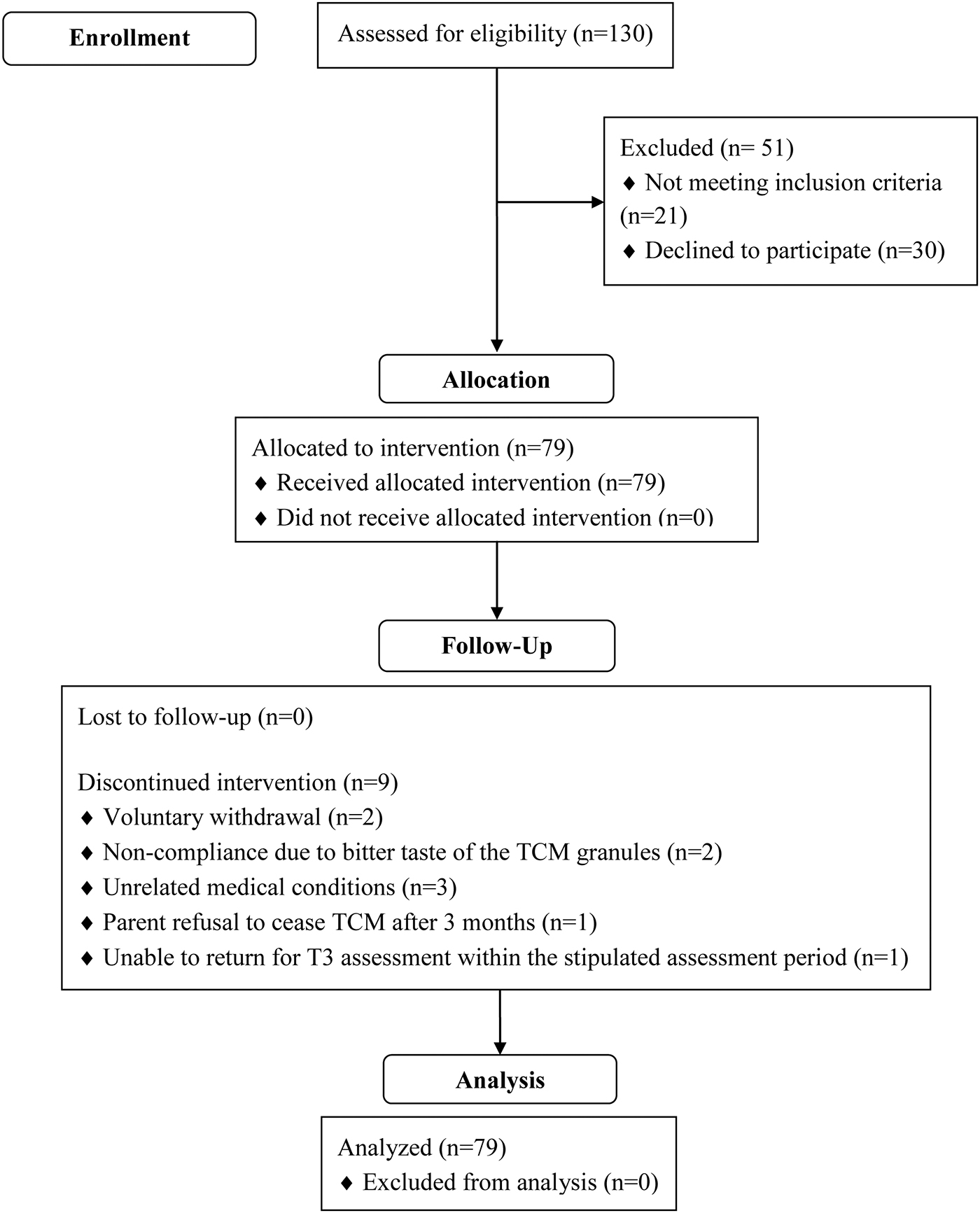
CONSORT flow diagram—modified for nonrandomized trial design. CONSORT, Consolidated Standards of Reporting Trials; TCM, Traditional Chinese Medicine.
Statistical analyses
The data of all 79 participants were analyzed using SPSS (version 17) repeated measures linear mixed models to account for missing data due to participant attrition. The compound symmetry covariance structure was selected for analyses after performing the two restricted log likelihood test. All analyses were adjusted for age and sex and an α level of 0.05 was used for all statistical tests. As this is an initial observational study, the sample size was calculated based on the referral rates of ADHD children to the TCM clinic. Postulating that the pre- and post-treatment difference is 10% higher with a standard deviation (SD) of 12.5%, a sample of at least 60 participants who completed all three assessments would be sufficient with a power of 80% and two-tailed test of 5%. The final recruitment target of 100 was set after accounting for possible attrition due to unsuitability, the longitudinal nature of the study, as well as voluntary withdrawal of participants.
Results
The final sample comprised 79 participants (77 Chinese and 2 Malay). Mean (SD) age was 9.34 (1.65), range was 6–12 years, and 81.0% were male. Participant data for the various instruments across assessments as well as the corresponding pairwise comparisons are summarized in Table 1. Analyses revealed significant differences [F(2,145.96) = 32.32, p < 0.001] between the total ADHD-RS-IV mean scores across the three assessments, with scores decreasing from T1 to T3. Pairwise comparisons with Bonferroni correction indicated that scores at T1 differed significantly from scores at T2 and T3, p's < 0.001, but no difference was found between scores at T2 and T3 (p = 1.00). Similar results were obtained for the Inattention [F(2,145.52) = 32.40, p < 0.001] and Hyperactivity and Impulsivity [F(2,145.60) = 24.23, p < 0.001] subscales, with pairwise comparisons showing T1 scores being significantly different from T2 and T3 (p's < 0.001), whereas scores between T2 and T3 were not different (p's = 1.00).
Participant Scores for Clinician and Parental Scales Across Assessments with Pairwise Comparisons a
Values adjusted for age and sex.
ADHD-RS-IV, attention-deficit/hyperactivity disorder-rating scale-IV; CBCL, child behavior checklist; CGAS, children's global sssessment scale; CGI-I, clinical global impressions-improvement; CGI-S, clinical global impressions-severity; CI, confidence interval; M, mean; SE, standard error; NA, not applicable.
Participants' total raw scores on the CBCL differed significantly across time, F(2,143.92) = 25.48, p < 0.001. Pairwise contrasts revealed that scores decreased remarkably from T1 to T2 and from T1 to T3 (p's < 0.001). However, there was no difference between total CBCL scores at T2 and T3 (p = 1.00). Similar results were obtained for other subscales, for instance, attention problems [F(2,144.74) = 29.90, p < 0.001], social problems [F(2,144.33) = 23.42, p < 0.001], and delinquent behavior [F(2,144.83) = 8.58, p < 0.001], with pairwise contrasts indicating a significant reduction of all scores at T2 and T3 (p's < 0.05) from baseline, whereas scores at T2 and T3 were not remarkably different (p's > 0.05), with exception of the Withdrawn subscale scores, which were substantially different between T1 and T3 (p = 0.002), but similar between T1 and T2 (p = 0.27).
Mean scores on the CGAS changed significantly across time, F(2,146.64) = 129.11, p < 0.001. Post hoc analyses indicated that increase of T2 (mean [M] = 72.39, standard error [SE] = 1.24) and T3 (M = 70.51, SE = 1.25) scores from T1 (M = 54.66, SE = 1.20) was significant, p's < 0.001, whereas the reduction of scores from T2 to T3, however, was not significant (p = 0.40).
Analyses of CGI-S mean scores indicated a significant main effect of time, F(2,146.99) = 99.00, p < 0.001, with scores varying across baseline, third month, and sixth month.
Further inspection of means indicated that scores at T1 (M = 4.01, SE = 0.10), which corresponded to between “Moderately Ill” and “Markedly Ill,” differed significantly from scores at T2 (M = 2.49, SE = 0.11) and T3 (M = 2.75, SE = 0.11), p's < 0.001. The increase of scores from T2 to T3 was not significant (p = 0.09) and both scores were between “Borderline Mentally Ill” and “Mildly Ill.”
Participants' clinical improvements on TCM treatment were assessed at T2 and T3 accordingly. Analyses revealed that the increment of CGI-I scores from T2 (M = 2.63, SE = 0.11) and T3 (M = 2.82, SE = 0.11) was significant, t(1,69.17) = 4.45, p = 0.04.
The frequencies and percentages of the Parental Satisfaction Questionnaire responses are displayed in Table 2. At T2, 95.83% of parents rated the TCM treatment as “Moderate,” “Good,” or “Very Good,” whereas the remaining 4.17% opined that the intervention was “Poor” or “Very Poor.” Similar findings were obtained at T3 assessment. No side effects or adverse events related to the TCM formula were reported at T2 or T3.
Frequency Table for Parent Satisfaction Questionnaire
Number of participants at 3 months = 72. Number of participants at 6 months = 70.
Discussion
The CGI-I scores at T2 indicated that participants were between the range of “Minimally Improved” and “Much Improved” after undergoing TCM treatment for 3 months. The significant drop in scores on the CGI-S, as well as all ADHD-RS-IV and pertinent CBCL subscales from T1 to T2, suggests that the TCM formula may reduce ADHD symptoms as well as most related problem behaviors. Improvements in general functioning as reflected by a remarkable increase of CGAS scores from baseline to the third month were also noted, which can possibly be attributed to the decrease of ADHD symptoms and psychopathology. Furthermore, scores across the various instruments indicated reduced psychopathology and improvements in functioning from T1 to T3. These preliminary findings may lend support to other similar studies that demonstrated the short-term effectiveness of TCM in treating ADHD. 49,50
Although there was a significant increase of CGI-I scores from T2 to T3, which shifted toward the direction of “Minimally Improved,” both scores still lie between “Minimally Improved” and “Much Improved” categories, indicating that participants generally became better over time with TCM treatment as compared to baseline. The consistent scores on all other clinician and parental measurements between T2 and T3 may indicate that improvements were sustained and that ADHD symptoms and related behaviors did not return to baseline levels. This supported the hypothesis that the effects of TCM formula could be sustained over a period of 3 months after treatment cessation and may back the findings of other investigations that have asserted the long-term effectiveness of TCM. 28,51
Although there were no significant differences on the CBCL Withdrawn subscale between T1 and T2 as well as T2 and T3, the decrease of observed withdrawn behavior from baseline to the sixth month was significant. A possible explanation could be that withdrawn behavior was dependent on improvements in other symptoms (e.g., anxiety/depressed) and thus changes in this domain could be more gradual overtime. The general reduction of ADHD symptoms and related psychopathology, improvements in functioning accompanied by the absence of side effects among participants suggest that the TCM formula has potential therapeutic benefits and is safe for consumption among children with ADHD, and may be consistent with research that have reported that TCM is well tolerated with limited side effects. 23 –26 Accompanied by the high parental satisfaction rates that were also observed in previous local studies, 32 the potential for this TCM formula as an adjunctive treatment for children with ADHD is thus encouraging and permits future RCTs to evaluate its efficacy.
Limitations and future research
This feasibility study is the first of its kind in Singapore and employed standardized diagnostic criteria, reliable and well-validated instruments to examine both short and long-term changes in psychopathology among CAM users. However, despite the positive findings observed, this study does not demonstrate efficacy of the TCM formula due to the lack of controls as well as participant, parental, and physician blinding. The significant short-term reductions in ADHD symptoms and improvements in functioning could be the result of placebo effects as well as reporting biases. This possibility is further supported by the finding that these benefits appear to be sustained even after treatment cessation. As the majority of participants were of Chinese ethnicity, cultural influences and practices could potentially generate a large placebo effect. With TCM being deeply rooted within the Chinese heritage, 32 the accompanying cultural acceptance, generally positive attitudes and beliefs as well as consequent better medication adherence could explain the present observed findings, which has been asserted by other research. 52 In the same vein, because participants were predominantly of Chinese descent, the treatment response, attitudes, and acceptability of this TCM preparation may not be generalizable to individuals of other ethnicities. Previous studies have indeed shown that the response and tolerability of TCM intervention varies across ethnicities. 53,54
As perceptively indicated by Lan et al., many TCM investigations lacked randomization, with most being open label trials and vulnerable to selection, performance, and measurement biases. 22 There is hence a need for double-blind RCTs using representative multicenter samples to support efficacy and overcome the low methodological quality of many TCM studies. Furthermore, more objective biomarkers such as blood, urine, and stool analyses can also be employed to objectively examine the safety and tolerability of TCM formulations, as demonstrated by a notable study. 20
Although TCM has been purported to have a delayed onset of therapeutic effects as well as having sustained effects, the duration of sustained therapeutic benefits cannot be readily established. This is further complicated by a combination of different varieties of herbs in TCM formulations, the majority of them have not been assessed for their pharmacokinetic profiles. Nonetheless, TCM treatment emphasizes on restoring functional balance and harmonizing the body, mind, and spirit 19,20 by adopting principles of compatibility and syndrome differentiation to determine the precise treatment of childhood ADHD. 55,56 In addition, TCM physicians tend to prescribe customized interventions for each patient according to their experience and expertise. 57 Although these factors distinguish TCM from other treatments, they inadvertently also render it difficult for western medicine practitioners to comprehend and validate due to differences in clinical methodologies assessing safety and efficacy. 58 –60 Despite its various limitations, TCM has been gaining popularity among children with ADHD 25 and seems promising as a viable adjunctive treatment for ADHD. With greater appreciation of TCM over time, more health care institutions internationally have started incorporating TCM interventions, paving the way toward a more holistic model of treatment.
Conclusions
This study suggests that TCM is relatively safe and has potential therapeutic effects in a group of children with ADHD. However, the findings could be subjected to placebo effects and reporting biases from physicians, participants, as well as their respective parents. Future double-blind RCTs should be conducted on this particular TCM formula to examine its efficacy.
Footnotes
Acknowledgments
This study would not have been possible without the invaluable contributions and dedication of the TCM physicians and staff from Science Arts Co. Pte. Ltd. The authors would also like to thank the Neuro-Behavioral Clinic at the Institute of Mental Health for their guidance and support.
Authors' Contributions
S.H.O. and Z.W.L. are the principal investigator and co-principal investigator of the study, respectively. S.H.O. and Z.W.L. both conceptualized the study, and wrote the article. Z.W.L. also provided statistical analysis of the data. Y.H.X., C.G.L., and D.F. gave significant inputs to the running of the study and to the article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported in part by a grant from the Institute of Mental Health Institutional Block Grant and Woodbridge Hospital Charity Fund.