
Abstract
Objectives:
To assess the efficacy and safety of mecobalamin on peripheral neuropathy.
Background:
Mecobalamin is an active form of vitamin B12 that has been suggested to be beneficial in improving nerve conduction and neuropathic pain symptoms. Although it is already widely used in Asia for the treatment of peripheral neuropathies, its efficacy remains unclear.
Methods:
Relevant electronic databases were systematically searched for randomized controlled trials investigating the efficacy and safety of mecobalamin on peripheral neuropathy, from inception through December 2019. Study selection, data extraction, and quality assessment were performed independently by two reviewers. The clinical therapeutic efficacy, pain score, neuropathic symptom score, nerve conduction velocities (NCVs), and adverse events of mecobalamin were assessed and were pooled by using a random-effects model. Heterogeneity was assessed by I2 and chi-squared tests.
Results:
Fifteen studies with 1707 peripheral neuropathy patients caused by diabetic peripheral neuropathy and herpetic neuropathy were included. Based on Cochrane's risk of bias criteria, most of the included studies (11/15, 73%) were rated high risk of bias, whereas 20% and 7% were rated some concerns and low risk of bias, respectively. In terms of the proportion of patients achieving clinical therapeutic efficacy, mecobalamin alone (risk ratio [RR] = 1.17; 95% confidence interval [CI] 1.03–1.33) and mecobalamin in combination (RR = 1.32; 95% CI 1.21–1.45) are more effective than active control. For NCV outcomes, only mecobalamin combination treatment was effective. Neither mecobalamin alone nor mecobalamin in combination is effective on the pain score and neuropathic symptom outcomes. No serious adverse events associated with mecobalamin were reported during the treatment periods.
Conclusion:
Our findings indicate that mecobalamin in combination may be effective in improving clinical therapeutic efficacy and NCV outcomes for peripheral neuropathy patients, but the evidence is not clear for mecobalamin alone. More high-quality studies are required to confirm this finding.
Introduction
Peripheral neuropathy is one of the most prevalent neurologic conditions worldwide and a common reason for neurologic consultation. 1 The prevalence of peripheral neuropathy is 2.4% in the general population, though it increases with age, reaching 8.0% in those older than 55 years. 2,3 Symptoms include tingling, burning, numbness, chronic pain, slow nerve conduction, and loss of sensation. 3 –5 Although the pathogenesis is unclear, peripheral neuropathy resulting from deterioration of the peripheral nerves is associated with cancer, herpes zoster or HIV infection, diabetes, and dysproteinemic disorders. Diabetes and sequelae of herpes zoster are associated with two specific types of peripheral neuropathy: diabetic peripheral neuropathy (DPN) and herpetic neuralgia (HN). 5 –7 The prevalence of DPN in diabetic patients (13%–68%) 8 and of HN after herpes zoster infection (5%–20%) are high. 9 Moreover; both have a significant impact on patient functional health and quality of life. 10,11
DPN is characterized by a progressive loss of nerve fibers after prolonged hyperglycemia, increased oxidative stress, and homocysteinemia. 5,12 HN, the debilitating sequelae of herpes zoster, can be divided into acute or subacute herpetic neuralgia (SHN) and postherpetic neuralgia (PHN). SHN is characterized by neuropathic pain occurring within 30–120 days of the onset of the herpes zoster infection, whereas PHN is neuropathic pain occurring after 120 days of infection onset. 7,10,13 The pathogeneses of pain in peripheral herpetic neuralgia are diverse and not fully understood, limiting their treatment. 6,12 Although several medications for the treatment of peripheral neuropathy are available, including tricyclic antidepressants, such as amitriptyline and nortriptyline, and antiepileptic drugs, such as gabapentin and pregabalin, 5,12,14 adverse drug reactions and questions regarding their efficacy limit their use.
Mecobalamin, a coenzyme form (active form) of vitamin B12, has a special affinity for neural tissues. Although all forms of vitamin B12 incorporate cobalt, the various forms differ on their sidechain at the cobalt group. For example, cyanocobalamin (or cobalamin), the common form of vitamin B12, contains a cyanide (-CN) sidechain; whereas mecobalamin (or methylcobalamin) contains a methyl (-CH3) sidechain. In comparison with the common form of vitamin B12, substitution of the cyanide group for a methyl group in mecobalamin increases its uptake by the subcellular organelles of neurons. This vitamin promotes myelination and transport of the axonal cytoskeleton, helps maintain the nervous system, and regenerates peripheral nerves. 15 –17
Because of its more effective systemic or local delivery, mecobalamin may show improved treatment of nervous disorders. Although the U.S. Food and Drug Administration has not approved mecobalamin for treatment of any type of peripheral neuropathy, 18,19 mecobalamin has been widely used for the treatment of DPN elsewhere, especially in Asia. In China, the National Medical Products Administration and Chinese practice guidelines have approved mecobalamin for the treatment of DPN. However, evidence for the effectiveness of mecobalamin treatment of DPN and HN is still controversial. 20 –31 Therefore, we have conducted a systematic review and meta-analysis of relevant randomized controlled trials (RCTs) evaluating the efficacy and safety of mecobalamin for the treatment of peripheral neuropathy due to diabetes and herpes zoster infections.
Materials and Methods
This systematic review was conducted according to the Cochrane Collaboration framework guidelines, 32 and the reporting follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 33 The review protocol can be accessed on PROSPERO (CRD42017059114).
Search strategies and study selection
The following databases were used to search for original research articles: EMBASE; PubMed; Cochrane Central Register of Clinical Trial; CINAHL; Scopus; Web of Science;
The inclusion criteria for research articles were RCTs investigating the clinical effects of any mecobalamin formulation on peripheral neuropathy diseases (including DPN), PHN, or SHN. Studies investigating other forms of vitamin B12 were excluded.
The titles and abstracts of all retrieved articles were initially screened by one investigator (S.T.) and confirmed by another investigator (R.S.). The full texts of potentially eligible articles were then independently examined by two investigators (S.T. and R.S.) to ensure that they fulfilled the eligibility criteria. Disagreements between the investigators were resolved by discussions with W.C. and P.P.
Data extraction and quality assessment
One investigator (S.T.) extracted the data, and this was confirmed independently by another investigator (R.S.). Discrepancies were resolved by discussion with a third investigator (W.C. or P.P.). A standardized extraction form was used to obtain the following information from each article: author; year of publication; study design; patient and intervention characteristics; sample size; duration of therapy; and outcome measurements.
The same process that was used in data extraction was also used to assess the quality of all included studies. The Cochrane risk of bias 2.0 tool was used for this purpose. 34 This tool examines five major sources (domains) of bias, including randomization process, intended intervention deviations, missing outcome data, outcome measurement, and selecting outcome report. The risk of bias in each study, against each source, was judged as low, high, or some concern risk of bias. We determined the overall risk of bias for each outcome (across domains) within studies as follows: (1) Low risk of bias, when all domains are assessed as being at low risk or plausible bias is unlikely to seriously alter the results; (2) Some concern risk of bias, when at least one domain is assessed with some concern risks, or plausible bias raises some doubt about the results; and (3) High risk of bias, when at least one domain is judged as being at high risk, or plausible bias seriously weakens confidence in the results.
Disagreements between the reviewers were settled through discussion and consensus with a third party (W.C. or P.P.). Where data were missing, reviewers attempted to contact the authors to retrieve the information.
Outcome measures and statistical analyses
The primary outcome was clinical therapeutic efficacy, defined as improvement of symptoms including pain, numbness, tingling and weakness, tendon reflex, and nerve conduction velocity (NCV). We defined clinical therapeutic efficacy as effective (alleviated subjective symptoms, improved tendon reflex, and increased NCVs by at least 3 m/s) or ineffective (no improvement in symptoms, tendon reflex, or NCVs). The secondary outcomes included: improvement of NCV, including both sensory NCV (SNCV) and motor NCV (MNCV); pain score, including both visual analogue score (VAS) and numerical rating score (NRS); neuropathic symptom score (NSS); and adverse events. Pooled effects were calculated and stratified according to outcomes. Data summary statistics of dichotomous outcomes were expressed as a risk ratio (RR) with a 95% confidence interval (CI), whereas summary statistics of continuous outcomes were expressed as weighted mean difference. Statistical heterogeneity between studies was assessed by using the chi-squared test and I2 . A significant difference for heterogeneity test was considered when p < 0.05, and substantial heterogeneity was represented by I2 of 50% or more. 35 If there was evidence of high heterogeneity, we attempted to explore the reasons for it, and subgroup analyses were performed where possible. Publication bias was assessed by using Egger weighted regression statistics and a visual inspection of funnel plots. 36,37 The Dersimonian and Laird random-effects model 38 was employed for all analyses.
Sensitivity and subgroup analyses
To ensure robustness of results, sensitivity analysis was performed by using a fixed-effects model 39 and only high-quality trials were included for analysis. In addition, subgroup analyses were performed based on types of neuropathy, duration of treatments, dosage form of mecobalamin, and active versus placebo control.
Results
Search results
The PRISMA flow diagram of studies is shown in Figure 1. Overall, 834 related articles were identified through database searching. After duplication removal, 720 articles were eligible for screening. Based on title and abstract screening, 51 articles in English, Chinese, and Japanese were selected for full text review. Subsequently, 36 articles were excluded after full text review: 12 articles evaluated other forms of vitamin B12; 15 articles did not evaluate the effects of mecobalamin; five articles were non-RCTs; and four articles were narrative reviews. Finally, 15 articles 40 –54 in English and Chinese were included in our study.
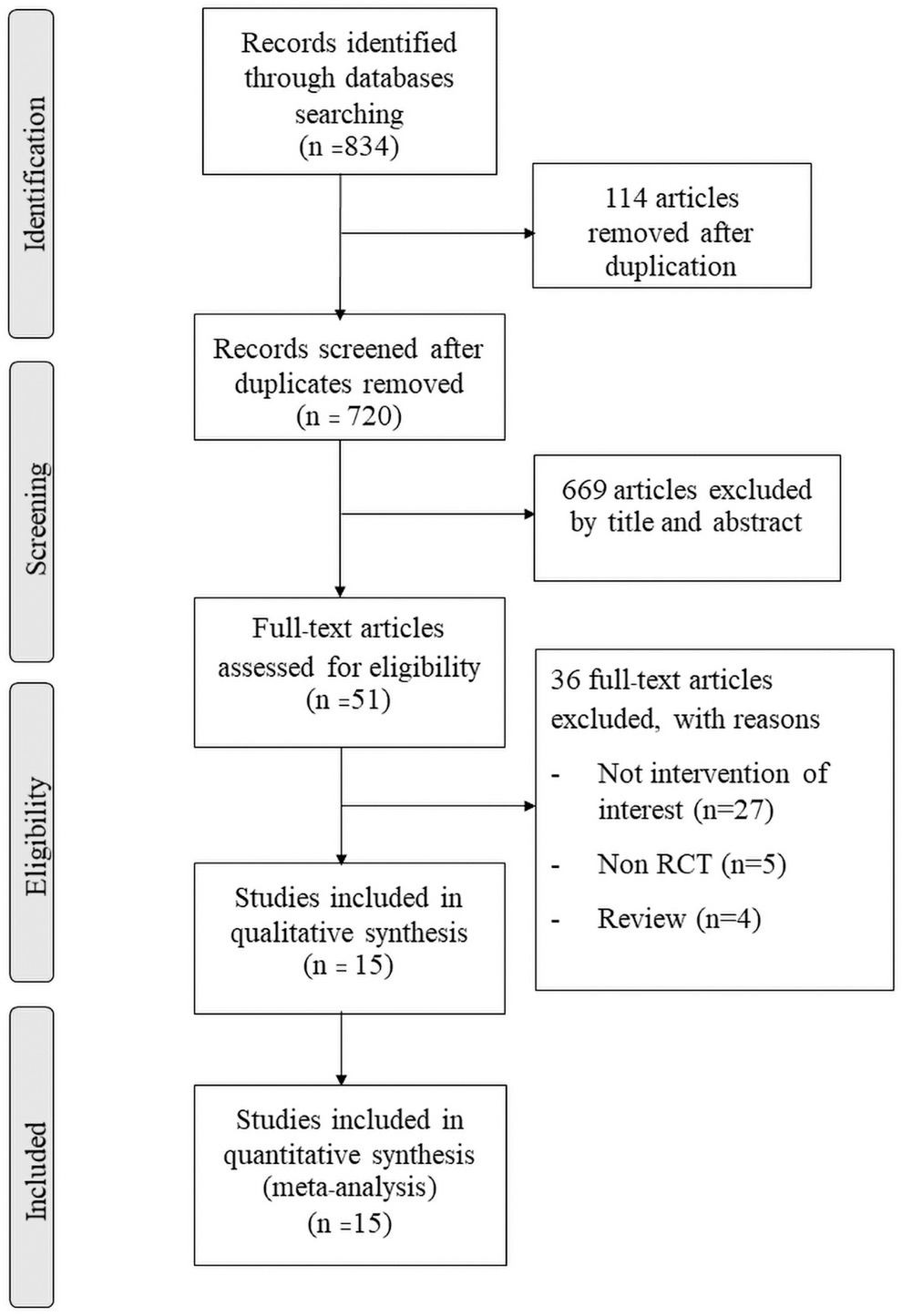
Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow chart of study selection. RCT, randomized controlled trial.
Characteristics of included studies
The characteristics and methodological quality of included studies are summarized in Table 1. Among the included studies, 14 studies were conducted in China and one in the United States. The dates of publication ranged from 1999 to 2016. Most studies (13/15) were single-center ones with open-label design, and half of them had sample sizes of fewer than 100 patients. A total of 1717 patients were involved, including 1379 DPN patients from 12 studies, 40 –46,48–50,52,53 240 PHN patients from two studies, 47,51 and 98 SHN patients from one study. 54 The age of the included patients ranged from 47 to 67 years of age. Several studies (7/12) did not report the types of diabetes associated with DPN. Six studies used mecobalamin alone, five studies used mecobalamin in combination with other active treatments, and four studies compared mecobalamin alone and mecobalamin in combination. Mecobalamin was commonly taken orally (1.5 μg/day), with treatment duration ranging from 10 to 24 weeks for DPN, and from 6 days to 4 weeks for HN. Chinese herbal medicine (e.g., puerarin, tonxingluo, xiangdan) and acupuncture were commonly used as comparators. Only one study compared mecobalamin with placebo. 49
Study Characteristics and Methodological Quality of Included Studies
AE, adverse events; ALC, acetyl-L-carnitine; C, comparator group; DPN, diabetic peripheral neuropathy; EOD, every other day; High, high risk of bias; IM, intramuscular; IV, intravenous; Low, low risk of bias; MC, mecobalamin; MNCV, motor nerve conduction velocity; N/A, data not available; NCV, nerve conduction velocity; NDS; neuropathic disability score; NRS, numerical rating scale; NSS, neuropathic symptom score; NTS, neuropathic total symptom score; PHN, postherpetic neuropathy; ROB, risk of bias; SC, subcutaneous; SHN, subacute herpetic neuralgia; SNCV, sensory nerve conduction velocity; Some concern, some concern risk of bias; T, treatment group; TCM, traditional Chinese medicine; VAS, visual analogue scale.
Methodological bias of the included studies
Regarding the quality of the 15 included studies, 11 studies (73%) were rated high risk of bias, 3 (20%) were rated some concern risk of bias, and 1 (7%) was rated low risk of bias. The major reason for the high risk of bias judgment was the use of non-blinded studies with non-objective outcome data (Table 2).
Risk-of-Bias Assessment of Randomized Controlled Trials
Overall efficacy
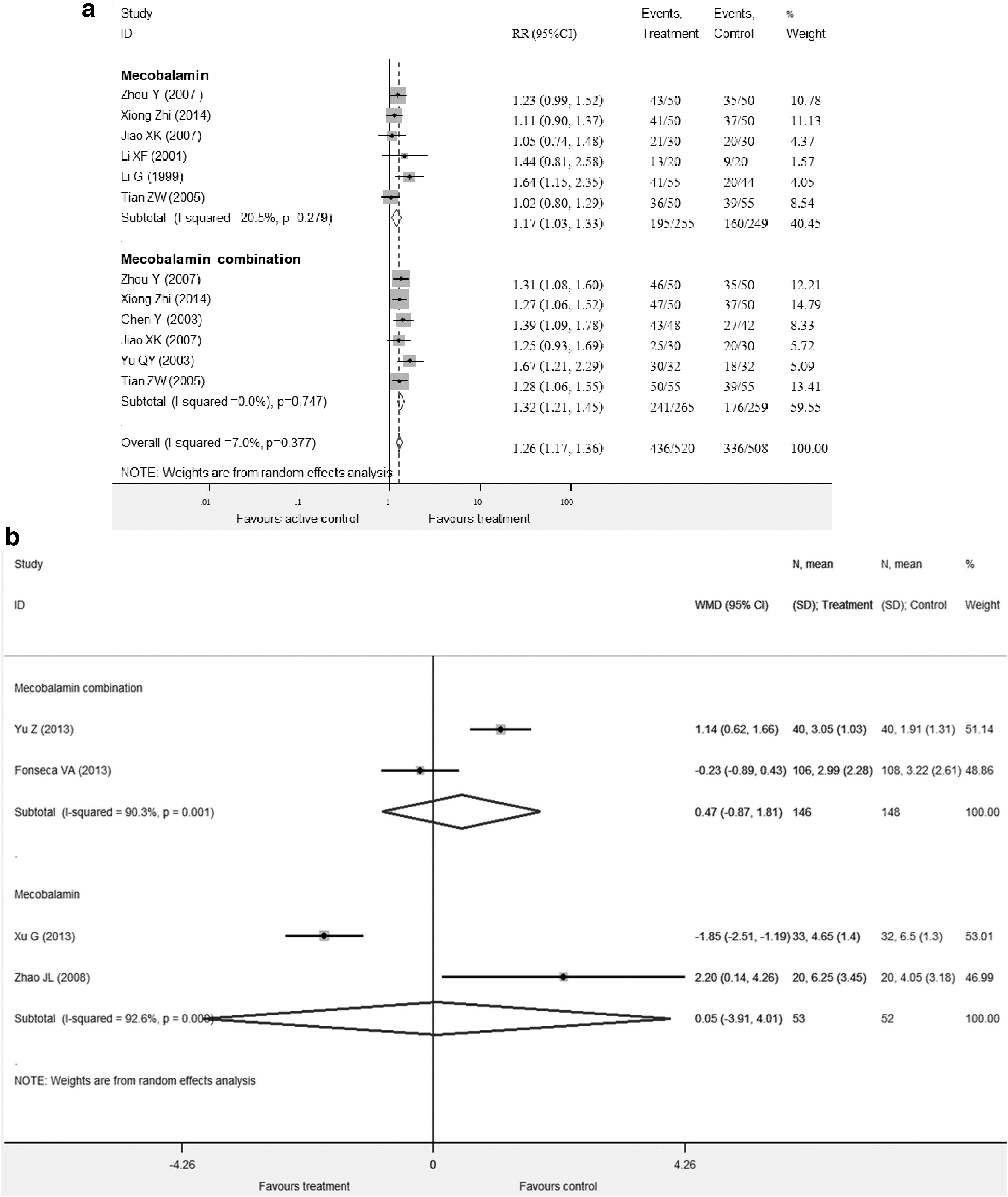
Eight studies involving 852 patients (692 DPN patients and 160 PHN patients) reported the proportion of patients who achieved a clinically effective outcome. 41 –43,45–47,50,53 Our meta-analysis demonstrated that mecobalamin alone was more effective on peripheral neuropathy than active controls (RR = 1.17; 95% CI 1.03–1.33; p = 0.015), with mild heterogeneity among studies (I 2 = 20.5%, p = 0.279). The proportion of patients who achieved clinical therapeutic efficacy was even higher for mecobalamin combination treatment with active control (RR = 1.32; 95% CI 1.21–1.45), with no evidence of heterogeneity among studies (I 2 = 0.00%, p = 0.747) (Fig. 2a). However, a subgroup analysis by neuropathic type revealed that only DPN patients showed a difference between the two groups (mecobalamin alone, RR = 1.22; 95% CI 1.06–1.40; p = 0.006; I2 = 16.0%, p = 0.312 vs. mecobalamin in combination with active treatments, RR = 1.34; 95% CI 1.21–1.48; I2 = 0.00%, p = 0.636) (Table 3).
Success in clinical effective outcome
Subgroup Analyses for Clinical Therapeutic Efficacy Outcome
The main analysis with significance was shown in bold values.
CI, confidence interval; DPN, diabetic peripheral neuropathy; IM, intramuscular; IV, intravenous; MC, mecobalamin; PHN, postherpetic neuropathy; RR, risk ratio.
Pain scores
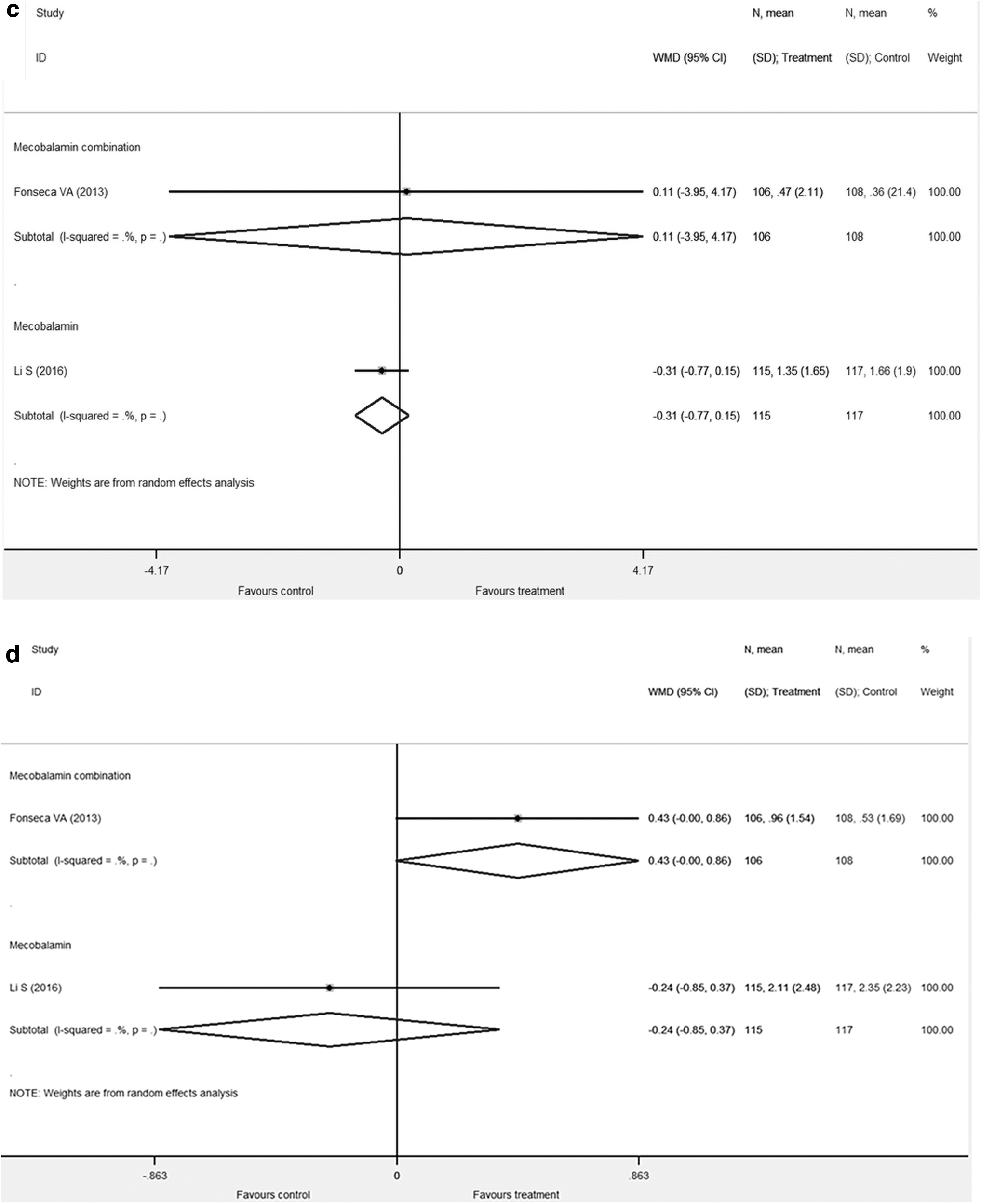
Pain scores measured by VAS and NRS were used for pooled analysis. Four trials, totaling 452 patients (274 DPN patients, 98 SHN patients, 80 PHN patients), investigating the effect of mecobalamin on pain reduction compared with other active treatments, 49,51,52,54 were included in the meta-analysis. Pain scores were significantly reduced in both groups when compared with the baseline. Our meta-analysis results indicate that pain scores in both mecobalamin alone and mecobalamin in combination groups were not significantly different from those in the active control groups (Fig. 2b). Two studies, 48,49 totaling 446 patients, reported NSS outcomes, including neuropathic disability score (NDS) and neuropathic total symptom score (NTS). Changes in NDS and NTS of mecobalamin in combination or mecobalamin alone were not different from the control group (Fig. 2c, d).
Nerve conduction velocity
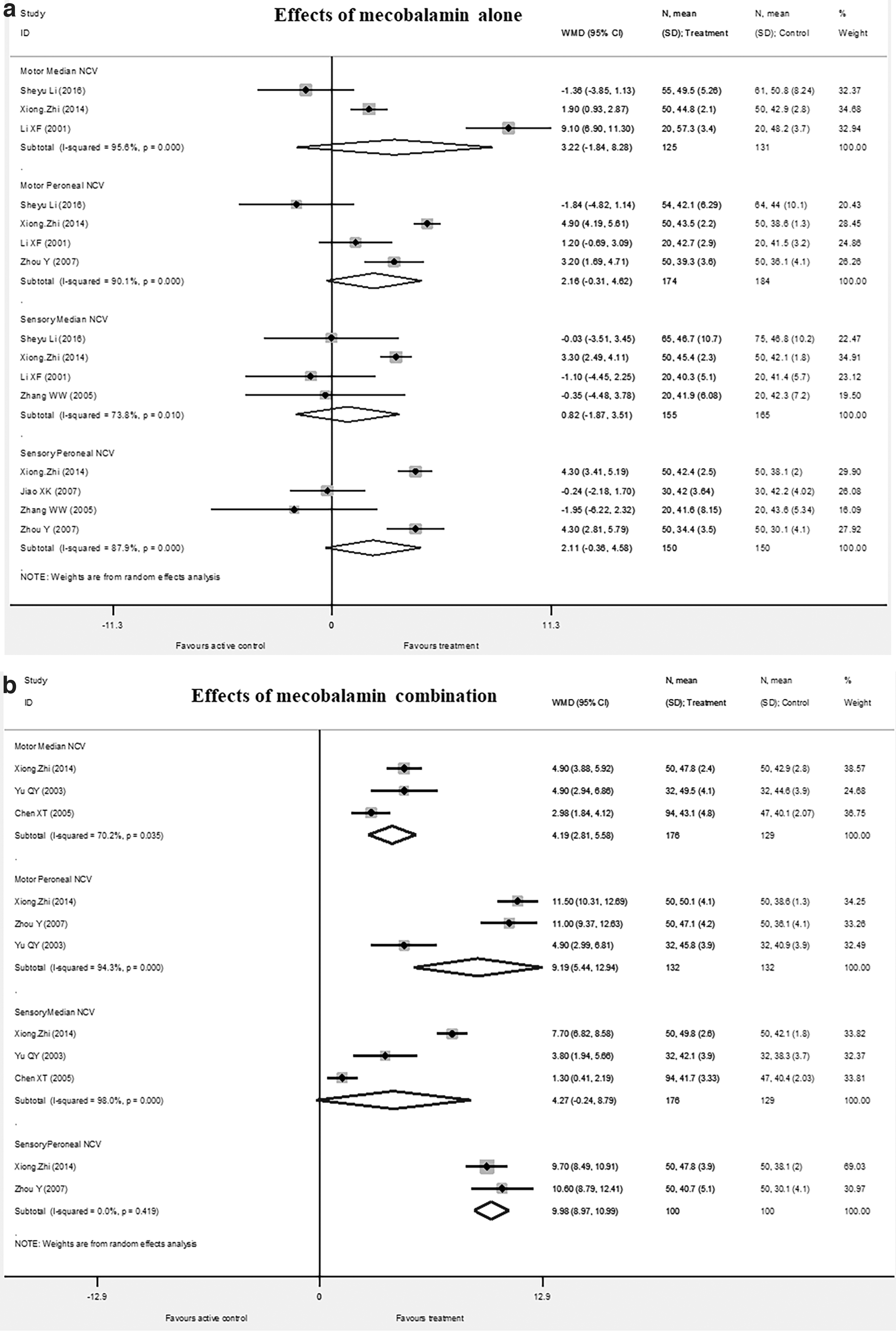
Nine studies (n = 1015) reported NCV outcomes, including median SNCV, peroneal SNCV, median MNCV, and peroneal MNCV. Six studies, totaling 667 patients, reported the median SNCV outcome 40,43 –45,48,50 ; whereas five studies, totaling 538 patients, reported the peroneal SNCV outcome. 42,44,46,50,53 Five studies, totaling 627 patients, and six trials, totaling 744 patients, reported the median MNCV, 40,43,45,48,50 and the peroneal MNCV 43,45,46,48,50,53 (Table 1). A pooled analysis of the effects of mecobalamin on all NCV types is shown in Figure 3a and b. The results indicate that NCV after mecobalamin alone was not significantly different from that of the control group (Fig. 3a). For mecobalamin combination, pooled-analysis results indicate that median MNCV, peroneal MNCV, and peroneal SNCV were significantly different compared with the active control group (Fig. 3b).
Nerve conduction velocity outcomes for mecobalamin
Adverse events
Safety outcomes were reported in 8 out of 15 studies with 987 patients. 40,41,44,45,48,49,53,54 The numbers of adverse events were comparable in the mecobalamin and active control groups. There was no report of serious adverse events or death during administration of any form of mecobalamin for one to 24 weeks. The most common adverse events reported in the mecobalamin (mecobalamin alone and in combination) groups were gastrointestinal symptoms (abdominal distension, 4 cases; diarrhea, 7 cases; and nausea, 5 cases), enhanced local skin redness and irritation (13 cases), edema (5 cases), and dizziness (4 cases). These adverse events were reported to be of mild severity. In two included studies, 48,54 the dropout rates were considerable, although the authors indicate that this was not related to treatment interventions. The dropout rates were 23 out of 181 (12.7%), 14 out of 117 (12.0%), and 4 out of 42 participants (12.5%), for mecobalamin, acetyl-L-carnitine, and lidocaine, respectively.
Publication bias
For clinical therapeutic efficacy outcome, publication bias tests using funnel plot, Begg's test, and Egger's tests indicated that there was no evidence of publication bias (p = 0.248) (Fig. 4).

Funnel plot for clinical effective outcome of mecobalamin and control group. RR, risk ratio.
Sensitivity analysis
It was not possible to perform sensitivity analysis by excluding data of studies with low quality from the meta-analysis for the following reasons: (1) the number of pool-able studies was limited; and (2) most studies were rated low quality (high or some concern risk of bias). However, when changing the model of analysis to the fixed-effects model, the main result, an effect of mecobalamin on clinical efficacy, was not changed.
Subgroup analysis
The results of the subgroup analyses for clinical therapeutic efficacy outcome are presented in Table 3. According to the subgroup analyses by type of peripheral neuropathy, dosage form of mecobalamin, and duration of treatment, mecobalamin alone and in combination is effective in patients with DPN during short-term treatment (≤4 weeks). Data were insufficient to determine the long-term effects (>4 weeks) of both mecobalamin regimens. All dosage forms showed clinical benefits during mecobalamin in combination treatment, but not with mecobalamin alone. Only the study of Fonseca et al. 49 compared mecobalamin with placebo. This study was not included in the primary outcomes, and therefore the placebo control did not affect the main outcome.
Discussion
Our systematic review and meta-analysis demonstrate the clinical efficacy of mecobalamin (used either as monotherapy or in combination with other treatments) on peripheral neuropathy with a comparable adverse effect compared with other interventions (tonxingluo, puerarin, vitamin B, moxibustion, acupuncture).
In 2005, Jia et al. 20 determined the effects of mecobalamin on DPN. They found that mecobalamin had a greater clinical efficacy on DPN patients compared with other interventions or other forms of vitamin B. The findings of our systematic review and meta-analysis are similar to this previous study. 20 Although our study determined the effects of mecobalamin on different types of peripheral neuropathies, the subgroup analysis indicated the greater clinical efficacy of mecobalamin for treating DPN.
The proposed mechanisms for mecobalamin efficacy include accelerating transmethylation in nerve tissues, increasing myelination, promoting conversion of homocysteine to methionine, decreasing oxidative stress and advanced glycosylated end-products, and correction of impaired neural signaling of protein kinase C (the main pathophysiology of DPN). 15,16 Mecobalamin also acts directly on the neuron and has a more rapid onset of action than other forms of B vitamin. 21 Possible mechanisms of other treatments, such as Chinese medicines (tonxingluo, puerarin), include improved blood flow to the nerves; attenuation of endothelial dysfunction via anti-oxidation and anti-inflammation properties 55 –57 indirectly affect the neurons. Therefore, these treatments require a longer time than mecobalamin to achieve clinical efficacy.
For patients with HN, there were insufficient data to support the use of mecobalamin. The reasons for the absence of an effect may be related to complex mechanisms of varicella zoster virus reactivation in neurons, 58 and to the characteristics of pain and discomfort symptoms related to HN. 47,51,54
Current evidence indicates that the benefits of mecobalamin on pain perception are comparable to the control group, which includes acupuncture, moxibustion, lidocaine, and placebo. Acupuncture, moxibustion, and lidocaine are considered active treatments that are effective for pain therapy. Acupuncture and moxibustion are complementary treatments and are forms of Oriental Medicine, Traditional Chinese Medicine, or Asian Medicine. Acupuncture has been used since ancient times to treat symptoms of DPN. 25 Moxibustion is a form of heat therapy involving the burning of mugwort (artemisia vulgaris) on or near the skin to relieve pain. 26,59 Lidocaine, a sodium channel blocker, is recommended for the treatment of localized peripheral neuropathic pain, and it is used alone or in combination with other treatments. 12 Most of the included trials indicate that mecobalamin was safe when used for 1–24 weeks. Similar to previous studies, our study indicates that mecobalamin has no known toxicity at the dosage used, is well tolerated, and has a safety and tolerability profile similar to that of the placebo. 17,23,25,26,28,29,60,61
The strength of our study is that it is a comprehensive summary of the effects of mecobalamin, undertaken in accordance with high standards of systematic review and meta-analysis and aligned with PRISMA. 33 Meta-analyses of RCT are at the top of the hierarchy of clinical evidence. In addition, we updated the current evidence on efficacy and safety of mecobalamin in diabetic neuropathy, and we included another major peripheral neuropathy, HN, in this review.
Although our systematic review and meta-analysis demonstrate the clinical efficacy of mecobalamin for peripheral neuropathies, interpretation and clinical application of these results should be performed with caution. The pooling results of each outcome were summarized based on the different dosage forms of mecobalamin. Therefore, a small number of included studies with a single-center and open-label design may have yielded an imprecise estimation, and some outcomes may have reached significance by chance. In addition, almost all included studies (14/15 trials) were rated as high risk or some concerns risk of bias. Hence, the current evidence may not be strong enough to support the effectiveness of mecobalamin over other treatment comparators for all types of peripheral neuropathies.
A number of limitations should be mentioned. Most of the included studies were low quality. Lack of blinding was a major reason for low methodological quality. Since pain outcome is subjective, if patients know about the intervention it may produce a positive effect. In addition, previous evidence suggests that some interventions, such as acupuncture, moxibustion, and the injection form of medicines, may be associated with a greater expectation than other therapies. The various types of comparisons, formulations of mecobalamin, and follow-up times (1–24 weeks) may also be major sources of heterogeneity. Therefore, further well-designed, large, multicenter, randomized placebo- or active-controlled trials investigating the long-term effects of mecobalamin on peripheral neuropathy are needed to support this evidence.
Conclusion
Based on current evidence, mecobalamin taken orally (1500 μg/day), intramuscularly, or intravenously (500 μg/day) (either as monotherapy or in combination with other treatments) may be effective and safe for the treatment of diabetic neuropathy. However, there are insufficient data to support an effect on PHN. A multicenter well-designed, randomized placebo or active-controlled trial investigating the long-term effects of mecobalamin on peripheral neuropathy should be performed to support current evidence.
Authors' Contributions
R.S. and S.T. conceived and designed the study, reviewed the quality of data, and wrote the article. All authors (R.S., S.T., W.C., and P.P.) performed the experiments, extracted the data, and read and approved the final manuscript.
Footnotes
Author Disclosure Statement
The authors declare that they have no conflict of interest.
Funding Information
This research project is financially supported by Mahasarakham University (Fast track 2020).