
Abstract
Objectives:
To determine the feasibility and acceptability of a heart rate variability biofeedback (HRVB) protocol in a focus group of Veterans with fibromyalgia (FM).
Design:
A multimethod feasibility and acceptability study.
Settings/location:
A Veterans Health outpatient pain medicine clinic in the southern United States.
Subjects:
The researcher enrolled seven women and three men between the ages of 33 and 68 years with a diagnosis of FM.
Interventions:
Participants practiced HRVB on the emWave2 at home for 20 min twice daily for 7 weeks.
Outcome measures:
Feasibility to adhere to the HRVB protocol was measured using the practice frequency and time (minutes) data collected from the emWave2. The author compared the individual reports from participants with the Credibility/Expectancy Questionnaire to measure the acceptability of the intervention. In addition, the principal investigator evaluated data from the Short-form McGill Pain Questionnaire (SFMQ) and the Revised Fibromyalgia Impact Questionnaire (FIQR) at the baseline and weekly study visits for a signal of efficacy for pain control, functional status, and quality of life (QOL).
Results:
The majority of participants (80%) expected 50% or more improvement in their pain, and (70%) felt HRVB would reduce their FM-related pain by 50%–80%. The mean daily practice frequency rate was 0.80. The mean practice duration was 19.36 min. Pain score differences from the SFMQ were insignificant preintervention and postintervention. The mean total FIQR scores postintervention improved by 18.1 points.
Conclusions:
Findings suggest twice-daily HRVB practice protocol is not feasible. However, 20-min HRVB sessions were feasible and acceptable. Improved FIQR scores post-treatment suggest HRVB may be an effective strategy to improve functional status and QOL for Veterans with FM.
Introduction
Fibromyalgia (FM) is a complex condition with predominant symptoms of pain, fatigue, depression, and sleep deprivation leading to a decrease in functional status and diminished quality of life (QOL). 1 FM affects 10 million individuals in the United States, contributing to a 1%–2% loss of national productivity 2,3 and $12–14 billion per year in national health care costs. 2 The FM cost to the military health care system in 2006 was $105.6 million, with an average individual cost of $12472; this is five times higher than the costs on non-FM diagnosed beneficiaries. 4
The Department of Veterans Health Administration (VHA) and the Department of Defense recognize FM as an illness related to deployment during wars in the Persian Gulf and Afghanistan. 5,6 Individuals diagnosed with FM have a higher prevalence of traumatic events such as those experienced in combat. 7,8 Carrying over 80 pounds of equipment daily for 6–12 months during multiple deployments is associated with the repetitive muscular injuries that resulted in more than 50% of service members reporting chronic pain not related to direct injuries such as shrapnel, gunshots, or blasts. 6,9,10
Pathophysiology of FM
In individuals with FM, functional magnetic resonance imaging demonstrates disruption of the pain network connectivity, possibly explaining diffuse chronic pain. 11 In addition, the default mode network (DMN), brain regions engaged in self-referential thinking, is disrupted during tasks like visual and cognitive attention, explaining memory, and cognitive impairment. 12,13 An abnormally increased level of connectivity between the DMN and the insular cortex may also contribute to increased pain levels. 13 Finally, a dysfunction of the cardiac autonomic nervous system (ANS), characterized by higher sympathetic and lower parasympathetic cardiac autonomic modulation, is associated with diminished heart rate variability (HRV) and worsening QOL. 14,15
Heart rate variability
HRV, the time measurement of the oscillations of the R-to-R intervals, 16 –18 reflects heart-brain interaction 17 and the ANS. 17,19 Spectra analysis of the high frequency (HF) and low frequency (LF) bands 20 in HRV measures the interaction of the sympathetic and parasympathetic nervous systems. 15,19,21 Significant psychological and physiological activities and slow breathing 20 affect the LF bands. Optimal HRV, cardiac coherence, is an ordered, harmonic cardiac pattern reflecting positive emotions and a general sense of well-being. 19 Low HRV, cardiac incoherence, reflects decreased resistance to stress, anxiety, and decreased emotional adaptability, 15,17,19,22 factors known to exacerbate chronic pain. Self-regulation techniques that improve HRV can reduce pain, improve physical activity, and improve cognitive function. 19
HRV biofeedback
Heart rate variability biofeedback (HRVB) enables self-regulation by using technology to guide deep breathing at an average rate of six breaths per minute. Deep breathing, an autonomic maneuver, may intensify the interaction between autonomic and nociceptive pathways, 14 HRV coherence (HRC), and ANS regulation. 14,19,23 –26 Repeated sessions of HRVB can sustain improved HRC and, optimize stress resistance and emotional adaptability to decrease pain, and increase overall well-being. 19,23,24
The purpose of this study was to ascertain the feasibility and acceptability of an HRVB protocol for Veterans diagnosed with FM. Feasibility and acceptability were determined through adherence to the treatment protocol, as ascertained by the emWave2, a handheld device that objectively monitors HRV and records session frequency and duration. In addition, the research collected data related to HRC, qualities of pain, and FM symptoms, including overall function and QOL, as an initial signal of the efficacy of HRVB.
Methods
Design/participants
The researcher used a multimethod design to inform the following questions: (1) Is it feasible for Veterans to adhere to the recommended HRVB protocol? and (2) Will Veterans find this intervention acceptable? An Institutional Review Board (IRB) and VA Medical Center, Research and Development Board, approved study Pro00079144. No concrete recommendations for sample size on feasibility studies exist. 27 The author based sample size on the pragmatics of recruiting from the VA, patient flow, and budget constraints for purchasing equipment, and therefore, a benchmark of 10 study participants was established.
The principal investigator (PI) placed IRB-approved recruitment flyers in the lobbies and examination rooms of primary care and mental health clinics of one Southeastern U.S. Veterans Administration (VA) clinic. The PI distributed flyers to clinic staff and provided time for questions and answers about the planned study. The health care providers and medical staff were not involved in the research and did not receive any finders' fees.
Inclusion criteria included male and female Veterans of all races and ethnicities, ages 18 and older with a documented diagnosis of FM. Exclusion criteria were any significant cardiovascular disease, current use of heart rate-controlling medications, significant pulmonary disease, a psychosis diagnosis, self-reported pregnancy, or prior experience with HRVB.
Procedures
Consistent with prior studies and recommendations from the developers of the emWave2, 24,28 –30 the PI conducted eight once-weekly 1-h individual HRVB practice sessions with each participant after participants provided informed written consent. Study participants received a $5 gift card during each visit. During the initial visit, participants provided demographic data, completed the Credibility/Expectancy Questionnaire (CEQ), Revised Fibromyalgia Impact Questionnaire (FIQR), and Short-form McGill Pain Questionnaire (SFMQ). Each participant received an emWave2 handheld device to use in the clinic and to take home for practice. The PI demonstrated the functions and care of the equipment, including how to clip the enclosed photoplethysmograph (PPG) sensor on the participant's ear. The PI assisted with the configuration of initial settings to default level 1 (low) using the included Quick Start Guide. Participants practiced HRVB during the initial visit to understand the rising and falling light in the Heart Action Strip with each breath, indicating heart rhythm and HRC. The researcher instructed each participant to take slow rhythmic breaths to increase HRC. Coherence level indicator lights were monitored for low, medium, and optimal adherence. In addition, based on the protocols used by Lehrer et al., 31 participants were instructed to practice with the device at home for 20 min twice daily. The researcher provided the participants with a phone number to call if they had any difficulty between study visits.
During visits 2–8, participants completed the SFMQ and the FIQR and reviewed the results with the PI. The PI downloaded and reviewed the practice data from the emWave2, and discussed and developed strategies to overcome practice barriers and any usage difficulties. Participants practiced on their emWave2 for 20 min during each visit and received additional breathing technique coaching as needed.
Outcomes measures
The author evaluated practice frequency and time (minutes) data from the emWave2 as a measure of protocol feasibility and reviewed all data with each participant to improve self-efficacy and shift the individual's perception of helplessness to a sense of ability to self-improve. 32,33 Responses from the CEQ 34,35 measured treatment outcome expectancy and credibility. Four questions ask if individuals expect treatment to improve their symptoms (expectancy), and two ask about treatment believability and logic (credibility). 34,35 The CEQ has two rating scales, 1–9 (not at all to very much) and 0%–100% (not at all to very much). Percentage ratings are transformed linearly to a scale of 1–9 (minimum to maximum), allowing for a sum score ranging from 3 to 27 (minimal to maximum credibility and expectancy). 35 The CEQ has reported high internal consistency of the expectancy factor (Cronbach's α range 0.79–0.90), the credibility factor (Cronbach's α 0.81–0.86), and a total standardized α of 0.84–0.85 for both factors. 35
The SFMQ assesses 11 sensory and 4 affective descriptors of pain. 36 The FIQR measures individual functional status and QOL with 21 questions divided into 3 domains: function, global impact, and FM-related symptoms in the past 7 days. 37 Questions rate on a 0 to 10 numeric scale, with a better QOL being a lower total FIQR score. 37 The HeartMath® software calculated HRC as the ratio between LF HRV divided by the sum of the HF and LF. 38 The resulting average weighted score ranged from 0 to 200 (low to high coherence). 38
Analysis
The researcher analyzed protocol feasibility by calculating the median and mean responses of intervention frequency and time spent using a 95% confidence interval. We evaluated participant acceptability and satisfaction with the intervention through manifest and latent content analysis 39,40 of participant statements and compared this to data of the CEQ. The first author presented the qualitative data in a separate article.
Results
Participant characteristics
The researcher enrolled seven women and three men between the ages of 33 and 68 years (mean age = 47). Participants were white (n = 5), African American (n = 4), and Hispanic (n = 1), and 7 (70%) were married. All had at least some level of higher education (Table 1). Only three participants were employed. All participants had a mental health diagnosis, including depression (n = 6), anxiety (n = 2), and/or post-traumatic stress disorder (PTSD) (n = 4). Fifty to 60% of the Veterans self-reported that they never exercise (Table 2).
Participant Demographics and Baseline History
Key:
College: Bachelor's degree.
Graduate: Postbachelor's degree.
GED, general educational diploma; PTSD, post-traumatic stress disorder.
Self-Reported Weekly Exercise Frequency
HRVB practice
Frequency
The emWave2 software recorded all practice sessions. The mean daily practice frequency rate was 0.80, suggesting there were days when the participants did not practice. One participant practiced twice daily during the first week of the study, and thereafter only 1–1.3 times per day, but for extended times (25.3–39.3 min). One participant practiced during the first week (mean frequency 0.1), did not practice during week 2, then stopped attending, and did not return the emWave2, and therefore data collection ceased. Women practiced 21.46% more frequently than men (Table 3). Participants with depression practiced 24.4% more often than those with anxiety and 27.16% more frequently than those with PTSD. Not employed Veterans practiced 40.54% more regularly compared to those who were employed (Table 3).
Heart Rate Variability Biofeedback Practice Frequency and Time (Minutes)
PTSD, post-traumatic stress disorder.
Time (minutes)
The researcher instructed the participants to practice for 20 min. The mean practice duration was 19.36 and ranged from 0 to 58.1 (Table 3), suggesting participants practiced for the prescribed time. Women practiced 17.57% longer than men (Table 3). Veterans with PTSD practiced 22.21% longer than those with anxiety and 11.85% longer than those with depression (Table 3). Participants who were not employed practiced only 0.41% longer than those working (Table 3).
Credibility/Expectancy Questionnaire
Treatment acceptability correlates positively with treatment outcomes expectancy and credibility. 34,35 Nine of the participants believed HRVB is a logical treatment and anticipated it would successfully reduce their pain (n = 7). Most expected 50% or more improvement in their pain (n = 8). When asked about how the participants really feel, half of the participants (n = 5) felt that HRVB would reduce their pain by 50%–80%.
Revised Fibromyalgia Impact Questionnaire
The PI measured FIQR scores at baseline and during weekly study visits. The functional and global impact domain scores improved postintervention, suggesting a slight improvement in functional status after HRVB (Table 4). The mean scores from symptoms of FM were essentially unchanged (63.9–64.9), indicating HRVB did not affect symptoms of FM. The weekly mean total FIQR scores postintervention (128.5) were lower than baseline (146.6), indicating HRVB improved overall QOL.
Outcomes Measurements
FIQR, Revised Fibromyalgia Impact Questionnaire; HRC, heart rate variability coherence; SFMQ, Short-form McGill Pain Questionnaire.
Short-form McGill Pain Questionnaire
Pain scores were measured using the SFMQ at baseline and each weekly visit. Pain scores did not vary greatly preintervention and postintervention (Table 4). The mean total pain rating index score was 25.4 at baseline and 25.9 at weekly visits, suggesting there was no improvement or worsening of pain preintervention and postintervention.
HRV coherence
HRC was measured each time the participant practiced HRVB (Table 4). The mean HRC recorded at baseline was 1.0, with a range from 0.3 to 1.72. Postintervention, the mean score was unchanged (1.05); however, the broader range (0.46 to 2.38) suggests a 29.94% increase in HRC scores for postintervention. The highest ratings (1.83–2.52) were reported by the two participants who had the highest rates of HRVB practice frequency (1.1 and 1.9). While examining the frequency (n = 57) of mean scores, it was noted 7 out of 57 practice sessions resulted in a higher HRC maximum base score of 1.72, indicating most practice sessions (n = 50) did not result in improved HRC week to week (Fig. 1).
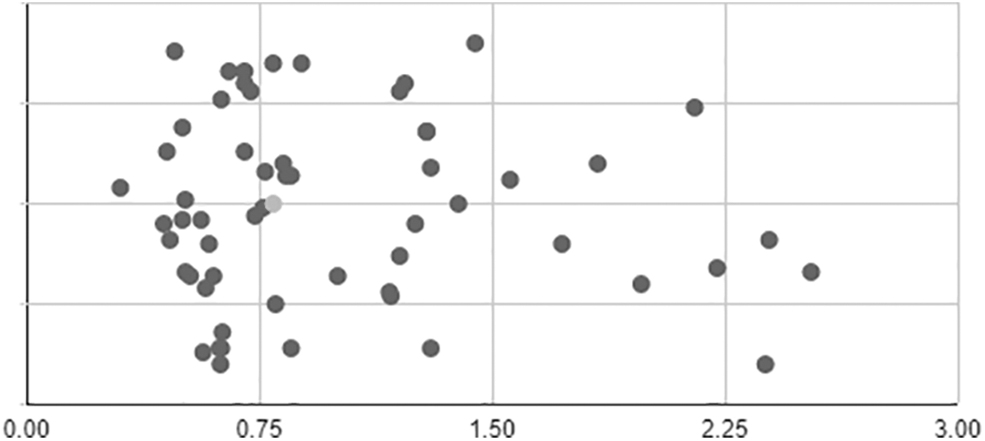
Scatter plot of heart rate variability coherence total means.
Discussion
The ANS dysfunction and diminished HRV associated with FM are generally not demonstrated in chronic musculoskeletal pain; thus, comparing treatment between these pain syndromes is challenging. 41,15 FM treatment must include an approach that prioritizes nonpharmacological methods and offers judicious pharmacological management. 1,42 Implementation of self-directed and self-managed interventions like HRVB can improve cognitive performance outcomes, 32,33 emotion regulation, stress resistance, and QOL. 21,24,26 However, Lehrer et al. 31 determined individuals cannot merely achieve and sustain HRC without training, and thus developed HRVB practice protocols.
Our data suggest that twice-daily HRVB practice sessions were not feasible. Poor adherence to the practice protocol was surprising based on favorable participant CEQ rates. In previous studies, treatment expectancy correlated positively with treatment outcomes. 34,35 This contradiction may be related to self-selection bias and may be minimized in a randomized controlled trial (RCT). Another factor to consider is participants' biases to a positive response on the CEQ to be included in the study.
Only one Veteran practiced twice daily for 1 week. He reported improved sleep and mood the first week. At subsequent visits, he reported a busy personal schedule and “getting out of the habit” as reasons for protocol noncompliance. Busy schedule was a common response among participants for protocol noncompliance. Thirty percent of participants were employed, which may have impacted twice-daily practice. The employed participants expressed discomfort of using the device around their co-workers because they feared the questions about the treatment and their FM diagnosis. HRVB improves emotional adaptability when used during times of increased stress or adversity, 19,23,24 so workplace practice should be encouraged. Future studies may anticipate decreased HRVB use in the workplace and assist participants in finding strategies to overcome unwanted attention. Plans may include finding a quiet spot outside, practicing in a car, or closing the office door if practical. The nonemployed participants reported busy personal schedules such as care for family members. Developing a practice schedule at the onset of the study, setting firm practice times, and amending the plans as needed with the participant may be helpful in future studies.
Another common report was difficulty operating the emWave2. Two participants had trouble getting a pulse reading from the PPG sensor, which caused the device to shut off automatically after a few minutes. One participant was not able to operate the emWave2 at all during the last 2 weeks of the study and did not call the given phone number for assistance or attend his weekly clinic visits. Other participants reported discomfort of the PPG sensor, being bothered by the audible beeps from the device, and of not recharging the equipment after use. Although the PI reviewed individual protocol adherence rates at each visit and discussed any barrier to practice, operational difficulties were not minimized. In future studies, the researcher recommends providing participants with links to the HeartMath website and online instructional videos for assistance.
The study resulted in one unexpected occurrence. A participant reported chest wall discomfort when she practiced for more than 10 min. She had a negative cardiac and respiratory examination, and the PI offered reassurance that the pain was muscular. She gradually increased her practice times, and by the end of the study, the discomfort was minimal, with once-daily 20 min of practice. Larger sample sizes may report more occurrences of this phenomenon.
The Veterans with depression practiced more frequently than those with PTSD and anxiety. However, Veterans diagnosed with PTSD practiced for more extended periods than those diagnosed with anxiety or depression. The PI unable to ascertain why this occurred, and was unable to find studies that reported such findings. 43 Sample size (n = 10) limited drawing any inference. Future studies should address a comorbidity of PTSD or anxiety that may be a barrier to treatment.
No studies were found addressing the feasibility or acceptability of Lehrer's HRVB practice protocol. 43 However, the participants' poor adherence is consistent with previous reports that FM patients are skeptical of treatments. 44 One prior study of HRVB for FM-related chronic pain prescribed twice-daily practice 24 ; yet treatment protocol adherence was not reported. Other previous HRVB studies for chronic pain did not adhere to recommendations set by Lehrer et al. 31 ; the studies only provided HRVB training during clinic visits. 23,29,45,46 More studies are warranted to ascertain the feasibility and acceptability of this protocol.
The emWave2 software calculates the HRC scores. A lower score indicates a less coherent HRV, reflecting a dysfunctional ANS, increased pain perception, decreased physical function, and poor QOL. 15,17,47 In our study, the mean HRC scores did not change substantially from week to week, suggesting there was no improvement in HRV postintervention. This finding is inconsistent with earlier studies, where HRC scores increased with HRVB, 23,24,29,45 and a small sample size may have been a contributing factor
A goal of HRVB is to improve QOL and functional status by decreasing FM-related symptoms. Data from the SFMQ and the FIQR suggest no improvement in pain symptoms following HRVB. Despite the persistent pain scores, data from the FIQR indicated an increase in sleep and functional status, and an overall improvement in QOL postintervention. Participants reported the ability to “deal with persistent pain.” Improved QOL indicators support treatment that addresses the dysfunctional ANS present in FM. 14,15 Improved sleep is associated with increased pain tolerance 1,2 and a recommended treatment goal in FM. 1,44 Similar QOL findings were reported in the HRVB study for FM patients by Hassett et al., 24 where results reported a statistically significant (p = 0.0002) improvement in FIQR scores 3 months postintervention. A larger RTC is warranted to confirm QOL and functional status of individuals with FM-related symptoms.
Conclusions
Twice-a-day HRVB practice is not feasible for this group of Veterans. Limitations of this study include small size and the lack of a control group. Future studies should anticipate participant time management challenges and make recommendations that will facilitate a regular practice schedule. Participants may also benefit from immediate access to help with the operational difficulties of the device. In this feasibility study, inferences about changes in pain, functional status, and QOL cannot be concluded. Thus, RCT are needed to evaluate the feasibility and acceptability of this HRVB protocol and to evaluate the effects on HRV, QOL, and functional status postintervention.
Author Contribution Statement
We listed all persons who meet authorship criteria as authors, and all authors certify that they have participated sufficiently in the article to take public responsibility for the content, including participation in the concept, design, analysis, writing, or revision.
Footnotes
Acknowledgments
This material is the result of work supported with resources and the use of facilities at the Ralph H. Johnson VA Medical Center, Charleston, SC. The author could not have completed this study without the support of Dr. Robert S. Friedman. The author would also like to acknowledge the mentorship and contributions of Julie Barroso, PhD, Michelle Nichols, PhD, and Jeffrey Meyer, PhD.
All persons who have made substantial contributions to the work reported in the article (e.g., technical help, writing and editing assistance, general support), but who do not meet the criteria for authorship, are named in the Acknowledgments and have given their written permission to be named.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Steward Doctoral Dissertation Award. Medical University of South Carolina College of Nursing, Dissertation Grant.