
Abstract
Objectives:
Frail patients with chronic obstructive pulmonary disease (COPD) have a higher risk of mortality, mood disorder, and poor quality of life (QOL). There are few intervention studies in frail patients with COPD, and there is a need for an effective therapy. Ninjin'yoeito (NYT) is a Kampo medicine that has been reported to improve fatigue, psychosomatic vulnerability, and respiratory symptoms. We examined the efficacy of NYT in frailty or prefrailty patients with COPD.
Design:
Prospective, single-center, open-label, randomized controlled trial.
Location:
Showa University Hospital, Tokyo, Japan.
Subjects:
Sixty-two patients (53 males and 9 females) with a mean age of 76 ± 6 years were included in the analysis.
Interventions:
The patients were divided into two groups: the NYT group (n = 31) and the control (standard treatment) group (n = 31).
Outcome measures:
The primary outcome was changes in Kihon checklist (KCL) scores at week 24, which reflect changes in frailty. The secondary outcomes were changes in the following assessment scores at week 24: Simplified Nutritional Appetite Questionnaire (SNAQ) scores, which reflect changes in appetite; COPD Assessment Test (CAT) scores, which reflect changes in QOL in patients with COPD; Hospital Anxiety and Depression Scale (HADS)-Anxiety scores, which reflect changes in anxiety; and HADS-Depression scores, which reflect changes in depression.
Results:
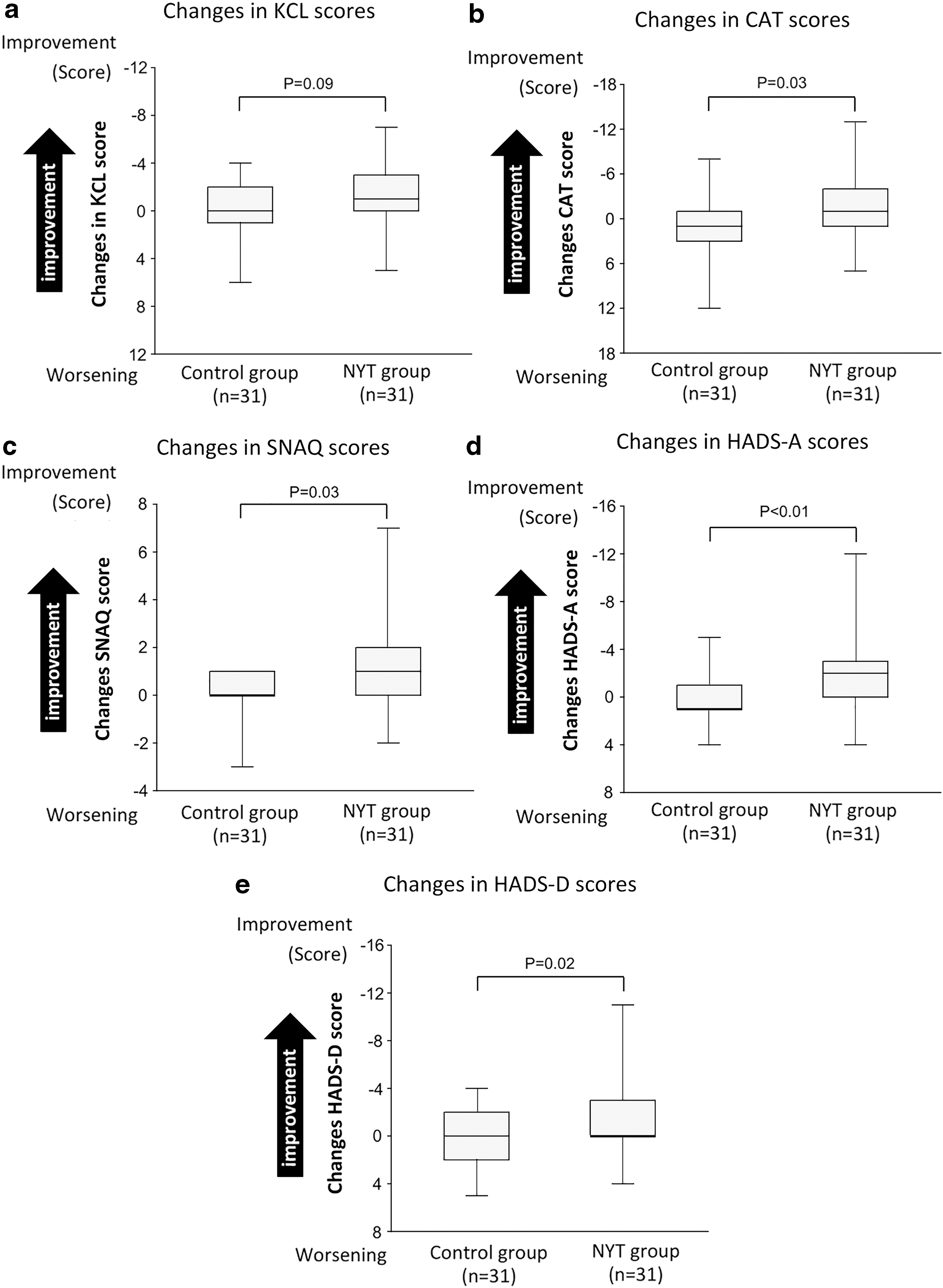
There was a slight but not significant difference in changes in KCL scores between the NYT and control groups (p = 0.09). However, there were statistically significant differences in changes in SNAQ (p = 0.03), CAT (p = 0.03), HADS-Anxiety (p < 0.01), and HADS-Depression (p = 0.02) scores between the two groups.
Conclusions:
Our results suggest that NYT is an effective and promising drug with various effects in patients with COPD who are frail, despite conventional treatment.
Introduction
Frailty is generally defined as a clinical state in which an individual's vulnerability for developing dependencies increases when exposed to a stressor, and is characterized by a reduction of muscle strength, endurance, and physiological function. 1,2 In the future, the number of frail elderly patients is anticipated to increase with the escalation in the number of elderly individuals in many countries. 2
Frailty is clinically investigated in patients with various diseases. In addition to risk factors, such as older age, smoking, endocrine dysfunction, and systemic inflammation, patients with chronic obstructive pulmonary disease (COPD) have a significantly higher prevalence of frailty and an increased risk of death than non-COPD patients. 3,4 We have previously shown that COPD patients with frailty have poor quality of life (QOL) and appetite, in addition to mood disorders and physical vulnerability 5 ; therefore, establishment of an appropriate intervention is required to address these symptoms. Although there are few intervention studies in frail patients with COPD, one study demonstrated that respiratory rehabilitation can improve the frailty status from a frail to either a prefrailty or to a nonfrail status. 6 However, considering that the rate of successful completion of pulmonary rehabilitation is lower in frail patients with COPD than in nonfrail patients with COPD and that not all hospitals can provide rehabilitation services, interventions other than rehabilitation need to be established.
While there are studies of nutritional supplementation therapy in patients with COPD and sarcopenia who have symptoms similar to those of frail patients, 7 to our knowledge, there have been no drug intervention studies or nutritional supplementation studies in frail patients with COPD. In Japan, Kampo medicines have historically been widely used for symptoms of frailty (e.g., fatigue, anorexia). Among these medicines, Ninjin'yoeito (NYT) is a typical Kampo medicine that improves symptoms such as fatigue, anorexia, mood disorders, and cognitive dysfunction. 8 NYT is considered to have a multifaceted clinical effect, as it contains many constituents. Each constituent is reported to show anti-inflammatory, antinociceptive, and antioxidant effects, a positive effect on ghrelin, and a palliative effect on pain. 9 We have experienced the case of a patient with severe COPD and frailty who showed dramatic improvement after receiving NYT. 10 However, there have been no clinical studies of NYT in frail patients with COPD to date. In this study, we, therefore, report the efficacy of NYT in our outpatients with COPD who were in a frail or prefrail state, despite treatment with established approaches.
Materials and Methods
The present study was conducted in accordance with the guidelines of the Helsinki Declaration. Study approval was granted by the Ethics Committee of Showa University School of Medicine (approval number: 2268), and the study was registered in the University Hospital Medical Information Network Clinical Trials Registry (UMIN-CTR) (UMIN-CTR number, 000034582). All patients provided written informed consent.
Materials
NYT is a traditional Japanese medicine derived from 12 herbal medicines (i.e., Rehmanniae Radix, Angelicae Acutilobae Radix, Atractylodis Rhizoma, Poria, Ginseng Radix, Cinnamomi Cortex, Polygalae Radix, Paeoniae Radix, Citri Unshiu Pericarpium, Astragali Radix, Glycyrrhizae Radix, and Schisandrae Fructus). NYT prescription is approved by the Japanese Ministry of Health, and as it is used to treat fatigue, anorexia, night sweats, and anemia, we hypothesized that it may be beneficial for frailty in patients with COPD.
Study sites and patients
Sixty-eight frail or prefrail outpatients with COPD were included in this 24-week prospective, single-center, open-label, randomized controlled trial. It was conducted at the Showa University Hospital, Tokyo, Japan, between October 2017 and December 2018. Patients were randomized into two groups, in a 1:1 ratio: a group that received NYT for 24 weeks and a control group that continued conventional treatment. The NYT group received 7.5 g/day NYT extract as fine granules (Kracie Pharma, Ltd., Tokyo, Japan), which has been approved as a prescription drug in Japan, three times daily, before or between meals.
The patient inclusion criteria were as follows: (1) age ≥65 years; (2) diagnosed with COPD and had started bronchodilator therapy; (3) a smoking history of Brinkman Index ≥200; and (4) presence of a state of frailty or prefrailty. The diagnosis of COPD was made according to the criteria of the Global Initiative for Chronic Obstructive Lung Disease (GOLD). All patients were confirmed to have forced expiratory volume in 1 sec (FEV1) of <70% after bronchodilator inhalation. 11 The diagnosis of frailty and prefrailty was based on the scores of the Kihon checklist (KCL), a medical questionnaire with established validity for the evaluation of frailty. 12
The exclusion criteria were as follows: (1) difficulty to undergo pulmonary function tests adequately; (2) presence of respiratory diseases other than COPD; (3) a history of an acute disease within 3 months of enrollment; (4) a Mini-Mental State Exam score <18; (5) a history of starting NYT therapy within a month before providing informed consent to participate in the current study; (6) presence of an active malignant tumor; (7) a history of having participated in another clinical study within the previous 4 weeks; and (8) deemed ineligible by the attending physicians.
Evaluation and outcomes
Kihon checklist
The KCL was developed by the Japanese Ministry of Health, Labor, and Welfare for the identification of elderly individuals at risk of requiring care/support. The KCL is a concise medical questionnaire consisting of 25 yes/no items; higher scores indicate frailer patients. Previous studies have established the effectiveness of evaluation of frailty based on the KCL score. 13 Based on the results of previous studies, patients with KCL scores of 0–3, 4–7, and 8–25 points were classified as robust, prefrail, and frail patients, respectively. 12
COPD assessment test
The COPD assessment test (CAT) allows simple and easy evaluation of QOL in patients with COPD. The questionnaire consists of eight items. All items are scored from 0 to 5, and the total score ranges from 0 to 40. The higher the score, the lower the health status of the patient. The CAT is a very important questionnaire in COPD treatment, and the GOLD guidelines recommend treatment according to the total CAT score. 14
Simplified Nutritional Appetite Questionnaire
The Simplified Nutritional Appetite Questionnaire (SNAQ) provides appetite scores predicting future weight loss. The questionnaire consists of four items. All items are scored from 1 to 5, and the total score ranges from 4 to 20. The lower the score, the lower the patient's appetite. 15
Hospital Anxiety and Depression Scale
The Hospital Anxiety and Depression Scale (HADS) is an effective model for the evaluation of anxiety and depression. 16 The HADS consists of a total of 14 items: 7 items on anxiety and another 7 items on depression. All items are scored from 0 to 3, and the total scores of the HADS-anxiety (HADS-A) and HADS-depression (HADS-D) range from 0 to 21, respectively. Scores of 0–7 points indicate a normal condition, 8–10 points indicate possible anxiety and/or depression, and 11–21 points indicate clear anxiety and/or depression.
As the primary endpoint, we evaluated the effects of NYT on frailty score by comparing changes in KCL scores from baseline to week 24 between the NYT and control groups. The secondary endpoints were changes in the CAT, HADS-A, HADS-D, and SNAQ scores from baseline to week 24 for the NYT and control groups. All patients underwent an examination of side effects at each visit, mainly confirmed by subjective symptoms and physical examination.
Sample size calculation
A power calculation estimated that a sample size of 75 patients in the Intervention group and 75 patients in the Control group to detect a two-point improvement of KCL scores. However, we recalculated the sample size, considering that it was difficult to achieve the target number of cases and KCL was expected to improve by three points in the Intervention group. A power calculation estimated that a sample size of 34 patients in the Intervention group and 34 patients in the Control group would have 80% power at α (significance) level 0.05 to detect a three-point improvement of KCL scores.
Statistical analyses
For baseline data, continuous variables with a normal distribution are shown as mean ± standard deviation, while the other variables are shown as median and the interquartile range. The Shapiro–Wilk test was used to assess the normality of data distribution for all variables. Categorical data are presented as percentages. Student's t test was used to compare the baseline data with a normal distribution between the NYT and control groups, while the Wilcoxon rank-sum test was used to compare data with a non-normal distribution between the two groups. The chi-square test was used to assess differences in the sex ratio. Changes in each item from baseline to week 24 are shown as median values. The Wilcoxon signed-rank test was used to assess differences in changes for each item between the two groups. A p-value <0.05 was considered to indicate statistical significance. All statistical analyses were performed using JMP Pro for Macintosh, version 14 (SAS Institute, Cary, NC). All authors had full access to all the data in the study and contributed to the final decision to submit the article for publication.
Results
Baseline patient characteristics
Sixty-eight frail or prefrail outpatients with COPD were included in this study. Patients were divided into the NYT (n = 33) and control (standard treatment, n = 35) groups, but three patients in the control group withdrew before starting treatment. After group allocation, in the NYT group, one patient developed lung cancer and another patient voluntarily discontinued outpatient visits, while one patient in the control group voluntarily discontinued outpatient visits. Thus, 62 patients were finally included in the analysis (Fig. 1). Although four patients in the NYT group had diarrhea requiring dose reduction (from 7.5 to 2.5 g), no serious side effects were observed in the NYT group during the course of the study.
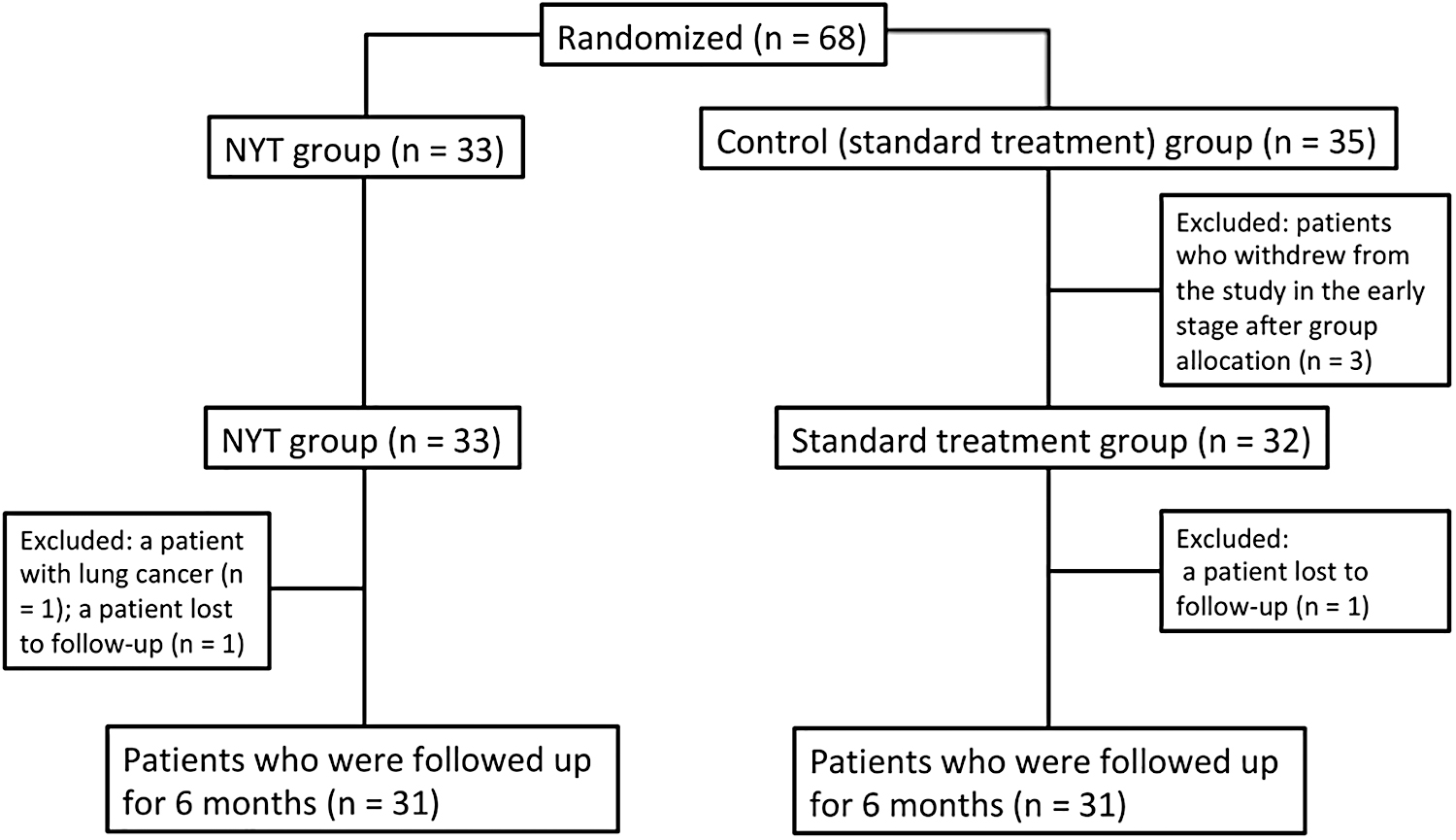
Flow-chart of patient selection. NYT, Ninjin'yoeito.
Clinical findings for the patients at baseline are shown in Table 1. The mean age of all patients was 76.4 years. Males accounted for 85.5% of all patients. The mean overall FEV1 was 58.3%. The median KCL score of 9.5 indicated the status of frailty. The median CAT score of 17.5 indicated a low QOL in patients. The median HADS-Anxiety score and the mean HADS-Depression score were both close to the cutoff of 8, indicating mood disorders. The median SNAQ score of 14 also indicated a low appetite. The results showed that the patients in this study were frail elderly patients with COPD, a low QOL, low appetite, and mental health disturbances. While at baseline, there was a significant difference in BMI (p = 0.03), there were no significant differences in the other items between the NYT and control groups.
Baseline Characteristics of Patients
Continuous variables with a normal distribution are shown as mean ± standard deviation, while the other variables are shown as median and the interquartile range or n (%). Student's t test was used to compare the baseline data with a normal distribution between the NYT and control groups, while the Wilcoxon rank-sum test was used to compare data with a non-normal distribution between the two groups. The chi-square test was used to assess differences in the sex ratio.
BMI, body mass index; CAT, chronic obstructive pulmonary disease assessment test; FEV1, forced expiratory volume in 1 second; HADS, Hospital Anxiety and Depression Scale; KCL, Kihon Checklist; NYT, Ninjin'yoeito; SNAQ, Simplified Nutritional Appetite Questionnaire.
Primary outcome
Table 2 and Figure 2a show changes in KCL scores for the NYT and control groups, respectively. While the NYT group showed an improvement in KCL scores at week 24 (amount of change: −1; range −3 to 0), the control group showed no improvement in KCL scores (amount of change: 0; range −2 to 1). The difference in changes between the two groups did not show statistical significance but showed a trend for improvement in the KCL with NYT (p = 0.09).
Changes in scores in the NYT and control groups after 24 weeks of treatment.
Changes in Clinical Factors After 24 Weeks
The Wilcoxon signed-rank test was used to assess differences in changes for each item between the two groups.
CAT, chronic obstructive pulmonary disease assessment test; HADS, Hospital Anxiety and Depression Scale; KCL, Kihon checklist; SNAQ, Simplified Nutritional Appetite Questionnaire.
Secondary outcomes
Table 2 and Figure 2b–e show the secondary outcomes of this study. While the NYT group showed an improvement in CAT scores (amount of change: −1; range −4 to 1), the control group did not (amount of change: 1; range −1 to 3). There was a significant difference in changes in CAT scores between the two groups (p = 0.03). The difference in changes in CAT scores between the NYT and control groups was 2, which is the minimal clinically important difference (MCID) of CAT scores. 17
While the NYT group showed an improvement in SNAQ scores (amount of change: 1; range 0–2), the control group did not (amount of change: 0; range 0–1). There was a significant difference in changes in SNAQ scores between the two groups (p = 0.03).
The NYT group showed an improvement after administration of medication in HADS-Anxiety scores (amount of change: −2; range −3 to 0), but the control group did not (amount of change: 1; range −1 to 1). There was a significant difference in changes in the HADS-Anxiety scores between the two groups (p < 0.01). The difference in changes in the HADS-anxiety scores between the NYT and control groups was greater than 1.5, which is the MCID of HADS-anxiety scores. 18 Both the NYT and the control groups did not show any improvement in the HADS-Depression scores after the administration of medication (amount of change: 0; range −3 to 0) (amount of change: 0; range −2 to 2). However, there was a statistically significant difference in changes in HADS-Depression scores between the two groups (p = 0.02), but did not reach the MCID.
Adverse events
Four patients in the NYT group had mild diarrhea, probably due to NYT, and required dose reduction. Another patient in the NYT group developed lung cancer, which may not have been related to NYT.
Discussion
There is a need for approaches that can improve frailty in patients with COPD. This trial evaluated the effect of NYT on frailty in elderly patients with COPD. We found that the KCL score (an indicator of frailty) improved in the NYT group after week 24 of NYT administration. However, the difference in changes in KCL scores between the two groups did not reach statistical significance. Second, the NYT group showed an improvement in QOL (CAT), appetite (SNAQ), and anxiety and depression (HADS-Anxiety and HADS-Depression) scores, and there were significant differences in the changes in these scores at week 24 between the NYT and control groups.
Although there was an improvement in KCL scores with NYT treatment, the difference between the NYT and control groups showed only a trend for significance (p = 0.09). Since only frail elderly patients with COPD were included in this study, the reason for the nonsignificant results may be the small sample size, leading to insufficient statistical power.
The NYT group showed significantly more improvements in many clinical endpoints than the control group. The CAT is a very important indicator as it allows a comprehensive evaluation of QOL in patients with COPD and is used for the selection of drug therapy in actual clinical settings. The results of this study are noteworthy in that there have been no other reports of drugs that improved the CAT scores of frail patients with COPD receiving bronchodilator treatment.
While mood disorders are important clinical factors that affect the prognosis of patients with COPD, 19 there are very few reports of drugs that have improved mood disorders in patients with COPD. 20 Therefore, the finding in this study that the NYT group showed a significant improvement in mood disorder, as compared with the control group, has high clinical significance.
Additionally, there is a strong relationship between appetite and COPD. It has been reported that patients with COPD have low appetite due to psychosomatic factors and systemic inflammation. 21 Although low weight is a poor prognostic indicator in patients with COPD, 22 there are no studies of pharmacotherapy for anorexia in patients with COPD. Therefore, anorexia in patients with COPD is a very important clinical problem, and the result of this study showing that NYT can be expected to improve appetite is clinically relevant.
NYT is a traditional Kampo medicine that has been approved as a prescription drug in Japan. The drug is used to improve fatigue and mood disorders in frail elderly individuals. NYT also improved appetite, QOL, and mental health in frail patients with COPD in this study. The efficacy of NYT on the various disorders may be because the drug is a Kampo medicine derived from 12 herbal medicines. A study of pharmacotherapy for anorexia showed an improvement of dietary intake with ghrelin in patients with COPD. 23 Previous studies reported that citrus unshiu peel in NYT promotes the secretion of ghrelin 24 and improves appetite in frail patients with Alzheimer's disease, 25 supporting the results of this study. One of the reasons that the NYT group showed an improvement in QOL (CAT scores) may be that ginseng and schisandra fruit in NYT improve fatigue. 26 In fact, previous studies demonstrated that NYT reduces chemotherapy-related fatigue in patients with multiple myeloma. 27,28 In addition, schisandra fruit has been reported to improve sputum and respiratory inflammation. 29 These results suggest the synergistic effect of these herbal medicines on patient QOL. An active constituent of roots of Polygala tenuifolia (Onji), 30 citrus unshiu peel, 31 and atractylodes rhizome 32 have been reported to have antidepressant and antianxiety effects. In addition, NYT has been reported to improve mood disorders in patients with Alzheimer's disease. 33 These ingredients may improve mood and anxiety disorders, including depression in frail patients with COPD.
Limitations
This study had some limitations. First, this open-label, randomized, controlled trial did not use a placebo. Therefore, patients in the NYT group may have anticipated some effect when they were assigned to the NYT group. Hence, caution should be exercised while interpreting the improvement in subjective symptoms, especially as the principal evaluation in this study was based on an interview. Therefore, the results of this study may not be completely accurate. In addition, frailty should have been evaluated using Fried's criteria 34 or a similar model with high objectivity alongside the KCL.
Second, the reason for the nonsignificant results of changes in KCL scores as the primary outcome may be because of the small sample. Because we were unable to recruit the number of patients we initially expected, multicenter studies will be needed to further increase the number of patients in the future. Third, this clinical study in frail or prefrail patients with COPD, including those without a history of low weight or weight loss, did not examine the effect of NYT on weight loss. Therefore, future studies should further investigate the effects on NYT on frail patients with COPD by using a placebo control and a larger sample size of patients, and should consider the effectiveness of low weight or weight loss.
Conclusions
The results of this study demonstrate that NYT improves appetite, QOL, and mood disorders in frail, elderly patients with COPD. This is the first report to demonstrate the clinical utility of NYT in frail patients.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported, in part, by the Japan Society for the Promotion of Science KAKENHI (grant number: 18K10654 to T.H.) and the Environment Research and Technology Development Fund (year 2019–2021) of the Environmental Restoration and Conservation Agency of Japan. This research was conducted with financial support from Kracie Pharma Ltd., Tokyo, Japan.