
Abstract
Objectives:
To investigate whether chiropractic care influences strength, balance, and/or endurance in active-duty United States military personnel with low back pain (LBP).
Design:
This study employed a prospective randomized controlled trial using a pragmatic treatment approach. Participants were randomly allocated to 4 weeks of chiropractic care or to a wait-list control.
Interventions:
Chiropractic care consisted of spinal manipulation, education, advice, and reassurance.
Settings/Location:
Naval Air Technical Training Center branch clinic at the Naval Hospital Pensacola Florida.
Subjects:
One hundred ten active-duty military personnel 18–40 years of age with self-reported LBP.
Outcome measures:
Isometric pulling strength from a semisquat position was the primary outcome. Secondary outcomes were single-leg balance with eyes open and eyes closed, and trunk muscle endurance using the Biering–Sorensen test. Patient-reported outcomes such as pain severity and disability were also measured. Outcomes were measured at baseline and 4 weeks. Linear mixed-effects regression models over baseline and 4 weeks were used for analysis.
Results:
Participants had mean age of 30 years (18–40), 17% were female, 33% were non-white, and 86% reported chronic LBP. Mean maximum pulling strength in the chiropractic group increased by 5.08 kgs and decreased by 7.43 kgs in the wait-list group, with a statistically significant difference in mean change between groups (p = 0.003). Statistically significant differences in mean change between groups were also observed in trunk muscle endurance (13.9 sec, p = 0.002) and balance with eyes closed (0.47 sec, p = 0.01), but not in balance with eyes open (1.19 sec, p = 0.43). Differences in mean change between groups were statistically significant in favor of chiropractic for LBP-related disability, pain intensity and interference, and fear-avoidance behavior.
Conclusions:
Active-duty military personnel receiving chiropractic care exhibited improved strength and endurance, as well as reduced LBP intensity and disability, compared with a wait-list control.
Introduction
Low back pain (LBP) is a prevalent problem, which commonly causes significant disability. 1,2 Between 1996 and 2016, health care spending for LBP and neck pain consistently ranked among the top 5 conditions in the United States. 3 Between 2001 and 2016, LBP was the most prevalent musculoskeletal pain-related diagnosis among active-duty U.S. military personnel. 4 Because back pain represents a large proportion of morbidity burden, it is a high-priority focus for prevention, treatment, and rehabilitation research in the military. 5
Trunk muscle strength, balance, and endurance, can be associated with LBP, potentially affecting mission readiness among military personnel. 6 –9 Low levels of trunk muscle strength may increase risk for, or be caused by, LBP through altered activity and/or movements to avoid potential pain. 10 –12 LBP also appears to negatively affect the ability to sustain prolonged or repeated positions or movements (endurance) and alter neuromuscular system factors influencing balance. 13,14
Spinal manipulation (SM), a nonpharmacological therapy commonly employed by doctors of chiropractic, is a guideline-recommended treatment for LBP. 15,16 Chiropractic services are available to active-duty personnel in the United States through health clinics on military bases. 17 Biological mechanisms underlying SM are complex. SM may facilitate trunk muscle strength through motor neuron facilitation or disinhibition. 18,19 SM may also alter sensory signaling, influencing changes in motor neuron output and reducing sensitivity to pain. 20 –24 A few studies report that SM positively influences immediate isometric muscle strength in healthy individuals; however, both the quantity and quality of available research is currently limited. 25 Additional study is necessary to understand whether SM influences strength in clinically meaningful ways and over longer periods for people with neuromusculoskeletal problems, specifically those suffering from LBP.
This randomized controlled trial (RCT) was conducted to understand whether chiropractic care, primarily consisting of SM, influences strength, balance, and/or endurance, independent of the impact on pain severity and disability, in active-duty U.S. military personnel with LBP. Because trunk muscle strength is a fundamental element required for performing balance and endurance activities, 26,27 the primary aim of this clinical trial was to compare the effects of chiropractic care over 4 weeks, consisting of SM and nonspecific effects, versus a wait-list control on trunk muscle strength. Secondary aims estimated the effects of chiropractic care versus a wait-list control on balance and trunk muscle endurance.
Materials and Methods
A detailed trial protocol was previously published. 28 This prospective RCT using a pragmatic treatment approach was conducted at the Naval Air Technical Training Center branch clinic at the Naval Hospital Pensacola, Florida. The RCT was approved by civilian and military Institutional Review Boards at Palmer College of Chiropractic (2015G171), the RAND Corporation (2013-0159), and Naval Medical Center Portsmouth, VA (NHPC.2015.0003). The trial was also overseen by an independent data and safety-monitoring committee. All participants provided verbal and written informed consent. There was no compensation for participating in the trial.
Eligibility, allocation, and blinding
Active-duty military personnel 18–40 years of age with self-reported LBP with severity of ≥2/10 over the prior 24 h were eligible. Final eligibility was determined at the end of the baseline visit, when the project manager, who led the informed consent process, and the trial clinician, who independently performed the baseline exam, jointly verified inclusion/exclusion criteria through a structured consensus process. 29 Participants were ineligible if they reported receiving chiropractic care within 30 days of consent, were pregnant or seeking to become pregnant, were aware of an impending transfer or other absence during the trial timeframe, were in a process of disability evaluation, were unable or unwilling to follow trial protocols, and if the patellar height was <38.1 cm (15 inches) or >64.8 cm (25.5 inches).
Participants were also excluded if one or more of the following were identified by the doctor of chiropractic during the initial examination: LBP from a confirmed or suspected visceral source; conditions contraindicating SM, spinal fracture, or spinal surgery within 6 months; confirmed stenosis (neuroforaminal or spinal canal) or neurogenic claudication; diagnoses of chronic pain syndrome; inflammatory spinal arthropathy; need for referral for an urgent or emergent condition; and unsafe to perform physical performance tests.
Within 30 days of the initial visit, participants attended a second visit in which baseline strength, balance, and endurance data and patient-reported outcomes were collected. After completion, participants were allocated to chiropractic care or to the wait-list control group in equal proportions. The allocation process used a computer-generated and concealed restricted randomization scheme with random block sizes. The chiropractors, participants, and the site project manager were not blinded to treatment assignment after allocation. Approximately 4 weeks after allocation both groups attended a final visit during which follow-up strength, balance, and endurance, and patient-reported outcomes were again collected.
Wait-list control
After group allocation, wait-list group participants were asked to attend a follow-up visit after 4 weeks. Wait-list group participants were free to seek any health care, except chiropractic or SM from any provider during the trial timeframe; they were offered the option to receive chiropractic care after the final visit.
Chiropractic care
Participants allocated to chiropractic care attended visits over 4 weeks. The number of visits varied depending on factors such as the working diagnosis, condition severity, and scheduling availability. During the 4-week treatment phase, participants were asked to refrain from receiving SM or other chiropractic care in addition to what was provided by the trial chiropractor. No other health care was restricted.
Chiropractic care included clinical evaluation, SM, education, and self-management advice about daily activities that benefit and/or negatively impact symptoms. Keeping with the pragmatic nature of this trial, condition-specific education, which can include reassurance that symptoms are benign and addressable, and self-management advice were not standardized by trial protocol. Rather, these clinical elements reflect evidence-based chiropractic care practiced at the trial site. SM consisted of high-velocity thrust-type manipulation directed toward the thoracolumbar or pelvic regions. SM involving other spinal regions or extremities was also allowed when clinically indicated. During the trial, care was provided by two different chiropractors, each with more than 20 years of experience.
Strength, balance, and endurance
All tests were conducted by the project manager. Isometric pulling strength from a semisquat position was the primary outcome; balance and endurance were secondary outcomes. The isometric strength test required maintaining a semisquat position while pulling on a bimanual handle. 30 The handle was attached to a chain containing a force transducer and connected to the floor through a height-adjustable support. Handle height was determined by patellar height (Fig. 1). The strength test was always performed second.
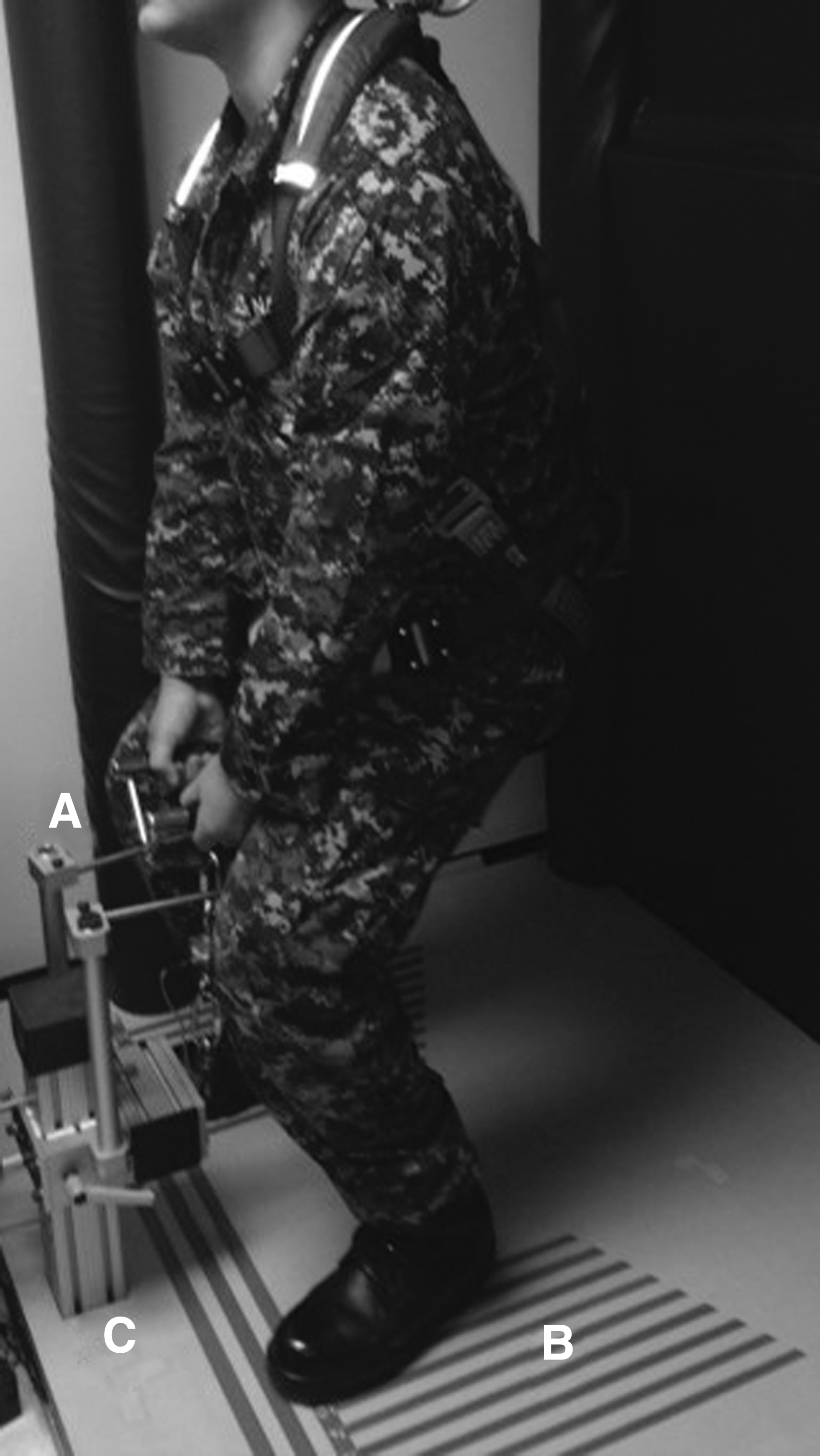
Strength test: Isometric pulling on a bimanual handle
Participants assumed a lifting position, spreading the feet comfortably, bending the knees, with a straightened back, arms angled perpendicular to the floor, and with the eyes looking straight ahead. The first test occurred with instructions to pull for less than 5 sec with a light force. Participants were instructed to stop pulling if they noted increased discomfort. If the light pull occurred without any discomfort, participants were instructed to conduct a second pull (no more than 5 sec) with a medium force. If medium force pulling occurred without an increase in discomfort, the maximum effort test was conducted.
During maximum effort tests participants gradually increased pull effort until a maximum was reached. Maximum effort pulling did not exceed 5 sec. Upon successful completion, the test was conducted two more times separated by a minimum 2-min rest period. The maximum pulling force recorded during any test was used in data analysis. Stance width used at baseline was recorded and repeated at the follow-up assessment.
The balance test was performed first to minimize potential remaining effects from either the strength and/or endurance tests. First, the dominant foot (kicking foot) was determined. Next, participants placed both hands on the iliac crests and stood on the nondominant foot; the dominant foot was placed against the supporting leg below the knee. The test initiated when the heel of the supporting foot was raised from the floor. 31 A sensor pad on the floor surrounding the participants feet activated a computer timer, which was automatically stopped when the heel touched the pad or when the dominant foot touched the floor. After a practice test, the test was performed with the eyes open (three times) and with eyes closed (three times). The longest holding times with eyes open and eyes closed were used for data analysis (Fig. 2).

Balance test: Performed with eyes open and eyes closed. Pressure-sensitive pads
The Biering–Sorensen test was always the third test. It was used to measure trunk muscle endurance. 32,33 The test was always performed last because it is designed to fatigue trunk and lower extremity musculature. Therefore, by performing last, muscle fatigue would not adversely influence the strength and balance tests. Participants assumed a prone position on a therapy table. The head, shoulders, and trunk extended off the edge of the table while supported by the arms (Fig. 3). The lower extremities were held firmly with adjustable straps at the upper thigh and lower legs. The test began when the arms lifted from the support and a neutral trunk position held. The test ended when participants were unable to maintain a neutral position for any length of time due to fatigue or when pain/discomfort occurred. If no pain/discomfort or fatigue ended the test, then the test was ended after 180 sec. Holding time was recorded with a stopwatch.

Endurance (Biering–Sorensen) test: Timing began when arms were lifted from support stool. Timing ended if pain or discomfort was experienced, if a neutral position could no longer be maintained, or when 180 sec was reached.
Safety precautions were necessary to protect participants from injury. During the strength and balance tests, participants wore a harness to prevent accidental falls. The strength test consisted of maximum contraction of muscles in the upper extremity, trunk, and lower extremity, which produced high spinal and other joint loading. The strength test was stopped if participants experienced increased discomfort during the test. If increased discomfort did not resolve within a few minutes, no further strength tests were performed, even if the maximum effort test was not reached. If for any test a participant was unable to attain the initial position without discomfort, the test was not conducted. The balance test was not repeated if participants could not comfortably assume the correct position/stance or if the test caused increased discomfort. Discomfort from muscle fatigue during the endurance test was expected and did not stop testing. However, if participants were unable to attain the test position without pain, the test was not performed.
Patient-reported outcomes
Patient-reported outcomes included average pain over the past 24 h reported on a 0–10 numerical rating scale (0 = no pain, 10 = worst imaginable), 34 the Roland Morris Disability Questionnaire, 35,36 PROMIS-29, 37 Fear-Avoidance Beliefs Questionnaire, 38 and expectation of benefit from chiropractic care (collected only at baseline). Patient-reported outcomes were collected through electronic data capture before group allocation at the second baseline visit and at the final visit.
Sample size
Sample size was estimated and based on our primary outcome variable, maximum strength using a standard deviation (SD) of 21.77 kg, obtained from pilot study data, and the assumption that this variable would be unchanged in the wait-list group. A sample size of 82 participants allocated in a 1:1 ratio to groups provided 90% power to detect at least a 20% difference in mean change between groups at a 0.05 significance level. The sample size was increased to 110 (55 per group) to account for potential loss to follow-up and other missing data.
Statistical analyses
We used an intention-to-treat approach that analyzes data based on original group assignment. We performed data analyses using all observed data in SAS (release 9.4, Cary, NC). We analyzed all outcomes with linear mixed-effects regression models over baseline and week 4 with terms for time, group, and group × time interaction using an unstructured covariance. Normality assumptions were evaluated through residual plots and variables were transformed accordingly. Within-group mean change from baseline and the difference in mean change between groups were estimated from the regression model and reported with 95% confidence intervals.
Results
Two hundred two patients were screened for the trial between April 6, 2016 and November 20, 2018 with 110 allocated to receive either chiropractic care (55) or be placed on the wait-list (55) (Fig. 4). Data collection ended on December 19, 2018. Mean participant age was 30 years (18–40), 19 (17%) were female, 36 (33%) were non-white, and 95 (86%) reported chronic LBP (>3 months duration), with 66% reporting LBP duration of over 1 year (Table 1). Two participants in the chiropractic care group attended no chiropractic visits. Of the 53 participants with at least 1 chiropractic visit, the mean (SD) number was 5.3 (1.7) and all received SM. No wait-list group participants reported receiving chiropractic care during the trial period. Two chiropractic care group participants reported receiving stretches and exercises from a physical therapist. One additional participant reported receiving physical therapy and acupuncture. Four wait-list group participants received outside care (one massage therapy, and three received prescriptions for non-steroidal anti-inflammatory medications [NSAIDs] and muscle relaxants).
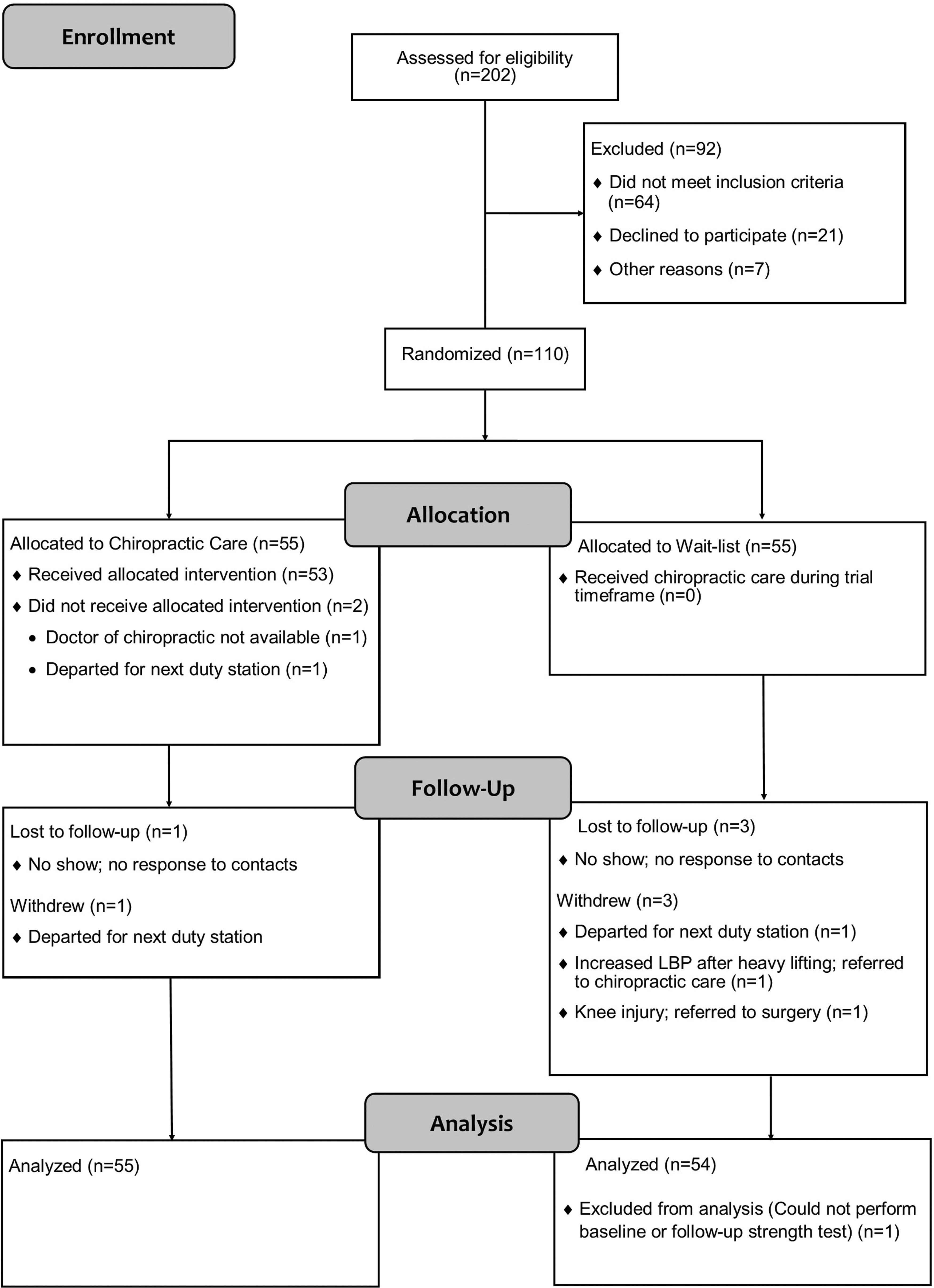
Study flow diagram.
Baseline Characteristics
LBP, low back pain; SD, standard deviation.
Mean maximum isometric pulling strength in the chiropractic care group increased by 5.08 kgs, whereas it decreased by 7.43 kgs in the wait-list group, with a statistically significant difference in mean change between groups (p = 0.003; Table 2). We also found statistically significant differences in mean change between groups for endurance and balance with eyes closed, but the magnitude of the latter was very small. Data for balance with eyes open were skewed, so it was log transformed for analysis and the results were transformed back to the original scale for reporting. Difference in mean change between groups was not statistically significant for balance with eyes open. Differences in mean change between groups were statistically significant, favoring chiropractic care, for the Roland Morris Disability scale, average pain intensity over the past 24 h, physical fear-avoidance behavior, and pain interference (Table 3).
Changes in Strength, Balance, and Endurance
Estimated from mixed-effects models using all observed data, an unstructured covariance, and terms in the model for time (two times: baseline and follow-up), group and group by time interaction.
Analyzed on the natural log scale, with results transformed back to the original scale.
CI, confidence interval; SD, standard deviation.
Patient-Reported Outcomes
Estimated from mixed-effects models using all observed data, an unstructured covariance, and terms in the model for time (2 times: baseline and follow-up), group and group by time interaction. PROMIS T-scores (0–100) are normed to a mean of 50 and SD of 10 for the U.S. general population based on 2000 census data.
Higher scores indicate worse functioning or symptoms.
CI, confidence interval; LBP, low back pain; PROMIS, Patient-Reported Outcomes Measurement Information System; SD, standard deviation.
Safety and adverse events
Safety protocols prevented the performance of four strength, six balance, and four endurance tests during the trial. Tests not performed by group are displayed in Table 4. There were 22 adverse events related to trial participation. All events were described as short-term and self-resolving symptom aggravation, stiffness, and muscle soreness. Four mild events were related to the eligibility exam (2) and treatment (2). Six mild and one moderate-severity (oblique muscle strain) events were attributed to the strength test. Four mild events were attributed to the endurance test, one to the balance test, and six to a combination of strength, endurance, and/or balance tests.
Number of Tests Not Performed Due to Safety Precautions
Discussion
Mean improvement in patient-reported LBP severity and disability in the chiropractic care group were consistent with the moderate short-term improvements reported in a large clinical trial assessing chiropractic care plus usual medical care in a similar population with a similar number of chiropractic visits. 39 We found improvements in isometric pulling strength, balance with eyes closed, and endurance that were statistically significantly greater in the chiropractic care group than the wait-list group.
Several clinical studies report increased lower and upper extremity muscle strength immediately following SM at a single timepoint. 18,19,25,40,41 These studies, mostly conducted with asymptomatic persons, suggest that SM-related muscle strength change involves complex neurological phenomena such as corticospinal excitability. One study involving asymptomatic participants reported a sustained increase in bite force 1 week after a single SM. 42 To our knowledge, our trial is the first to evaluate and report isometric strength, endurance, and balance changes following a course of care, including SM for symptomatic persons.
Participants with LBP receiving 4 weeks of chiropractic care in our trial showed statistically significant improvements in mean pulling strength of 5 kg (11.2 lbs) compared with wait-list control group participants who decreased by a mean of 7.4 kg (16.4 lbs). The mean isometric muscle endurance measured with the Biering–Sorensen test improved by 3.3 sec in the chiropractic care group compared with the 10.6 sec decrease in the wait-list group. These results are consistent with a study that reported an increase in mean holding time for 162 participants with LBP after a 120-h in-patient treatment program incorporating exercise, ergonomic training, psychological skill-building, back protection techniques, and exercise. 32 In that study, as in ours, the mean holding time in the control group also reduced (worsened).
Trunk muscle endurance improvement is associated with single-leg standing improvement in older adults. 43 Similarly, a relationship between the balance test used in our trial and performance of the Biering–Sorensen (endurance) test has been reported. 44 In this trial, improvement in mean single-leg balance time with eyes closed was very small, although consistent with changes in trunk muscle endurance in favor of the chiropractic care group. However, mean balance time with eyes open did not significantly improve over the control group. Therefore, we interpret this result as unlikely to be clinically meaningful.
Results from this trial may help inform our understanding of physiological mechanisms related to interventions applied through chiropractic care. In addition to complex neurological processes associated with SM that influence muscle function, mechanical forces of manual therapies may disrupt muscle spasm/hypertonicity and fibrosis between and within myofascial tissues in persons with chronic LBP, improving the potential for normalized local joint and tissue motion. 21,45 –47 Pain-inhibiting effects from SM may lead to greater mobility and more normalized trunk muscle motor firing patterns because of a reduced need to avoid painful positions or movements. 21,48,49 Nonspecific effects of provider interactions, including patient education, reassurance, and advice may also influence symptom perception, contributing to improved physical performance. 50 Thus, our results most likely suggest SM plus less-specific effects from education, mobility changes, and advice acted as catalysts. Altogether, these factors likely initiated neurological, physical, and/or cognitive changes culminating in a net normalizing of functional ability, which was otherwise limited by LBP and related adaptive processes.
Trial limitations
Limitations in this trial included lack of clinician, participant, and project manager blinding, the use of a wait-list control group, and missing data due to safety concerns in testing. As is the case in all studies of manual therapies, neither the clinicians nor the participants were blinded to group assignment. To minimize this limitation, the project manager used scripts and checklists to ensure actions and instructions were consistent during strength, balance, and endurance testing. A wait-list control was a practical design strategy because (1) the outcomes of strength, balance, and endurance were measured objectively, (2) there is no inert sham chiropractic treatment available, and (3) chiropractic care is an integrated treatment option at the trial site. A few participants were unable to complete all tests due to safety concerns, resulting in some missing data. However, our statistical analysis used available data for all participants. Finally, the magnitude of differences in change for strength and endurance are likely to be clinically meaningful, but there are limited data to further guide these interpretations.
Conclusions
Four weeks of chiropractic care resulted in improvements in mean strength, balance with eyes closed, and endurance, but not balance with eyes open when compared with a wait-list control group. Chiropractic care also resulted in moderate short-term improvements in LBP intensity and disability and facilitated a return toward normal functional capacity in active-duty military personnel whose physical performance was likely compromised by LBP.
Footnotes
Author Contributions
C.G. oversaw trial design and implementation. M.R.G. and T.X. designed the biomechanical assessments. A.M. and R.V. oversaw training, safety, and other implementation logistics. C.L. performed the statistical analyses and oversaw data collection. R.V. led article development. I.C. and J.W. participated in obtaining funding, oversaw regulatory submissions, and provided other guidance. All authors reviewed and approved the article before submission.
Acknowledgments
The views expressed are those of the authors and may not reflect the official policy or position of the U.S. Army, U.S. Department of Defense, or U.S. government. Trial Registration: this trial was registered with ClinicalTrials.gov, ID number: NCT02670148.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by grant W81XWH-11-2-0107 to the RAND Corporation from the Chiropractic Research Program of the Congressionally Directed Medical Research Programs, U.S. Army, U.S. Department of Defense.