
Abstract
Objectives:
Veterans often suffer from multiple chronic illnesses, including mental health disorders, diabetes, obesity, and cardiovascular disease. The improvement of engagement in their own health care is critical for enhanced well-being and overall health. Peer-led group programs may be an important tool to provide support and skill development. We conducted a pilot study to explore the impact of a peer-led group-based program that teaches Veterans to become empowered to engage in their own health and well-being through mindful awareness practices, self-care strategies, and setting life goals.
Design:
Surveys were collected before and immediately after participation in the Taking Charge of My Life and Health (TCMLH) peer-led group program.
Settings/location:
Sessions were held in non-clinical settings within a VA medical center in the Midwest.
Subjects:
Our sample comprised 48 Veteran participants who were enrolled in TCMLH and completed a pretest and post-test survey.
Intervention:
TCMLH is a 9-week peer-led group program with an established curriculum that leverages the power of peer support to improve patient engagement, empowerment, health, and well-being among Veterans through Whole Health concepts, tools, and strategies. Programs were led by 1 of 12 trained Veteran peer facilitators.
Outcome measures:
Program impact on Veteran well-being was assessed by pre-post measures, including the Patient Activation Measure (PAM), the Perceived Stress Scale (PSS), the Patient-Reported Outcomes Measurement Information System Scale (PROMIS-10), the Perceived Health Competency Scale (PHCS), and the Life Engagement Test (LET).
Results:
There was a significant decrease in perceived stress (PSS score). Significant improvements were also seen in mental health and quality of life (PROMIS-10), participant accordance with the statement “I have a lot of reasons for living” (LET), and patient engagement (PAM score).
Conclusions:
As the Whole Health movement expands—both in VA and elsewhere—our findings suggest that guiding patients in an exploration of their personal values and life goals can help in key areas of patient engagement and mental and physical health outcomes. Further study is warranted, and expansion of the TCMLH program will allow for a more rigorous evaluation with a larger sample size.
Introduction
The Veterans Health Administration (VHA) has made significant inroads in transforming its health care system from disease-oriented to personalized, proactive, and person driven, with the goal of helping Veterans achieve their highest possible health and well-being. 1 –4 Implementation of such patient-centered practices can increase patient satisfaction and health outcomes, 5 and it can decrease health care utilization. 6 As the largest integrated health care system in the nation—serving 9 million Veterans—the VHA is working toward a cultural transformation that can impact the lives of Veterans and their families and set a precedent for health care systems.
The VHA established the Office of Patient Centered Care and Cultural Transformation (OPCC&CT) in 2011 to help cultivate and sustain a culture of health that prioritizes the individual values, needs, and goals of Veterans. A key priority of OPCC&CT was to design a framework within which health professionals could involve Veterans to develop personalized strategies that enhance their physical and mental health and well-being. The Whole Health initiative, created in this spirit, focuses on the Veteran as a whole person (rather than a patient with a disease), the relationships between Veterans and their community (including their providers), the role of self-care strategies that empower Veterans to engage their innate healing capacities, and the importance of conventional and complementary integrative health (CIH) practices as mechanisms for health and healing. 1,2
To conceptualize system-wide change, OPCC&CT declared three key aspects of the Whole Health System (Fig. 1) for Veterans: (1) the pathway (empowering); (2) well-being programs (equipping); and (3) Whole Health clinical care (treating). Through the pathway, the VA partners with Veterans to help them (1) determine what matters most to them by exploring their life Mission, Aspiration, or Purpose (MAP) and (2) develop a personalized health plan. 7,8 Well-being programs equip Veterans with the knowledge, self-care strategies, skills, and conventional and CIH approaches they need to optimize their health and well-being. Finally, clinical care is provided by health professionals trained in Whole Health. 9,10 The Whole Health System not only embraces the need to empower and engage Veterans to take charge of their own health goals and practices, but it also recognizes that Veterans will need support, guidance, and treatment from health care professionals.
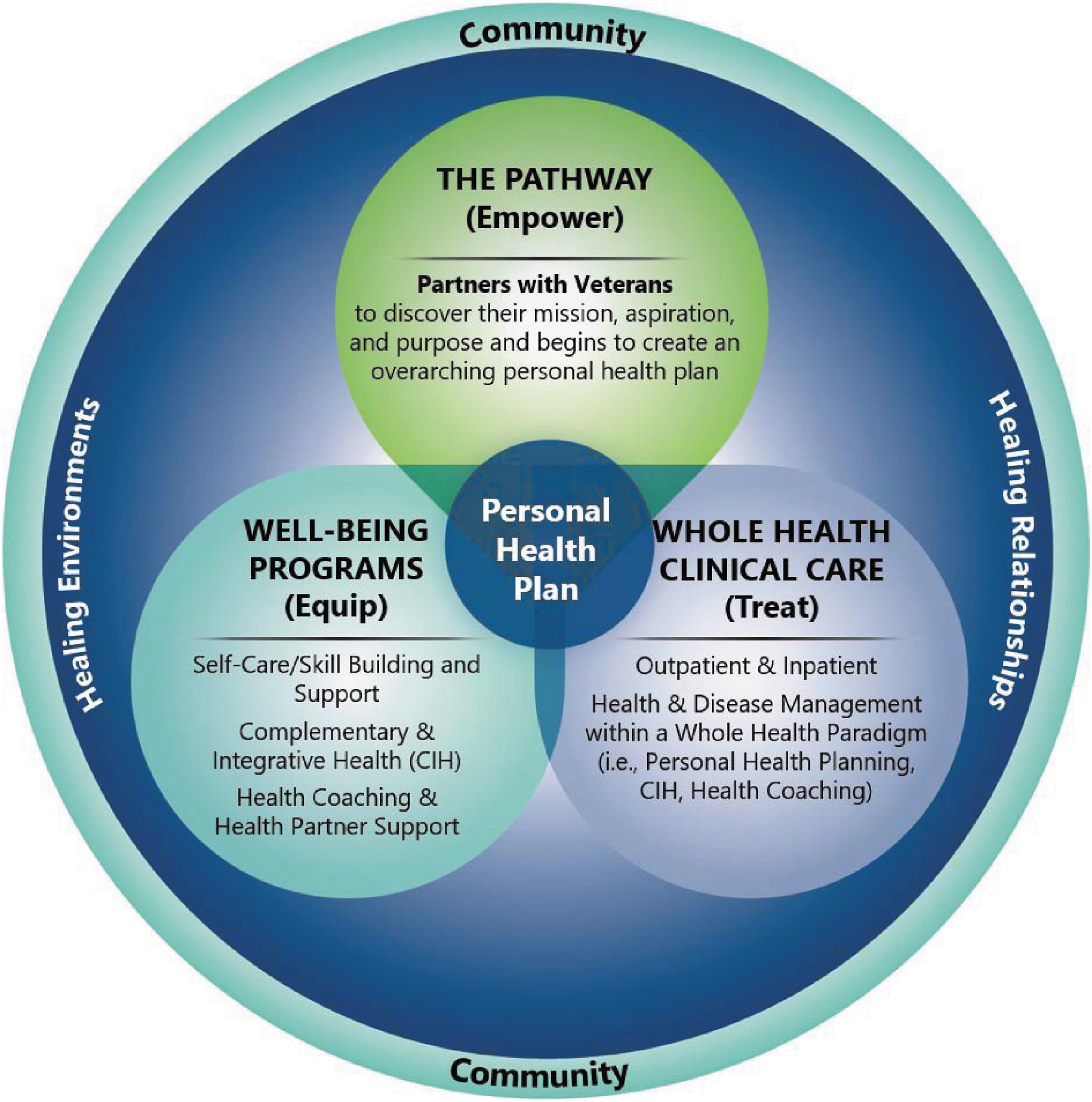
Whole Health system of care.
One approach to engaging and empowering patients is through peer-led group programs. A growing body of research shows that peer-led group programs may provide the necessary support and skill development for participants to become engaged in their own health care, ultimately improving health outcomes. 11 –17 However, much of the research in this area is disease specific, and more research is needed to determine the impact of peer-led group programs on whole-person health and well-being. 18 We conducted a pilot study to assess the impact of one approach to the Whole Health Pathway, a person-driven peer-led group program called Taking Charge of My Life and Health (TCMLH), which fosters Veterans' empowerment and engagement in behaviors to improve their health and well-being. The key objective of our study was to determine whether this nine-week program could impact Veterans' engagement in their own health care, as well as their mental and physical health and well-being.
Methods
We evaluated the impact of the TCMLH program on Veterans who took the course at one midwestern VA medical center. We used a pre–postintervention design with willing participants in 23 group programs. As the primary goal of the study was to inform future implementation of TCMLH, the project was designated as quality improvement by the local Institutional Review Board and written informed consent was not required.
TCMLH curriculum
TCMLH is a 9-week peer-led well-being group program for Veterans (Table 1). Each session is held in nonclinical settings (e.g., conference rooms) for 90-min. TCMLH was developed to provide Veterans with a safe, comfortable, and healing environment in which they can take time with their peers to explore what really matters to them, to consider what they want for their optimal health, and to acquire skills and strategies that will empower them to actively engage in their health care decisions.
Taking Charge of My Life and Health Curriculum
MAP, Mission, Aspirations, Purpose; PHI, Personal Health Inventory; PHP, Personal Health Plan; SMART, specific, measurable, action-oriented, realistic, and timed.
Volunteer Whole Health peer facilitators lead the groups of Veterans through TCMLH. These peer facilitators are not the same as VA peer support specialists, who are Veterans in recovery and specially trained to work with Veterans to engage in mental health and substance use treatment. Whole Health peer facilitators are trained during a 3-day, in-person training course focused on knowledge and skills acquisition related to Whole Health, effective facilitation and group management, and the TCMLH program curriculum. 19 The course provides participants with a facilitator manual that includes an outline, scripts, and resources for each session to help ensure core content and components are delivered with consistency and quality.
During TCMLH, facilitators use the Circle of Health 20 to help Veterans choose areas in their lives where they would like to make changes and learn how self-care and professional care can support their health and life mission (Fig. 2). The process starts with an exploration of the Veterans' MAP—the vision and values that give their life meaning and guide their health plan. Then, peer facilitators use the Personal Health Inventory 20 —a series of questions based on the Circle of Health—to facilitate goal setting and enable Veterans to engage in mindful awareness and self-reflection activities.

Components of proactive health and well-being (circle of health).
TCMLH aims at helping Veterans realize that what matters most to them in their lives is what matters most to achieving their optimal health, and that all areas of their lives—including their body, mind, environment, and relationships—are interconnected. Veterans are guided by peer facilitators to develop SMART (specific, measurable, action-oriented, realistic, and timed) goals, action steps, and accountability partners to achieve success in the area of health they choose. Mindful awareness is central to this program and to the Circle of Health, as the state of being present with one's thoughts and feelings can inform how Veterans choose their path to wellness, including their choice of self-care strategies, their choice of a community that supports their path, and their choice of what matters most to them. Mindful awareness practices are incorporated into weekly sessions, and group participants are provided practices they can do at home to help set their health goal intentions for the day. Other CIH approaches, such as yoga, tai chi, and music therapy, are introduced and resources are provided to participants, so they may seek these self-care strategies within their VA and community.
Participants
Veterans were recruited from participants in 23 TCMLH programs that were offered over the study period (April 2017 to April 2018). Everyone who attended the first session were invited to participate in the evaluation. Groups were held at the hospital's Patient Education Center conference rooms and typically had four to eight participants.
Recruitment and data collection
Before the start of the first group session, a program assistant (not a group facilitator) informed patients about the evaluation (purpose, length, and content of survey, time points, voluntary nature, confidentiality, and contact information) and invited them to participate. Patients who agreed to participate completed the survey. The post-test was completed immediately after the last group session. Participants who did not attend the last session had the option of having surveys mailed to their home address with prepaid return envelopes, or meeting with the program assistant after a VA care appointment. The survey took about 30 minutes to complete. Participants received a $10 VA canteen voucher for each survey completed.
Measures
Veteran characteristics, including age, gender, race/ethnicity, education, employment, financial, housing, and Veteran combat status, and self-reported medical health conditions were collected at baseline.
Survey measures related to pre–post outcomes were aligned with the overarching purpose of OPCC&CT's TCMLH program: to engage Veterans in taking charge of their health and well-being, and to empower them to live their best life with optimal health.
Health status
The PROMIS 10-item global health scale 21 was used to assess overall health status. This validated measure asks 7 general health questions (including quality of life) on a 5-point Likert-type scale (from “poor” to “excellent”), followed by 1 item asking the frequency of being “bothered by emotional problems” (5 points ranging from “never” to “always”), a fatigue rating (5 points from “none” to “very severe”), and pain rating on a 10-point scale from “no pain” to “worst imaginable pain.” There are two PROMIS-10 summary scores: Global Physical Health and Global Mental Health; these subscales are each a t-score normalized to 50. We replaced the PROMIS pain score with the Defense and Veterans Pain Rating Scale (DVPRS), which not only uses the same 10-point scale but also includes verbal and graphic explanations of the scale items. 22
Perceived stress
The 4-item Perceived Stress Scale (PSS) 23 is a validated measure that asks the frequency of perceived stress events on a 5-point scale from “never” to “very often,” where a lower score indicates improvement. Participants were asked how often, over the past month, they felt “things were going your way” and their confidence in their ability to handle personal problems; conversely, they were asked how often they felt “difficulties were piling up so high that you could not overcome them” and unable to control important things in their lives.
Patient engagement and self-efficacy
Patient engagement was measured by using the validated 13-item Patient Activation Measure (PAM), 24 on a 4-point Likert scale from “disagree strongly” to “agree strongly” with an “N/A” option. The PAM measures basic knowledge and beliefs related to patients' confidence in managing their own health, such as knowledge about prescribed medication and treatment options and beliefs in their ability to talk to a provider about concerns or follow through on medical treatment. The items are summed and normalized to a 100-point scale, with higher scores reflecting higher levels of activation. The validated Perceived Health Competency Scale (PHCS) 2-item measure, 25 which has a 5-point Likert scale (from “disagree strongly” to “agree strongly”), was used to assess self-efficacy. The two items are: (1) “I am able to do things for my health as well as most other people” and (2) the reverse-coded statement, “It is difficult for me to find effective solutions to the health problems that come my way.”
Mission, Aspiration, or Purpose
The Life Engagement Test, 26 which was developed to assess “purpose in life,” was used to ascertain the impact of participants' reflections on their MAP as part of the course curriculum. This is a validated 6-item measure with a 5-point Likert scale (from “disagree strongly” to “agree strongly”).
Data analysis
We conducted a pre–post analysis of respondents who completed surveys at both time points, obtaining summary statistics (means, standard deviations [SD], proportions) for the demographic variables collected at baseline and the overall scores at the two time points. We compared the distribution of demographic variables and outcomes between those who completed both surveys with those who only completed baseline surveys by using a chi-square test (categorical variables) and a t-test (continuous variables).
We also tested the significance of the differences in the distribution of the overall scores and the responses to individual questions (considered continuous) between the two time points by using paired t-tests. All analyses were conducted in SAS 9.3 (SAS Institute, Cary, NC). A two-sided p-value <0.05 was considered significant.
Results
Sample characteristics
Of the 97 program participants invited to join the study, 61 completed the pretest survey (a 63% response rate). Of the 61 enrolled participants, 48 (79%) completed the post-test survey. Table 2 displays the distribution of the demographic variables and the outcome scores at baseline overall and by respondent/nonrespondents. Overall, participants were middle aged (50% ages 50–64), male (80%), Non-Hispanic White (72%), unmarried (51%), had at least a college education (75%), basic financial needs were met (53%), unemployed (80%), living in an apartment or house (92%), no Veteran combat status (70%), and had at least two health conditions (95%). On average, they had 6.6 (SD = 3.4) health conditions. The distribution of the demographic variables or the outcomes were similar between respondents and nonrespondents at all waves, except that a greater proportion of respondents than nonrespondents were married (56% vs. 23%; p = 0.03); however, the scores did not vary between them.
Distribution of Veteran Characteristics at Baseline
Multiracial includes two or more checked categories among White, Black or African American, Hispanic, Asian, Native Hawaiian or Other Pacific Islander, or American Indian or Alaska Native.
LET, Life Engagement Test; PHCS-2, Perceived Health Competency Scale-2, PROMIS-10, Patient-Reported Outcomes Measurement Information System Scale-10; PSS, Perceived Stress Scale.
Patient-reported outcomes
Distribution of outcomes at the pre- and post-test are presented in Table 3. Participants reported decreases in perceived stress [mean (SD): 7.5 (3.2) vs. 6.7 (3.2), p = 0.05]. Improvements were observed in both quality of life (as measured by a single item on the PROMIS-10 scale [2.4 (0.9) vs. 2.8 (0.9), p = 0.01] and mental health (as measured by the PROMIS-10 mental health subscale [38.8 (8.9) vs. 40.7 (8.3), p = 0.05]. Responses to the Life Engagement Test scale showed only marginal improvement [20.7 (5.1) vs. 21.8 (4.2), p = 0.11], but responses for the item “I have a lot of reasons for living” increased from pretest to post-test [3.7 (1.2) vs. 4.1 (0.8), p = 0.02]. Finally, participants reported an improvement in patient activation from pretest to post-test, as measured by the PAM score [54.7 (12.1) vs. 60.2 (15.1), p = 0.003]. The overall PROMIS-10 scale, other items of the LET, and the PHCS-2 were distributed similarly in the two groups.
Outcomes at Pre- and Postintervention
T-score normalized to 50.
PHCS-2, Perceived Health Competency Scale-2; PROMIS, Patient-Reported Outcomes Measurement Information System Scale.
Discussion
Providing Veterans with an opportunity to start health care planning with a mindful process to identify what matters most to them in their lives may empower them to engage in their own health care and self-care practices. 18 Our study provides preliminary support for such an approach, as participation in TCMLH positively impacted several important patient-reported health outcomes. Veterans reported lower perceived stress at post-test, which is an important finding since Veterans often endure stress related to physical and mental health, and to nonclinical issues such as housing and unemployment. It is possible that this reduction in stress occurred through use of the program's recommended mindful awareness practices, as studies show that such practices are effective for stress management. 27,28
Veterans also reported improvements on the PROMIS-10, suggesting that TCMLH not only prepares patients to engage in their health care but may also have direct impacts on quality of life.
Although we did not observe overall considerable improvements on the LET, there was an increase in one item that asked participants whether they believed they have “lots of reasons for living.” Depression among the Veteran population is a significant public health concern and can negatively impact appropriate health care utilization, 29 so programming that enhances Veteran perceptions of self-worth and value is extremely important. The group setting, where Veterans who have been through similar experiences are providing support and accountability, may have also influenced this outcome. 12
Veterans reported improvements in engagement with their own health and health care, with an average increase of 5.44 points, and changes as little as 3 points have been associated with improvements in health behavior. 30 Those with greater activation as measured by PAM are more likely to engage in preventive behavior, such as regular check-ups, screenings, and exercise; they are also more likely to prepare notes for doctor's visits, have improved communication with providers, seek out health information, and know about treatment guidelines. 31
The TCMLH group program is unique in that its focus is on overall health and well-being, rather than on a particular disease or illness. Overall, these findings suggest that starting a health program by exploring one's life mission and incorporating mindful awareness in program activities can have a positive effect on well-being and physical and mental health. Our findings are supported by other peer-support studies that show that a peer-facilitated patient-centered care planning process can increase the extent to which participants feel they are receiving responsive care that is inclusive of all clinical and nonclinical issues they face. 12 In this way, participants have an increased sense of engagement and control over the issues they face daily.
In addition, our study provides early evidence that peer interventions can supplement clinical care by teaching patients tools they can use to engage in their own self-care and self-healing. In a busy health care environment, providers often do not have time to engage patients in this type of in-depth exploration of personal health goals. However, we know that goal setting and care focused on patients' goals yields better results. It is possible that a TCMLH group led by a health care professional would yield similar findings, yet the impact of peers is well established in prior work. The use of peer-led group programs is a good alternative to help patients identify their goals, increasing the likelihood of implementing these programs into communities and discontinuing complete reliance on the health care system while cultivating programs that facilitate long-term behavior change. 32 In fact, a meta-analysis on peer support found that peer leaders can help increase participants' sense of hope, control, and ability to activate change, as well as increase their self-care, sense of community belonging, and satisfaction with various life domains, and decrease their feelings of depression and hopelessness. 12
Limitations
Veterans self-selected into the program at a time conducive to their schedule and needs, which may have caused selection bias. Therefore, these results might not be generalizable to Veterans who did not participate in the study or have similar health profiles. Further, since this was a feasibility pilot study, our sample size was small, including group programs offered over the course of a year at one VA medical center. Another limitation is that we did not have access to a control or comparison group, so we cannot rule out other explanations for the improvements we observed. Finally, we did not have access to data about the number of sessions each participant attended nor data on implementation fidelity or quality. Since these types of data may impact outcomes, future evaluations should assess dosage and fidelity as moderating variables. Although the research presented here is an important first step, additional research is required to ensure we can replicate these findings, employing a control group and long-term follow-up.
Conclusion
TCMLH is a part of VA's fundamental shift in approach to health care. The program starts with facilitators helping Veterans realize that what matters most to them in their lives is what matters most to achieving their optimal health, and they begin to understand how all areas of their lives—including their body, mind, environment, and relationships—are interconnected. Central to the TCMLH program is the use of Veteran peers in a group-based setting. As the Whole Health movement expands, both in VA and elsewhere, our findings suggest that engaging patients in an exploration of their life mission and its connection with their health can help patients in several ways, including physical and mental health and overall well-being. Measuring the key concepts in Whole Health that are meant to improve both engagement with care and well-being—and not the typical disease-focused outcomes—will help ensure that the true value of the program is being assessed. Improvement in key areas of health and well-being indicates that TCMLH is an exemplar group-based peer-led intervention. Further study is warranted, and expansion of the program will allow for a more rigorous future evaluation.
Footnotes
Authors' Contributions
D.R. led the design of the TCMLH group program curriculum. B.G.B., A.M.B., and S.R.R. designed the study and survey instrument. A.M.B. collected the survey data. A.M.B., B.G.B., S.R.R., and M.O. analyzed the data. M.H.A., A.M.B., and B.G.B. wrote the article with input from all authors.
Acknowledgments
The authors gratefully acknowledge the contributions of the Veterans Health Administration's Office of Patient-Centered Care and Cultural Transformation, for their guidance with the development and implementation of the TCMLH program and evaluation.
Disclaimer
The views expressed in this article are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs, or the United States Government.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by the Veterans Health Administration Office of Patient Centered Care and Cultural Transformation [VA777-12-C-0002; Rychener, PI], and the U.S. Department of Veterans Affairs, Quality Enhancement Research Initiative (PEC 13–001).