
Abstract
Objectives:
Patients with osteoarthritis (OA) are more likely to develop coronary heart disease (CHD) than the general population. Acupuncture is commonly used in OA patients; however, the therapeutic effect of acupuncture on the risk of CHD in patients with OA and the association between OA patients and their risk to develop CHD in Taiwan are unknown. We investigated the risk of CHD according to acupuncture use in OA patients and compared it with the general population.
Design:
Records obtained from Taiwan's National Health Insurance Research Database identified 84,773 patients with OA, which were compared with 727,359 patients without OA diagnosis. Five thousand forty-six of those who met study inclusion criteria had 1:1 frequency matching and were categorized as OA-acupuncture cohort (n = 1682), OA nonacupuncture cohort (n = 1682), and non-OA cohort (n = 1682). Cox proportional hazards regression analysis determined the risk of CHD, which was defined as the study main outcome. Therapeutic effects of acupuncture and medical expenditure were also analyzed.
Results:
OA nonacupuncture cohort had 3.04 higher risk to develop CHD compared with OA-acupuncture cohort (95% confidence interval [CI], 2.54–3.63, p < 0.001) and non-OA cohort had 1.88 higher risk to develop CHD compared with OA-acupuncture cohort (95% CI, 1.52–2.32, p < 0.001). In subgroup analyses, OA patients treated with both acupuncture and oral steroids were at significantly lower risk of CHD compared with those who used neither (adjusted hazard ratio 0.34; 95% CI, 0.22–0.53), and OA patients treated with acupuncture had the lowest medical expenditure in a follow-up time of 6 months, and 3 and 5 years.
Conclusion:
This is the first large-scale investigation in Taiwan that shows the association between OA and CHD and the beneficial effects of acupuncture in OA patients, and their associated risk to develop CHD. Our results may provide valuable information for health policy decision making. Further randomized controlled trials are needed to confirm these observational findings.
Introduction
Osteoarthritis (OA) is the most common form of arthritis among more than 100 different rheumatic diseases 1 and is thought to be a leading cause of disability worldwide. 2 Because of its high morbidity rate, OA is also a major cause of health care expenditures. 2 The most predominant symptoms are pain and loss of movement and function, which greatly affect quality of life. 3 Women and patients older than 50 are more prone to develop the disease, and the knee, hip, and hand are the most affected joints. 4 Nonsteroidal anti-inflammatory drugs (NSAIDs) are added to or substituted for pharmacotherapy with paracetamol, which is considered the first line of oral analgesic before seeing a primary care physician 5 –7 ; however, little evidence exists to support the safety of NSAIDs in patients with cardiovascular risks. 8 In cases of little analgesic effect or NSAID contraindication, glucocorticoids and weak opioids may be used in the short term. 9
Previous epidemiological studies have found an association between OA patients and increased risk of developing cardiovascular disease. 10,11 Several causes that may have a role in pathogenesis include shared etiological features and risk factors like hypertension, diabetes, hypercholesterolemia, and obesity. 11 Oxidative stress, in which diet may also contribute to this condition, has a role with vascular pathogenesis and the progression of coronary heart disease (CHD). 12 Studies have also shown an association between atherosclerosis and OA, 13,14 and the suspected underlying mechanism is vascular alterations that cause a disruption in the circulation of the synovial membrane and subchondral bone, which leads to cartilage destruction. 10,15
Acupuncture, which is part of Traditional Chinese Medicine (TCM) treatment modalities, is commonly used in Asia, 16 and in recent years, its popularity has increased in Western countries. 17 In Taiwan, TCM use is integrated into a modern health care system, supported and subsidized by the National Health Insurance (NHI) program. 18 In 1996, the World Health Organization published a comprehensive review on controlled clinical trials studying acupuncture 19 and outlined 64 conditions for which acupuncture has proven to be an effective treatment. Among them are several types of pain-related conditions, both acute and chronic. 20,21 In a recent survey conducted in Taiwan, the use of acupuncture for diseases of the musculoskeletal system and connective tissue ranked second among adult patients. 16
Acupuncture has been shown to have anti-inflammatory effects in animal models. 22 Moreover, in a randomized clinical trial, electroacupuncture has been observed to have beneficial effect in reducing serum prooxidant antioxidant balance values in obese patients. 23 A recent meta-analysis of randomized controlled trials about the use of acupuncture in OA treatment has demonstrated statistically significant reductions in pain intensity, as well as improvements in functional mobility and health-related quality of life. 24 However, no study has yet demonstrated the effects of acupuncture in OA patients and their risk for developing CHD. Moreover, no prior population-based studies exist, which have evaluated an association between OA and the risk of CHD in the Taiwanese population. Thus, we used the National Health Insurance Research Database (NHIRD) to investigate the incidence of CHD after OA diagnosis among three cohorts: OA-acupuncture, OA nonacupuncture, and non-OA.
Materials and Methods
Data resource
The compulsory NHI program was launched in 1995 and now covers nearly the entire Taiwanese population. The Longitudinal Health Insurance Database 2000 (LHID 2000), was used in this cohort study. This dataset, which is part of the NHIRD databases, contains information of 1 million beneficiaries randomly sampled from the NHI program in the year 2000. LHID 2000 comprises records of clinic visit and hospitalization, which includes, demographic features, medical costs, drug prescriptions, and diagnostic codes, all based on the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). 25 This study was approved by the Institutional Review Board of China Medical University (CMUH104-REC2-115(CR-4)).
Sample participant
From 1 million beneficiaries randomly sampled from LHID 2000, we identified three cohorts, which were assigned to a study period between January 1, 2000, and December 31, 2012: OA cohorts that include patients with the principle diagnosis of OA (ICD-9-CM code 715), which were further divided as OA-acupuncture cohort (n = 2263), OA nonacupuncture cohort (n = 82,520), and non-OA cohort (n = 727,359), which includes patients without any principle diagnosis of OA. Patients in the OA cohorts had at least two ambulatory claims or at least one hospitalization claim with a diagnosis of OA. Patients younger than 18 years (n = 87,453), who had a diagnosis date of CHD (ICD-9-CM codes 410–414 and 429.2) before the initial diagnosis date of OA (n = 57,396) and had missing information for age or sex (n = 75,460) were excluded from the analysis.
In the OA-acupuncture cohort, we further restricted the analysis to include patients who underwent at least 10 times of acupuncture treatments, 6 months following their OA diagnosis with the following treatments codes: manual acupuncture (B41, B42, B80–84, B90–94, P27041, P31103, P32103, and P33031), electro acupuncture (B43, B44, B86–89, and P33032), and complex acupuncture (B45). A total of 1723 OA-acupuncture, 60,352 OA nonacupuncture, and 529,748 non-OA patients were included as the study population. The selection procedure between the OA cohorts was performed using 1:1 frequency matching of each cohort by age (per 5 years), sex, initial diagnosis year of OA, and index year, resulting in a total of 1682 patients in each cohort.
The date of first acupuncture use after the principle diagnosis date of OA was defined as the index date for the OA-acupuncture cohort. The immortal time was defined as the period from the initial diagnostic date of OA to the index date. As patients in the OA nonacupuncture cohort could not be assigned an index date for first acupuncture treatment, they were each randomly assigned a “pseudo-diagnostic date” as an index date. The selection procedure between the OA nonacupuncture cohort and non-OA cohort was performed using 1:1 frequency matching, as well for age (per 5 years), sex, and initial diagnosis year of OA; however, because both cohorts did not receive any acupuncture treatment, their index date was defined as the first date of OA diagnosis. As patients in the non-OA cohort could not be assigned an index date for OA diagnosis, the “pseudo-diagnostic date” as an index date was applied in this cohort as well so that all cohorts could enroll in a similar time. All subjects were followed up until December 31, 2012, or until the first incident of any kind of CHD (ICD-9-CM codes 410–414 and 429.2), which was chosen to be the study primary outcome.
Comorbidity and Medications
Baseline comorbidities included hypertension (ICD-9-CM code 401–405), diabetes mellitus (ICD-9-CM code 250), hyperlipidemia (ICD-9-CM code 272), chronic obstructive pulmonary disease (COPD, ICD-9-CM codes 490–496), epilepsy (ICD-9-CM codes 345), congestive heart failure (ICD-9-CM codes 402.01, 402.11, 402.91, 404.01, 404.03, 404.11, 404.13, 404.91, 404.93, and 428.0), fibromyalgia (ICD-9-CM codes 729.0 and 729.1), stroke (ICD-9-CM codes 430–438), depression (ICD-9-CM codes 296.2–296.3, 300.4, and 311), anxiety (ICD-9-CM codes 300.0, 300.2, 300.3, 308.3, and 308.91), alcoholism or alcohol-related disorders (ICD-9- CM codes 291, 303, 305.00–305.03, 790.3, and V11.3), tobacco dependence (ICD-9-CM code 305.1), and obesity (ICD-9-CM codes 278 and A183). The use of medications included oral steroids, statins, angiotensin-converting-enzyme (ACE) inhibitors, Plavix, and NSAIDs such as aspirin, ibuprofen, naproxen, and celecoxib.
Statistical analysis
Between-group differences in baseline characteristics were estimated using Chi-squared test to compare categorical variables, whereas the Student's t-test was used to compare continuous variables. Univariate and multivariate Cox proportional hazards regression models were used to assess the risk of OA, and the hazard ratio (HR) and the 95% confidence interval (CI) were estimated. A multivariable model was performed by controlling for potential confounding variables like demographic characteristics such as gender, age, monthly income, urbanization level (highest and lowest levels were defined as level 1 and level 7, respectively), and all included comorbidities and medications. Urbanization levels were defined according to population density (people/km2), education levels, and the physician's number per 100,000 people. The differences between the OA-acupuncture cohort and the two other cohorts in the cumulative incidence of CHD were estimated by Kaplan-Meier curves using a log-rank test. Statistical analyses were performed using SAS software (version 9.4 for Windows 10; SAS Institute, Cary, NC, USA) and the significance level was set at 0.05.
Results
The final analysis included 1682 patients of the OA-acupuncture cohort, 1682 patients of the OA-non acupuncture cohort, and 1682 patients of the non-OA cohort (Fig. 1), 1:1 frequency matched by age (per 5 years), sex, initial diagnosis year of OA, and index year of first OA diagnosis (Table 1). For all 5046 patients in the three cohorts, baseline characteristics, comorbidities, medication use, and follow-up time are detailed in Table 1. There were no significant between-group differences in sex and age distributions, urbanization level, and monthly income. Females, monthly income of more than NTD 20,000 and living in a high level of urbanization, were more predominant in all cohorts. Compared with OA-acupuncture cohort, OA nonacupuncture cohort and non-OA cohort had a higher risk of CHD stratified by gender, age, monthly income, and urbanization. OA-acupuncture cohort demonstrated higher risk of comorbidities, and medication use, including hyperlipidemia, COPD, fibromyalgia, stroke, depression, anxiety, oral steroids, statin, NSAIDs, aspirin, ibuprofen, and naproxen, compared with non-OA cohort. OA nonacupuncture cohort demonstrated higher risk of comorbidities and medications, including hypertension, ACE inhibitors use, and celecoxib use, compared with non-OA cohort. Mean follow-up times were 5.33 (median 3.15) years, 3.73 (median 3) years, and 3.8 (median 2.93) years for OA-acupuncture cohort, OA nonacupuncture cohort, and non-OA cohort, respectively. Mean duration in days between diagnosis of OA and index date of first acupuncture treatment was 50.8, 50.9, and 50.7 for OA-acupuncture cohort, OA nonacupuncture cohort, and non-OA cohort, respectively. Table 2 displays the incidences and crude and adjusted HRs (aHRs) and 95% CIs calculated by univariate and multivariate cox proportional hazard models for all three cohorts. Eight hundred three were diagnosed with CHD, 193 (11.3%) were OA-acupuncture cohort, 405 (24.0%) were OA nonacupuncture cohort. and 205 (12.1%) were non-OA cohort. Cox proportional hazards regression analysis after adjusting for sex, age, comorbidities, and drug use showed that OA nonacupuncture cohort had 3.04 higher risk to develop CHD compared with OA-acupuncture cohort (95% CI, 2.54–3.63, p < 0.001), and non-OA cohort had 1.88 higher risk to develop CHD compared with OA-acupuncture cohort (95% CI, 1.52–2.32, p < 0.001). Table 3 displays the therapeutic effects of acupuncture and oral steroids on the risk of CHD in patients with OA. Patients who used only acupuncture or both acupuncture and oral steroids were at significantly lower risk of CHD compared with patients who used neither (aHR 0.19; 95% CI, 0.08–0.47) (aHR 0.34; 95% CI, 0.22–0.53), as were those who used oral steroids only (aHR 1.03; 95% CI, 0.68–1.56). Table 4 displays the therapeutic effects of acupuncture and NSAIDs on the risk of CHD in patients with OA. Patients who used both acupuncture and NSAIDs had 3 times lower incidence rate compared with patients who used only NSAIDs; however, the results were not significant (aHR 0.30; 95% CI, 0.04–2.34). Table 5 displays the average daily medical expenditure of hospitalization and outpatient care, calculated in New Taiwanese dollars (NT$), of diagnosed OA and non-OA patients categorized by follow-up time of after 6 months, and 3 and 5 years. There was a significant difference in medical expenditure between OA-acupuncture cohort compared with the two other cohorts in a follow-up time of after 6 months, and 3 and 5 years. Table 6 displays the top 10 disease categories in the OA-acupuncture cohort, which were accompanied with OA diagnosis. Disease of the musculoskeletal system and connective tissue and injury and poising were the most common categories. Table 7 displays the top 10 OA diagnostic codes in the OA-acupuncture and OA nonacupuncture cohorts. Figure 2 displays the Kaplan-Meier analysis with the log rank test that indicated a lower cumulative incidence of CHD in OA-acupuncture cohort compared with OA nonacupuncture and non-OA cohort (log-rank test, p < 0.001)
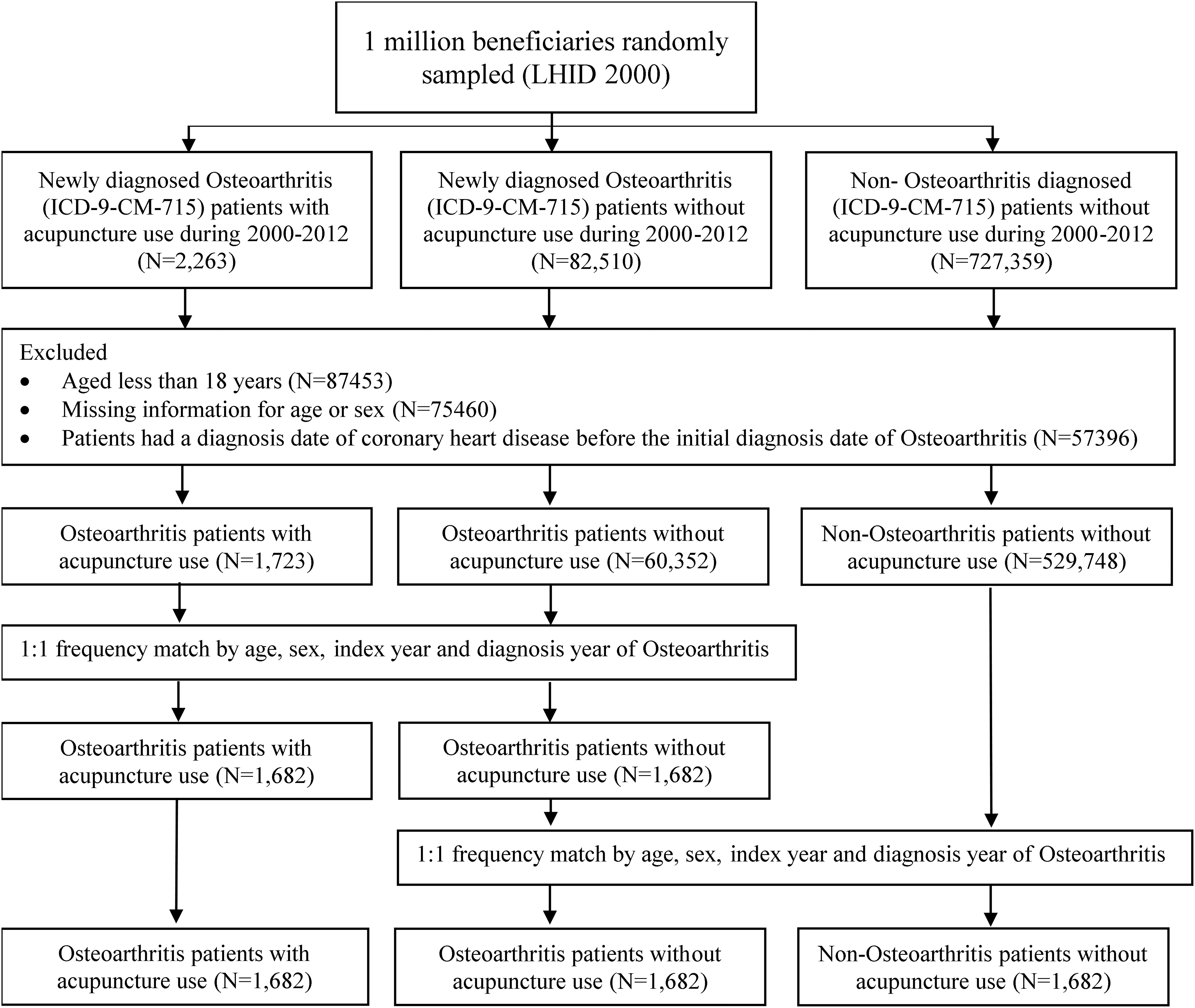
Study population flowchart depicting the rationale for the selected study sample of newly diagnosed OA patients and non-OA diagnosed patients in Taiwan's National Health Insurance Research Database. OA, osteoarthritis.
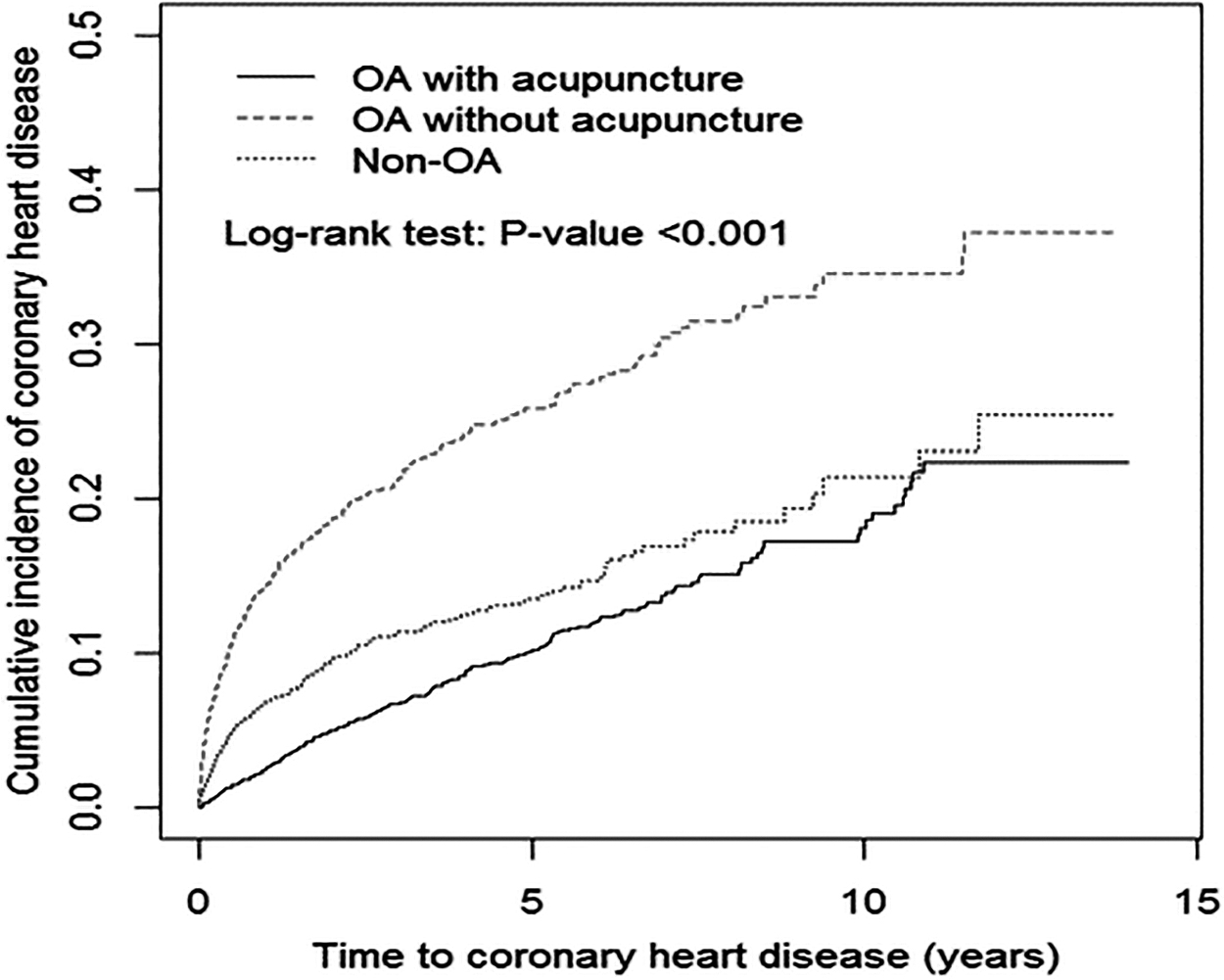
Kaplan-Meier curves with differences in cumulative incidence of coronary heart disease between OA patients with acupuncture, OA patients without acupuncture, and non-OA patients using the log-rank test (p < 0.001). OA, osteoarthritis.
Cox Proportional Hazard Regression Analysis Showing the Risk of Coronary Heart Disease Associated with Acupuncture or Oral Steroidal Treatment in Osteoarthritis Patients
p < 0.05.
p < 0.01.
p < 0.001.
aHR, adjusted hazard ratio for sex, age, monthly income, urbanization, and comorbidities and medication; cHR, crude hazard ratio; CI, confidence interval; IR, incidence rate, per 100 person-years; PY, person-years.
Cox Proportional Hazard Regression Analysis Showing the Risk of Coronary Heart Disease Associated with Acupuncture or Nonsteroidal Anti-Inflammatory Drug Treatment in Osteoarthritis Patients
aHR, adjusted hazard ratio for sex, age, monthly income, urbanization, and comorbidities; cHR, crude hazard ratio; CI, confidence interval; IR, incidence rate, per 100 person-years; NSAIDs, nonsteroidal anti-inflammatory drugs; PY, person-years.
Medical Expenditure of Hospitalization and Outpatient Care of Diagnosed Osteoarthritis and Nonosteoarthritis Patients Categorized by Time of Follow-up
Medical expenditure was categorized according to all-cause disease.
p < 0.05.
p < 0.001.
NT$, New Taiwanese dollars; OA, osteoarthritis; TWD, Taiwan New Dollar.
Top 10 Disease Categories in Osteoarthritis-Acupuncture Cohort
ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification.
The Top 10 Osteoarthritis Diagnostic Codes in Osteoarthritis-Acupuncture and Osteoarthritis Nonacupuncture Cohorts
ICD-9-CM, International Classification of Diseases, Ninth Revision, Clinical Modification; OA, osteoarthritis.
Incidence Rates and Crude and Adjusted Relative Hazards of Coronary Heart Disease Categorized by Osteoarthritis-Acupuncture, Osteoarthritis Nonacupuncture, and Nonosteoarthritis Cohorts and Stratified by Gender, Age, and Baseline Comorbidity and Medication Use
p < 0.05.
p < 0.01.
p < 0.001.
ACE, angiotensin-converting-enzyme; aHR, adjusted hazard ratio for sex, age, monthly income, urbanization, and comorbidities and medication; CHD, coronary heart disease; cHR, crude hazard ratio; CI, confidence interval; COPD, chronic obstructive pulmonary disease; IR, incidence rate per 100 person-years; NSAIDs, nonsteroidal anti-inflammatory drugs; NT$, New Taiwanese dollars; OA, osteoarthritis; PY, person-years.
Baseline Characteristics of Osteoarthritis and Nonosteoarthritis Patients Categorized by With or Without Acupuncture
Chi-squared test; a one-way analysis of variance.
ACE, angiotensin-converting-enzyme; COPD, chronic obstructive pulmonary disease; NSAIDs, nonsteroidal anti-inflammatory drugs; NT$, New Taiwanese dollars; OA, osteoarthritis.
Discussion
This study is the first large-scale investigation in Taiwan that shows the association between OA and CHD and the beneficial effects of acupuncture in OA patients and their associated risk of CHD. After controlling for known risk factors for CHD, our results demonstrate that OA patients who used acupuncture had a significantly lower overall risk of CHD compared with OA patients who did not use acupuncture. Our study also reveals that in both cohorts without the use of acupuncture treatment, the OA cohort had a significantly higher overall risk of CHD compared with non-OA cohort. Our data correlated with previous investigations that found an association between OA and the risk to develop CHD, 10,11 and also highlight a possible role of acupuncture treatment in lowering this risk. In subgroup analyses, OA patients who used only acupuncture or both acupuncture and oral steroids were at significantly lower risk of CHD compared with patients who used neither. We also found that OA patients treated with acupuncture had significantly lower medical expenditure in a follow-up time of 6 months, and 3 and 5 years compared with both OA nonacupuncture and non-OA cohorts.
Acupuncture has shown therapeutic effects on chronic pain and significant differences between true and sham acupuncture indicated that acupuncture is more than a placebo. 21 Acupuncture is a commonly used treatment for painful joints and in a meta-analysis of randomized controlled trials for chronic knee pain, it was reported that acupuncture effect size on pain was similar to that of NSAIDs. 26 Moreover, acupuncture as an adjunctive therapy to topical ibuprofen in patients with chronic knee pain due to OA, has shown effectiveness in decreasing pain and improving functionality. 27 Based on the findings of this study, we suggest some possible explanations underlying the mechanisms of acupuncture in the reduction of CHD. Several studies have postulated the possible association between OA and atherosclerosis. 10,13 While traditionally OA was considered to be a degenerative joint disorder, nowadays, it is being observed as a disorder that is highly correlated to the metabolic syndrome and chronic inflammation plays an important role in the pathogenesis of OA, as well as with other comorbidities like diabetes mellitus, hypertension, and cardiovascular disease. 28 Apart from its analgesic effects, acupuncture has been shown to exert anti-inflammatory effects. In animal models, acupuncture has shown significant reduction of proinflammatory factors such as tumor necrosis factor-alpha, interleukin-1beta, interleukin-6, nitric oxide synthase, cycloxygenase-2, and matrix metalloprotease-9. 29 Electroacupuncture has shown to exert a neuroprotective function in ischemic stroke through inhibition of TLR4-/NF-κB-mediated inflammation. 22 In clinical studies, acupuncture has been observed to have a beneficial therapeutic effect on vascular function by improving lipid profile 30 and lowering blood pressure, 31 known risk factors for CHD. In diabetic patients, acupuncture has shown to improve insulin sensitivity by reducing body weight and inflammation and improving lipid metabolism and adipokines. 32 Therefore, acupuncture appears to reduce the incidence of CHD by improving known risk factors for CHD and exerting anti-inflammatory properties. Our study also evaluates the effects of acupuncture, NSAIDs, and oral steroids in a subgroup analysis for the risk of CHD in OA patients. The analgesic effect of NSAIDs in OA of the knee is small and short term. 33 In our study, patients who used both acupuncture and NSAIDs had 3 times lower incidence rate compared with patients who used only NSAIDs (Table 4). Although the result was not significant, given the fact that in patients with cardiovascular risk factors, NSAIDs should be used in caution even for short term and in some cases are contraindicated, 34 the use of acupuncture, which is a safe with very minimal adverse effects, 35 as a pain relief treatment should be considered for both OA management and CHD prevention. OA is associated with an extremely high economic burden, with direct costs for medical procedures and medication use and indirect costs for time lost for both patients and health care providers. 36 Our data suggest that OA-acupuncture cohort was significantly less costly to care for and our finding is similar to other Taiwanese reports that showed that TCM services are associated with lowest medical expenditure. 37,38 Limited physical activity, which is mainly caused by OA of the hip or knee, is considered a known risk factor for CHD. 39 At the same time, there is evidence to support the use of exercise to improve the damage of the joints and alleviate pain. 6 Nevertheless, generalized and unspecified site diagnostic code was found to be the most common and there was no significant change between the OA-acupuncture and OA nonacupuncture cohorts (Table 7). The possibility for acupuncture's prevention effect on CHD might be related to the patient's lifestyle. A previous population-based study found that TCM users, who used acupuncture as well, more regularly engage in physical exercise. However, it was revealed in the same study that TCM users have more comorbidities; their health status is considered to be worse and in need of more comprehensive health care. 40 In our study, OA-acupuncture cohort also demonstrated a higher risk of comorbidities and medication use; however, this cohort had the lowest incidence of CHD, suggesting the role of acupuncture treatment on CHD prevention.
This study had several limitations, which arise from the nature of retrospective analysis and characteristics of the NHIRD database. First, patient's lifestyle information is not provided by the NHIRD. Therefore, these potential confounding variables such as smoking, alcohol drinking, and dietary habits, patients' body mass index values, exercise, and family medical history may all affect the interpretation of our results. Second, NHIRD does not provide more detailed clinical evaluations, which include, physical, laboratory, and imaging examinations; therefore, the level of OA severity in both cohorts is unknown. In recognition of these limitations and the fact that CHD is a heterogeneous disease, we preformed 1:1 frequency matching to determine the association of OA to CHD with or without acupuncture treatment, resulting in similar baseline characteristics in all cohorts, which also included comorbidities and medications. Moreover, even though information on lifestyle risk factors was lacking, our analysis included diagnostic codes of diseases resulted from these lifestyle habits, such as tobacco dependence, obesity, and alcohol-related disorders. Third, the diagnosis of any type of disease in the NHI database, including OA, CHD, or any other comorbidity, relies entirely on ICD codes. However, NHIRD database is considered to be a reliable and accurate source of information. 41 To ensure correct diagnosis and prevent falsified clinical records, heavy penalties of up to 100-fold of the claimed amount of reimbursement are charged. 42 Fourth, selection of acupoint and treatment protocols by TCM doctors is not recorded in the database. According to TCM treatment principles, acupoint selection is individualized, may vary during the progress of the disease and based on pattern differentiation. Therefore, we restricted the analysis to include patients who underwent at least 10 times of acupuncture treatments and were followed up for long term. Nevertheless, this large-scale, nationwide matched cohort study offers valuable insights into the protective effect of acupuncture treatment on CHD prevention and the possible role of acupuncture as part of integrative medicine in the reduction of risk for CHD among patients with OA. Future randomized controlled trials, with long-term follow-up, comparing the effects of acupuncture on OA patients and their risk to develop CHD are needed.
Conclusion
Our findings show that patients with OA are at a higher risk to develop CHD and acupuncture has beneficial effects on OA patients and their associated risk of CHD. Our data may provide valuable information for health policy decision making. Therefore, rigorous prospective clinical studies are warranted and further mechanistic studies are needed to confirm these observational findings and to investigate the underlying mechanism.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported, in part, by grants from Taiwan's Ministry of Health and Welfare Clinical Trial Center (MOHW109-TDU-B-212-114004), MOST Clinical Trial Consortium for Stroke (MOST 108-2321-B-039-003-), and Tseng-Lien Lin Foundation, Taichung, Taiwan.