
Abstract
Objectives:
To investigate the efficacy of acupuncture in preventing cerebral vasospasm following aneurysmal subarachnoid hemorrhage (SAH) and explore its underlying mechanism.
Design:
A randomized, double-blinded, and placebo-controlled trial.
Setting/Location:
Subjects were recruited from Kyung Hee University Hospital at Gangdong, Seoul, Korea
Subjects:
A total of 50 patients admitted with acute SAH.
Interventions:
The study group received acupuncture treatments (n = 25), while the control group underwent mock transcutaneous electrical nerve stimulation and sham acupuncture (n = 25) six times/week for 2 weeks.
Outcome measures:
The primary outcome was the incidence of delayed ischemic neurologic deficit (DIND), and secondary measurements included angiographic vasospasm, vasospasm-related infarction, modified Rankin Scale score, and plasma nitric oxide (NO) and endothelin-1 (ET-1) levels.
Results:
The study group treated with acupuncture showed a lower incidence of DIND (9.1%) than the control group (20.8%); however, this difference in the incidence of DIND was not statistically significant. The study group demonstrated better clinical outcomes, especially in functional recovery. Significant alterations in plasma NO and ET-1 levels after the 2-week intervention were observed only in the study group.
Conclusions:
Their study shows that acupuncture treatment improved functional recovery after SAH and could potentially prevent cerebral vasospasm. These effects could be attributed to the recovery of endothelial dysfunction by acupuncture through modulating the plasma NO and ET-1 levels.
The study protocol has been registered on
Introduction
Subarachnoid hemorrhage (SAH) is a common and devastating disease affecting 7.9 cases/100,000 person-years worldwide. Aneurysmal SAH can induce heavy financial burdens on those affected due to its high mortality and morbidity. 1 Cerebral vasospasm, one of the leading causes of disability and death after SAH, usually occurs on the third day after SAH (peaks on day 7–10) and lasts for up to 2–3 weeks. 2 It is important to reduce the incidence of cerebral vasospasm in patients because it can cause delayed ischemic neurologic deficits (DINDs) in almost 50% cases. DIND can trigger secondary cerebral infarction in 50% cases and lead to permanent sequelae (35%) or death in severe cases (30%). 3
The pathophysiology of cerebral vasospasm after SAH is complicated and only partially understood. When an intracranial aneurysm ruptures, interconnected cascade of events such as smooth muscle contraction, free radicals, and disrupted endothelial factors contribute to the occurrence of cerebral vasospasm. Furthermore, the development of cerebral vasospasm is associated with the acceleration of oxidative stress by breakdown products from the ruptured aneurysm, leading to endothelial damage causing an imbalance between vasodilation and vasoconstriction. 4,5
Based on this pathophysiology, many therapeutic attempts, including triple-H therapy, calcium blockers, statin, endothelin (ET) receptor antagonist, and selective inhibitor of phosphodiesterase type-3, have been established to prevent cerebral vasospasm. However, an optimal strategy has not yet been elucidated, because no particular treatment successfully improved clinical outcomes or maintained a sustained effect, and larger-scale studies were required for verification. 6,7
In East Asia, acupuncture has been used for centuries for the effective and safe treatment of cerebrovascular diseases. Recently, some studies have reported that acupuncture can improve vascular endothelial dysfunctions, 8 –10 and these effects could provide clues about the mechanisms of cerebral vasospasm prevention. The authors conducted a retrospective case–control study on the efficacy of acupuncture in preventing cerebral vasospasms and showed promising results. 11 Based on the preliminary study, a randomized controlled trial was conducted to confirm the efficacy of acupuncture and explore the potential mechanisms of cerebral vasospasm.
Materials and Methods
Study design
This was a randomized, double-blinded, and placebo-controlled trial. The authors followed the CONSORT (Consolidated Standards of Reporting Trials) and STRICTA (Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture) recommendations.
12
The protocol of this trial has been registered on
Ethics approval
The present trial was carried out according to the Declaration of Helsinki and Korean Good Clinical Practice Guidelines. This study was approved by the Institutional Review Board of the Kyung Hee University Hospital at Gangdong (KHNMC-OH-IRB 2014-001-002). Written informed consent was obtained from each patient or a legal representative.
Participants
Participants were recruited from September 2014 to June 2017 in the Kyung Hee University Hospital at Gangdong. Their study recruited patients admitted with acute SAH. Inclusion criteria were as follows: (1) confirmation of aneurysmal SAH by cerebral angiography or computed tomography (CT); (2) management of ruptured aneurysm through surgical clipping or endovascular coiling (Guglielmi detachable coiling); (3) acupuncture treatment within 96 h after SAH; (4) Hunt and Hess Scale (HHS) score 1–4; (5) age >18 years; and (6) voluntary participation and signed informed consent.
Exclusion criteria were as follows: (1) nonaneurysmal or recurrent aneurysmal SAH; (2) HHS score 5; (3) severe heart, liver, or renal failure; (4) prior experience with acupuncture or electroacupuncture (EA) treatment; and (5) attachment of cardiac pacemakers.
Drop out criteria included the following: (1) missing >3 sessions out of 12; (2) withdrawal of informed consent; (3) serious adverse events making the trial unsustainable; and (4) difficulty in proceeding with the trial due to worsened condition as determined by the principal investigator.
The authors enrolled 50 healthy controls (HCs) that had not experienced any cerebrovascular diseases and were of the same sex and age as the SAH patients to compare the plasma nitric oxide (NO) and ET-1 levels at baseline.
Randomization
This was a randomized controlled trial, with all acute SAH patients allocated in a 1:1 ratio either to the control or study group. Stratification was performed according to sex and initial HHS. Randomization was conducted by an independent administrator not involved in the intervention or assessment using a computer-generated list of numbers with a block size of 4. After the informed consent form was signed, and the HHS score was evaluated, the physician involved in the intervention received a random number by phone. The outcome assessors and participants were blinded to the intervention type.
Intervention
Interventions were conducted six times a week every day for 2 weeks by qualified Korean Medicine doctors with over 3 years of clinical experience who completed a college education of 6 years. All participants received conventional treatment (nimodipine) along with prophylactic therapy and general management.
In the study group, every session included the application of manual acupuncture, EA, and intradermal acupuncture. Acupuncture needles (Dong Bang Acupuncture, Inc., Chungnam, Korea) were inserted bilaterally at the acupoints PC6 (Neiguan), ST36 (Zusanli), ST43 (Xiangu), and SP4 (Gongsun). The depth of insertion was between 1.0 and 1.5 cm, depending on the acupuncture points. The needles were then manipulated until de qi (composite needling sensation considered as effective stimulation) was acquired. The handle of the needle was connected to an electric stimulator (ES-160; ITO Co., Japan) at bilateral PC6 and ST36 and charged with a current of 5 Hz. The degree of stimulation was sufficient to reveal slight muscle contraction, reaching the maximum tolerable intensity not felt by pain. The needles were in position for 20 min before removal. The physician could regulate the intensity according to the patient's response. After removal of the needles, intradermal acupuncture needles with tape (DB130A, 0.25 × 1.5 mm; Dong Bang Acupuncture, Inc.) were attached to the same bilateral acupoints and maintained until the next session.
Mock transcutaneous electrical nerve stimulation and sham intradermal acupuncture were applied in the control group. First, electrical insulators (Medi trace 200 foam electrodes; Ludlow Technical Products Canada, Ltd., Ontario, Canada) were affixed to the bilateral PC6 and ST36 acupoints. Second, the same electrical stimulator was connected to the acupoints for 20 min without a current. The subjects in the control group could see the same lights and hear the same sounds coming from the machine as those in the study group. After electrical stimulation, the acupuncture needles were removed, and 3M micropore medical tape (1 × 1 cm) was placed on the skin at the bilateral PC6 and ST36 acupoints. Then, sham intradermal acupuncture needles, not penetrating the skin, were applied at the acupoints. Micropore medical tapes of the same size were placed over the needles and maintained until the next session.
Outcome measures
As a primary outcome, the incidence of DIND was compared between the study and control groups. DIND was defined as an unexplainable new neurologic change on cerebral angiography, lasting >2 h, and not attributed to other causes.
Secondary measurements included incidence of angiographic vasospasm, defined as an arterial spasm, as seen on digital subtraction angiography. 14 The occurrence of vasospasm-related infarction was also measured. It was determined in the area of vasospasm using magnetic resonance imaging or CT. Mortality and modified Rankin Scale (mRS) for functional independence were evaluated at a primary endpoint and 2 weeks after that or during discharge. Plasma NO and ET-1 levels were assayed before and after the intervention. For the assay, a 3 mL blood sample from the brachial vein was centrifuged at 3000 rpm and stored at −70°C before the assay. The level of NO was quantified in duplicate by absorbance at 540 mm for 10 min using a Total Nitric Oxide and Nitrate/Nitrite Parameter Assay Kit (R&D systems, Inc., USA), while the concentration of ET-1 was assayed in duplicate by absorbance at 450 mm for 5 min using an Endothelin-1 Quantikine ELISA Kit (R&D systems, Inc.). Mean values were calculated as the representative value.
Statistical analyses
All data were analyzed using the Statistical Program for Social Sciences (SPSS, version 18.0, Inc., Chicago, IL, USA). Data are expressed as mean (standard deviation) or number (%). To compare the parameters between both groups, an independent sample t test or Mann–Whitney test was used for continuous variables, and Fisher's exact test or Chi-square test was applied for noncontinuous variables. Analysis of covariance (ANCOVA) was conducted to compare the difference in average mRS between baseline and follow-up. To determine the adequate sample size and significance level, post hoc power calculations were performed with the use of the inequality tests for a two-proportion module in PASS 15 software (NCSS Statistical Software) on the basis of normal approximation. 15 To control for possible confounding factors (age, sex, baseline HHS), the ANCOVA was conducted to compare postintervention plasma levels of NO and ET-1. In all cases, p values <0.05 were considered statistically significant.
Results
In this study, 123 SAH patients were screened and 50 were enrolled. In the study group, three participants were dropped due to the presence of bacterial meningitis, septic shock, or pneumonia, while one participant was dropped from the control group for severe pneumonia. Finally, 22 participants in the study group and 24 in the control group completed the study (Fig. 1). There were no significant demographic differences between the two groups, including hypertension, HHS, and Fisher Grade (Table 1).
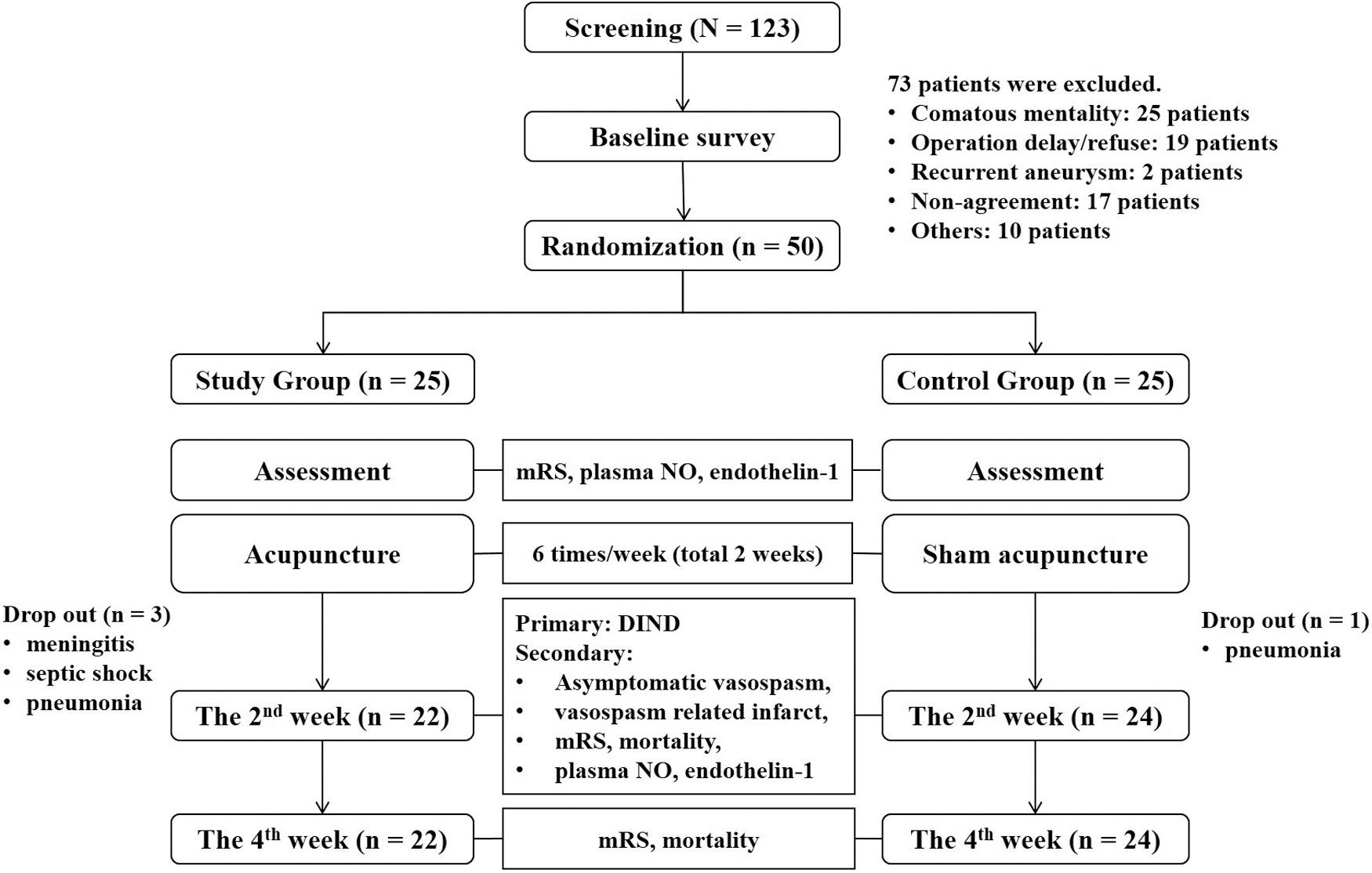
Flow chart of the investigation. DIND, delayed ischemic neurologic deficit; mRS, modified Rankin Scale; NO, nitric oxide.
Baseline Demographics and Clinical Characteristics
Independent t test for age; Chi-square test for sex, hypertension, and operation type; and Fisher's exact test for aneurysm location, Hunt and Hess Scale, Fisher Grade, and modified Rankin Scale were applied. There were no significant differences in demographics and clinical characteristics between the two groups.
The study group showed a low incidence of DIND, although it was not statistically significant. Only 9.1% of the study group experienced DIND, whereas 20.8% suffered from it in the control group. Moreover, the study group (9.1%) had a lower tendency of angiographic vasospasm compared to the control group (25%). While vasospasm-related infarction occurred in 16.7% of the control group, only 4.5% experienced it in the study group. In addition, the average mRS during the second follow-up was significantly lower in the study group, indicating improved functional independence longitudinally. No serious adverse events were reported in either group (Table 2).
Outcome Measurements Between the Study and Control Groups
Bold value indicates the Modified Rankin scale at second follow-up was significantly lower in the study group.
Fisher's exact test.
Analysis of covariance.
The baseline level of plasma NO was significantly lower in the SAH group than HC group. This shows that impaired vasodilation through decreased NO expression is distinctively involved in the occurrence of SAH. Both NO and ET-1 levels were significantly different between the vasospasm SAH subgroup and HC group, but only NO was lower in the nonvasospasm SAH subgroup than HC group (Table 3 and Fig. 2a).

Plasma NO and ET-1 assay results.
Baseline Levels of Plasma Nitric Oxide and Endothelin-1 in Subarachnoid Hemorrhage and Healthy Control Groups
Bold values indicate the baseline level of plasma NO was significantly lower in the SAH group than HC group (p < 0.001). NO was lower in the nonvasospasm group than HC group (p < 0.001). Both NO and ET-1 levels were significantly different between the vasospasm group and HC group (p < 0.001, p = 0.028).
Data represented as mean (standard deviation).
Independent t test.
Mann–Whitney test.
NO, nitric oxide; SAH, subarachnoid hemorrhage; HC, healthy control; ET-1, endothelin-1.
According to the follow-up results, the plasma NO level significantly increased only in the nonvasospasm SAH subgroup, while the ET-1 level showed a decreasing tendency in both the vasospasm and nonspasm groups (Fig. 2b). When comparing the study and control groups, the plasma NO and ET-1 levels in the study group showed simultaneous significant changes after intervention. In the control group, only the level of NO changed after intervention (Fig. 2c).
Discussion
Their study demonstrated that acupuncture could potentially prevent occurrence of cerebral vasospasm after SAH. Moreover, the study group had a higher functional recovery rate and a lower tendency to develop DIND, angiographic vasospasm, and spasm-related cerebral infarction than the control group. These effects could be attributed to the endothelial dysfunction recovered by acupuncture by modulating the plasma NO and ET-1 levels.
Clinically, symptomatic vasospasm or DIND is defined as the clinical development of new focal neurologic signs by arterial spasm. This could be more important than angiographic vasospasm itself because it directly induces disability in patients, lowering the quality of life. 14 Therefore, it is noteworthy that the study group undergoing acupuncture showed significantly improved mRS outcome, considering its relevance in the quality of life. However, the DIND incidence was not significantly different between both groups, with reduced tendency in the study group, and could be due to small sample size. The sample size was planned based on preliminary results, where the incidence of DIND was 10% and 38.9% in the study and control groups, respectively. 11 However, the actual incidence of DIND in the control group (20.8%) was much lower than 38.9%.
During functional recovery, the study group showed a significant difference in the second follow-up of mRS. This improvement could be attributed to two main mechanisms. First, although there was no significant difference, the tendency for vasospasm decreased in the study group that received acupuncture treatment. This can be attributed to acupuncture helping to prevent vasospasm and ischemia. The functional recovery score was confirmed four weeks later. In addition, previous studies have demonstrated that acupuncture treatment might protect neurons from being damaged when the brain is in a hypoxic state. 16,17 Therefore, in this study, even in patients with cerebral ischemia, the neuroprotective effect of acupuncture treatments may have reduced neuronal damage and improved function during recovery. 18,19 Acupuncture treatment in the acute stage of SAH is suggested to be clinically effective for functional recovery and should be widely used as it is effective in preventing vasospasm and has neuroprotective effects.
In their laboratory assay, there was a significant difference in baseline plasma NO levels between SAH patients and HC groups. The SAH group showed simultaneously lower NO levels compared to the HC group, and the vasospasm subgroup showed higher ET-1 levels underlying obvious vasoconstriction. Especially in the baseline ET-1 levels, there was no significant difference between the nonspasm and HC groups, but the vasospasm subgroup showed significantly higher ET-1 level compared with the HC group. Therefore, it is suggested that both NO and ET-1, known as endothelium-derived mediators, could be associated with post-SAH cerebral vasospasm.
After intervention, plasma NO changed significantly in the nonvasospasm SAH subgroup, but not in the vasospasm subgroup. This result implies that in patients without vasospasm, the impaired endothelial vasodilation recovered successfully and did not lead to cerebral vasospasm. As far as the authors know, this is the first report dealing with the temporal recovery of both plasma NO and ET-1 levels in SAH patients, regardless of the presence/absence of vasospasm. Finally, in the longitudinal assay, the study group showed significant increase in plasma NO and decrease in ET-1 levels, but the control group only showed changes in the plasma NO level.
There have been many investigations about the role of plasma NO and ET-1 as screening biomarkers of the vasospasm pathophysiology. NO is a signaling molecule involved in the vasodilation, significantly decreased in SAH, and further reduced in patients with vasospasm. 20,21 ET-1 is a potent vasoconstrictor, elevated in patients with clinical vasospasm. 22,23 Therefore, to prevent cerebral vasospasm following SAH, the disrupted NO and ET-l levels should be recovered.
Thus, it is suggested that acupuncture can modulate the vasodilation of blood vessels through the expression of NO and downregulation of ET-1 and help recover the endothelial dysfunction through the modulation of endothelial NO and ET-1 levels. Acupuncture is known to improve endothelial nitric oxide synthase (NOS) and neuronal NOS synthesis as a regulating mechanism of vascular function. 24,25 EA significantly reduced plasma ET-1 level by improving peripheral blood circulation and elevating skin temperature. 26 The massive sympathetic nervous activation is linked to the genesis of cerebral vasospasm, and it interacts with endogenous ET-1 regulating vascular tone. 27,28 Acupuncture can lower the hyperactive sympathetic tone, suggesting a possible mechanism to regulate endothelial ET-1 levels. 29 Similar to their results, another study showed that EA treatment significantly upregulated the circulating endothelial NOS (eNOS) concentration and downregulated the ET-1 level. 8
It has been reported that EA on ST36 increases the activity of eNOS and the generation and activity of NO. 24,30 eNOS is secreted from vascular endothelial cells to maintain the tension of the vascular wall, and it can be expected that acupuncture on ST36 promotes the production of NO, thus normalizing the function of arterial endothelial cells. Acupuncture on PC6 has been reported to have reduced arterial stiffness in patients with hypertension, 31 and a previous study confirmed that acupuncture on PC6-ST36 improves endothelial cell-dependent vascular extension in hypertension patients with impaired arterial endothelial cell function. 9 There have also been reports that acupuncture on PC6 activates the vagus nerve and inhibits the activity of the sympathetic nerve. 29 Based on these, a retrospective case–control study on the efficacy of acupuncture on PC6-ST36 in preventing cerebral vasospasm after SAH was conducted, and promising results were identified. Therefore, in this study, randomized controlled trial was performed as a follow-up study by adding acupuncture points.
The control group showed significant elevation in plasma NO during the intervention. Hence, even minimal acupuncture may produce contextual effects for benefit, including positive expectations. NO has been pointed out as a possible mechanism in the placebo effect through autonomic nervous system. 32,33
However, this study has several limitations. The sample size was planned based on the preliminary results, but the actual incidence of DIND in the control group was much lower in this study. This may have led to there being no statistical difference in the primary outcome. In addition, despite no statistical difference being apparent, the control group appeared to have a higher initial HHS and Fisher Grade at the start of the study. Therefore, the authors cannot rule out the possibility that these may have affected the outcome measures.
Conclusion
In conclusion, their study shows that acupuncture treatment improved functional recovery after SAH and could potentially prevent cerebral vasospasm. The effect could be attributed to the recovery of endothelial dysfunction by acupuncture through modulating the plasma NO and ET-1 levels. If future studies can include wait-list controls only undergoing conventional therapy, the actual effect of acupuncture in preventing vasospasm can be examined more precisely.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (Grant No.: HI 14C0870).