
Abstract
Background:
There is currently no effective treatment against coronavirus disease 2019 (COVID-19). The optimal selection of interventions targeting the virus is unknown. Therefore, evidence from randomized controlled trials (RCTs) to support specific treatment against COVID-19 is urgently needed. The use of Chinese herbal medicines (CHMs) might have a role in the treatment and symptomatic management of patients with COVID-19. It was aimed at providing an overview of the available evidence and ongoing trials concerning the effects of CHMs for the treatment of COVID-19.
Methods:
This is a narrative review of relevant studies. Searches were conducted to identify documents published till April 22, 2020. Electronic databases, evidence-based collections, websites of relevant organizations, and trial registries were consulted.
Results:
A total of 25 guidelines on the treatment of patients with COVID-19 were identified. Four guidelines provided recommendations on the use of CHMs; these guidelines were developed in China and South Korea and were based on the consensus of experts exclusively. The remaining 21 guidelines provided no guidance on CHMs. No finished RCTs of CHMs for the treatment of patients with COVID-19 was found. According to the evidence evaluated in this review, a Cochrane review of CHMs for severe acute respiratory syndrome and five uncontrolled observational studies of the effects of CHMs in patients with COVID-19, the effects of CHMs for COVID-19 are unknown. A total of 52 ongoing clinical trials of CHM interventions for the treatment of COVID-19 were found. These trials will be carried out mostly in China (n = 51). Forty (77%) of the ongoing trials will be randomized, whereas 12 (23%) have an unclear sequence generation procedure. Forty-seven trials (90%) will have a sample size <400 participants.
Conclusions:
To the authors' knowledge, only the Chinese and the South Korean guidelines recommend CHMs as a treatment option for patients with COVID-19. These guidelines base their recommendations on the consensus of experts. Clinical guidelines or health authorities from other countries do not provide advice on CHMs. Due to the absence of RCT, there is currently no reliable evidence on the effects of any specific CHM intervention for the treatment of patients with COVID-19. A high number of clinical trials of different herbal products are being currently conducted in China.
Introduction
Coronavirus disease 2019 (COVID-19) is an acute respiratory disease caused by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2). COVID-19 has rapidly spread globally since an outbreak first reported in Wuhan in December 2019. As declared by the World Health Organization (WHO) on March 11, COVID-19 is a “public health emergency of international concern,” and the pandemic is overloading health care facilities worldwide.
There is currently no effective treatment against COVID-19. The optimal selection of antiviral agents and interventions targeting the virus is unknown. Therefore, high-quality evidence from randomized controlled trials (RCTs) to support decisions concerning the treatment of COVID-19 is urgently needed.
Traditional Chinese Medicine (TCM) is an essential part of the health care system in China. 1,2 The WHO recognizes this situation and supports the Member States of the Western Pacific Region to integrate traditional medicine into their national health systems. 3 In this line, the WHO International Classification of Diseases (ICD 11) has introduced a new chapter on traditional medicine. 4 TCM is also used in Western countries and is recognized as a complementary or alternative medicine. 5 –7
Chinese herbal medicines (CHMs) are an essential part of TCM. 7 CHMs include single herbs, Chinese proprietary medicines, and mixtures of different herbs, 8 which might be used alone or in combination with Western medicines. CHMs might have a role in the treatment and symptomatic management of patients with COVID-19. 9,10 Herbal plants are routinely used for treating viral respiratory infections in China and might have compounds with capacity against 2019-nCoV. 11 CHMs are considered to have a generalized antiviral effect based on the direct inhibition of viruses, and the control of the associated inflammatory response. Previous in vitro studies of Chinese medicinal herbs have suggested their antiviral activity. For instance, Weng et al. demonstrated the activity of Sambucus Formosana Nakai ethanol extract against human coronavirus NL63. 12
The state administration of TCM of the People's Republic of China, in collaboration with the WHO, initiated clinical research projects on integrated TCM and conventional medicine for the management of SARS. 13 A total of 21 projects covering prevention and treatment were already started, but firm conclusions on intervention efficacy could not be drawn yet. Experts recommended WHO continue to support the research of TCM in treating SARS and other diseases. 13
The Institute for Complementary and Integrative Medicine 14 (Zurich University Hospital) has prepared this report to summarize the evidence concerning CHMs for the treatment of COVID-19. This review has three specific objectives. First, to describe the recommendations on the use of CHMs for the treatment of COVID-19 in clinical guidelines and documents of relevant organizations. Second, to summarize the evidence on CHMs in patients with COVID-19. Third, to provide an overview of the ongoing RCTs of CHMs in patients with COVID-19.
Materials and Methods
This study is a scoping review and did not require written consent or institutional ethical review because it is based on published work exclusively.
Inclusion and exclusion criteria
Type of study designs
The focus of this review was to identify rigorous secondary research and RCTs on this review topic. Thus, we looked for evidence-based clinical guidelines, health technology assessments, systematic reviews, and RCTs. If there was no secondary research or RCTs available, nonrandomized trials were looked for, that is, quasi-randomized controlled trials (quasi-RCTs) and nonrandomized clinical trials. Only if previous designs were not found, observational studies, narrative reviews, and opinion of experts were included. Since it was expected that the evidence base would be scarce or absent, systematic reviews on the effects of CHMs in patients with SARS were also included.
Types of participants
Patients with COVID-19 (the diagnosis as provided by the study authors was accepted). A specific set of diagnostic criteria was not required as these have changed since the beginning of the outbreak.
Types of interventions
Studies evaluating the use of CHMs (combined or not with conventional medicines) for the treatment of patients with COVID-19 were included. To classify an intervention as CHMs, the operational definition provided by the Cochrane review on Chinese herbs combined with Western medicine for SARS was followed. 8,15 Consequently, Chinese herbs were defined as “either raw or refined products derived from plants or parts of plants (e.g., leaves, stems, buds, flowers, roots, or tubers) used for treating diseases.” 8,15 Therefore, this review also covered herbal products used in other countries besides China under the Traditional Eastern Asian Medicine, such as South Korea and Japan. This includes decoction of raw herbs prepared in medical facilities, or concentrated herbal extracts provided according to good manufacture practices by pharmaceutical companies.
This review excluded other interventions defined in Western countries as complementary, alternative, or integrative therapies, such as the use of vitamins or other food supplements, mind–body exercises (e.g., t'ai chi, yoga), psychotherapy, or acupuncture.
We included studies with any comparator and cointerventions. To include a study, the cointerventions should be similar in both study groups to allow determining the effects of CHMs.
Types of outcome measures
It was planned to assess the following outcomes measured at the end of treatment or the end of follow-up: all-cause mortality; COVID-19–related mortality; days to loss of fever; symptom scores (symptoms included fever, fatigue, cough, poor appetite, perspiration, constipation, and diarrhea); duration of symptoms; duration of absorption of pulmonary infiltration; absorption of pulmonary infiltration (assessed with chest X-ray); average daily dose of corticosteroid; dosage of corticosteroid at the end of treatment; duration of corticosteroid treatment; quality of life; number of days in the hospital; and adverse effects. These outcomes were similar to those measured in a Cochrane review of Chinese herbs combined with Western medicine for SARS. 8
Search methods for identification of studies
Literature searches were conducted looking for documents published till April 22, 2020, with no language of publication restriction. The following sources were consulted: (a) electronic databases (Tripdatabase; MEDBOX Rapid Response Toolbox; Epistemonikos; The Cochrane Database of Systematic Reviews [CDSR], and The Cochrane Central Register of Controlled Trials [CENTRAL]); (b) evidence-based collections; and (c) websites of relevant organizations. Experts in China were also contacted asking for related studies or guidelines. To identify ongoing RCTs evaluating interventions for the treatment of COVID-19, the Cochrane COVID-19 Study Register was consulted. 16 Appendix A1 details the search strategies used. The results of the searches were managed with the software Endnote X7. 17
Analysis methods
A narrative description of the evidence found was provided and any meta-analysis was not foreseen to be performed.
Results
Appendix A2 lists all the documents consulted for this report.
Description of the studies
The electronic searches until April 23, 2020, identified a total of 641 records after removal of duplicates. The review finally included 25 guidelines, 1 systematic review, no RCT, and 52 ongoing trials (40 RCTs and 12 trials with unclear randomization). Figure 1 presents a flow diagram describing the results of the searches and the selection process.
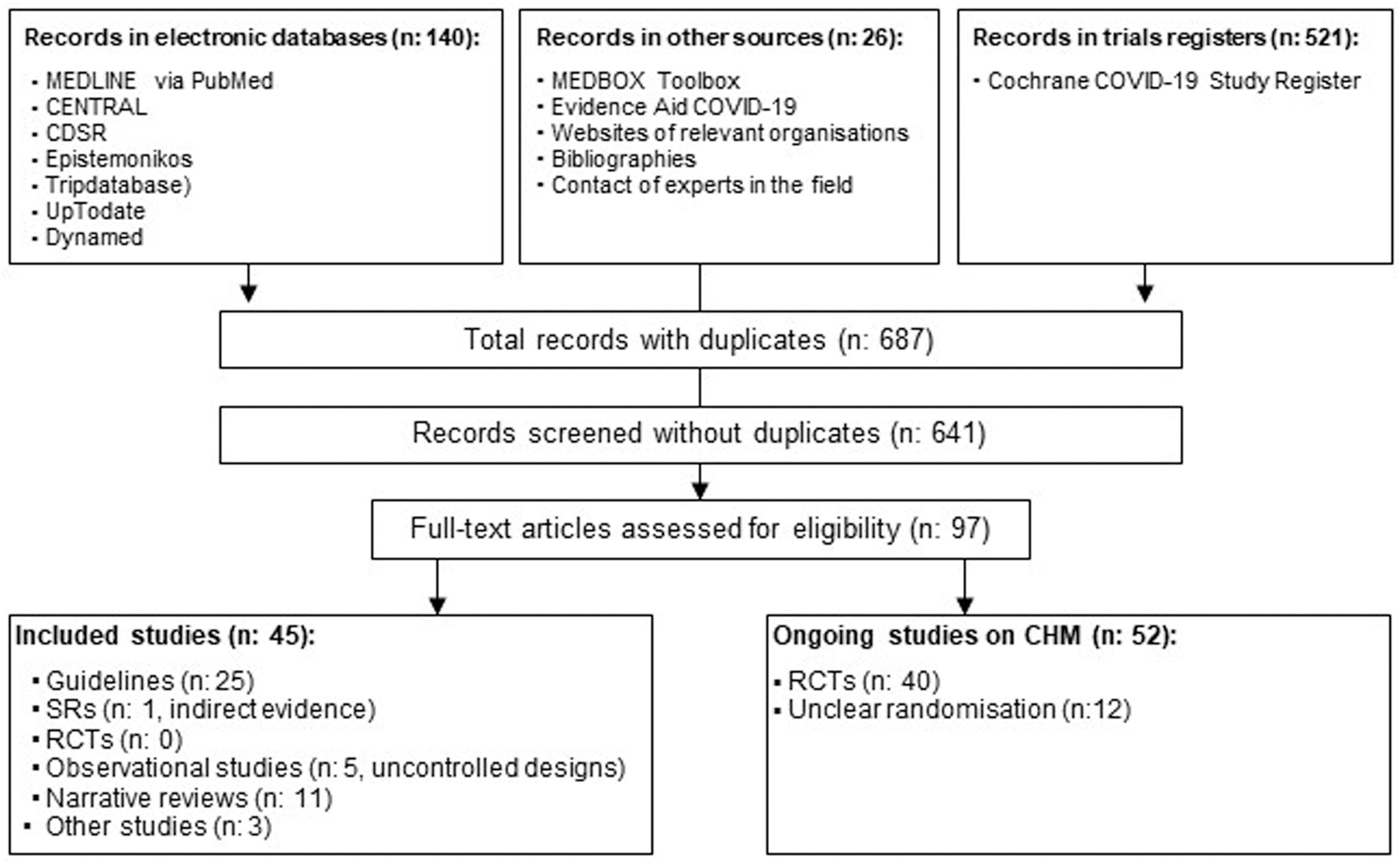
Flow chart. CDSR, Cochrane Database of Systematic Reviews; CENTRAL, Cochrane Central Register of Controlled Trials; CHM, Chinese herbal medicine; RCT, randomized controlled trial; SRs, systematic reviews; TCM, Traditional Chinese Medicine.
Objective 1: To describe the recommendations on the use of CHMs for the treatment of COVID-19 in clinical guidelines and documents of relevant organizations
We identified a total of 25 guidelines providing recommendations on the treatment of patients with COVID-19 (Appendix A2). The guidelines were published in the following countries: United States (n = 5), 18 –22 United Kingdom (n = 4), 23 –26 Canada (n = 3), 27 –29 China (n = 3, reported in 4 publications), 30 –33 Australia (n = 2), 34,35 Germany (n = 1), 36 South Korea (n = 2), 37,38 and Malaysia (n = 1). 39 International organizations developed the remaining guidelines (n = 4), that is, the WHO, 40,41 the European Centre for Disease Prevention and Control (ECDC), 42 and the Surviving Sepsis Campaign. 43 Sixty percent of the assessed guidelines were developed in Western countries (n = 15), whereas 24% (n = 6) in Asia.
The three Chinese guidelines 30 –32 and the Korean Traditional Medicine guidelines 38 were the only ones providing recommendations on CHMs for the treatment of COVID-19. The Surviving Sepsis Campaign guidelines 43 did not provide any recommendation on CHMs, but they stated that several TCMs are undergoing testing. The remaining 20 guidelines (80%) 18 –29,33–37,39 –42 provided no information on CHMs. Two additional guidelines 44,45 were not included in our analysis as, although covering Traditional Chinese Medicine, the focus was on acupuncture.
The three Chinese guidelines 30 –32 and the Korean Traditional Medicine guidelines 38 recommend CHMs as a treatment option for COVID-19. These guidelines are exclusively based on the consensus of experts, and the data to support the recommendations are not detailed. Following we provide a more detailed description of these guidelines.
1. National Health Commission (NHC), National Administration of Traditional Chinese Medicine, sixth edition 32
We consulted two documents related to this guideline: the full guideline, 32 which contained the sixth version of the diagnosis and treatment plan for COVID-19, and a report with the seventh version of this chapter. 31 The guideline claims that “COVID-19 can also be treated with Traditional Chinese Medicine” and describes in detail (including formulas and compounds) an exhaustive list of CHM options according to the clinical situation of the patient, covering from patients with “fatigue with gastrointestinal upset” to “critical patients.” For example, the guideline recommends administering Xue Bi Jing injection 100 mL/day, twice a day for the treatment of severe and critical cases. For patients with “fatigue with gastrointestinal upset,” Huoxiang Zhengqi (capsule/pill/oral liquid) is recommended. More examples of suggested CHM interventions are Qingfei Paidu decoction (QPD), Gancao Ganjiang decoction, Shegan Mahuang decoction, or Qingfei Touxie Fuzheng decoction (see more details in Ren et al. 46 and the guidelines). 32
The authors state that “the guidelines were written based on the study, analysis and summary of the treatment of previous COVID-19 cases.” However, it seems that the recommendations are based on the experts' experience, and no empirical data are provided to support these recommendations. It is also unclear how the guideline team managed their potential conflicts of interest, it seems that there was not a rigorous search of the literature, and there was no assessment of the quality of evidence.
2. Jin et al. 30
According to this article, these guidelines were developed according to the GRADE approach and the WHO guideline development manuals. However, the recommendations for the treatment of COVID-19 with CHMs are based on the guideline already described. 32 Thus, the same conclusions on the limitations apply to these recommendations.
3. The First Affiliated Hospital, Zhejiang University School of Medicine 33
This guideline synthesizes the clinical experience of The First Affiliated Hospital, Zhejiang University School of Medicine (FAHZU), in the treatment of COVID-19. The guide also has a section dedicated to CHMs. However, it has the same weaknesses of the previous two guidelines.
4. Association of Korean Medicine, Korean Association of Traditional Pulmonary Medicine 38
These guidelines recommend the use of CHMs for the treatment of COVID-19 and they are also based on the consensus of experts exclusively. The description of the methods of the guidelines is incomplete, so it could not be known whether there was a rigorous search strategy, the evidence that was considered, or whether there was any attempt to assess the certainty of the evidence.
Objective 2: To summarize the evidence on CHMs in patients with COVID-19
Systematic reviews (n = 1, indirect evidence)
No systematic review of the effects of CHMs on the treatment of patients with COVID-19 was found. One Cochrane review published in 2012 was identified that evaluated the effects of Chinese herbs combined with conventional medicine for SARS. 8 The review included 12 RCTs and 1 quasi-RCT. The review concluded that Chinese herbs plus conventional medicine did not reduce mortality in patients with SARS, as compared with conventional medicine alone. Besides, the review suggested that the addition of the Chinese herbs may have a beneficial impact on the following outcomes: symptoms, absorption of pulmonary infiltration, the average daily dose of corticosteroids, the dosage of corticosteroids, days of corticosteroid treatment, quality of life, and length of stay in hospital. 47 –56 It was considered that the potential benefits identified in this Cochrane review cannot be directly transferred to patients with COVID-19 because the results obtained from patients with SARS may not apply to patients with COVID-19. Besides, as highlighted in the Cochrane review, the quality of the evidence was low.
RCTs (n = 0)
There is no current evidence from RCTs to recommend any specific anti-nCoV treatment for patients with suspected or confirmed COVID-19. 40 Thus, the same conclusion applies to CHMs.
Observational studies (n = 5)
Hereunder, five observational studies describing the effects of different preparations of CHMs in patients with COVID-19 are presented. All these studies are descriptive (without a comparator) with small samples. Three studies are case reports (less than five patients in total), 46,57,58 and one study is a series of 214 cases. 9 The remaining study did not report the sample size. 59
All these studies share the common pitfalls inherent to uncontrolled designs, which do not allow determining the effects of an intervention; they can only suggest that there may be an effect. In addition to that, there was a poor report of the CHM compounds and the conventional treatment received.
According to this one-case report, described in two articles, 46,60 an early intervention with CHMs based on a plant-based mixture called QPD prevented the severe and critical disease in one patient with suspected COVID-19. This case report raises serious concerns mainly because it describes the success of just one patient and because the patient was not confirmed as suffering from COVID-19. 61,62
2. Yang et al. 9
According to this report, the State Administration of Traditional Chinese Medicine has recently recommended combining CHMs and conventional medicine for the treatment of COVID-19 pneumonia. As an example, QPD has been devised to be used in viral infections. According to Yang et al., in the 214 cases who received this treatment, the symptoms disappeared quickly, and there was a rapid disease recovery.
3. Wang et al. 58
This report described the care provided to four patients with mild-to-severe COVID-19. The patients received antiviral treatment (including lopinavir/ritonavir and arbidol), Shufeng Jiedu capsule, that is, a CHM herbal formula, and other necessary supportive care. The authors stated that Shufeng Jiedu capsule may alleviate acute lung injury in patients with COVID-19 and warrants further investigations. 58
4. Kaijin Xu et al.
This report describes the experience of treating patients with COVID-19 at the main hospital in Zhejiang (the number of patients treated is not reported). The authors state that they “[…] also integrated Chinese medicine in treatment to promote disease rehabilitation through classification methods of traditional Chinese medicine.” However, only the abstract could be accessed, which describes the intervention vaguely and does not provide any outcome measure to prove treatment effects.
5. Ni et al. 57
This report describes the first family case of COVID-19 confirmed in Wuhan. The three family members (parents and daughter) responded poorly to routine conventional treatments, so they also received Shuang Huang Lian (SHL) oral liquid, a Chinese Traditional patent Medicine. SHL contains extracts of three Chinese herbs, namely, honeysuckle, forsythia, and Scutellaria baicalensis, and is used to treat sore throat, cold, and cough with fever. The report highlights that “the three cases […] achieved rapid recovery” and suggests that SHL treatment might be effective. Thus, the authors have started a clinical trial (ChiCTR2000029605) to assess the effects of SHL for the treatment of COVID-19. This multicenter nonblinded RCT seems to have started in February 2020.
Other studies (n = 3)
To identify treatment options as soon as possible is critical to alleviating the impact of the COVID-19 outbreak. The WHO has published a list of candidate therapeutics, 63 which does not include any CHM intervention. However, CHMs for the treatment of COVID-19 are still considered in China as an area that requires further clinical research. 64 Zhang et al. 11 proposed a system to screen CHM compounds that may be candidates against COVID-19. This approach has identified 13 natural compounds that exist in Chinese herbs with potential anti-SARS-CoV-2 activity. In total, 125 Chinese herbs contain 2 or more of these 13 compounds.
Objective 3: To provide an overview of the ongoing RCT of CHMs in patients with COVID-19
This search in the Cochrane COVID-19 Study Register threw a total of 521 ongoing trials on interventions to treat COVID-19 with a randomized or unclear assignment. After screening all these records, 52 ongoing trials were identified on the effects of CHMs for the treatment of COVID-19 (Table 1). These CHM trials represent 5.6% of the 921 trials of the Cochrane COVID-19 Study Register (consulted on April 23, 2020). In total, 46 out of the 52 trials (88%) were registered on the Chinese Clinical Trial Registry (ChiCTR), whereas only 6 (12%) in
Ongoing Trials on Chinese Herbal Medicines for the Treatment of Coronavirus Disease 2019 (in Alphabetical Order)
RCT, randomized controlled trial.
Forty (77%) of the ongoing studies on CHMs have been planned to assign the participants to the study arms after a random sequence. The remaining 12 trials (23%) did not report whether they were randomized or not, so we assumed they were not. The planned sample sizes of the trials ranged from 20 to 550 participants (median 120 participants). Only five trials (10%) planned to obtain a sample of at least 400 participants. The trials will evaluate the effects of different herbal products administered orally (n = 40, 77%) or by injection (n = 12, 23%). In 11 (27.5%) of the 40 trials evaluating oral CHMs, the administration form (capsule, granules, tablets, liquid, etc.) was not reported. Table 1 lists all the CHM products that were evaluated. Besides, other nine studies assessing the effects of TCM in patients with COVID-19 were found, but could not conclude whether they focused on CHMs due to poor reporting of the interventions.
Discussion
Summary of main results
A total of 25 guidelines were identified on the treatment of patients with COVID-19. Only four guidelines, all developed in China and South Korea, included recommendations on the use of CHMs. These recommendations on herbal medicines were based on the consensus of experts exclusively.
This review did not find reliable evidence on the effects of any specific CHM intervention for the treatment of patients with COVID-19. No finished RCT was identified. In contrast, indirect evidence provided in a Cochrane review published in 2012 was found on the effects of Chinese herbs combined with conventional medicine in patients with SARS. This Cochrane review concluded that Chinese herbs did not reduce mortality, but that they may have a beneficial effect in several clinical outcomes, such as symptoms, or the absorption of pulmonary infiltration. However, the review authors rated the quality of the evidence as low. Thus, we judged that the indirect evidence obtained from this review does not suffice to consider that CHM interventions have an impact on COVID-19. Five observational studies were also found pointing to a benefit associated with the use of CHMs. All these studies were uncontrolled designs, with small sample sizes and poor reporting, and they do not allow determining the effects of a health care intervention.
This review highlights the need of RCTs to determine the benefits and harms of CHMs for the treatment of COVID-19. A total of 52 ongoing trials evaluating the effects of different Chinese herbal products for the treatment of COVID-19 were found. This is an important step to get solid findings. All the studies but one will take place in China and 40 out of the 52 seem randomized designs.
Potential biases in the review process
The main limitation of this review is its narrative approach. However, the authors tried to state a clear set of objectives with predefined eligibility criteria for the studies. In this line, a review question was formulated according to the PICO-D format, that is, defining the participants, interventions, comparators, outcomes, and the eligible study designs. Also, it was attempted to reduce the risk of publication bias, as demonstrated hereunder.
It is acknowledged that this review did not search in several relevant electronic databases, such as Embase or the Chinese Biomedical Literature. However, MEDLINE (through PubMed) and CENTRAL were consulted (the latter is the largest database of trials in the world). Also, the authors were able to translate documents from Chinese and Korean to English, and contacted Chinese experts asking for relevant trials in the field.
Another weakness of this review is that a direct search of the ChiCTR for ongoing trials was not done. However, ChiCTR is indexed in the WHO ICTRP platform, which, in turn, can be accessed from the Cochrane COVID-19 Study Register, the tool consulted in this review.
The Institute for Complementary and Integrative Medicine 14 (Zurich University Hospital) hosts Cochrane Complementary Medicine Switzerland, 65 a satellite group of Cochrane Complementary Medicine. 66 Cochrane Complementary Medicine is a field established in Cochrane “in 1996 to support and promote systematic reviews of complementary, alternative, and integrative therapies and to function as a link between Cochrane, a worldwide organization that prepares systematic reviews of all kinds of health care therapies, and practitioners, researchers, and consumers with an interest in complementary medicine.” On April 7, 2020, Cochrane launched its COVID-19 Study Register 16 to support rapid evidence synthesis by all systematic review producers. This tool was used to identify ongoing RCTs on CHMs for the treatment of COVID-19. This register was helpful as it allowed searching the ongoing trials on COVID-19 from one source.
It is also acknowledged that the search strategy in MEDLINE focused on Chinese herbal products, the topic of this review. This might have hampered the identification of relevant guidelines or studies on herbal products used in other Asian countries and not categorized as “Chinese.” However, it is still considered that this search strategy allowed identifying the most relevant evidence. First, because the search strategy in MEDLINE also used MeSH terms related to herbal products in general, and not only the Chinese products (“Oriental Traditional Medicine” and “Medicinal Plants”). Second, other sources than MEDLINE were searched, such as databases collecting guidelines (e.g., Trip Medical Database) or the bibliographies of relevant documents.
Agreements and disagreements with other studies or reviews
This review did not find reliable evidence on the effects of any specific CHM intervention for the treatment of patients with COVID-19. This conclusion is consistent with previous analyses that concluded that, to date, there is no intervention recommended to treat SARS-CoV-2. 40
The lack of reliable evidence of the benefits of CHMs in patients with COVID-19 does not support the expectations that CHMs would be a valuable treatment against COVID-19. 64,67 –70 For example, there is no evidence on the effects of CHMs on critical outcomes in the context of the current pandemic, such as the length of hospital stay. A reduced length of stay of patients with COVID-19 is an essential outcome to support decision making in overloaded health care facilities worldwide.
However, the use of CHMs to contain SARS-CoV-2 has been promoted in China, 69 and the Chinese and South Korean guidelines have endorsed the use of CHMs as a treatment option for COVID-19. 30 –32,71 Besides, CHMs have been widely used in China to treat patients with COVID-19. 67 For example, Yin Qiao powder, Huopo Xialing decoction, Maxing Shigan decoction, Liang Ge powder, Qingwen Baidu decoction, and Da Yuan decoction have been widely prescribed for the treatment of COVID-19. 72 Also, ∼85% of the total confirmed COVID-19 cases may have received TCM interventions. 69 In fact, Qingfei Paidu Tang is recommended in the Chinese and the Korean guidelines. 71
Although CHMs have been proposed in China as a treatment option in patients with COVID-19, its efficacy and safety still need to be confirmed by well-designed clinical studies. The website of the National Center for Complementary and Integrative Health in the United States explicitly states that “There is no scientific evidence that any of these alternative remedies can prevent or cure the illness caused by this virus.” 73 Besides, as this site highlights, some alternative treatments may not be safe to consume. 73,74 Gray and Belessis brought up the point that the use of CHMs to treat SARS-CoV-2 may cause harm 75 due to its potential for iatrogenic lung injury (interstitial pneumonitis). 75,76 Also, the interactions of the herbs with conventional treatment should be carefully assessed. 69,77 Therefore, the benefit–risk balance for CHMs needs to be carefully evaluated and acknowledged.
All the Chinese guidelines evaluated in this review recommend the use of CHMs in combination with conventional medicine for the treatment of COVID-19. This finding may lead us to think that the inclusion of TCM-related information in Chinese clinical guidelines is the norm. However, of a total of 604 Chinese clinical practice guidelines on Western medicine, only a small number (74/604; 12%) recommended the use of TCM therapy. 5
All the Chinese national guidelines identified in this overview recommend herbal medicines for the management of COVID-19, and health care professionals in China have used them frequently in patients with COVID-19. Interestingly, as already stated, only 12% of the Chinese biomedical clinical guidelines for other diseases recommended CHMs. 5 This gap might be explained by the fact that there has not been an effective treatment against COVID-19 so far. Nevertheless, extreme situations such as COVID-19 seem to change the processes to generate, synthesize, and implement the evidence, and how all the relevant stakeholders involved (policy makers, guideline developers, and health care professionals) contribute. A deeper understanding of how the evidence ecosystem adapts to a pandemic might be an interesting topic of future research.
This review highlights that so far no recommendation of CHMs in the Chinese guidelines was developed according to transparent, explicit, and rigorous methods. This finding is compatible with the results of another study, which found that only 9% (7/74) of the Chinese clinical guidelines providing recommendations on TCMs had followed a system to grade the evidence and develop the recommendations. 5
This review found a high number of trials (n = 52) that are currently running to determine the effectiveness of CHMs for the treatment of COVID-19. However, 12 of these trials will be nonrandomized, and only 5 trials will have a sample size of at least 400 participants. Small samples imply that most of the ongoing trials will not be powered enough to detect differences in the primary outcome of the study. Besides, 27.5% of the trials evaluating oral CHMs did not report the form of administration (capsule, granules, tablets, liquid, etc.). Also, nine additional ongoing trials were found with a poor reporting that prevented knowing whether they were planning to evaluate CHMs. These findings are broadly compatible with the results of previous studies, which highlighted that the COVID-19 trials on TCM registered so far were poorly reported and small sized, thus they might not provide reliable information for decision making. 69,78, * , †
Conclusions
Implications for practice
To the authors' knowledge, only the Chinese and the South Korean guidelines recommend CHMs as a treatment option for patients with COVID-19. These guidelines exclusively base their recommendations on the consensus of experts. Clinical guidelines or health authorities from other countries do not provide advice on CHMs.
There is currently no reliable evidence on the effects of any specific CHM intervention for the treatment of patients with COVID-19. No completed RCTs on CHMs were found for the treatment of patients with COVID-19. According to the evidence evaluated in this review, a Cochrane review of CHMs for SARS and five uncontrolled observational studies, the effects of CHMs for COVID-19 are unknown.
Implications for research
Well-designed and adequately powered RCTs to determine the effects (benefits and harms) of CHMs in patients with COVID-19 are needed. A high number of RCTs of different herbal products are being conducted in China.
Footnotes
Acknowledgments
The authors thank Hospital Universitario Ramón y Cajal (Madrid) for the provision of full text articles. They also thank Jianping Liu for providing information on relevant studies and guidelines.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.