
Abstract
Objectives:
Acupuncture is an important Traditional Chinese Medicine modality based on the fundamental theory that disease is caused by disruptions in the body's qi. Understanding the use of acupuncture in dermatology is important due to the rising prevalence of complementary and alternative medicine use. A systematic review published in 2015 found that acupuncture improves outcomes in several dermatological diseases. We performed a systematic review of studies that have been done since then to present updated evidence.
Methods:
A systematic search of MEDLINE, EMBASE, and the Cochrane Central Register was performed. Studies were limited to clinical trials, controlled studies, case reports, comparative studies, and systematic reviews published in the English language. Studies involving moxibustion, electroacupuncture, or blood-letting were excluded.
Results:
Results showed that acupuncture improves clinical outcomes in uremic pruritus, atopic dermatitis, urticaria, and itch. Acupuncture does not significantly reduce postoperative itch in patients undergoing cesarean section under spinal anesthesia.
Conclusions:
While there are some promising studies that support the use of acupuncture for skin diseases, additional large-scale, randomized, sham-controlled trials need to be performed to present consistent high-level evidence of acupuncture's role in dermatology.
Introduction
Acupuncture is a Traditional Chinese Medicine (TCM) modality that primarily uses needles to stimulate specific points on the body to restore the balance of qi, or vital energy in the human body. 1 Other variations that use heat or moxibustion, cupping, suction, or pressure are also practiced. Traditionally, acupuncture is usually used in conjunction with other modalities in TCM. 2 The basis of acupuncture is the theory that disease is caused by disruptions in the body's qi, which flows along channels, or meridians that form a network throughout the body. 2,3
Acupuncture is used complementarily to modern medicine and independently with a long history of use in China, Taiwan, Japan, and Korea. 4,5 The National Institutes of Health (NIH) declared that there was scientific evidence of acupuncture's efficacy in select clinical situations in 1997 as acceptable alternatives to mainstay treatments or adjunct treatments. These situations included postoperative and chemotherapy nausea and vomiting, postoperative dental pain, addiction, fibromyalgia, menstrual cramps, headaches, and musculoskeletal pains such as osteoarthritis, low back pain, and tennis elbow. 6 Acupuncture use in the general population in the United States was estimated at a prevalence between 0.6% and 1.4% in 2007. 7 An understanding of acupuncture in treating skin disease is vital as the number of patients seeking complementary and alternative medicines increases. A systematic review in 2015 by Ma and Sivamani concluded that acupuncture improves outcome measures in several dermatological conditions, including dermatitis, chloasma, pruritus, urticaria, hyperhidrosis, and facial elasticity. 8 Since then, many new studies on acupuncture in skin disease have been completed. Herein, we present a systematic review from 2014 onward that assesses the results and quality of the studies that investigate the use of acupuncture to treat a variety of dermatological disorders.
Methods
Study selection
A systematic search of Pubmed, EMBASE, and Cochrane Central Register was performed looking for articles from January 1, 2014 to December 31, 2020 (Fig. 1). Search terms included Acupuncture [AND] (“dermatology,” “skin disease,” “atopic dermatitis,” “psoriasis,” “hidradenitis suppurativa,” “pruritus,” “urticaria,” “dermatitis,” “rosacea,” “itch,” “melasma,” “acne,” and “wart”). We originally followed the 2015 systematic review protocol that only used “dermatology,” “skin disease,” and “acupuncture” as search terms, but then adjusted our methods to include the more commonly found dermatological conditions in our search to identify additional articles. Seven hundred thirty-six articles across all three electronic databases were initially found. We replicated the 2015 systematic review's inclusion criteria, which included studies in English evaluating acupuncture or acupressure as the main treatment modality in dermatological conditions. Studies that used moxibustion, electroacupuncture, or blood-letting as forms of acupuncture were excluded. Case reports, clinical trials, controlled studies, comparative studies, and systematic reviews were included. Systematic reviews were included for reference review. After abstract and title review, a total of 23 articles in the English language were included.
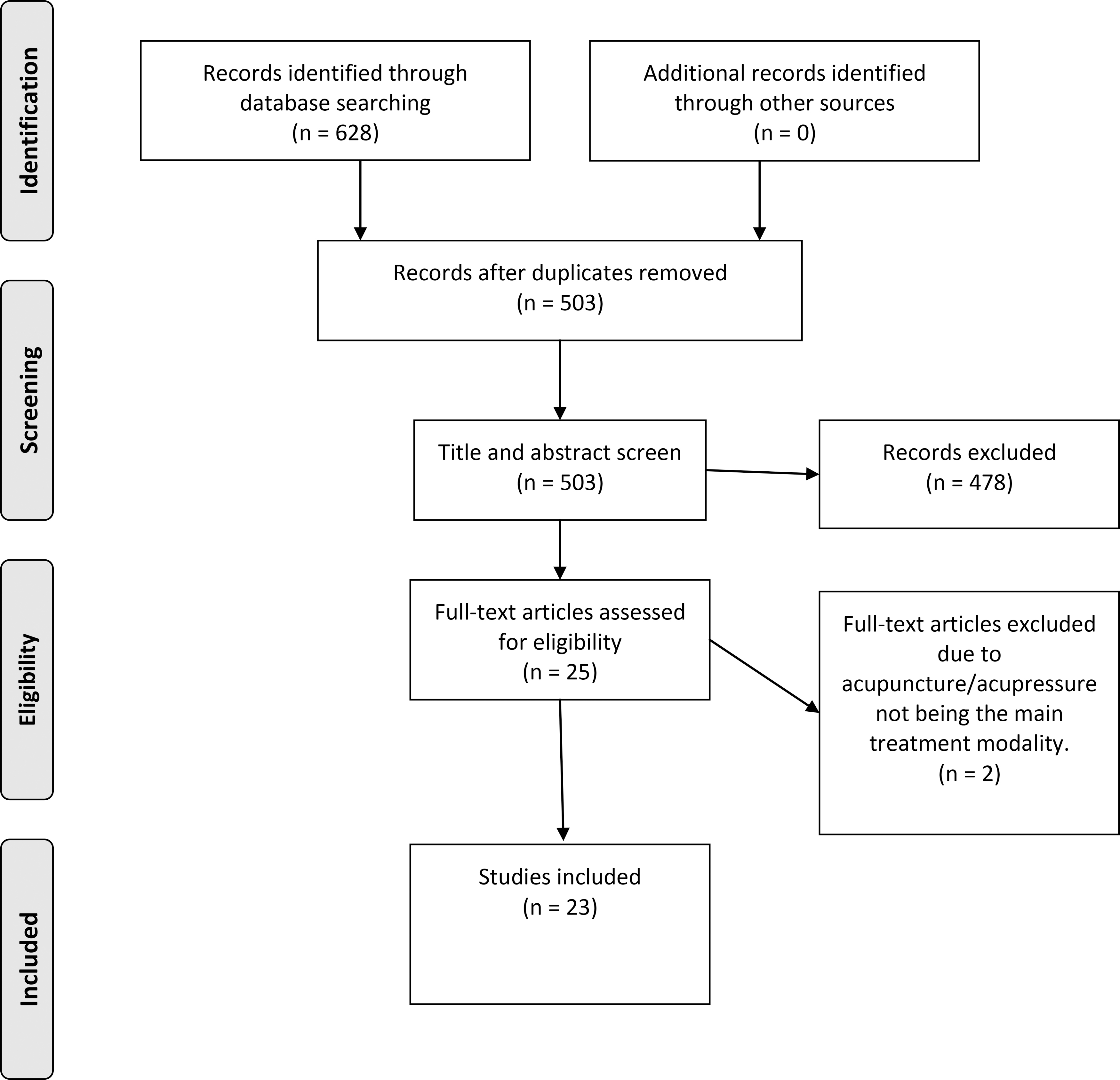
PRISMA flow diagram. From Moher D, Liberati A, Tetzlaff J, Altman DG; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med 2009;6:e1000097. For more information, visit
Data extraction, grading evidence levels, and risk of bias
Data extracted included study characteristics (author, year, study design), study population (size, age), condition treated, interventions (acupuncture and control), outcome measurements, and main results and conclusions.
Level of evidence was graded by using guidelines from the Oxford Center for Evidence-Based Medicine (OCEBM) tool with levels from I-V. Level I studies include systematic reviews of randomized controlled trials (RCTs) or n-of-1 trials. Level II studies include RCTs or observational studies with dramatic effect. Level III evidence is defined as nonrandomized controlled cohort/follow-up studies. Level IV includes case-series, case-control studies, or historically controlled studies, and level V evidence is mechanism-based reasoning. 9 The OCEBM tool instructs users to grade up or down a level depending on the specific studies' quality, imprecision, indirectness, consistency, and absolute effect size.
Risk of bias was assessed by using the Evidence Project risk-of-bias tool, which is a tool developed to assess risk of bias in reviews that include both randomized and nonrandomized trials. 10
Results
Twenty-three studies were identified in total, and results are summarized in Table 1. Dermatological conditions investigated were psoriasis (n = 2), atopic dermatitis (AD; n = 4), itch (n = 2), urticaria (n = 1), chronic idiopathic pruritus (n = 1), postoperative itch/pruritus (n = 2), uremic pruritus (n = 5), seborrheic alopecia (n = 1), acne (n = 1), hidradenitis suppurativa (n = 1), lichen simplex chronicus (n = 1), warts (n = 1), and melasma (n = 1). Acupuncture resulted in statistically significant improvements in outcome measures in 10 out of 14 of the completed studies found. Efficacy was determined by a combination of level of evidence and improvement in outcome measures. Eight studies had level II evidence, two had level III, three had level IV, and one had level V; no studies with level I evidence were found, and ongoing studies were not graded.
Results Table—Acupuncture in Dermatology
AD, atopic dermatitis; CES-D, Center for Epidemiologic Studies-Depression Scale; CRP, C-reactive protein; CU, chronic urticaria; DLQI, Dermatology Life Quality Index; EASI, Eczema Area Severity Index; EQ5D-3L, Euro quality of life 5D; ESR, erythrocytic sedimentation rate; HAMA, Hamilton Anxiety Scale; HAMD, Hamilton Depression Scale; ISS, Itch Severity Score; NA, not applicable; PASI, Psoriasis Area Severity Index; POEM, Patient Oriented Eczema Measure; PPT, pressure pain threshold; PSQI, Pittsburgh Sleep Quality Index; QoL, quality of life; RCT, randomized controlled trial; SA, sham acupuncture; SCORAD, Scoring Atopic Dermatitis Index; SF-12, General health related quality of life; STAXI, State-Trait Anger Expression Inventory; TCM, Traditional Chinese Medicine; TEAS, transcutaneous electrical acupoint stimulation; TEWL, trans-epidermal water loss; UAS, urticaria activity score; VA, verum acupuncture; VAS, Visual Analogue Scale.
Due to ongoing study with no published results.
Risk of bias is reported in Table 2; the Evidence Project tool does not give a summary score due to possible misleading effects and differences in the weight of each item. We explored the possibility of giving an interpretation of the overall estimated risk of bias for each study. However, the Evidence Project has not done so to date and does not provide guidelines for assigning these values. 10 Therefore, we only compared whether one trial had a “higher” or “lower” risk of bias than another and left overall interpretation up to the reader. Studies were ordered in the same order as the results table, and ongoing studies were not assessed.
Evidence Project Risk-of-Bias Tool Assessment
AD, atopic dermatitis; NA, not applicable.
Psoriasis
The only publication found for psoriasis was a case report of a 49-year-old woman treated with acupuncture for migraines with a noted concurrent improvement in her psoriasis. 11 However, a two-arm parallel, assessor-blinded, RCT that will assess 180 adult patients with psoriasis is currently ongoing. The study will evaluate the Psoriasis Area Severity Index), Visual Analogue Scale (VAS), and Dermatology Life Quality Index (DLQI). 12
Atopic dermatitis
A double-blinded, sham-controlled, randomized trial with three arms found a significant difference in Scoring Atopic Dermatitis Index (SCORAD), Eczema Area Severity Index (EASI), Patient Oriented Eczema Measure (POEM), and DLQI in the two verum acupuncture arms versus the sham acupuncture (SA) arm. However, no significant differences were observed in VAS pruritus or VAS itch scores between groups. 13 An observer-blinded, prospective, randomized, clinical pilot trial compared acupuncture with needle embedding treatment and found significant differences from baseline to study completion in SCORAD, trans-epidermal water loss, DLQI, and skin hydration but no significant differences between groups. 14 There are two ongoing RCTs for AD. One is a randomized, double-blind, sham-controlled trial of 36 mild-to-moderate AD adult patients and will evaluate SCORAD, EASI, quality of life (QoL), POEM, DLQI, and dyspepsia symptoms. 15 The other has three arms with 120 adult AD patients and will compare acupuncture with osteopathy and no treatment. It will assess VAS, DLQI, topical corticosteroid use, SCORAD, EASI, and general health-related QoL (SF-12). 16
Itch, pruritus, and urticaria
A randomized, uncontrolled pilot study on chronic itch found decreases in VAS, Itch Severity Score (ISS) compared with baseline; significance was not assessed, and there were no calculated p-values. In addition, objective signs of pruritus were absent at weeks 5 and 7. 17 Another study investigated histamine-induced itch and was a randomized, crossover, participant-blind trial that gave 20 healthy patients 1% histamine after acupuncture or placebo treatment. VAS was significantly decreased in the acupuncture arm versus placebo. The same study also assessed skin blood perfusion to measure itch subjectively and found significant decreases in the acupuncture arm versus placebo. 18
An uncontrolled nonrandomized pilot study of 10 adult patients with chronic idiopathic pruritus found that 7 of 10 patients reported relief and noted 1 patient with elevated ESR return to normal after treatment. Significance was not assessed, because no p-values were calculated. 19
For postoperative itch prevention, a patient-blinded RCT prophylactically gave acupuncture or shame acupuncture to 80 patients undergoing elective cesarean section who were administered spinal anesthesia. There was a nonsignificant trend to reduce itch in the acupuncture group and no reduction in the mean or median VAS score between groups. 20 A randomized, double-blind, placebo-controlled trial assessed morphine-induced pruritus on 30 adult patients scheduled for C-section under spinal anesthesia with intrathecal morphine. Acupuncture or SA was given prophylactically the day before the C-section and removed 48 h postoperatively. They found no significant difference in the incidence of postoperative pruritus. 21
Uremic pruritus
All five studies found were RCTs. All three completed studies found significantly decreased VAS in acupuncture compared with control in patients undergoing hemodialysis with uremic pruritus. The first study compared acupuncture with SA in 30 adult patients in a multicenter, patient-blinded RCT. 22 The second completed study is an RCT of 75 patients with three arms that compared acupressure, transcutaneous electrical acupoint stimulation, and normal clinical treatment of antihistamine tablets. In addition to a significantly decreased VAS in the acupressure group, this study also observed a significant decrease in antihistamine tablets used in the treatment groups versus control. 23 The last completed study is an assessor-blind RCT that compares auricular acupressure with Vaccaria seeds to a tape control in 71 patients. In addition to VAS, it also found a significantly greater decrease in serum histamine levels in the acupressure versus control group. 24 One ongoing RCT will be assessing acupressure, and the outcomes will be the Pittsburgh Sleep Quality Index, Euro QoL 5DEQ (5D-3L), and 5D itch scale. 25 The other will be assessing acupuncture with outcomes of VAS, mast cells per 40 × magnification, and QoL. 26
Other
A single-blinded RCT assessed 32 adult patients with lichen simplex chronicus and found significantly larger improvements in DLQI and significantly lower VAS scores in treatment versus placebo. 27 A participant-blinded RCT assessed 18 adult patients with a history of warts for 2 years of more with unsuccessful conventional treatment. Significantly more (36%) acupuncture-treated warts disappeared versus the placebo group (0%). 28 A randomized uncontrolled trial in 45 adult women with melasma observed a significant decrease in size and pigmentation in the acupuncture treated groups from baseline. 29 Three current ongoing RCTs will assess acupuncture in seborrheic alopecia, acne, and hidradenitis suppurative. 30 –32
Discussion
In this systematic review, we have updated on the previously done systematic review in 2015 by Ma and Sivamani. For patients with uremic pruritus, there is consistent level II evidence that acupuncture is an effective treatment modality for treating symptoms of pruritus, which may be due, in part, to decreased histamine levels, as seen in one of the studies. Although the interventions vary slightly in acupoints used, all three completed studies reported significant decreases in VAS score in the intervention group versus control. This supports the previous systematic review that found one RCT and one non-RCT in which acupuncture improved uremic pruritus. 8
AD has promising results that show it significantly decreases SCORAD and EASI but surprisingly had no significant difference in pruritus or itch VAS scores. However, sample sizes were small: One trial had 14 patients, and the other had 30 patients. Ma and Sivamani's review also observed small sample sizes with five studies involving 20 or fewer participants. 8 Psoriasis was not found in Ma et al.'s review, and our study only found one case report that is level V evidence. We eagerly await the results of the ongoing RCT of 180 patients, which would likely have a lower risk of bias and a higher level of evidence than the currently included case report.
Two level II evidence studies found that acupuncture was ineffective for prevention of itch in patients given spinal anesthesia for c-section. The 2015 review included one RCT by Jiang et al. that found a significant decrease in pruritus after spinal anesthesia when patients were given prophylactic acupuncture; however, the control in that study was a lack of intervention and not a placebo such as SA. 8 The studies in our review used SA or studs as their control groups, which resulted in lower risk of bias than the study included in Ma's 2015 review. In addition, Jiang et al.'s trial investigates patients undergoing transurethral prostatic resection whereas the trials in our review assess c-section patients. Therefore, we cannot draw general conclusions about prophylactic acupuncture usage for preventing itch in patients receiving spinal anesthesia, because outcomes may vary due to the different procedures the patients were undergoing. However, current evidence suggests that for c-section patients undergoing spinal anesthesia, acupuncture does not decrease the incidence of postoperative itch.
The role of acupuncture in treating itch has been assessed in several ways. The study using experimentally induced itch with histamine in healthy patients is promising but did not assess patients with disease. Acupuncture decreased VAS, ISS, and objective pruritus signs in one trial on chronic itch but was rated as level IV evidence. One study on chronic idiopathic pruritus was included: It had level IV evidence and found decreased “perceived itch” in patients. The lack of a control group and more objective measures of itch make it difficult to draw conclusions; in addition, the 2015 review did not find any studies on chronic idiopathic pruritus. 8 Conclusions about the use of acupuncture in itch and chronic idiopathic pruritus cannot be made.
Ma and Sivamani found two RCTs on chronic urticaria that showed acupuncture as effective in decreasing rate and duration of urticarial episodes and increasing clearance rate, which they rated as level II evidence. 8 Our review only found Shi et al.'s 33 ongoing RCT on chronic urticaria. Ma and Sivamani concluded that acupuncture improves outcome measures in chronic urticaria, and we are unable to include any significant updates to this knowledge.
Ma and Sivamani found one study in favor of acupuncture use in melasma and one against: Both were level I–II evidence, whereas our review only found one additional uncontrolled study of level IV evidence, which found decreases in melasma extent and pigmentation versus baseline. For acne, Ma and Sivamani did not find strong evidence for the use of acupuncture and our review only found one ongoing study with no results published. 8 No significant conclusions about acupuncture use in melasma or acne can be made.
Limitations to our study include only evaluating articles in English, so we could not assess the entire scope of articles found. The method of blinding used among the studies was highly variable. Some studies blinded participants only, assessors only, or did not blind at all. In addition, control groups had variable treatments with some using SA and others using creams or medications. Outcome measurements were also variable across studies, even when assessing for the same condition. This heterogeneity in studies made it difficult to uniformly assess and compare different studies and, consequently, prevented us from pooling findings in a valid form for meta-analysis. Although limiting inclusion criteria to only RCTs would be ideal, we ultimately decided against it due to our desire to replicate the 2015 systematic review inclusion criteria.
Conclusion
The increasing prevalence of acupuncture usage necessitates a better understanding of its potential uses in dermatology. We conclude that acupuncture may be effective in treating uremic pruritus and chronic urticaria but is not effective in preventing postoperative itch in patients receiving spinal anesthesia when undergoing elective c-section. Other promising conditions for treatment include AD and essential pruritus. Future studies should standardize placebo and blinding methods to control for bias, which could also lead to opportunities for meta-analysis. Additional large-scale RCTs are needed to assess acupuncture in dermatology to solidify efficacy as a valid treatment modality.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding of any sort was provided for this systematic review of the literature.