
Abstract
Introduction:
Medication nonadherence contributes to poor blood pressure control and increases cardiovascular disease risk in patients with hypertension. Identifying modifiable risk factors for low or nonadherence to antihypertensive medication is needed. Studies that have examined the relationship between herbal or dietary supplement (HDS) use and antihypertensive medication nonadherence provide inconsistent findings. Data from the National Health and Nutrition Examination Survey were used to examine the association between HDS use, current use of prescribed antihypertensive medication, and blood pressure status.
Methods:
The study sample included hypertensive adults (n = 5,478) who have been told by a health professional to take prescribed medication for their health condition. Respondents were classified as either HDS users or HDS nonusers. Depending on the kind of supplement used, HDS users were further divided into three mutually exclusive groups: hypertension HDS users, nonhypertension HDS users, and those who used both kinds of supplements. Supplements groupings were based on reports in the literature. Blood pressure status definition was based on Eighth Joint National Committee (JNC 8) recommendations. Adjusted odds ratios (aORs) and 95% confidence intervals (95% CIs) were obtained from logistic models.
Results:
Overall HDS use prevalence was 62%. Current medication use did not significantly differ between patients reporting no HDS use and those reporting HDS use (aOR: 1.45; 95% CI: 0.78–2.69). No observable differences were found in current medication use between patients reporting no HDS use and those taking nonhypertension HDS or both kinds of supplements. Use of hypertension HDS was associated with improved blood pressure (aOR: 1.90; 95% CI: 1.07–3.36) compared with no HDS use.
Conclusion:
In a nationally representative U.S. sample, HDS use did not compromise current use of prescribed medication and was associated with improved blood pressure control. More research is needed to better understand why HDS use is associated with better blood pressure control.
Introduction
More than 100 million Americans currently have hypertension. 1 Among U.S. adults taking antihypertensive medication, 53% have uncontrolled blood pressure. 2 About 3 million deaths from atherosclerotic cardiovascular disease could be averted over the next 10 years through the achievement and maintenance of blood pressure goals as recommended in the 2017 Hypertension Clinical Practice Guidelines. 3,4 Medication nonadherence contributes to poor blood pressure control and increases cardiovascular disease risk in patients with hypertension. 5,6 In a study using 2015 health insurance claims in combination with National Health Interview Survey, 7 only 31% of hypertensive adults were adherent to antihypertensive therapy. To design effective interventions to improve blood pressure control, it is important to identify modifiable risk factors for low adherence in this patient population.
Reasons for medication low adherence to medication in the hypertensive patient population are complex and multidimensional. 8 These include demographic, treatment, clinical, and behavioral factors such as use of herbal or dietary supplement (HDS) use. 9,10 Findings from studies examining the relationship between HDS use and antihypertensive medication nonadherence are inconsistent. There is some evidence to suggest that HDS use is positively associated with medication nonadherence in patients with hypertension, 9 but this finding has not been replicated in other studies. 11,12 The inconsistency may be a result of small sample sizes (range from 272 to 390) and differences in definitions of HDS use. 11,12
HDS use may be an important modifiable barrier or a signal of other barriers to antihypertensive medication adherence and subsequent blood pressure control in patients. For instance, patients may substitute HDSs for prescription medications due to costs of hypertensive medication. 9,13 Studies examining the association of HDS use, prescribed medication use, and subsequent blood pressure control in a nationally representative sample are needed.
For this report, a nationally representative sample was used to examine the association between dietary supplement use within the past 30 days and current use of prescribed antihypertensive medication. It was hypothesized that individuals reporting HDS use in the past 30 days would be less likely to report current use of prescribed antihypertensive medication. It was further hypothesized that HDS use would be associated with uncontrolled blood pressure.
Methods
Study design and objectives
This was a cross-sectional study designed to examine the association between HDS use and medication adherence among U.S. adults with hypertension who receive treatment for their condition. The association between HDS use and blood pressure control status was also evaluated. Publicly available deidentified data were used and, as such, did not require approval from the institutional review board.
Study setting and sample
Data from the National Health and Nutrition Examination Survey (NHANES) were used. NHANES uses a complex multistage sampling design to select a representative sample of the civilian noninstitutionalized population in the United States. 14,15 During the survey, data were collected in two ways: (1) through a medical examination in which participants' blood pressure readings, height, and weight are measured, and (2) using questionnaires to collect information on self-reported health status and dietary habits. 14 In this study, NHANES questionnaires and medical examination data collected between 2009 and 2014 were used.
Study participants
Individuals younger than 18 years old (n = 11,964) and pregnant women (n = 190) were excluded. Participants were asked a series of questions during the survey. First, they were asked whether they had ever been told by a doctor that they have hypertension or high blood pressure. Those who responded with a “yes” were subsequently asked whether they had been told to take prescribed medication because of their hypertension status. The following individuals were further excluded: (1) adults who had not been told (or did not know (n = 26) whether they had been told) by a doctor that they have hypertension (n = 11,919) and (2) those who had been told by a doctor that they have hypertension, but had not been told (or did not know [n = 5] whether they had been told) to take prescribed medication by their doctor (n = 886) (Fig. 1). The final analytic sample was n = 5,478 participants, weighted to correspond to 60,890,423 U.S. adults.
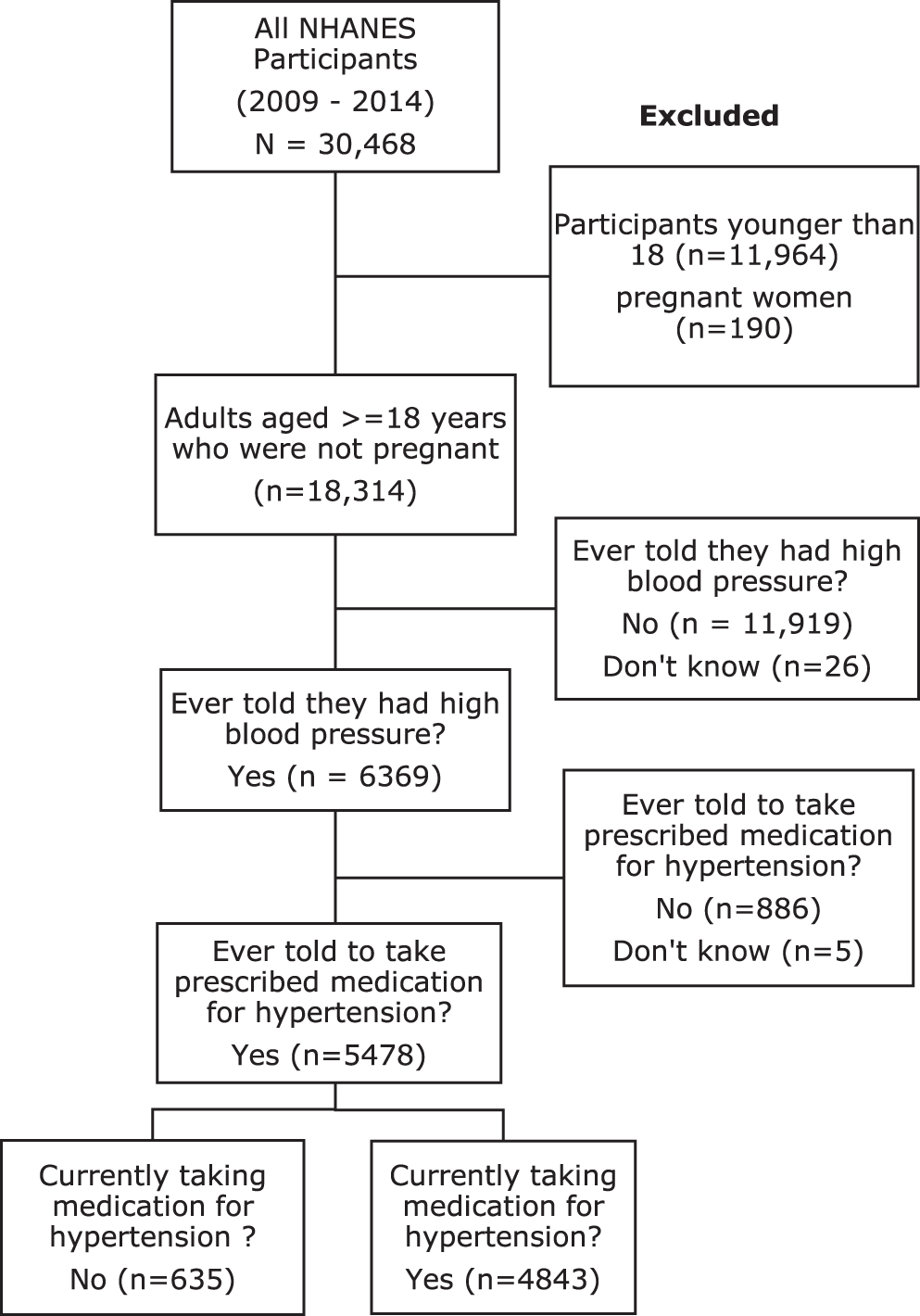
Flowchart of participants who responded to the National Health and Nutritional Examination Survey (NHANES) between 2009 and 2014 and were included in this study. Participants with missing data on herbal or dietary supplement use (n = 4) were excluded.
Herbal or Dietary Supplement Use (independent variable)
Herbal or Dietary Supplement use was measured using the interviewer-administered Dietary Supplement Questionnaire (DSQ). The DSQ is used to collect detailed information on participants' use of vitamins, minerals, herbals, and other supplements over the past 30 days. HDS use was evaluated using the question, “Have you used or taken any vitamins, minerals, or other dietary supplements in the past 30 days?” Participants who respond with a “no” were classified as HDS nonusers and those who respond with a “yes” as HDS users.
Depending on the type or kind of supplement used, HDS users were further divided into three mutually exclusive groups (Fig. 2). Participants reporting use of hypertension supplements were classified as hypertension HDS users. Nonhypertension HDS users were those who reported dietary supplement use but did not report use of any of the mentioned hypertension supplements. Participants who reported use of both hypertension HDS and nonhypertension HDS were placed into the third group. The three subgroups of HDS users were (1) hypertension HDS users, (2) nonhypertension HDS users, and (3) those who used both hypertension HDS and nonhypertension HDS. These groupings were based on supplements reported in the literature to improve hypertension, which include garlic, 16,17 vitamin D, 18 magnesium, 19,20 fish oil, 21 fiber, 22 green tea, 23 folic acid, potassium, lemon, flax seed, ginger, 24 melatonin, 25,26 and hawthorn. 27
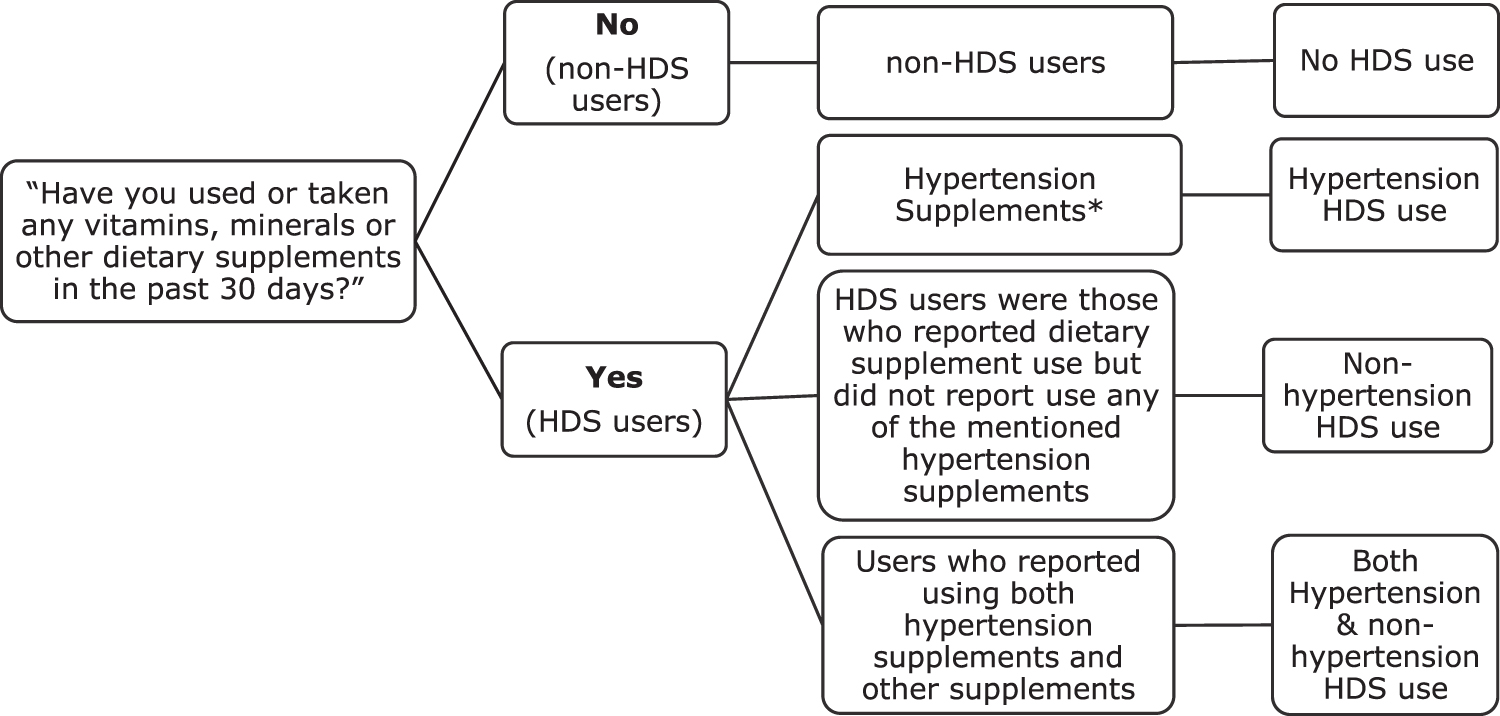
Operational definitions of herbal or dietary supplement use implemented in the study that used National Health and Nutritional Examination Survey (NHANES) 2009–2014. *Garlic, vitamin D, magnesium, fish oil, fiber, green tea, folic acid, potassium, lemon, flax seed, ginger, and hawthorn, nitric oxide, lemon, vinegar, hawthorn,
Current medication use (hypothesis 1 dependent variable)
Participants who reported receiving advice from the doctor to take medication for hypertension were asked whether they were currently taking the prescribed medication. Those who answered “yes” were classified as current medication users and those who answered “no” were classified in the current medication nonusers category.
Blood pressure status (hypothesis 2 dependent variable)
Blood pressure status was defined as either having controlled or uncontrolled hypertension. Based on the Eighth Joint National Committee (JNC 8) recommendations, 28 participants were classified as having controlled blood pressure if systolic blood pressure was <140 mm Hg or diastolic blood pressure was <90 mm Hg. The JNC 8 guidelines were used because data were collected between 2009 and 2014 when these guidelines were in effect. All 0 mm Hg readings were excluded in the present analyses.
Statistical analyses
The percentage distributions of socioeconomic demographics by HDS use are presented. Group differences in demographic factors between HDS users and nonusers (and type of supplement used) were assessed using chi-square test for categorical variables and t-test for continuous variables. Two separate logistic regression models were used to assess the association between HDS use in the past 30 days and current medication use, and the association between HDS use and blood pressure status. In the logistic model examining the association between dietary supplement use and current medication use, we adjusted for sex, race, education level, health insurance status, marital status, income, and systolic and diastolic blood pressure readings. In the logistic model examining the association between supplement use and blood pressure status, we adjusted for sex, race, education level, health insurance status, marital status, income, and current medication use. Odds ratios (ORs) and 95% confidence intervals (CIs) are presented. Additional analyses were performed to evaluate whether the observed associations in the multivariable logistic models varied when data were stratified by age, race, and gender. No substantial differences were found. In a sensitivity analysis, participants were classified as having controlled blood pressure if systolic blood pressure was <130 mm Hg or diastolic blood pressure was <80 mm Hg, based on the most recent 2017 guidelines for prevention and management of blood pressure in adults. 28 The sample data were weighted in the analysis to compensate for the sampling design and known biases that occur due to nonresponse. A more complete description of the sampling methodology can be found on the NHANES website. 15 All analyses were conducted using STATA version 15.
Results
Fifty-four percent of eligible survey respondents were women, with average age of 62 years (standard deviation [SD], 13.5 years). Most (88%) reported current use of prescribed hypertension medication, and 70% had controlled blood pressure. Overall, HDS use prevalence was 62%. HDS use prevalence was estimated at 60% (95% CI: 0.564–0.635) between 2009 and 2010, 61% (95% CI: 0.571–0.644) between 2011 and 2012, and 63% (0.600–0.676) between 2013 and 2014. The most used supplement was vitamin D (58%), followed by fish oil (19%) (Fig. 3).
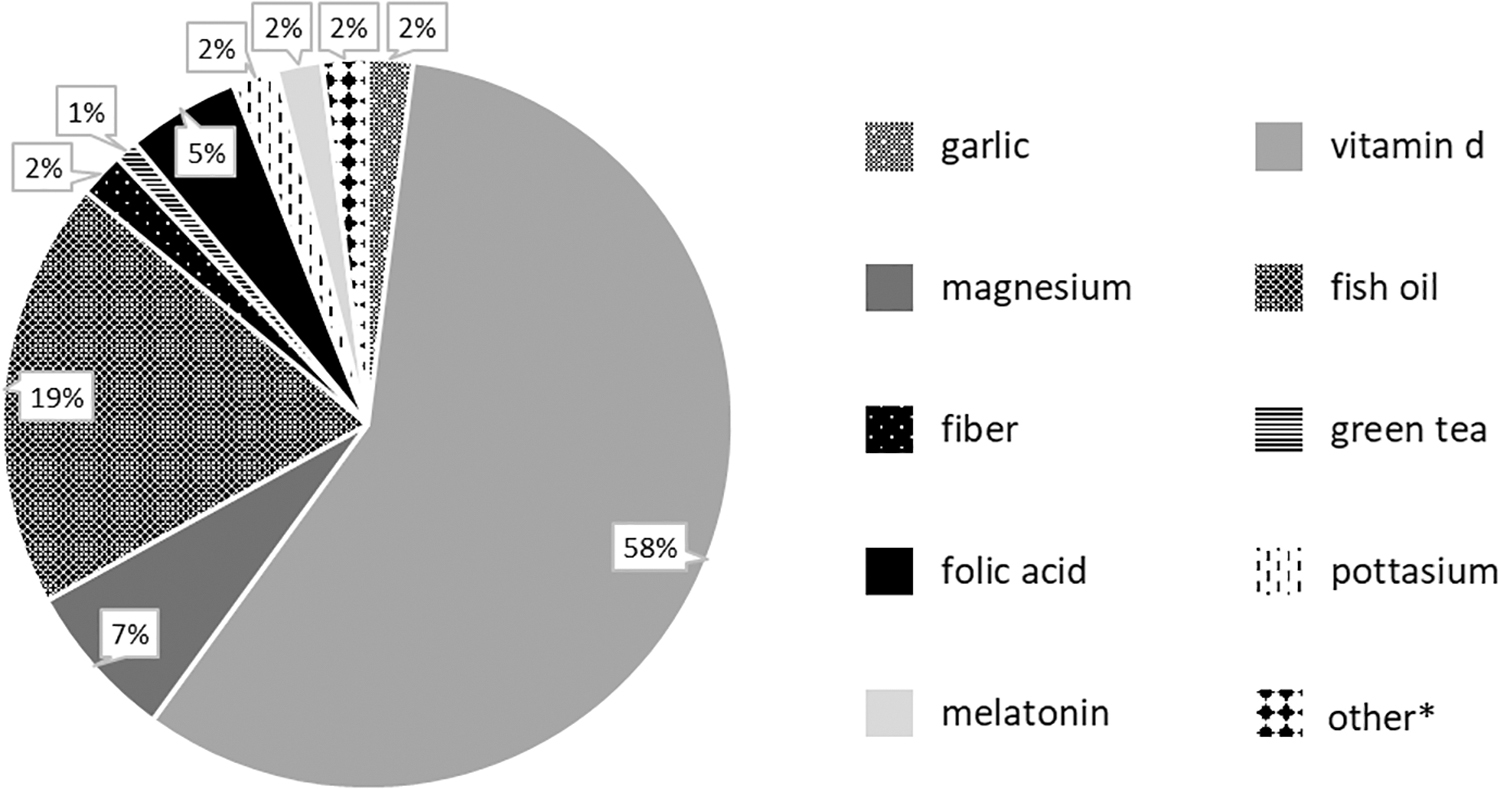
Percentage of U.S. adults with self-reported hypertension who used herbal or dietary supplements, National Health and Nutritional Examination Survey (NHANES) 2009–2014. *Other category includes: nitric oxide, lemon, vinegar, flax seed, ginger, hawthorn,
Table 1 shows sociodemographic factors by HDS use and type. Adults who reported any form of HDS use were older than nonusers (59.0 years (14.0) (p-value <0.05). Mean age of hypertensive adults who reported HDS use was 62.3 years (SD, 13.9) for nonhypertension HDS users, 66.2 years (SD, 11.5) for those who used both kinds of supplements, 64.9 years (SD, 12.3) for adults who used hypertension HDS, and 59 years (SD, 14.0) for nonusers. Women were more likely to report HDS use (52% used nonhypertension HDS, 64% used both, and 61% used hypertension HDS) than men (p-value <0.05). Non-Hispanic whites made up 43% of participants taking nonhypertension HDS, 53% of those taking both hypertension and nonhypertension HDS, and 39% of those taking hypertension HDS. Individuals taking nonhypertension HDS (31%) and those taking both hypertension and nonhypertension HDS (33%) were more likely to have some college level education or associate degree (p-value <0.05) compared with HDS nonusers (24%). Regardless of type of supplement used, average systolic blood pressure was 133 mm Hg. HDS nonusers had a slightly higher average diastolic blood pressure reading than users.
Patient Characteristics by Herbal or Dietary Supplements Use Among U.S. Adults (18 Years and Older) with Self-Reported Hypertension, NHANES 2009–2014
p-value <0.05.
GED, General Educational Diploma; HDS, herbal or dietary supplement; NHANES, National Health and Nutrition Examination Survey; SD, standard deviation.
Table 2 gives crude and adjusted associations between dietary supplement use and current medication use. Individuals taking hypertension HDS were more likely to report current medication use (aOR: 1.45; 95% CI: 0.78–2.69) than those reporting no current medication use. There were no observable differences in current medication use between HDS nonusers and nonhypertension HDS users (aOR: 1.04; 95% CI: 0.76–1.42), or users of both hypertension HDS and nonhypertension HDS (aOR: 1.00; 95% CI: 0.69–1.45). Similar patterns of associations were found when we stratified by age and gender, but reverse patterns of associations emerged when we stratified by race. Among non-Hispanic whites, the adjusted odds of current medication use were 1.93 for those taking hypertension HDS (95% CI: 0.67–5.59), 1.08 for those taking both kinds of supplements (95% CI: 0.66–1.79), and 1.14 for those using nonhypertension HDS (95% CI: 0.75–1.75). For individuals who self-identified as non-Hispanic black, Mexican American, other Hispanic, and other race, the odds of current medication use were 0.93 for those taking hypertension HDS (95% CI: 0.54–1.64), 0.88 for those taking both kinds of supplements (95% CI: 0.58–1.33), and 0.86 for those using nonhypertension HDS (95% CI: 0.59–1.25).
Association Between Herbal or Dietary Supplements Use and Current Medication Use Among U.S. Adults (18 Years and Older) with Self-Reported Hypertension and Recommended by Provider to Take Medication, NHANES 2009–2014
Weighted percentage currently taking medication as prescribed by the doctor.
Adjusted for age, sex, race, education level, health insurance status, marital status, income, and systolic and diastolic blood pressure readings.
CI, confidence interval; HDS, herbal or dietary supplement; OR, odds ratio.
Table 3 gives crude and adjusted associations between dietary supplement use and blood pressure status. Individuals taking hypertension HDS were more likely to have controlled blood pressure (aOR: 1.90; 95% CI: 1.07–3.36) than those reporting no HDS use. Stratified analysis by age, race, and gender revealed similar patterns in the association between HDS use and controlled blood pressure. Similar patterns between blood pressure status and hypertension HDS use were observed when blood pressure definitions (<130/80 mm Hg) were based on the 2017 guidelines; however, the association was no longer significant (aOR: 1.06; 95% CI: 0.71–1.58) (Supplementary Table S1).
Association Between Herbal or Dietary Supplements Use and Blood Pressure Control Status Among U.S. Adults (18 Years and Older) with Self-Reported Hypertension and Recommended by Provider to Take Medication, NHANES 2009–2014
Weighted percentages of individuals with controlled blood pressure control status.
Adjusted for age, sex, race, education level, health insurance status, marital status, income, and current medication use.
CI, confidence interval; HDS, herbal or dietary supplement; OR, odds ratio.
Discussion
We assessed the associations between HDS use, current prescribed medication use, and blood pressure status. Prevalence of HDS use among U.S. hypertensive adults increased from 60% in 2009 to 63% in 2014. The most used dietary supplement type was vitamin D. We observed differences between HDS users (including type of supplement used) and non-users. We initially hypothesized that individuals taking HDS would be less likely to report current medication use; however, these findings did not support this hypothesis. Instead, patients who reported HDS use were no less likely to report current medication use when compared with patients who did not report HDS use. In contrast, we found a significant association between HDS use and blood pressure control was which remained after multivariable adjustment. In the paragraphs below, these findings are placed in the context of prior literature and potential explanations for the results are explored.
There has been a notable increase in vitamin D supplement use since 1999, 29 which was consequent to the growing body of research evaluating the potential benefits of vitamin D on several health outcomes. 30,31 This may explain why vitamin D is prevalent in this patient group. Consistent with prior reports, 32 –35 we found that a high proportion of older adults, women, non-Hispanic whites, and those with some college education reported HDS use. It was also found that users were more likely to have some college education, be married, have health insurance, and less likely to be cigarette smokers. Furthermore, HDS users had significantly lower average diastolic blood pressure readings than nonusers with diastolic blood pressure average being lowest among hypertension HDS users. These findings are consistent with prior national U.S. reports that indicate that supplement users report good health, have health insurance, and avoid cigarette smoking compared with nonusers. 29
Prior reports of the association between HDS use and current medication use are mixed. 10 –12 These findings are consistent with a prior study that reported no association between HDS use and medication adherence. 12 After adjustment, the OR reduced from 2.66 to 1.45 for hypertension HDS use and the CI overlapped 1.0 (not significant). This suggests that the positive association seen in the unadjusted model may have been confounded by covariates. Current study findings suggest that herbal use may be a marker for an underlying desire to be well or may reflect a more complex pathway between HDS use and current medication use mediated by side effects from prescribed medication, which was unable to be explored in this data set. Nevertheless, concurrent use of HDS and antihypertensive medications may result in drug–supplement interactions. A few drug–supplement interactions have been reported in the literature, 36,37 but many are still unknown. Health care providers should be aware of and be able to discuss issues related to HDS use to improve patients' understanding of issues involving safety and efficacy. It will be beneficial for health care professionals to seek out information about HDS use from their patients.
Stratified analysis showed that herbal and dietary supplement use was positively associated with medication use in non-Hispanic whites, and negatively associated with medication use in other racial groups. These findings are similar to those reported by Krousell-Wood et al. who found a negative association between complementary medicine use and antihypertensive medication adherence in African American or black, but not in non-Hispanic white patients. 9 A Possible explanation for this finding could be differences in reasons for HDS use among patients. Patients groups that report use of HDS as a means to reduce medication expenses 38 may be more likely to be noncompliant with prescribed medications. Further research is needed to identify reasons for use of HDS and their influence on medication compliance among hypertensive patients.
Patients who had used hypertension HDS in the past 30 days tended to have controlled blood pressure. Systematic reviews provide no conclusive evidence on the clinical benefits of dietary supplements (potassium, 39 vitamin D 40 ) use on blood pressure control, but HDS use remains highly prevalent among hypertensive patient populations. 41 The observed association may be a result of HDS users engaging in healthy behaviors to improve their health condition. HDS use may be a marker of positive self-care and is shown to be associated with dietary adherence in hypertensive patients. 11 It is important to acknowledge the self-care behavior of hypertensive patients, to assess potential harm, and encourage effective methods of self-care.
This study had limitations. This was a cross-sectional study, thus the temporal relationship between dietary supplement use, medication use, and blood pressure was not assessed. Measures used to assess current use of antihypertensive medication are not a valid measure of medication adherence. Use of valid measures such as the Morisky scale 42 may provide a better conclusion for the influence of HDS use on appropriate medication use. Given the limited knowledge of HDS use in the literature, the list of hypertension supplements provided in this study is not comprehensive. For instance, we did not have data on use of linolenic acid in this sample, which has been shown to lower systolic blood pressure readings. 42 Also, we may have grouped a wide range of HDS products together that may have varying effects on hypertension outcomes.
Conclusion
In a nationally representative U.S. sample, HDS use did not compromise current use of prescribed medication and was associated with better blood pressure control. However, we were unable to assess whether the observed association was a result from patients' engagement (who report HDS user) in health behaviors such as dietary adherence or whether HDS use actually does improve blood pressure. More research is needed to understand why HDS is associated with better blood pressure control.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
Supplementary Material
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.