
Abstract
Objective:
To compare the effect of dextrose prolotherapy (DPT) with saline in the treatment of chronic lateral epicondylopathy (LE).
Design:
Triple-blinded randomized controlled trial.
Setting:
Physical medicine and rehabilitation outpatient clinic.
Subjects:
Sixty cases of chronic LE participants were included in the study.
Methods:
Participants were randomly divided into two groups as DPT and normal saline. Saline or hypertonic dextrose (15%) was injected at the baseline, and at the end of the 4th and 8th week. Assessments were performed at baseline, and at the end of the 4th, 8th, and 12th week.
Outcome measures:
Primary outcome measures were Visual Analog Scale (VAS) for pain, Patient Rated Tennis Elbow Evaluation (PRTEE-Total [PRTEE-T], PRTEE-Pain, PRTEE-Function); secondary outcome measures were Disabilities of the Arm, Shoulder, and Hand Score (DASH) and pain-free handgrip strength.
Results:
Intragroup analysis demonstrated that both groups significantly improved in VAS, PRTEE, DASH scores, and handgrip strength during the study period (p < 0.001, for all outcome measurements in both groups). Intergroup analysis showed that PRTEE-T score changes between baseline-4th and -12th week; VASrest change between baseline and 4th week in the DPT group were significantly higher than the saline group (p = 0.041, p = 0.038, p = 0.013 respectively). There was no significant difference between groups in VAS, DASH scores, and handgrip strength between any time points, in terms of improvement (p > 0.05).
Conclusion:
Our study results showed that DPT outperformed saline in PRTEE-T score. Although saline seems to be a comparable clinical effect with DPT, further studies comparing the effects of saline injection and DPT are necessary, in chronic LE.
Introduction
Lateral epicondylopathy (LE) is a painful enthesopathy of the common extensor tendon at the fibro-osseous junction. 1 Degenerative changes and microtears of extensor tendons origin have more responsibility than local inflammation for the development of LE. 2
The treatment of LE includes nonoperative and operative procedures. Nonoperative procedures consist of conservative and interventional treatment methods. Conservative treatment of LE includes: wait-and-see, rest, analgesics, splints, exercises, and physical therapy. 3 The most preferred interventional procedures are: corticosteroid injection, prolotherapy, botulinum toxin, platelet-rich plasma, autologous blood injection, and stem cells; the latter three are included in biologic treatment options 2,4 As supported histopathologically, instead of inflammation suppression, treatment strategies based on biological stimulation of tendon repair, preventing the apoptotic process and increasing the synthesis of the extracellular matrix, might be rationale options for chronic LE. 5,6
Prolotherapy is an injection technique that causes iatrogenic inflammation by using osmotics/irritants or chemotactic (sodium morrhuate, phenol). 3 Although it works similar to biologic injection procedures, it is cost-effective and easy to access. This treatment includes multiple injections of the solution to the tendon–ligament attachments. 7 Hypertonic dextrose is the most preferred solution. Although there has been some evidence for the beneficial effects of dextrose prolotherapy (DPT) in the treatment of LE, the limited number of studies comparing the effectiveness of DPT and saline led us to design the relevant study. 8
In this study, we aimed at comparing the effects of DPT versus saline injection in cases with chronic LE. We hypothesized that both saline injection and DPT will result in a clinically important improvement in chronic LE, although DPT will outperform saline.
Materials and Methods
We designed this study as a prospective, randomized, triple-blinded study with a 12-week follow-up. The study was approved by the local Ethics Committee (15/03/2017-8) and Health Ministry Alternative and Complementary Medicine Department. The study was conducted according to the Declaration of Helsinki (14/11/2017-77979112). Each patient gave written informed consent before the enrollment.
Subjects
Chronic LE patients aged between 18 and 65 with pain at the lateral side of the elbow lasting minimum 3 months, despite the treatment methods [Non-steroidal antiinflammatory drugs (NSAID), splint, corticosteroid injection, physical therapy], were included in the study. The LE diagnosis was based on pain on resisted extension of the wrist or middle finger test and local tenderness at the lateral epicondyle. Participants were needed to score their pain minimum of 4/10 Visual Analog Scale (VAS). Direct x-rays of the elbow were obtained to rule out osseous pathologies. Exclusion criteria were: corticosteroid injection within 6 months, radial nerve compression, pregnancy/breastfeeding, and trauma history within the past 3 months; thrombocytopenia, coagulopathy, bleeding diathesis; diffuse pain syndrome, history of DPT, and inflammatory arthritis; and fear of needles.
Randomization and blindness of patients and the investigators
A table of random numbers was used to allocate the patient to the saline or DPT group. The numbers 0.0 to 0.49 were enrolled in the DPT group, and the numbers 0.50 to 0.99 were assigned to the saline group. The allocation was performed by an author who neither interacted nor was aware of any of the patients.
Only the investigator who prepared the solutions had information about which group the patients were included in. The physician who did not communicate with the patients about their symptoms and functions administered the injections. The two investigators performed the injection procedure, and the assessment task of the investigators was kept constant during the study. The patients were also blinded to group allocation throughout the trial.
Injection procedure
All subjects received one of the study medications according to the randomization group: (1) DPT (15% Dextrose), (2) Saline (0.9% NaCl). Injections were performed at baseline, at the end of the 4th, and 8th weeks, in both groups with the same technique.
Fifteen percent dextrose was obtained with a combination of 3 cc 50% dextrose and 7 cc saline in sterile conditions. As local anesthetic has not been an integral part of the effectiveness of DPT, we did not include it in the solution. In both groups, a 2.5 mL syringe was filled with 1.5 cc solution. A 22-gauge, 1.5-inch needle was used for all injections. Solutions were identical in appearance and viscosity, so masking of numbered bottles was not needed. The patients' arm was positioned with elbow flexion and forearm pronation. The lead author injected solution at the lateral epicondyle, annular ligament, and supracondylar ridge, in sterile conditions. 8 A total of 1.5 mL of solution was administered at each primary injection site deeply, by touching the needle to the bone. We did not use the peppering technique. The subjects were monitored for 30 min. Patients were advised to undertake normal activities on condition avoiding the activities that may aggravate symptoms. Anti-inflammatory medications were discontinued during the study. They were allowed to take oral paracetamol for postinjection pain. A home-based exercise program was given to subjects 4 weeks after the first injection, including eccentric forearm and dorsiflexion exercise.
Visual Analog Scale
Pain intensity was assessed by 0–10 cm VAS, indicating pain at rest and motion during the past week. The reliability and validity of VAS were described. 9 At least a 2 cm improvement in VAS score was considered for a minimum clinically important difference (MCID). 10,11
Patient Rated Tennis Elbow Evaluation
Patient Rated Tennis Elbow Evaluation (PRTEE) is a disease-specific, self-reported questionnaire consisting of five pain, 10 functional disability items on 11-point numerical rating scales. PRTEE-Pain (PRTEE-P), PRTEE-Function (PRTEE-F), and PRTEE-Total (PRTEE-T) scores were recorded. PRTEE is a reliable, reproducible, and sensitive assessment scale for determining pain severity; disability resulted from chronic LE. 12 The validity and reliability of Turkish version have been previously demonstrated. 13 A decrease of PRTEE score on a minimum of 11 points or %37 is considered MCID. 14
Disabilities of the Arm, Shoulder, and Hand
The Disabilities of the Arm, Shoulder, and Hand (DASH) is a self-administered questionnaire measuring symptoms and functionality in subjects with upper extremity disorders, containing 30-item questions with five response options for each of them, with a total score ranging from 0 to 100. 15 The validity and reliability of the Turkish version have been previously demonstrated. 16 A decrease in 12.7 or more points is considered to demonstrate MCID. 17
Pain-free handgrip strength
Loss of grip strength is one of the most important symptoms that affects daily activities. 18 Pain-free grip strength is a sensitive measurement in patients with LE. 19 The average of three trials was recorded for grip strength.
Sample size estimation
One of the primary outcome measurements of this study was to compare the improvement in PRTEE-T score among groups. We designed a preliminary study to calculate the sample size, including seven patients in each group. When the effect size of Cohen's d was considered as 0.94, a total sample size of at least 44 (22 for DPT, 22 for controls, and allocation ratio was considered as 1:1) was required to achieve a power of 85% at the 5% significance level. It was decided to include 30 cases for each group considering a drop-out rate of 30%. An effect size of 0.94 was taken from our pilot study. Sample size estimation was performed by using G*Power (Franz Faul, Universität Kiel, Kiel, Germany) version 3.0.10.
Statistical analysis
Data analysis was performed by using IBM SPSS Statistics version 17.0 software (IBM Corporation, Armonk, NY). The distribution of continuous variables was determined by the Shapiro-Wilk test. Continuous variables were expressed as mean ± SD or median (Q1–Q3) according to the distribution of normality, whereas categorical variables were presented as the number and percentage. Baseline demographic and clinical continuous variables were compared by the Student's t test or Mann-Whitney U test, which was appropriate. In the comparison of categorical variables, the chi-square test was used (to compare the binary categorical variables, the continuity-corrected chi-square test was used when one or more of the cells had an expected frequency of 5–25; otherwise, the Fisher's exact test was used when one or more of the cells had an expected frequency of 5 or less). Since the mixed analysis of variance assumptions were not met, the effects of interventions on outcome measures (pain intensity, PRTEE, DASH, and pain-free handgrip strength) over time were analyzed by the Friedman's test (for within-group comparison) and Mann-Whitney U test (for between-group comparison). When the p-value from the Friedman test was statistically significant, pairwise comparisons with the Bonferroni correction were performed to know where the differences lie within a group. All the p-values <0.05 were considered as statistically significant.
Results
Of the 60 participants included in the study, 10 patients (7 in the DPT group and 3 in the saline group) dropped out. A flow-chart of the study is demonstrated in Figure 1.
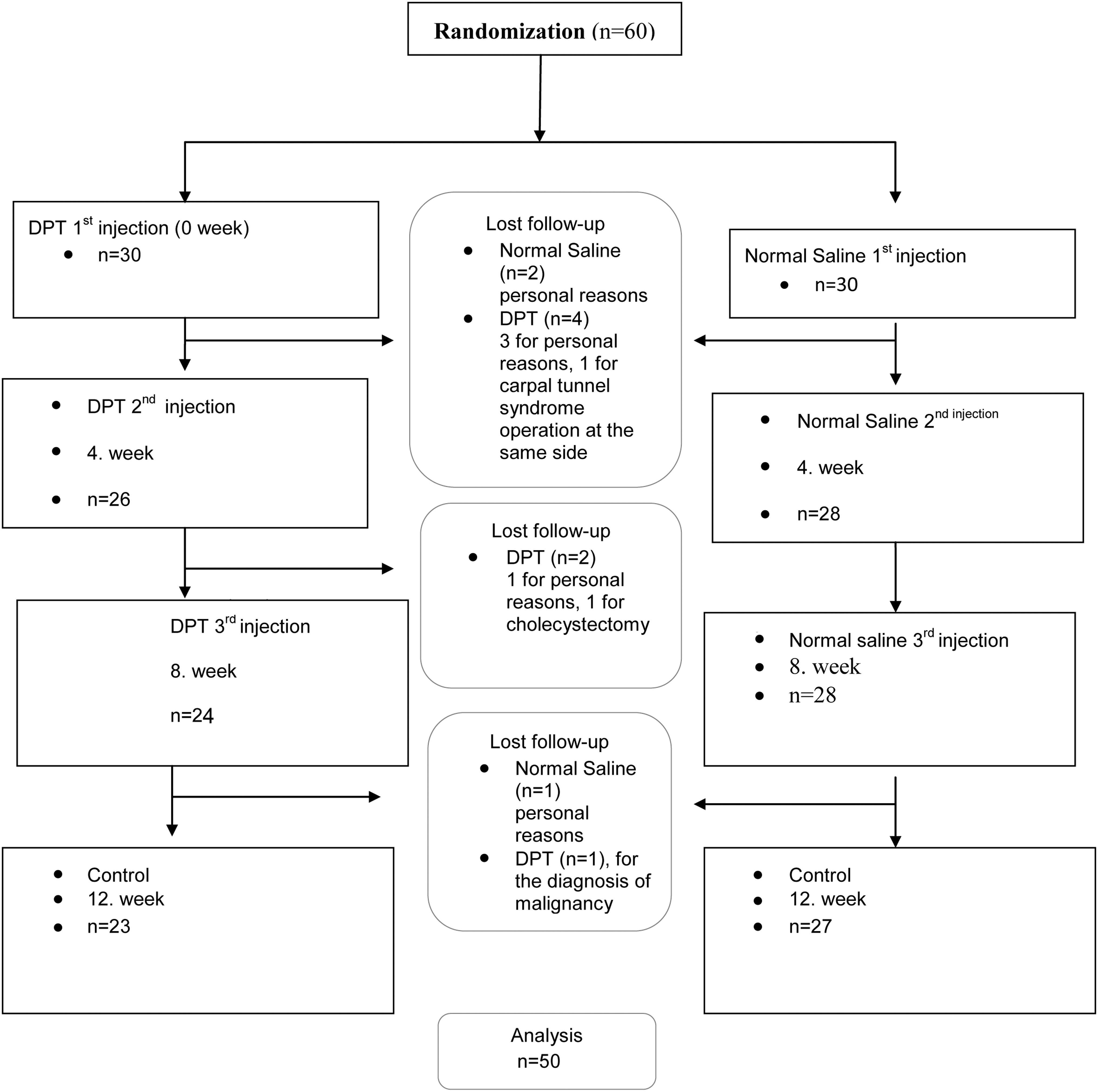
Flowchart of the study population. DPT, dextrose prolotherapy.
Baseline demographic and clinical characteristics are summarized in Table 1. There was no significant difference between groups in terms of baseline clinical and demographic characteristics.
Demographic and Clinical Characteristics of Participants by Dextrose Prolotherapy and Saline Groups
DPT, dextrose prolotherapy.
There was no significant difference in terms of VASrest, VASmotion, handgrip strength, and DASH between groups at baseline (p = 0.462, p = 0.599, p = 0.233, p = 0.483, respectively). The baseline values of VASrest, VASmotion, DASH, and handgrip strength for saline and DPT groups are shown in Table 2.
Intragroup Comparisons of Dextrose Prolotherapy and Saline Injection on VASrest, VASmotion, Pain-Free Handgrip Strength, and Disabilities of the Arm, Shoulder, and Hand Score Between All Time Points
Bold indicates significance at p < 0.05.
The data are shown in median (Q1–Q3) format.
According to the Friedman test.
Pairwise comparisons: p-value is adjusted according to the Bonferroni method.
The difference between week 0 and 12 is statistically significant (adjusted p < 0.05).
The difference between week 0 and 8 is statistically significant (adjusted p < 0.05).
The difference between week 0 and 4 is statistically significant (adjusted p < 0.05).
The difference between week 4 and 12 is statistically significant (adjusted p < 0.05).
The difference between week 4 and 8 is statistically significant (adjusted p < 0.05).
DASH, Disabilities of the Arm, Shoulder, and Hand Score; DPT, dextrose prolotherapy; VAS; Visual Analog Scale.
PRTEE-P was significantly higher in the DPT group than the saline group, at baseline (p = 0.027). Therefore, intergroup comparisons of variables were carried out over changes, not at individual time points. There was no significant difference among groups at baseline levels of PRTEE-F and PRTEE-T (p = 0.483, p = 0.176, respectively) (p > 0.0083). Baseline values of PRTEE-P, PRTEE-F, and PRTEE-T for saline and DPT groups are shown in Table 3.
Intragroup Comparisons of Dextrose Prolotherapy and Saline İnjection on Patient Rated Tennis Elbow Evaluation Values Between All Time Points
Bold indicates significance at p < 0.05.
The data are shown in median (Q1–Q3) format.
According to the Friedman test.
Pairwise comparisons: p-value is adjusted according to the Bonferroni method.
The difference between week 0 and 12 is statistically significant (adjusted p < 0.05).
The difference between week 0 and 8 is statistically significant (adjusted p < 0.05).
The difference between week 0 and 4 is statistically significant (adjusted p < 0.05).
The difference between week 4 and 12 is statistically significant (adjusted p < 0.05).
The difference between week 4 and 8 is statistically significant (adjusted p < 0.05).
DPT, dextrose prolotherapy; PRTEE, Patient Rated Tennis Elbow Evaluation.
Both saline and DPT groups showed significant improvement in all outcome measures between baseline and 12th week assessment. The intragroup improvements in terms of pain severity, handgrip strength, and DASH in saline and DPT groups between each time point are detailed in Table 2. Both groups showed significant improvement in PRTEE-P, PRTEE-F, and PRTEE-T scores between baseline and 12th week assessment. The improvement of PRTEE-T and its subgroups between each time point is detailed in Table 3.
The improvements between the assessment intervals for VASrest, VASmotion, handgrip strength, DASH, and PRTEE-T over time are shown in Figures 2 –6, respectively.

VASrest improvement by groups over time. (Values represent the median, and the error bars represent the Q1 and Q3). DPT, dextrose prolotherapy; VAS, Visual Analog Scale.

VASmotion improvement by groups over time. (Values represent the median, and the error bars represent the Q1 and Q3). DPT, dextrose prolotherapy; VAS, Visual Analog Scale.

Pain-free handgrip strength measures by groups over time. (Values represent the median, and the error bars represent the Q1 and Q3). DPT, dextrose prolotherapy.

DASH scores by groups over time. (Values represent the median, and the error bars represent the Q1 and Q3). DASH, Disabilities of the Arm, Shoulder, and Hand; DPT, dextrose prolotherapy.
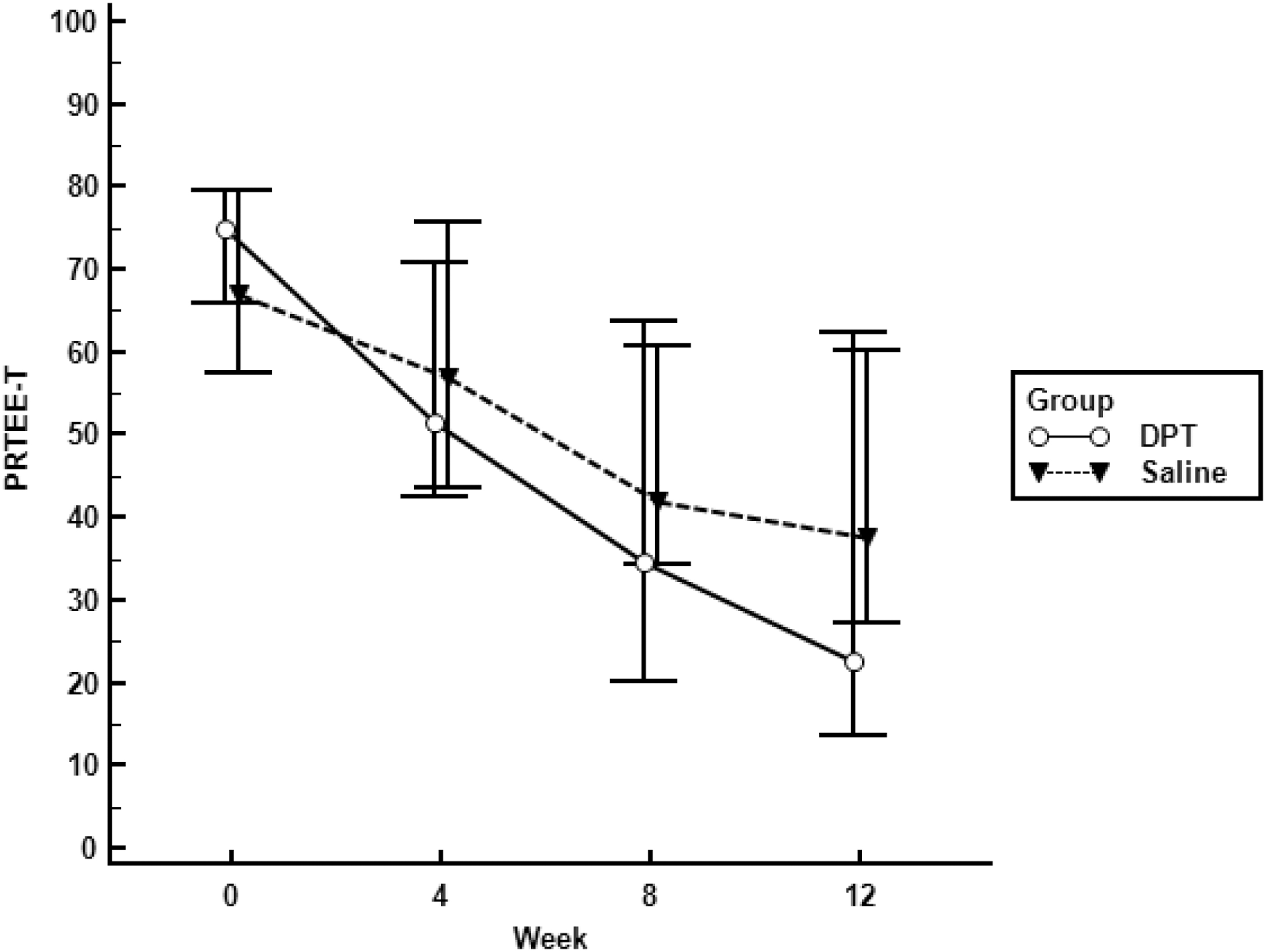
PRTEE-Total scores by groups over time. (Values represent the median, and the error bars represent the Q1 and Q3). DPT, dextrose prolotherapy; PRTEE, Patient Rated Tennis Elbow Evaluation.
The intergroup analysis of the change scores for clinical variables between assessment time points is shown in Table 4. The improvement of VASrest was found to be significantly higher in the DPT group than the saline group, between baseline and 4th week (p = 0.013). PRTEE-T score improvement in the DPT group was significantly higher than the saline group between baseline and 4th and 12th week (p = 0.041, p = 0.038, respectively). There were no significant differences between groups in terms of score change amounts, in terms of VASrest, VASmotion, handgrip strength, and DASH scores (p > 0.05).
Intergroup Changes in Clinical Measurements at 4, 8, and 12 Weeks of Follow-up Based on the Baseline
Bold indicates significance at p < 0.05.
The data are shown in median (Q1–Q3) format.
Actual differences were calculated by using tx − t0 formula.
DASH, Disabilities of the Arm, Shoulder, and Hand Score; DPT, dextrose prolotherapy; PRTEE, Patient Rated Tennis Elbow Evaluation; VAS, Visual Analog Scale.
A significant rate of both groups achieved MCID for all outcome measurements at the end of 12 weeks. Overall, 77.8% and 81.5% of the saline group, 87% and 91.3% of the DPT group achieved MCID in terms of VASrest and VASmotion, respectively. In PRTEE, 74.1% of saline and 78.3% of the DPT group achieved MCID; 66.7% of the saline group and 73.9% of the DPT group achieved MCID in terms of DASH. There was no significant difference among groups in terms of MCID achievement (p > 0.05 for VASrest, VASmotion, PRTEE, and DASH).
Discussion
We aimed at comparing the effect of DPT with saline injection in chronic LE. The results of this randomized controlled trial (RCT) indicated that both DPT and saline injection improve pain, functionality, and handgrip strength. Improvement in VASrest, VASmotion, handgrip strength, DASH, and PRTEE scores seemed to be favored in the DPT group in figures. Intergroup analysis showed that PRTEE-T score change was significantly higher in the DPT group whereas none of the other variables was statistically significant.
For the management of the patients with LE, interventional treatment strategies should be considered for the patients resistant to the other conservative treatment options. In our study, we included the patients who had been symptomatic for at least 3 months and the other treatment options had failed.
The exact mechanism of DPT is not completely clarified. It has been suggested that DPT promotes the release of growth factors, stimulation of fibroblasts, angiogenesis, and dense collagen deposition and causes cellular lysis. 20,21 Animal studies revealed that hypertonic dextrose stimulates the healing process of chronic injuries of intra/extra-articular tissues by triggering the inflammation to increase the connective tissue regeneration. 20 –23 In spite of the traditional mechanism, there has been histopathological evidence that showed that DPT (with 10% concentration) increases tendon thickness and irregularity of subsynovial connective tissue, neovascularization, and chondrogenesis without evidence of inflammation. 24 –26 Dextrose in 5% concentration was shown to be effective by inhibiting capsaicin receptor activation, substance-P, and calcitonin gene-related peptide. 27,28 Different concentrations of dextrose (10%, 20%, 30%) and saline were all found to be effective for reducing pain and functionality in temporomandibular dysfunction. 29
In patients with LE, handgrip strength is reduced. 21 Rabago et al. reported that the DPT group showed significant improvement in handgrip strength than morrhuate and wait-and-see groups. Both groups revealed significant improvement in PRTEE scores as well as handgrip strength. 30 Scarpone et al. compared saline and prolotherapy for LE. 8 They reported that both groups showed improvement but the prolotherapy group resulted in more improvement of pain severity and handgrip strength than the saline group. But they did not use functional outcome measurements and the sample size was too small. 8 In our study, we assessed disability with two functional outcome scales, in addition to pain severity and handgrip strength. Some former studies did not find any superiority of DPT to corticosteroid injection, physiotherapy, and combined treatment. 31,32 Our study indicated that the DPT group showed a significantly higher PRTEE-T score change over the saline group, whereas the other outcome measures did not. Although VASrest change was found more in the DPT group than the saline group between 0 and 4 weeks, it may not be correct to comment on this early result. Based on the median values, it is perceived that there is almost twice the difference between the groups in terms of PRTEE and DASH change between groups. However, if the graphics is examined in detail, it is understood that the data distribution ranges are wide, which may impact the statistical analysis results.
Saline has been used for the control group in many studies. Saline injection with the same technique may have a therapeutic effect by stimulating micro-bleeding, cell membrane rupture in LE treatment. 20 In two meta-analyses, 20 studies that evaluated saline injection for LE were analyzed. 33,34 Only one of the studies included in the meta-analyses compared DPT with the saline injection that was mentioned earlier. 8 The authors concluded that saline injection may result in symptomatic relief as well as a favorable functional outcome, and also in terms of MCID of variables. 33,34 In our study, PRTEE-T score improvement in the DPT group outperformed the saline group between baseline-4th week and baseline-12th week. This result may be related to the early effect of saline or the late onset of the clinical effect of DPT. A comparison of early and late effects of saline and DPT is required in future studies. As shown in the figures, VASrest, VASmotion, DASH, and PRTEE scores trended in favor of DPT over time, but none of the changes in those variables reached significance level.
Time elapsed during the study period may stand for wait-and-see, which is one of the choices for LE treatment. The self-limiting nature of LE should be considered while interpreting the comparison studies of DPT and saline in different tendinopathies. It should be kept in mind that the home-based exercise program may contribute to the improvement in outcome measurements in both groups. But the opposite practice might not be appropriate ethically.
There has been no consensus for DPT in LE treatment in terms of the concentration; injection number, and intervals. In this study, we used a 15% concentration of dextrose. The previous studies used 11%, 16%, 20%, and 12.5% concentrations of dextrose. 8,30 –32,35,36 In addition, the injection techniques are different between studies. In some of them, practitioners used the peppering technique, whereas in others the DPT solution was injected into the tendon insertions without the peppering technique. 8,30,31,35 We injected the DPT solution into the insertion of extensor tendons, annular ligament, and supracondylar ridge. 8 Multiple injection methods had been used in most of the studies; however, some of the authors applied only one injection. 8,30,35,36
DPT is a safe and inexpensive regenerative treatment strategy. We observed no adverse effects in this study except pain while having injections in any of the interventions. None of the participants reported a need for analgesics beyond paracetamol in both study groups. Although the drop-out rate is higher in the DPT group than the saline group, neither pain nor other possible adverse events were the reason.
Limitations of this study were a short follow-up time and a relatively small study group. However, compared with previous studies, we consider that the follow-up time and the number of subjects were acceptable. 8,30,31,35 Addition of an amide local anesthetic to the DPT solution would be helpful in pain management and result in more comfort during the procedure. Although none of the participants reported any reason for discontinuing the study, the unpleasant feeling related to intervention procedures may have directed them to seek alternative procedures and solutions. An experimental model showed that usage of short-term NSAID does not have a negative impact on the effects of DPT on tendon specimen and fibroblast number. 37 On the other hand, results of an in vitro study may not always match with the findings in in vivo and clinical studies. Avoiding NSAIDs is the most rational method to not cause a multifactorial bias. Avoiding NSAIDs may be one of the factors for the high dropout rate of our study.
Because of the placebo effect of the injections and the possibility of spontaneous remissions of LE, the effect of DPT and saline may have been overestimated. We do not know, but a bias for high reporting is postulated in our study group. The placebo effect may contribute to the high improvement reports in the saline group. Although we predicted a 30% dropout because of the compliance problems, we suspect that the patients who dropped out of the study might be nonresponders and exaggerating the improvement of outcome scores. One of the reasons for the high baseline scores may be the enrollment of the chronic LE patients with a minimum VAS value of 4. The previous studies had enrolled the patients with less symptomatic severity than that of our study group. 31,32,36 It is also possible that the participants who accepted to participate in the study might have been more severely affected than the general.
Although we calculated that at least 22 participants for each group (with 85% power) should be included based on our pilot study, the post hoc power of this study was calculated as ∼60%. Future studies are necessary with a larger study group comparing the effect of DPT with saline injection.
The strengths of the study are: randomization and successful blinding of the investigators and patients. It has been one of the few studies assessing the effect of DPT in comparison with saline injection. It will create a background for examining the effectiveness and mechanisms of DPT in different concentrations and saline injection, in the treatment of chronic LE. Future experimental and clinical studies are necessary to compare the effectiveness of different solution types.
Conclusion
In this RCT, we compared the short-term effect of DPT and saline injection in chronic LE. Our results suggest that both saline and DPT lead to an improvement in pain severity and functionality. It is noteworthy that saline injection with the same technique has a favorable outcome in LE. On the other hand, PRTEE-T change was significantly higher in the DPT group than the saline group. Future studies are designed with more objective measurements, longer follow-up periods, and larger number of patients; an exploration of the effect of solution type and injection type regarding the use of DPT for chronic LE treatment is required.
Footnotes
Author Disclosure Statement
None of the authors received any financial payments or other benefits from any commercial entity related to the subject of this article.
Funding Information
No funding was received for this article.