
Abstract
Background:
Vitiligo is an autoimmune skin condition that affects people globally anywhere, from <0.1% to more than 8% of individuals. The disease destroys skin melanocytes, resulting in a patchy depigmentation of the skin. About 50% of all patients develop the disease before their 20s.
Methods:
We systematically searched the literature and reviewed the evidence for the use of nutritional supplements and diet in the management of vitiligo. Embase and Medline were searched for diet, herbal, and nutrition-based clinical studies. Additional filters were applied that looked for controlled trial or randomized controlled trial and article or article in press or letter and English and clinical study. We selected clinical studies in humans that showed how diet or natural supplements can improve the symptoms of vitiligo in all of our searches.
Results:
There were 62 manuscripts that resulted from the PubMed search and 259 from the Embase search. A final of 26 studies were reviewed, and other supplemental case and case-control studies were used to introduce diet components that may influence either exacerbation or amelioration of vitiligo. Possible mechanisms of action are introduced for natural and supplemental interventions.
Conclusion:
Some of the supplements reviewed include Gingko biloba, oral Polypodium leucotomos, alpha lipoic acid, vitamins B12, D, and E, folic acid, phenylalanine, canthaxanthin, Nigella sativa oil, and other combined herbal bio-actives. Overall, the growing evidence is promising, but more studies are needed in this area to further explore the impact that supplements and diet can have on vitiligo management. The most promising therapies included oral phenylalanine as adjuvant therapy with UVA therapy, oral G. biloba as monotherapy, both of which can be used with other traditional therapies, and oral P. leucotomos with phototherapy or photochemotherapy.
Introduction
Vitiligo is a common autoimmune skin condition that is estimated to affect 0.1% to more than 8% of individuals and about 1% of the U.S. and European populations. 1 Vitiligo is generally classified as segmental or generalized and further classified into subtypes, such as localized, generalized, or universal, which is based on how many patches of skin are affected, with generalized being the most common. The disease destroys skin melanocytes, giving the appearance of patchy depigmentation. 2 The disease can affect many areas on the body and frequently affects visible parts of the body such as the face, which can lead to embarrassment and to lowering the quality of life of the people affected, in part because of the public's response to its resemblance to leprosy. 2
Multiple factors are involved in the etiology of vitiligo. Genetics plays a role in vitiligo since first-degree relatives have a 6%–8% risk of developing vitiligo later on in life. 3 The inheritance of the skin condition is not very clear due to the fact that it is a multi-genetic disease with a complicated pathogenesis. 3 There are different theories that attempt to explain vitiligo pathogenesis, including the neural theory for segmental vitiligo, 4 –7 the autoimmune theory, 8 the ROS (reactive oxygen species), 9 and the melanocytorrhagy theory, 10 all of which are detailed in Table 1.
Theories of Pathogenesis Related to Vitiligo Type
ROS, reactive oxygen species.
Treatments for vitiligo have typically focused on corticosteroids, immunomodulators, and phototherapy. For participants who do not respond well to topical therapies, the alternative is narrow-band ultraviolet B (NB-UVB) light. 3 Although conventional medicine can be effective in controlling vitiligo, limitations, including the requirement of frequent phototherapy visits, risks of immunosuppression, increased risk of skin cancer with photochemotherapy use, limited accessibility due to drug and treatment costs, side effects from pharmaceuticals, or limited efficacy with incomplete patient satisfaction, can all be additional gaps in therapy that need to be addressed.
In a study on patient satisfaction from vitiligo treatment, out of a score of 100 (extreme satisfaction), patients ranged from on average of 41 with topical tacrolimus to 78 with NB-UVB phototherapy. 11 Alternative therapy may help increase efficacy, safety, and patient satisfaction. Although the research for the use of alternative and adjunctive therapies for vitiligo is growing, there have already been multiple case reports and studies that have been completed. In this review, we describe these studies and present the evidence for the utilization of diet, supplements, and herbs, and their role in an integrative approach to the treatment of vitiligo.
Materials and Methods
Searches for articles published before April 26, 2020 were conducted on Embase and MEDLINE. The MEDLINE and Embase searches were for diet, herbs, or nutrition and vitiligo. Additional filters were applied that limited for controlled trial or randomized controlled trial (RCT) and article or article in press or letter and English and clinical study. We selected clinical studies in humans that showed how diet or natural supplements can improve the symptoms of vitiligo in all of our searches. Although topical therapies were typically removed, we allowed studies that utilized oral agents that had also been studied topically or if the topical agent was a herbal one.
There were 62 papers that resulted from the PubMed search and 259 from the Embase search. The titles and abstracts were reviewed for relevance, which yielded a total of 72 papers. Seventy-two papers were reviewed for study type, and a final 26 studies were reviewed in detail (Tables 2–4). Other supplemental case and case-control studies were used to introduce diet components that may influence either exacerbation or amelioration of vitiligo. Possible mechanisms of action are introduced for natural and supplemental interventions. See Figure 1 for flow diagram for the inclusion of studies. The associated PRISMA 2009 Checklist is available as Supplementary Material.
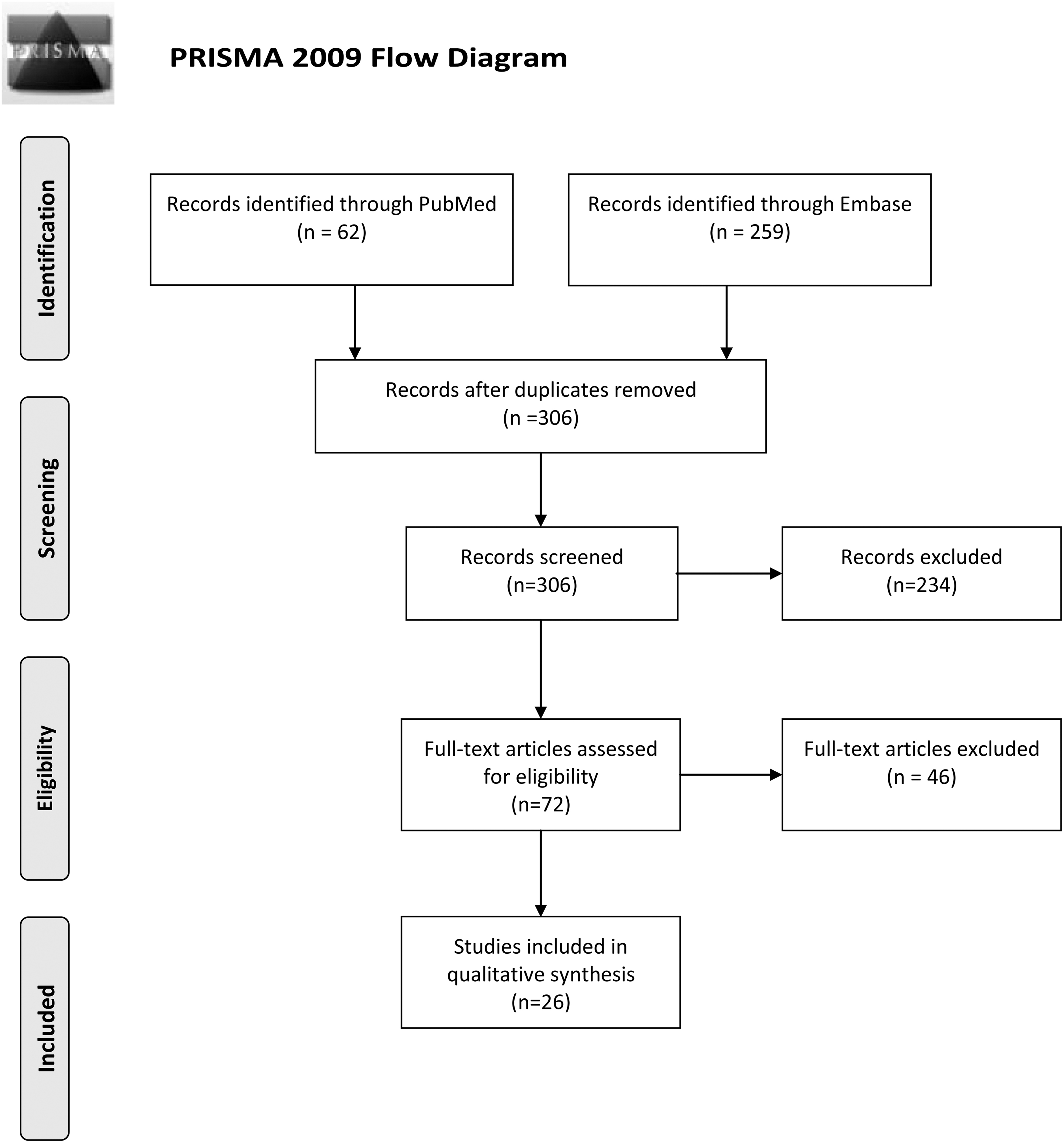
PRISMA 2009 flow diagram. From: Moher et al. 113
Diet Components and Amino Acids Involved in Vitiligo Treatment
ALA, alpha-lipoic acid; NB-UVB, narrow-band ultraviolet B; Phe, phenylalanine.
Vitamins Involved in Vitiligo Treatment
NB-UVB, narrow-band ultraviolet B; PUVA, psoralen and ultraviolet A; VD, Vitamin D.
Botanicals and Herbs Involved in Vitiligo Treatment
ER, excellent re-pigmentation; GR, good re-pigmentation; KUVA, khellin used with UVA therapy; MEL, monochromatic excimer light; MR, moderate re-pigmentation; PL, Polypodium leucotomos; PoR, poor re-pigmentation; PR, proliferative response; VASI, Vitiligo Area Scoring Index.
Results
Database search results for adjunct therapies were categorized into diet components, amino acids, vitamins, vitamin analogues, and botanicals and herbs. Tables 2–4 summarize clinical trials and utilize the Jadad score 12 to evaluate for quality of methodology and risk of bias. This review aims at summarizing efficacy, as demonstrated in the current literature, and at introducing possible mechanisms of action and side effects of interventions. Diet-related adjustments and supplements that may be associated with improvement of vitiligo in case-control and case studies are briefly reviewed as well.
Diet components and amino acids
Gluten
Case reports have shown that participants with vitiligo might experience improvement after stopping the ingestion of gluten. 13,14 When a young female adult with vitiligo began a gluten-free diet, she experienced early and extensive re-pigmentation of her facial lesions. 13
Another report presented a girl with vitiligo who also had concomitant celiac disease. After being on a gluten-free diet for a year, her depigmented macules showed re-pigmentation after 3 years. After 7 years on the diet, she still maintained the pigmentation. 14 Although these case reports are interesting, formal studies are lacking and follow-up is needed on the case reports here. Future studies in patients with vitiligo could measure gut permeability surrogate markers such as zonulin levels before and after gluten elimination and evaluate antigen translocation across the small intestinal barrier due to gluten.
Fatty acids
Intake of fats can also be associated with autoimmune conditions such as vitiligo. Evidence shows that participants with vitiligo consume more saturated fatty acids and less eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) than individuals without vitiligo. In addition, a higher total fat intake was linked to a higher incidence risk of vitiligo. 15 These findings might be related to the fact that EPA and DHA have been shown to have anti-inflammatory effects.
Alpha-lipoic acid
Alpha-lipoic acid has recently been studied as an adjuvant treatment for vitiligo. 16,17 In addition to its role in biological mitochondrial reactions, it is an antioxidant. In its reduced form of dihydrolipoate, it reacts with ROS, protects cell membranes with its involvement with vitamin C and E pathways, and has been shown to have beneficial effects in oxidative stress models and several clinical conditions characterized by inflammation. 18 One might note that dihydrolipoic acid can reduce oxidized Vitamin C into the reduced form.
Clinical studies have studied alpha-lipoic acid in combination therapy with other antioxidants such as vitamins C and E, polyunsaturated fatty acids, and for use in combination with NB-UVB phototherapy. 19 The treatment with various antioxidants, in addition to the NB-UVB treatment, significantly improved the effectiveness of the phototherapy, with 47% of participants obtaining >75% re-pigmentation versus 18% in the placebo group. 19 The success of the combined therapy suggests that the antioxidant's role of eliminating free radicals from phototherapy helps treat vitiligo while also helping to counteract the oxidative stress occurring in patients with vitiligo.
Phenylalanine
Phenylalanine (Phe), an amino acid, is theorized to work as a potential treatment for vitiligo through playing a central regulatory role in melanin, catecholamine, and antibody synthesis, contributing to the hypotheses of autoimmune and neural theories of vitiligo pathogenesis. Phe is hydroxylated to tyrosine and feeds into the melanogenesis pathway. Phe and tyrosine are also implicated in catecholamine synthesis. Within the neural theory of vitiligo, catecholamines generated by autonomic nerve endings are hypothesized to be implicated in the etiopathogenesis of vitiligo through either direct cytotoxic effects or indirect action. 6 Disruption in catecholamine synthesis due to Phe or metabolite levels could be influencing vitiligo development or progression.
It has been shown in vitro that primary epidermal melanocytes of vitiligo participants have decreased
In a clinical trial examining the effects of Phe on vitiligo, each of the participants acted as their own control, where they were first treated with oral Phe (50 mg/kg) twice weekly alone for 4 months after 4 months of UVA therapy alone. Improvement was not seen when the therapies were given in isolation. When phenylalanine was given in combination with UVA light, 94.7% of the participants experienced follicular re-pigmentation, with 26.3% experiencing dense re-pigmentation. 22
Another study of Phe separated vitiligo participants into two groups, with one group receiving oral
The results suggest that perhaps incorporating topical and oral phenylalanine into a treatment program with phototherapy can provide more re-pigmentation for vitiligo participants. In a group of 36 patients using a topical formulation of Phe, cucumis melo extract, and acetyl cysteine and the addition of NB-UVB therapy showed a greater increase of re-pigmentation in vitiligous lesions than in the 33 patients using clobetasol 0.05% ointment alone. 24 Additional studies on adjunctive use of Phe are reviewed in Table 2. 25 –27 Currently, there are very few UVA-based phototherapy booths and future studies with NB-UVB and Phe may be more relevant.
Topical antioxidant mixture
Topical antioxidant mixture Vitiskin® is a combination of superoxide dismutase, copper, zinc, vitamin B12, and calcium panthotenate that has been studied for use with 308 nm excimer light therapy to treat vitiligo. In a prospective comparative randomized study with 30 participants with localized stable vitiligo, the combination of Vitiskin and phototherapy was shown to outperform (p < 0.001) phototherapy alone for improving vitiligous lesions (based on the percent of lesions showing graded re-pigmentation responses). 28
Vitamins
Vitamin B12 and folic acid (vitamin B9)
Vitiligo and pernicious anemia have been previously associated with one another, which motivated research to investigate an association between vitamin B12, vitamin B9, and vitiligo. 29 In one textbook describing nutritional management of vitiligo written by an Argentinian dermatologist, he notes that abnormally low levels of vitamin B12, folic acid, vitamin C, and copper have been seen with a large number of his patients. 30
Both vitamin B12 and B9 are implicated in the biosynthesis of melanin in human epidermis, with vitamin B12's role in methionine production regulation and folate's role as components of pteridine and N-N-methylene tetrahydrofolate. 31 Deficiencies in enzymes (e.g., cystathionine β-synthase in homocystinuria) or metabolites (e.g., pteridine deficiency) can create clinical problems with pigment formation. 32,33 In addition, in vitiligous skin, defective 4a-hydroxytetrahydrobiopterin dehydratase impairs tyrosine production, which alters melanin production. 34
One clinical study showed that serum levels of folic acid and vitamin B12 in vitiligo participants were not significantly different from controls, which led to their conclusion that folic acid and vitamin B12 do not have a role in the pathogenesis of vitiligo. 29 On the other hand, another study showed that folic acid and vitamin B12 in combination with sun exposure gave better re-pigmentation for vitiligo participants than either one alone could. 35 However, another controlled study showed that when folic acid and vitamin B12 were used in combination with narrow band UVB, there was no significant difference in re-pigmentation when compared with the group of participants who received phototherapy alone. 36 Overall, results are mixed in regards to the role of vitamin B12 and folic acid supplementation.
Vitamin D
Vitamin D is believed to have potential for vitiligo, because it may be able to modulate Wnt/β-catenin signaling in melanocytes under oxidative stress. Also, vitamin D inhibits the accumulation of ROS and cell apoptosis in H2O2-treated melanocytes and promotes their proliferative and migratory activity. Low vitamin D levels have been associated with various autoimmune diseases, and since vitiligo is an autoimmune disease, this can help explain why vitamin D insufficiency was also shown to be associated with severity of oxidative stress in vitiligo participants. 37 This evidence might suggest that vitamin D can possibly help prevent autoimmunity and be protective from various autoimmune diseases.
Topical synthetic vitamin D3 analogues (i.e., calcipotriol and talcalcitol) are forms of conventional therapies and their clinical studies for vitiligo have been reviewed elsewhere 38 and thus are not reviewed here in detail since they are not an oral approach to the treatment of vitiligo. Discussion here is limited to oral vitamin D supplementation.
To investigate whether vitiligo participants had an increased association with vitamin D deficiency, a study compared the serum levels between control and vitiligo participants. The study found no difference in the median serum levels of vitamin D between the controls and vitiligo participants. 39 However, another study did find an association, showing that only 2.5% of vitiligo participants had normal 25(OH)D levels in comparison to 82.5% of healthy controls. 40
In a prospective study comparing 30 young (ages 6–17) participants, half of whom had vitiligo (using tacrolimus) with those who did not, 14 of the participants were vitamin D deficient and received vitamin D supplementation. Oral vitamin D supplementation and topical tacrolimus in combination was found to be more effective in re-pigmentation than topical tacrolimus alone. 41 Vitamin D supplementation (daily 5000 IU for 5 months) was compared with no intervention in a blinded randomized trial of 48 females with rhododendrol-induced vitiligo. It was found that improvement scores were significantly higher in the intervention group than in the control group. 42
Vitamin E
Vitamin E is a fat-soluble vitamin that behaves like an antioxidant due to its radical scavenger capacity, giving it an important role in many processes contributing to the overall health of a person. 43,44 Vitiligo participants as well as other participants with skin conditions (i.e., psoriasis and alopecia areata) have a statistically significant lower tissue and serum level of vitamin E in comparison to controls. 43
When oral vitamin E was given in combination with NB-UVB, marked to excellent re-pigmentation was observed in 72.7% of vitiligo participants. A second group of vitiligo participants who were only treated with NB-UVB had only 55.6% of participants achieve marked to excellent re-pigmentation. 45 The study concluded that oral vitamin E might be beneficial as an adjuvant therapy for the treatment of vitiligo and that it can increase the effectiveness of NB-UVB.
When vitamin E was added to psoralen and ultraviolet A (PUVA) therapy in treatment of vitiligo, it was found that although there was no significant difference between those treated with PUVA and oral vitamin E and controls who only received PUVA, there was a significant increase in skin lipid peroxidation (a measure of oxidative stress generation) in the PUVA-only group, whereas the vitamin E-receiving group did not have a significant difference. This study showed that vitamin E may have a protective effect against oxidative stress from PUVA therapy when the two were used together. 46 The photoprotective effect may be due to antioxidant properties, decreased skin lipid peroxidation, and the fact that vitamin E absorbs certain light wavelengths. 47
Botanicals and herbs
Ginkgo biloba
G. biloba extracts are produced from the Gingko tree's leaves and have been used in Chinese medicine. 48 The extract has been studied as potential therapy for vitiligo when taken as a tablet once to three times daily for more than 3 months. 16,49
In addition to its more well-known neuroprotective, vasodilative, and platelet-related effects, Ginkgo has antioxidant and immunomodulatory properties. 50 Specifically, G. biloba extract has been shown to modify the Nrf-2 pathway in the H2O2 oxidative pathway. 51 Terpenes in the extract called ginkgolides B, C, J, and M were shown to neutralize free radicals. 52 In addition, they have been shown to reduce oxidative stress in murine macrophages and endothelial cells. 53 As an adjunctive therapy to UVB light therapy, G. biloba extract components biflavones can reduce UVB cytotoxicity, as shown in studies with cultured normal human fibroblasts. 54
In a study investigating the effect that G. biloba extract would have on vitiligo, participants with slowly spreading vitiligo who were given 120 mg of oral G. biloba extract daily experienced a statistically significant cessation in the progression of their depigmentation in comparison to the placebo group. The study, therefore, concluded that the extract could be a safe and effective therapy for stopping the progression of vitiligo. 50 Although the study showed promising results, more studies are needed to follow up on these results.
Polypodium leucomotos
P. leucotomos (PL) is a species of fern that has been studied for use in various skin conditions such as atopic dermatitis, psoriasis, and vitiligo and prevention of UV-induced skin damage and it has been used in Central and South America for traditional folk medicine. 55 PL has been studied for its antioxidant, anti-inflammatory, immunomodulating, and photoprotective properties. UV-induced photoprotection in inhibiting the formation and quenching ROS in human and animal models in vitro and in vivo may increase the efficacy of photo(chemo)therapy for vitiligo by increasing tolerability and decrease adverse effects by preventing sunburn and phototoxic reactions.
Both topical and oral preparations of the extract have been shown to have photoprotective effects by preventing acute sunburn and psoralen phototoxic reactions, quenching ROS, improving membrane integrity of fibroblasts and keratinocytes, inhibiting matrix metalloproteinases at low doses, and reversing loss of elastic fibers at high concentrations. 56 –59 PL also has been shown to have immunomodulatory behaviors in human PHA-stimulated peripheral blood mononuclear cells by inhibiting Th1 cytokines and stimulating Th2 cytokine production. 60
For vitiligo, oral PL has been shown to increase the efficacy of NB-UVB when used in combination with the phototherapy. 61,62 Increased re-pigmentation with combined therapy with PL and PUVA has also been shown. Participants in the PUVA and PL treatment group had more individuals who achieved >50% re-pigmentation than participants who were in the PUVA and placebo group.
Immunosuppressive effects were also demonstrated, with PUVA and PL provoking a significant decrease in proliferative response (PR) of peripheral blood mononuclear cells. IL-4 significantly reduced the PR of PUVA and PL groups and did not do so in the control group. There was a significant correlation between clinical response and percentage of CD3+CD25+ cells. 63 Another interesting finding was that after 5 months of treatment with Anapsos, a lipid hydrosoluble extract derivative of P. leucotomos, all of the vitiligo participants had full improvement of their disease. 64
Capsaicin
Capsaicin is an ingredient found in hot chili pepper and is commonly used in spices, food additives, and drugs. 65 Vitiligo is believed to be due to oxidative stress that causes melanocyte degeneration, 65 and the antioxidant effects of capsaicin and curcumin have been reported. 65 The results showed that curcumin and capsaicin inhibited apoptosis by inhibiting caspase activation and increased total antioxidant capacity. In one study, capsaicin was able to inhibit oxidative stress damage in cells that were derived from the perilesional skin from a patient with vitiligo. 65 Although this cellular finding is promising, there are no clinical studies on capsaicin and vitiligo.
Phyllanthus emblica fruit extract and carotenoids
P. emblica is a tree that bears fruit used in extracts that has been shown to have anti-inflammatory properties that, when paired with another plant extract from Plumbago zeylanica, has been shown to have comparable anti-inflammatory effects to that of aspirin in mice and rat models. 66 Carotenoids have been identified as antioxidants with vitamin E and have been shown to have photoprotective effects, clinically as suppression of erythema, when used in conjunction with ultraviolet phototherapy. 44,67 Individual carotenoids have different effectiveness in protecting against free radicals and quench free radicals in intact cells with many supporting studies. 68
P. emblica fruit has also been studied in conjunction with carotenoids and vitamin E for use with traditional vitiligo treatments in 130 subjects. Half of the study participants received conventional treatments such as phototherapy and topical treatments only. The other group received conventional therapy with topical or phototherapy and the combination oral antioxidant (oral antioxidant supplement containing P. emblica, vitamin E, and carotenoids thrice daily). The study showed that after 6 months, a significantly higher number of participants in the group supplemented with antioxidants had mild re-pigmentation on head/neck regions and trunk. The group without antioxidants experienced more inflammation, more rapid growth of vitiligous regions, a higher percentage of worsening disease, and more erythema. 69
Canthaxanthin
Canthaxanthin is a carotenoid present naturally in plants, bacteria, algae, and a variety of animals that possesses an orange to red color. In Canada and Europe, it has been used as “oral tanning tablets” that accumulate in the subcutaneous fat to “pigment” the skin without any effect on melanin pathways. Adverse effects include orange palms and soles, orange stools, orange blood, retinal deposits, and retinopathy. One study in Canada examined the use of canthaxanthin in participants with vitiligo. It was found that it produced clinically satisfactory cosmetic results for 45% of the total 56 participants, and more so (72%) in the subgroup of lighter-skinned individuals. “Tanning” effect would be lost after participants discontinue drugs. 70
Nigella sativa seed oil
N. sativa is an annual flowering plant that produces black seeds (black cumin) whose oil extracts have been used for a variety of therapeutic roles, including skin disorders. Its major component is thymoquinone, which has been studied as the major component providing many medicinal properties, including as an anti-inflammatory, anticancer, and immunomodulating agent. 71 –73 Topical application of Nigella sativa oil was shown to significantly improve the Vitiligo Area Scoring Index score 74 (VASI score) within 4 months. At 6 months, VASI score improved from 4.98 ± 4.81 to 3.75 ± 3.91 in the Nigella sativa oil group (p = 0.02) and from 4.98 ± 4.80 to 4.62 ± 4.36 in the fish oil group (p = 0.067). 75 The topical use of this oil could be a safe and effective adjunctive treatment to traditional vitiligo treatment.
Picrorhiza kurroa
P. kurroa is a well-known Ayurvedic herb that is traditionally known as Kutki and it is used for its hepatoprotective properties. It has also been shown to have immunomodulating effects on cell-mediated and humoral immunity, though these are still through largely unclear mechanisms. 76 P. kurroa active ingredient apocyanin has been shown to be an effective antioxidant by inhibiting NAPDH oxidase in neutrophils and microglia in vitro. 77,78 In a mouse model of dextran-sulfate-sodium (DSS) induced colitis, P. kurroa supplementation improved clinical and histological features of colitis by attenuating NF-κB messenger RNA (mRNA) induction and by decreasing release of inflammatory cytokines (IL-1b and TNF-a) and oxidation. 79
It was studied as an agent that may potentiate photochemotherapy in vitiligo, increasing the speed of re-pigmentation in the 27 of 30 participant cases used in conjunction with methoxsalen and prescribed sunlight exposure. 80
A seemingly paradoxical effect of P. kurroa is that it has been interestingly shown to be an immunostimulant of both humoral and cell-mediated immunity, shown to attenuate iatrogenic immunosuppression by cyclophosphamide. 81 Since vitiligo is suspected to be an immune-mediated disease, therapies would be believed to be down-regulators of immune activity.
In a study using an oral preparation of biopolymeric fraction, RLJ-NE-205 in mice showed that mice fed the extract had demonstrated a dose-dependent increase in hemoagglutin titer (p < 0.05), delayed hypersensitivity index (p < 0.01), plaque-forming cell assay (p < 0.05), and phagocytic index (p < 0.05). At the dose of 50 mg/kg, lymphocyte proliferation (p < 0.001) and IL-4 and IFN-gamma in serum (p < 0.001) were significantly increased. 82 These markers of humoral and cell-mediated immunity were demonstrated to be stimulated by the plant extract. However, it was shown that CD4:CD8 ratio was also increased (p < 0.01). In vitiligo, CD4:CD8 ratio is decreased. 83
A restoration of CD4:CD8 balance may be a possible benefit of P. kurroa, although additional immunological studies are warranted in the setting of vitiligo. In the limited study of the use of oral P. kurroa for vitiligo when used for light therapy, its action seems to be largely based on photoprotective antioxidant effects rather than immunomodulatory ones.
Khellin
Khellin is a crystalline extract of herb Ammi visnaga that has been used in Mediterranean folk medicine. When combined with UV therapy, activated khellin taken orally has been shown to stimulate melanogenesis and melanocyte proliferation in cultured normal human melanocytes, Mel-1 melanoma cells in vitro, thus potentially photosensitizing in vitiligo therapy similar to the effect of psoralen. 84 One uncontrolled retrospective study of 28 participants with extensive generalized vitiligo who had used oral khellin along with UVA therapy (KUVA) in a 14-year period showed that there was a statistically significant correlation between re-pigmentation response and number of KUVA treatments and total UVA dose. 85
The combination of topical khellin 4% preparation and 308-nm monochromatic excimer light (MEL) therapy has also been shown to have significantly more improvement of depigmented lesions when compared with no intervention. However, there was no significant difference in response between phototherapy alone and phototherapy with addition of topical khellin, which does not confirm the benefit of topical khellin. 86
In an uncontrolled prospective trial of 20 participants with recalcitrant localized vitiligo, the combination of MEL and topical khellin therapy yielded 70% of total participants in the “excellent” or “good” response categories and re-pigmentation of lesions was found to be significantly higher with disease duration <2 years (p = 0.02) and number of sessions (p = 0.03). 87 One concern with topical khellin as adjunctive measure to phototherapy is that the proposed photosensitizing effect (like that of psoralen) may increase the adverse phototoxic and carcinogenic effects of phototherapy.
Discussion
The importance of reviewing nutrition, dietary supplement, and herbal studies lies in the need for supportive measures to traditional vitiligo therapies that have largely focused on topical anti-inflammatories, phototherapy (UVA or UVB), with the addition of photosensitizing agents and sometimes systemic corticosteroids. Conventional approaches largely address the autoimmune hypothesis of vitiligo with immunomodulation and anti-inflammatory approaches. There is still a lack of satisfactory results in some patients. Phototoxicity and the production of more oxidative damage to the skin may result from phototherapy or photochemotherapy.
The utilization of photo-protective adjunct therapies to supplement light therapy can be a tool in achieving balance between the benefits of light-induced stimulation of melanogenesis and immunomodulation, with increased oxidative stress as an adverse side effect. Nutrition, supplement, and herb-based therapies better address the ROS and autoimmune hypotheses; offer a synergistic option with conventional options; and may increase the tolerability of light therapies, especially in those of low phototypes.
Most recently, NB-UVB has been shown to be one of the safest and most effective therapies for vitiligo. 88 However, its mechanism of action in stimulating melanogenesis and modulation of cutaneous immune system is still unclear. Because of the perifollicular pattern of re-pigmentation that results from treatment, phototherapy has been hypothesized to mainly act on follicular melanocyte precursor reserves by stimulating melanocyte migration, mitogenesis, and melanogenesis. 89,90
Within preserved melanocytes, there are many pathways within melanogenesis and other various factors regulating pigment formation but UV radiation is the most important. 91 UV-induced melanogenesis has a complex mechanism that is initiated by the resulting DNA damage and repair activity in keratinocytes and melanocytes. 91,92 UVB directly damages DNA damage with pyrimidine dimer formation. 93 –95 Gene expression of melanocortin 1 receptor, a regulator of melanogenesis, has been found to increase in skin of patients with stable vitiligo after being treated with NB-UVB. 96 UVA predominantly produces indirect DNA damage through forming ROS. 97,98 So even though oxidative stress from ROS formation from UVA can actually stimulate melanogenesis, it can also be toxic to melanocytes.
One study showed that the inhibition of melanogenesis was seen in B16 melanoma model cells with exposure to H2O2 through time- and dose-dependent downregulation of melanogenic enzymes, which could mean that hypopigmentation could result from oxidative stress. 99 Melanogenesis, itself, can result in pro-oxidant state. 100 Skin cancer development is also a major concern for UV-based therapies. There is a clear need for studies on antioxidant supplementation and photoprotective agents in vitiligo, especially for use in conjunction with phototherapy. It has been shown that both UV radiation and tyrosine exposure have increased oxidative stress in melanocytes, which also implicates possible modulators of tyrosine levels in the diet and adjunctive therapies. 101
Though the complex pathogenesis of nonsegmental vitiligo with multiple genetic and environmental contributors is still unclear, in the past decade, the idea of the oxidative stress-autoimmunity-mediated melanocyte loss seems to provide a union between the ROS and autoimmune theories. 102,103 Excess ROS have been found in the skin of active vitiligo due to polymorphisms of ROS-associated genes and various disturbed antioxidant pathways. 103,104 It has been shown that in cultured melanocytes strains from active advancing borders of vitiligo were shown to have increased sensitivity to oxidative stress and have abnormal tyrosinase expression, contributing to the ROS theory of vitiligo. 105
Vitiligo lesional epidermis also has accumulation of H2O2 and low catalase levels. 106,107 Patients with active vitiligo had higher levels of DNA damage and lipid peroxidation associated with oxidative stress. 108 Melanogenesis is a metabolically demanding process. Defective membrane lipids, mitochondrial electron transport train impairment, and the resulting increase in the generation of ROS may be implicated in melanocyte degeneration in vitiligo. 109 In addition, oxidative stress in erythrocytes and neutrophils has been shown to generate autoantigens (e.g., oxidized tyrosinase) and increased levels of specific serum IgG are found in the patients with vitiligo, correlating with disease duration. 110
Tissue damage and local inflammation causes melanocytes to result in the production of damage-associated molecular patterns and chemokines that trigger the innate immune system. 111,112 This provides a connection between the ROS and autoimmune theories, where the innate immunity (activated and matured dendritic cells) presents the ROS-generated autoantigens to adaptive immunity, eventually leading to cytotoxic T cell recruitment and melanocyte destruction or disease progression. 104
One can imagine that the antioxidant, immunomodulatory, and photoprotective properties of adjunctive agents can target many contributing factors of vitiligo, including the initiating factor of oxidative stress, the progressive autoimmune destruction of melanocytes, and challenges with melanocyte regeneration. The increase in knowledge about the pathogenesis of vitiligo can tell us more about the specific mechanism of actions of emerging treatments.
Most of the reviewed studies had populations of generalized vitiligo participants. Active and stable cases of generalized vitiligo may require different doses or therapies. There were no cases of alternative or adjunct therapies being used to treat segmental vitiligo that resulted from the database search. More research needs to be done on the possible mechanisms of alternative agents that may modify elements of the neural theory of segmental vitiligo. Because some of the natural alternatives and adjunct therapies are often discovered from folk medicine origins, there are often a few RCTs. Nevertheless, our review shows that combined treatments, such as antioxidants or P. leucotomos, show promising results in pilot studies that warrant further future investigations.
Most promising therapies included oral and topical phenylalanine as adjuvant therapy with phototherapy, oral G. biloba as monotherapy (that may be used with other traditional therapies), and oral P. leucotomos with phototherapy or photochemotherapy. These warrant further investigation.
G. biloba and P. leucotomos have unique immunomodulatory effects in shifting toward type 2 dominant cytokine profile and could attenuate the mechanisms involved in the autoimmune theory of the pathogenesis of vitiligo. Vitamin E, G. biloba, P. leucotomos, and possibly P. emblica fruit extracts, and carotenoids could be used for their antioxidant and photoprotective features. Khellin and P. kurroa may accelerate benefits from phototherapy but will need additional studies to better assess for efficacy. Classifying these different therapies as antioxidant, immunomodulation, anti-inflammatory, and photoprotective or even photosensitizers can be useful for use in combination with traditional Western therapies or with other alternative therapies.
The next steps in investigating integrative vitiligo therapies include additional RCTs and the implementation use of placebo-controlled, double-blind, and randomized trials. After understanding the antioxidant profiles and cellular stabilizing features of each ingredient, there could be standardized development of oral antioxidant “cocktail” and combination topical therapies that could be used for subsequent RCTs for improved clinical efficacy.
An additional layer in integrative strategies for vitiligo is also treating the emotional stress in vitiligo participants. Supplement interventions such as G. biloba and P. leucotomos can help address stress response, oxidative stress, and immunomodulation in an interconnected way. Phototherapy studies should incorporate NB-UVB since most of the previous studies focused on UVA and phototherapy are typically done with NB-UVB at this time.
The challenges to research and implementation of these interventions include the multifactorial pathogenesis and contributing factors to development of vitiligo, which is a challenge to finding an efficacious monotherapy, and further support the use of integrative approaches. It has yet to be confirmed whether integrative therapies will be better in the active or stable state of vitiligo. Risks and side effects should be closely monitored. Botanicals, herbs and their extracts are multicomponents that can be beneficial, but active ingredients and predominant effects need to be elucidated.
Batch variation, purity, and sourcing of these supplements are also a challenge, which investigators can help avoid by consistent use across studies from a few reliable sources and consistent dosing. In the past 25 years, advancements in the biochemical understanding of mechanisms of action of G. biloba and P. leucotomos have proved to be encouraging in providing a platform as new therapies with identified targets. As we continue to classify and incorporate these alternative and adjunct therapies with traditional therapies, there is promising outlook for safe, efficacious, and accessible integrative treatment for vitiligo participants.
Footnotes
Author Disclosure Statement
R.K.S. serves as a scientific advisor for LearnHealth and Arbonne and has received honoraria from Burt's Bees, Abbvie Pharmaceuticals, Sun Pharmaceuticals, Leo Pharmaceuticals, Physicians Exclusive, Nutrafol, and Regeneron Pharmaceuticals, and is a stockholder of Dermala. C.J.C. has received honoraria from Burt's Bees. No competing financial interests exist for the other authors.
Funding Information
No funding was provided for the work in this article.
Supplementary Material
PRISMA 2009 Checklist
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.