
Abstract
Objectives:
This study aimed to explore barriers and facilitators to integrative oncology (IO) service provision and access in Australia.
Design:
The study design was mixed method with two substudies: a cross-sectional national cancer service survey of public and private sectors; and focus group interviews and an online survey of cancer survivors. Triangulation analysis of qualitative and quantitative data was used to identify and interrogate meta-themes.
Subjects:
The cancer service response rate was 93.2% (n = 275/295); 71/275 (25.8%) provided IO. Thirty-three cancer survivors from Anglo-European, Arabic, Vietnamese, and Chinese backgrounds were interviewed, and 121 survivors answered the online survey.
Results:
IO gaps were substantial, with no services in many regions and cities; a lack of diversity and availability of therapeutic options, including culturally appropriate services; and a mismatch between the high use of natural health products by survivors and types of IO services provided. Two overlapping meta-themes were identified: “barriers and facilitators” and “peoples and institutions”; each with four subthemes, respectively, “access/provision, affordability/funding, information/evidence, and culture/values” and “cancer survivors, healthcare professionals, organizations, and policies.” While affordability/funding was the greatest barrier to survivors and providers, solutions varied (e.g., building a stronger evidence-base, business model advice) and often conflicted (e.g., public verses private sector funding). The most insidious barrier was professional/corporate cultures and values that influenced hospital policies (or lack thereof), conceptions of evidence and the therapeutic alliance. Survivors called for a change of mindset in the culture of medicine and value-based health care.
Conclusions:
The barriers and facilitators to IO services were more complex than building the evidence-base and demonstrating value to justify funding. To achieve a better alignment of patients' preferences with service provision, providers require more guidance on clinical governance, business models, local service gaps, and interprofessional collaboration. National strategies and funding models are needed to ensure appropriate, equitable IO service provision.
Introduction
Despite the ongoing controversy about the benefits and risks of traditional, complementary and integrative medicine (TCIM), 1 demand by people who have had a diagnosis of cancer (herewith, referred to as cancer survivors) and its integration into conventional cancer services continues in Australia and abroad. 2 –8
The Society for Integrative Oncology defines integrative oncology (IO) as “a patient-center, evidence-informed field of cancer care that utilizes mind and body practices, natural products, and/or lifestyle modifications from different traditions alongside conventional cancer treatments. Integrative oncology aims to optimize health, quality of life, and clinical outcomes across the cancer care continuum and to empower people to prevent cancer and become active participants before, during, and beyond cancer treatment.” 9,10
Research in Australia has mostly focused on TCIM use, patient experiences, and clinical trials. 2,5,11 –14 Before this study, there was limited information about extent of IO service provision and key determinants influencing implementation and access. 15 –19 In response, a national survey of cancer services was conducted in 2017 that was accompanied by an online survey and focus group interviews with cancer survivors. 20 The main results of the two substudies have been reported seperately. 21 –24 This article reports the final synthesis of all the results and combines the perspectives of cancer service providers and cancer survivors. The aim was to identify and explore the barriers and facilitators of IO service provision in Australia.
Materials and Methods
Design
A mixed-method triangulation protocol as outlined by O'Cathain et al. 25 and Farmer et al. 26 was used to integrate and synthesize a more complete understanding of the research findings from two substudies and three data sources: a national cross-sectional survey of health care organizations that provided specialized cancer services, and a mixed-method study comprising of focus group interviews with cancer survivors that was supplemented with an on-line survey. The materials and methods from the two substudies are summarized below and are reported in detail elsewhere. 21 –24
Settings and participants
An extensive search strategy identified all health care organizations in Australia that provided clinical care to cancer survivors of any age. Inpatient or outpatient services linked to a hospital, registered day hospital, or community-based organizations were eligible. Australia has a mixed public–private health care service that aims to ensure universal health care. As such, organizations from both the public and private health sectors were eligible. Excluded were organizations that only provided palliative care services and small businesses with consultation rooms only. Eligible organizations were contacted and invited to participate. Consenting organizations then nominated one staff member from their cancer service to answer the survey.
Purposive sampling was used to recruit adult cancer survivors of Anglo-European, Arabic, Chinese, and Vietnamese Australian backgrounds for the interviews. The three culturally and linguistically diverse (CALD) groups were common in the geographical region of Sydney where the research team was based. Survey participants were a convenience sample of adult cancer survivors recruited through social media networks from across Australia.
Procedures, instruments, and data collection
The cancer services survey was a self-administered, purpose-specific, 52-item questionnaire with open and closed questions and skip-questions. Information was collected about the types of cancer services provided, organizational policies, important regional unmet needs and service gaps, and perceived barriers and facilitators to providing IO. Participants had the option of answering the survey online via SurveyMonkey, 27 as an electronic pdf, or on paper. The online survey was open for 8 months in 2016.
The focus group interviews used an “extended conversation” technique, 28, p. 96 with accredited interpreters as needed to explore their subjective experience with IO in the context of cancer service provision. The interviews were audiorecorded and transcribed verbatim. An anonymous, purpose-specific, online survey, consisting of 26 closed and open-ended questions, was designed to complement the focus group interview schedule and administered through SurveyMonkey. 27 The interviews were conducted in the first half of 2016. The survey was open for 3 months in mid-2016.
Analysis
The two substudies and their datasets were first analyzed and reported separately. 21 –24 For the two surveys, IBM SPSS Statistics for Windows, Version 24.029 was used for the descriptive and inferential statistical analyses that were supplemented by a descriptive qualitative analysis on an electronic spreadsheet of the open-ended answers and comments. The denominators used were the number of responses to a question. The interview transcripts were analyzed in NVivo Version 1130 using and inductive approach for a thematic analysis. 31 All qualitative data were independently analyzed and coded by at least two researchers.
The mixed-method triangulation analysis used an iterative process that was both inductive and deductive. 25 Key findings and themes that had emerged during the initial analysis of each substudy were first identified. Through a process described as “following a thread,” 32 themes identified in one dataset were searched for in the other datasets to identify meta-themes that were further interrogated for convergence (agreement or partial agreement), complementary (additional) information, and dissonance (contradictions, discrepancies, or disagreements). 25 The interrogation process aimed to optimize the strengths and limitations of the quantitative and qualitative research methods to facilitate a multifaceted understanding. 32
Consensus decision-making was applied throughout. All members of the research team had access to the de-identified data. To minimize bias and improve diversity, the research team comprised of five females and three males, with and without backgrounds in TCIM, IO, and/or cancer care.
Ethics
Human Research Ethics Committee (HREC) approval was granted by the Western Sydney University HREC (H11389) and the relevant state and local hospital HRECs. All participants gave specific consent.
Results
Response rates and participant characteristics
Of the 295 eligible health care organizations with cancer services, 275 (93.2%) participated in the study (Table 1). Most survey respondents (55.6%, n = 153/275) had dual roles as a health care professional and administration/management, 26.5% (n = 73/275) were health care professionals only, and 17.8% (n = 49/275) were in administration/management roles only.
Characteristics of Cancer Services (n = 275)
IO, integrative oncology.
A total of 140 cancer survivors participated, of which 29 were interviewed in 1 of 4 focus groups and 1 face-to-face interview (due to none of the other potential participants attending this focus group), and 121 answered the online survey (Table 2). A further four caregivers participated in the Arabic-speaking focus group. Notably, with the exception of the Arabic focus group, a large proportion of participants had used TCIM as part of their cancer care.
Characteristics of Cancer Survivors (n = 140)
Denominator used for interviews n = 29 and survey n = 121.
Four caregivers also attended the Arabic focus group.
Estimate based on diagnosis of breast/gynecological cancer.
No-one in the Arabic-speaking focus group had used TCIM.
Most common modalities were massage/touch therapy, meditation/relaxation, art/music therapy, and yoga/Tai Chi.
SD, standard deviation; TCIM, traditional, complementary, and integrative medicine.
Barriers and facilitators to IO
A wide range of barriers to accessing or using IO were reported by 85.0% (n = 91/107) of the cancer survivor survey respondents (Fig. 1) and all the focus group participants. Multiple reasons were given by the 204 non-IO providers for why their cancer service did not provide IO (Fig. 2), of which 130 (63.7%) answered the optional open-ended question about potential solutions (Fig. 3).
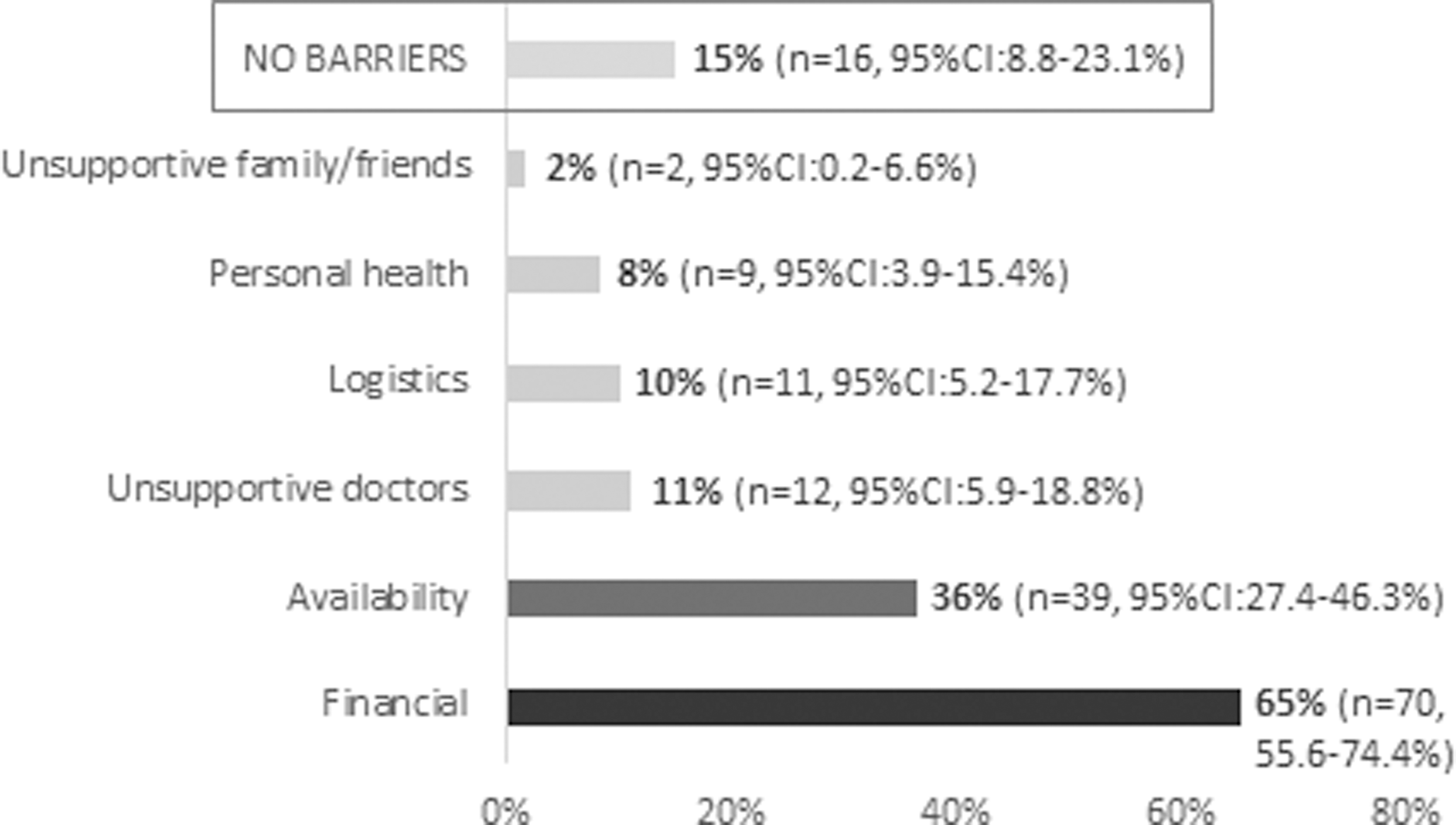
Cancer survivor barriers to accessing or using more IO (n = 107 [81.7%] of 131 survey respondents). IO, integrative oncology.

Cancer service barriers to providing IO services (n = 204 [100%] of non-IO providers answered this question).

Solutions for reducing barriers to IO service provision (n = 130 [63.4%] of 204 non-IO providers answered this question).
Two interrelated meta-themes, each with four subthemes were identified (Fig. 4). The first meta-theme, “barriers and facilitators” had four subthemes: “access/provision, affordability/funding, information/evidence, and culture/values,” which overlapped with the second meta-themes, “peoples and institutions” and its subthemes, “cancer survivors, healthcare professionals, organizations, and policies.” Most data within and between the substudies either converged or were complementary. Dissonance was only identified in some aspects of the meta-themes: barriers to access/provision and solutions for affordability/funding (Table 3).

IO barriers and facilitators.
Thematic Interrogation of Barriers and Solutions to Integrative Oncology
Number of symbols reflects both frequency and strength of quantitative and qualitative results: √, convergence/agreement; +, complementary/additional; x, dissonance/disagreement; −, silence/not discussed; n/a, not applicable (comparison between studies not possible due to silence in one study).
HCP, health care practitioner.
Access/provision
The most obvious barrier to cancer survivors accessing IO was the general under provision of services. Only a quarter of the cancer services in Australia (25.5%, n = 71/275) provided some type of IO, mostly on a fractional basis. Six of 30 health districts and 2 of the 8 States in Australia offered no IO services.
Despite the high use of TCIM by participating cancer survivors (Table 2), 36% (n = 39/107) of survey respondents still reported that a lack of available services had prevented them from accessing the IO they wanted (Fig. 1). Participants in the Anglo-European focus group who were purposively recruited through a public hospital that provided IO, also commented that local IO services were “often very booked,” with “demand far, far greater than the service that's available.”
Mismatches between TCIM use and the types of IO services provided were also identified. Ingestible TCIM were most often used by cancer survivors and the need for culturally appropriate IO services was emphasized by cancer survivors. Yet, less than a quarter of the IO services (23%, n = 16/71) had suitably qualified practitioners to provide advice on product use, including Chinese herbal medicine, Ayurveda medicine, and traditional medicines indigenous to Australia. Instead, nonbiologically based IO was mostly commonly provided (Table 1).
Personal circumstances further impacted access, for example, current health status, physical mobility, access to transport, available social support, the colocation of IO alongside their other health care services and the intensity of cancer treatment (e.g., number of appointments or treatment side effects). Access barriers were often amplified for cancer survivors living in regional and remote areas.
However, not all service providers agreed that there was an under provision. Low patient demand was selected by 31.9% (n = 65/204) of non-IO providers as a reason why their cancer service did not provide IO (Fig. 2) and only eleven respondents (4%, n = 11/275) nominated IO as the most important service gap in their region. In response, a few (4.6%, n = 6/130) non-IO providers called for local research to better ascertain patient demand and preferences (Fig. 3).
Workforce issues, such as finding appropriately trained TCIM practitioners with experience in cancer care was another barrier that both service providers and cancer survivors identified.
Affordability/funding
Overwhelmingly, affordability and funding were the greatest barriers limiting access to, and provision of IO services (Figs. 1 and 2). Similarly, addressing funding dilemmas and developing sustainable business models were commonly proposed solutions to improving access and service provision (Fig. 3).
The affordability of IO was a substantial personal barrier for the clear majority of TCIM users and nonusers alike. This, in turn, impacted patient demand and equity. IO was described as “very expensive as an ongoing treatment given all the out-of-pocket expenses associated with cancer” (cancer survivor survey), “especially when income capacity is reduced due to illness” (cancer survivor survey). Around half (49%, n = 35/71) of IO services relied, in part, or fully on patient payments that for some survivors, could include a partial subsidy from their private health insurance. Philanthropic funding of IO services (48%, n = 34/71) and volunteer practitioners (42%, n = 30/71) were common, and not-for-profit companies were significantly more likely to provide IO services (p < 0.001) compared to for-profit (odds ratio [OR] 0.21, 95% confidence interval [CI]: 0.11–0.41) and Government owned cancer services (OR 0.20, 95% CI: 0.06–0.31).
Funding policies were recognized by cancer survivors and providers as a key barrier that was often explained by the value judgment that IO is a “luxury item” (cancer survivor survey). Therefore, “government authorities do not recognize complementary therapies as being essential in supporting cancer patients through cancer treatment and beyond” (non-IO provider, cancer service survey). Some cancer survivors went on to emphasize, however, that IO services “aren't a luxury item, they are a necessity” (Anglo-European interviewee) that helps minimize the side effects of cancer treatment and supports recovery. To this end, one service provider affirmed that “I really have no interest in providing any of these services. We are too busy complying with accreditation and providing the best possible known treatment services to our patient … But if they were paid by the Health Funds as inpatient services at great reward, I would reconsider this.” (non-IO provider, cancer service survey).
There was also substantial disagreement about appropriate funding policies and business models. Some providers strongly contended that IO service provision was the responsibility of the public sector to provide affordable and equitable services, whereas others stated that “given the number of competing demands for resources within a public hospital” the private sector should pay, or that patients could “seek this if they wish to.” Similarly, while most respondents from the cancer survivor survey thought the public health sector should fund IO (85.9%, n = 92/107), many also thought the private health sector (48.6%, n = 52/107) and/or the cancer survivor or their family (23.4%, n = 25/107) should incur some, or all of the cost. Mixed views were also expressed by the focus group interviewees, including some who had very strong views about public funding as a just reward for a lifetime of work and taxes, or to reduce rising social inequalities.
Information/evidence
Accessing reliable information about IO and the need for more scientific evidence demonstrating benefits were common barriers. For some cancer survivors, the key reason they had not used TCIM or IO services was “we don't know anything about it—nobody tell us” (Arabic focus group). Indeed, patient information was only available in 61% (n = 43/71) of IO services and 34% (n = 69/201) of non-IO services. Other information barriers for cancer survivors included 63% (n = 69/110) preferring that referrals and recommendations for IO came from a medical doctor, yet, only 47% (n = 25/94) received such advice and many strongly expressed frustrations due to the failure of their doctors to discuss TICM, being slow to refer or giving conflicting information. Consequently, information and recommendations were often sourced from TCIM practitioners, family, friends, and the Internet, with a further 46% (n = 43/94) self-referring or self-initiating TCIM use.
While a paucity of access to information about the benefits and risks of IO was not considered a common barrier to service provision (10.8%, n = 22/204) (Fig. 2), “establishing an evidence-base” was an important part of the solution (49.2%, n = 64/130) (Fig. 3). For some, it was paramount as “until there is adequate evidence to support significant objective benefit the other barriers are irrelevant.” Demonstrating evidence of benefit was closely interrelated with demonstrating financial value. Both were among the most commonly suggested solutions (Fig. 3). While cancer survivors also recognized that scientific research was needed to “prove” the benefits they experience, some also viewed themselves as educators and living proof. By providing information and sharing their experiences with TCIM, they hoped that their cancer care team and doctors would learn more about the benefits of IO. The need for more staff education was also suggested by 26.9% (n = 35/130) of IO providers (Fig. 3).
Additional information barriers for cancer services included a lack of knowledge: how about how to establish or develop IO services (27.0%, n = 55/204), uncertainty about which IO services to provide (31.4%, n = 64/204) (Fig. 2), and uncertainty (35.5%, n = 93/262) about their organization's TCIM policies.
Culture/values
The term “culture” refers to the shared knowledge, belief, behavior, attitudes, and practices of a group of people be they racial, religious, social, professional, or organizational/corporate. Values reflect an individual's or group's priorities and beliefs about what is important, which, in turn, both influences and are influenced by culture.
The most obvious examples of cultural barriers came from the CALD focus group interviews. Despite the high proportion of CALD patients in a hospital, participants were frustrated by the lack of TCIM expertise, stating “they don't know anything. They only have Western people” (Chinese focus group). The use of TCIM reflected cultural norms and pride in their traditional knowledge, including a tendency to “always tell a good story” (Chinese focus group) despite the outcome. Survivors emphasized that respecting cultural diversity and providing culturally appropriate services required health care professionals and organizations to change their mindset so that IO services aligned with the traditional healing practices that are valued by the CALD groups they serve.
More insidious, however, was a corporate culture of biomedical dominance that marginalized IO practitioners and survivors who wanted to use these therapies. Survivors appreciated that it was the professional “duty” of doctors to “not recommend anything [that] is not proved” (Chinese focus group). Others talked about “there's always been this thing between doctors and alternative therapy practitioners” (Anglo-European focus group), however, “it shouldn't be looked at as an ‘us and them’ thing, the patient needs to get well asap” (Cancer survivor survey) “and to not have to justify, as if I am some kind of gullible idiot” (Cancer survivor survey).
Indeed, many of the 71 IO services were considered to be poorly integrated with the other cancer services and tended to operate on the fringe. While 83% (n = 58/71) of IO service providers held multidisciplinary team meetings or case conferences, 60% (n = 43/71) did not invite the TCIM practitioners. Other relevant barriers to IO service provision included unsupportive oncologists (25.0%, n = 51/204), management (7.8%, n = 16/204), and organizational policies (18.6%, n = 38/204), including instances where the hospital policy categorically banned self-initiated TCIM use (6.5%, n = 17/262).
The negative attitudes of some providers toward IO that were reflected in the experiences described by survivors were exemplified by the following quote: “I feel we are here to heal people, not be airy fairy, there are plenty of places for that. I also feel these complementary treatments belittle what we are trying to achieve.” (non-IO provider, cancer service survey)
The solutions provided by cancer survivors mostly focused on changing the dominant medical attitude through the open disclosure of TCIM use and the benefits experienced. Providers identified the need for top-down support, clinical governance directives, and a change in provider and practitioner attitudes (Fig. 3). “Guidance from a well-established complementary service” and “leadership to champion” were other suggestions.
Discussion
This is the first national study to concurrently explore the barriers and facilitators to IO services in Australia from the perspectives of cancer survivors and service providers. The findings were consistent with other studies, including a 2012 systematic review of IO programs, which found that service provision was influenced by evidence for safety and effectiveness, clinical experience, funding models, patient demand, practitioner availability, organizational culture, and logistical constraints. 33
The model in Figure 4 that emerged from the thematic analysis outlines a wide range of determinants that influence IO service provision and access in Australia. While similar to other conceptual frameworks that use the sociological levels of macro-, meso-, and micro-groupings, 34,35 due to the inclusion of cancer survivors in the research, this model illustrates how provision, affordability, funding, information, evidence, culture, and values impact IO access and utilization at the individual level (i.e., the cancer survivor). By placing the cancer survivor in the center of the model, it serves to remind us of the importance of listening to the consumer voice to ensure that policies, service provision, and cancer care are person-centered. Indeed, patient preferences are a cornerstone of value-based health care—a strategy that is increasingly being used for allocating limited resources. 36
The findings from this study are complemented by other Australian research, including a survey of supportive care cancer services that also found a general under provision of IO with little systematic integration. 16 In-depth interviews with leaders of 10 IO services in Australia were then conducted to explore their experiences and understand the factors underpinning the various IO service models and the challenges they faced. Four themes were identified—cultural context, human components, systematic components, and resource availability. 15
In keeping with other research, out-of-pocket costs were a personal barrier for both TCIM users and nonusers. 37 –39 In the context of Australia's public health system, the heavy burden of out-of-pocket costs relative to income mostly affects access to supportive care. 40 Compared to cancer treatment and palliative care, the additional costs of supportive services, including IO, are minimal. 38,41 Yet, these additional costs are often considered to be prohibitive by patients, hence the opinion expressed by some survivors and providers that the public health sector should fund IO to help reduce social inequalities. Not everyone agreed, however. This contention may reflect ongoing debate in Australia calling for more funding of all allied health and supportive services. 42 It was unclear the degree to which other types of supportive cancer care are also judged as nonessential, luxury items. Like supportive care in general, some have questioned whether integrating TCIM can be expected to directly lower health care costs, as IO services are generally used as an add-on, rather than a substitute for conventional cancer treatment. 43 The additional cost of IO will therefore need to demonstrate financial savings in other ways, for example, by improving adherence to life-saving cancer treatment and reducing the overall burden of disease. 44 –46
Finally, while a lack of evidence is commonly cited as a reason not to provide or fund IO, 47,48 the findings suggest that building the evidence-base is only one part of the solution. These findings are in line with other non-IO health services research that recognizes the complexities of cultural biases, pragmatic constraints, and the political and organizational realities of decision-makers that combined, often have a greater influence than scientific evidence in “real-world” health care priority setting and funding decisions. 49
The study and its substudies have numerous strengths and limitations that have been discussed in detail elsewhere. 21 –24 While a wide range of views and perspectives were obtained, oncologists and other cancer care providers not working in a larger health care organization were underrepresented, as were policy and decision-makers. The sample of cancer survivors was not statistically representative of the Australian population and in-depth focus group data did not adequately capture the views of cancer survivors from other CALD groups, including people who identify as Aboriginal and Torres Strait Islander. Further, thematic saturation was not achieved for many of the subthemes, particularly regarding potential solutions (Table 3). Notable gaps also included providers' perspectives on providing person-centered care, their own IO education and information needs, and supporting health literacy and shared decision-making with cancer survivors who want to access IO services. Despite these limitations, the findings were compatible with a similar study in Australia that focused on IO service providers, 15,16 suggesting that a larger, more representative sample of health care practitioners and policy makers is unlikely to substantially change the thematic model that emerged. Other validation of the model includes an earlier iteration that was successfully applied when comparing IO use and service provision in Australia, the United States, Canada, and across Western Europe. 7 Notwithstanding, further research is required to address these gaps, verify the model, and explore its relevance in other countries.
Conclusion
The barriers and facilitators to IO service provision identified in this study were more complex than building the evidence-base and demonstrating value to justify funding. To achieve a better alignment of patients' preferences with service provision, a change of mindset and the culture of medicine is required to truly provide value-based health care. Guidance on clinical governance and business models, local needs assessments to identify service gaps, more user-friendly patient information, interprofessional education and collaboration, and stronger national policies and leadership will be required for the strategic provision of appropriate, equitable IO cancer service provision in Australia.
Additional HREC Information
HREC approval was obtained from Western Sydney University HREC (H11389) and the Joint University of Wollongong and Illawarra Shoalhaven Local Health District Health (LHD) and Medical HREC (HREC/16/WGONG/178). In addition, HREC approval was obtained from Calvary Health Care, Adelaide HREC (16-CHREC-E011). Site approval was obtained for St. John of God hospitals (1004), Albury Wodonga Health (2016/344), Central Coast LHD (1116–117C), Illawarra Shoalhaven LHD (DT16–131481), Northern New South Wales LHD (G320), Murrumbidgee LHD (SSA/16/MLHD/43), and Western New South Wales and Far West LHDs (SSA/16/GWAHS/159).
Footnotes
Acknowledgments
The authors acknowledge and thank Alex Hawkey for helping to conduct the focus group interviews; Zelalem Mengesha for helping with the coding of the focus group transcriptions; Mike Armour for assistance with preparation of HREC submissions and contributing to recruitment and the arrangements for the focus groups interviews; Eleanor Oyston for her content expertise in the study design and implementation; and Oncology Massage Ltd., and their volunteers for their assistance with identifying local cancer services and recruiting cancer survey respondents.
Author Disclosure Statement
The study was conducted at the NICM Health Research Institute, Western Sydney University. As a medical research institute, NICM Health Research Institute receives research grants and donations from foundations, universities, government agencies, individuals, and industry. Sponsors and donors also provide untied funding for work to advance the vision and mission of the Institute. The project that is the subject of this article was not undertaken as part of a contractual relationship with any donor or sponsor. All authors declare no competing financial interests. J.H. is engaged in integrative medicine, primary care clinical practice. G.P.D. is a clinical oncologist, Director of Cancer Services for the South Western Sydney Local Health District, and Director of Liverpool Cancer Center in Australia. S.G. is engaged in Chinese Medicine clinical practice. All other authors have no declarations of interests.
Funding Information
This project was funded through a 2016 Research Partnerships Program, Western Sydney University. Partner funding was obtained from Oncology Massage Ltd, a registered charity that provides training to massage practitioners in Australia and internationally; and from South West Sydney Local Health District. Additional support was provided by NICM and the Center for Health Research at the University of Western Sydney.