
Abstract
Background:
Coronavirus disease 2019 (COVID-19) has become a pandemic with no specific and widely accepted effective drug or vaccine. However, studies have shown that Traditional Chinese Medicine (TCM) may play a significant role as an auxiliary treatment for COVID-19.
Objective:
This study aimed to assess the effects of TCM as an auxiliary treatment for COVID-19 through a systematic review of randomized-controlled trials (RCTs).
Methods:
Four English and three Chinese language databases were searched from December 1, 2019, to June 30, 2020. RCTs comparing TCM in combination with Western medicine (WM) with the same WM therapies alone for confirmed COVID-19 patients were included. The outcome measures were cure rate, lowering of body temperature, cough relief, improvement in chest computed tomography (CT) images, deterioration of condition, and adverse effects. Methodological quality was assessed using the Cochrane risk-of-bias tool. A series of meta-analyses were conducted for selected outcomes using RevMan 5.3 software. The quality of evidence was appraised using the grading of recommendation, assessment, development, and evaluation (GRADE) recommendations.
Results:
Ten RCTs with a total of 1,285 patients were included. Compared with WM alone in treating COVID-19, WM with auxiliary treatment by TCM appears to have increased the cure rate (risk ratio [RR] 1.15 [95% confidence interval (CI) 1.04–1.26]), relieved cough (RR 1.32 [95% CI 1.15–1.52]), improved chest CT images (RR 1.23 [95% CI 1.11–1.37]), and reduced the number of cases transitioning from a moderate to severe condition (RR 0.58 [95% CI 0.43–0.77]). The authors are uncertain whether TCM combined WM has effects on fever normalization (RR 1.10 [95% CI 0.94–1.29]) or adverse effects (RR 0.81 (95% CI 0.42–1.57]). Although they evaluated the certainty of evidence for lowering body temperature and adverse effects as very low, and low for cure rate, certainty was evaluated as moderate for improvement in chest CT images, cough relief, and deterioration of condition.
Conclusion:
TCM may be an effective auxiliary treatment for COVID-19 patients, which is likely to help improve the main symptoms and reduce disease progression. However, due to the limited number of studies and apparent heterogeneity among them, a more definitive conclusion on the effect of TCM on lowering body temperature and adverse effects cannot be drawn at this time.
Introduction
In December 2019, a novel coronavirus disease (COVID-19) emerged in Wuhan, Hubei, China. 1 COVID-19 patients have symptoms of varying severity, ranging from flu-like symptoms such as fever, cough, sore throat, shortness of breath to cardiac injury, and acute respiratory distress syndrome, as well as death. 2 COVID-19 is highly contagious, which has reached almost every country and geographic area in the world within only a few months. 3 This outbreak has been characterized as the first pandemic caused by a coronavirus, 4 with no approved therapeutic treatment or preventive vaccine for COVID-19 currently available.
Preliminary studies reported that some medications may be effective in inhibiting COVID-19 and in improving symptoms. Remdesivir, a promising drug currently under clinical trial, is reported to cause severe adverse reactions, such as multiple organ dysfunction syndrome, septic shock, and acute kidney injury, although it has shown certain beneficial effects in patients with severe COVID-19. 5,6 Data have also demonstrated that hydroxychloroquine does not reduce the mortality of hospitalized COVID-19 patients compared with standard care. 7 As a result, supportive treatment remains the mainstream Western medicine (WM) practice for COVID-19. 8
Traditional Chinese Medicine (TCM) has been widely recognized to regulate body function and improve immunocompetence in humans. 9 In China, TCM has been shown to be effective in treating female reproductive system diseases such as polycystic ovary syndrome, 10 pulmonary heart disease, 11 and nonsmall-cell lung cancer. 12 TCM has also attracted increasing attention in the treatment of various diseases, including Alzheimer's disease in Brazil, 13 rheumatoid arthritis in South Korea, 14 and menopausal symptoms in Netherlands. 15 One double-blind trial in Germany showed a significant decrease in fasting plasma glucose concentrations in diabetic patients following intake of 3 g of cinnamon powder per day for almost 7 years. 16
Previous studies have demonstrated that TCM has therapeutic effects in patients with SARS, 17 H1N1, 18 and Ebola. 19 In an observational study, an increase in the CD4/CD8 ratio was found in healthy volunteers after a 3-month intake of two herbal formulas (Sang Ju Yin, mainly containing Astragali Radix, Atractylodis Macrocephalae Rhizoma, and Saposhnikoviae Radix, as well as Yu Ping Feng San, containing Platycodonis Radix, Forsythiae Fructus, and Armeniacae Semen Amarum) daily for 14 days. 20 Another study showed that the use of Maxingshigan-Yinqiaosan (containing Forsythiae Fructus, Platycodonis Radix, and Arctii Fructus) alone could enhance fever resolution in H1N1 patients. 21
Unlike WM, which usually targets specific organ systems or particular pathogens, TCM takes a holistic approach toward well-being. 22 This approach may be particularly useful for multisystem disorders such as COVID-19 with no widely acceptable WM treatment. One study reported that the rational use of TCM+WM could reduce mortality in COVID-19 patients with critical illnesses and shorten the length of hospital stay. 23 In one case report, all symptoms resolved using a combination of WM and Shuanghuanglian oral liquid (SHL, containing Lonicerae Japonicae Flos, Scutellariae Radix, and Forsythiae Fructus). 24 However, due to the complex compositions of SHL and the possible herb/drug interactions in different individuals, TCM may have adverse effects such as diarrhea, vomiting, and renal toxicity. 25,26 Consequently, the safety of TCM needs to be carefully assessed. A critical analysis of effects would be useful to confirm the safety and efficacy of TCM. The purpose of the present review is to summarize the available evidence on the effects of TCM as auxiliary treatment for COVID-19.
Methods
The authors followed the PRISMA (preferred reporting items for systematic reviews and meta-analysis) guidelines in conducting this review. 27 The study protocol was registered with PROSPERO (CRD42020178684) before data extraction.
Search strategy
Four English databases (Web of Science, PubMed, Embase, and Cochrane Central Register of Controlled Trials [CENTRAL]) and three Chinese databases (China National Knowledge Infrastructure [CNKI], Wanfang, and SinoMed) were searched from December 1, 2019, to June 30, 2020. In addition, the authors searched clinical trials registries for ongoing or recently completed trials (ClinicalTrials.gov, Chinese Clinical Trial Register [ChiCTR], and the World Health Organization International Clinical Trials Registry and Platform [WHO ICTRP]) during this period. The authors also scanned conference proceedings and reference lists of review articles related to the treatment of COVID-19 with TCM in addition to WM. A combination of key terms and/or subject headings in English or Chinese was applied. Duplicates were electronically removed using the EndNote de-duplicate function before review of abstracts (see Supplementary Appendix A1 for the complete set of search terms used in each electronic database). As an example, the search strategy used with PubMed is presented below.
#1 “Medicine, Chinese Traditional”[Mesh]
#2 “Drugs, Chinese Herbal”[Mesh]
#3 “Medicine, East Asian Traditional”[Mesh]
#4 “Chinese herb*”[Title/Abstract] OR “Oriental Medicine”[Title/Abstract] OR “Complementary Medicine”[Title/Abstract]
#5 #1 OR #2 OR #3 OR #4
#6 “COVID-19”[Title/Abstract] OR “2019-nCoV”[Title/Abstract] OR “SARS-CoV-2”[Title/Abstract] OR “coronavirus disease 2019”[Title/Abstract] OR “novel coronavirus pneumonia”[Title/Abstract] OR “NCP”[Title/Abstract]
#7 #5 AND #6
Inclusion/exclusion criteria
Participants
All patients confirmed with COVID-19 were included, 28 regardless of age, gender, and course and severity of the disease. Confirmed cases were those with laboratory confirmation of COVID-19 infection, irrespective of clinical signs and symptoms. 29 Asymptomatic cases were therefore considered eligible for this review. Patients were excluded if they used TCM for other chronic diseases, or were in convalescence after recovery from COVID-19.
Interventions and comparators
The authors included randomized-controlled trials (RCTs) comparing TCM in combination with WM with the same WM therapies alone for COVID-19 patients. For purposes of this review, TCM is defined as Chinese herbal medicine, including single herbs, proprietary Chinese medicine, or a compound of several herbs irrespective of preparation (decoction, oral liquid, tablet, capsule, powder, or injection). The mode of drug delivery, dosage, and treatment course and regimen was not restricted. Studies that used acupuncture, moxibustion, acupressure, and other nonpharmaceutical TCM therapies as interventions were excluded. WM treatment in this review includes antivirals and immunotherapy, as well as supportive and symptomatic therapies. They excluded studies if WM treatment regimen in the trial arm was not the same as that used in the control arm.
Outcomes
The primary outcomes were cure rate and relief of fever and cough. Clinical cure was defined as no-detection of SARS-CoV-2 in two successive nasopharyngeal swabs, obvious resolution of inflammatory infiltrates on chest computed tomography (CT) images, body temperature normalization (≤37.2°C for axillary temperature) for more than 3 days, and significantly improved respiratory symptoms. 28 Data on relief of fever and cough included the number of patients (dichotomous data), time to recovery (continuous data), and symptom score (continuous data). The symptom score was defined as the score of common TCM clinical symptoms, which can be scored as 1 point (no symptom), 2 points (mild), 4 points (moderate), or 6 points (severe), 30 or scored ranging from 0 to 3 points based on the severity of symptoms. 31
Secondary outcomes were chest CT image improvement, deterioration of clinical condition, and adverse effects, all of which were dichotomous. Improvement in chest CT images was defined as a more than 30% decrease in the volume of pulmonary inflammatory infiltrates after treatment. 32 Deterioration of condition was defined as a transition of the severity of the patients' condition from mild or moderate to severe or critical. 28 An adverse effect was defined as a composite outcome, including diarrhea, vomiting, and liver damage and/or kidney dysfunction following treatment.
Although there was no limit on the duration of treatment, the follow-up time was at least one course of TCM treatment. Data as of the last follow-up were chosen for analysis if there were more than two time points for outcome ascertainment.
Study types
RCTs written either in Chinese or English were included. Case reports, observational studies, abstracts, interviews, commentaries, reviews, book chapters, or animal experiments were excluded.
Study selection
Titles and abstracts of the retrieved articles were evaluated independently by two reviewers (L.P.Z. and J.W.). Abstracts that did not provide sufficient information regarding the eligibility criteria were retained for full-text evaluation. Two reviewers (L.P.Z. and J.W.) independently evaluated full texts and determined study eligibility based on the inclusion criteria. Any discrepancies between the two reviewers were resolved by discussion with a third independent reviewer (R.H.X.).
Risk of bias
Studies were assessed independently by the two reviewers (L.P.Z. and J.W.) for methodological validity using the risk-of-bias (ROB) assessment tool from the Cochrane Handbook. 33 Any disagreements with respect to validity were resolved by the third reviewer (R.H.X.).
Data extraction
Two investigators (L.P.Z. and J.W.) independently extracted relevant data from eligible articles using standard forms. The following data were recorded from each eligible study: last name of the first author, publication year, type of study participants, sample size, age and gender of study participants, intervention, control, and courses and outcomes of treatment. Any disagreements between the two reviewers (L.P.Z. and J.W.) were resolved by the third independent reviewer (R.H.X.).
Data synthesis
Measures of treatment effect
Meta-analyses based on a random effects model implemented using RevMan 5.3 software were conducted if more than two included studies assessed the same outcome. The mean differences (MDs) and 95% confidence intervals (CIs) were calculated for continuous outcomes, and the risk ratios (RRs) calculated for dichotomous outcomes.
Assessment of heterogeneity
The authors carried out a chi 2 test for heterogeneity with significance set at p < 0.10, and applied the I2 statistic with significance set at ≥50%. Data permitting, subgroup, and sensitivity analyses were conducted to assess possible sources of heterogeneity.
Assessment of reporting bias
The potential publication bias was not conducted using funnel plots because <10 trials for any one outcome were identified. 34
Subgroup analysis
The authors conducted a subgroup analysis on disease severity in consideration of clinical or methodological heterogeneity.
Sensitivity analysis
The authors performed a sensitivity analysis using a fixed-effects model for the synthesized data to evaluate whether it alters the significance of the results in comparison with a random effects model. They also sequentially removed each study from the analysis to explore the influence of individual studies on the stability and strength of the overall results.
Quality of evidence
The quality of evidence was classified into one of four categories: high, moderate, low, or very low using the grading of recommendation, assessment, development, and evaluation (GRADE) method implemented in GRADEpro GDT software. 33,35 To evaluate imprecision, the authors first calculated the optimal information size (OIS) using the online calculators based on a 5% type I error rate (α) and 80% power with a two-tailed test. High certainty indicates high confidence that the estimate of effect reflects the true effect, while very low certainty indicates that evidence is either unavailable or does not permit a conclusion. Discrepancies in certainty of evidence ratings were resolved by group discussion.
Results
Search results
These search strategies yielded 2,186 potentially relevant citations from the seven electronic databases searched. After excluding duplicates and screening titles and abstracts for eligibility, 13 publications were retained for full-text evaluation. Of these 13 studies, three studies were excluded due to lack of information about the effect of TCM treatment (Supplementary Appendix A2). A total of nine Chinese publications 36 –44 and one English publication 45 were included in the final analysis in this systematic review (Fig. 1). Eighteen ongoing RCTs from three clinical trials registries that were eligible for further review are summarized in Supplementary Appendix Table A1.
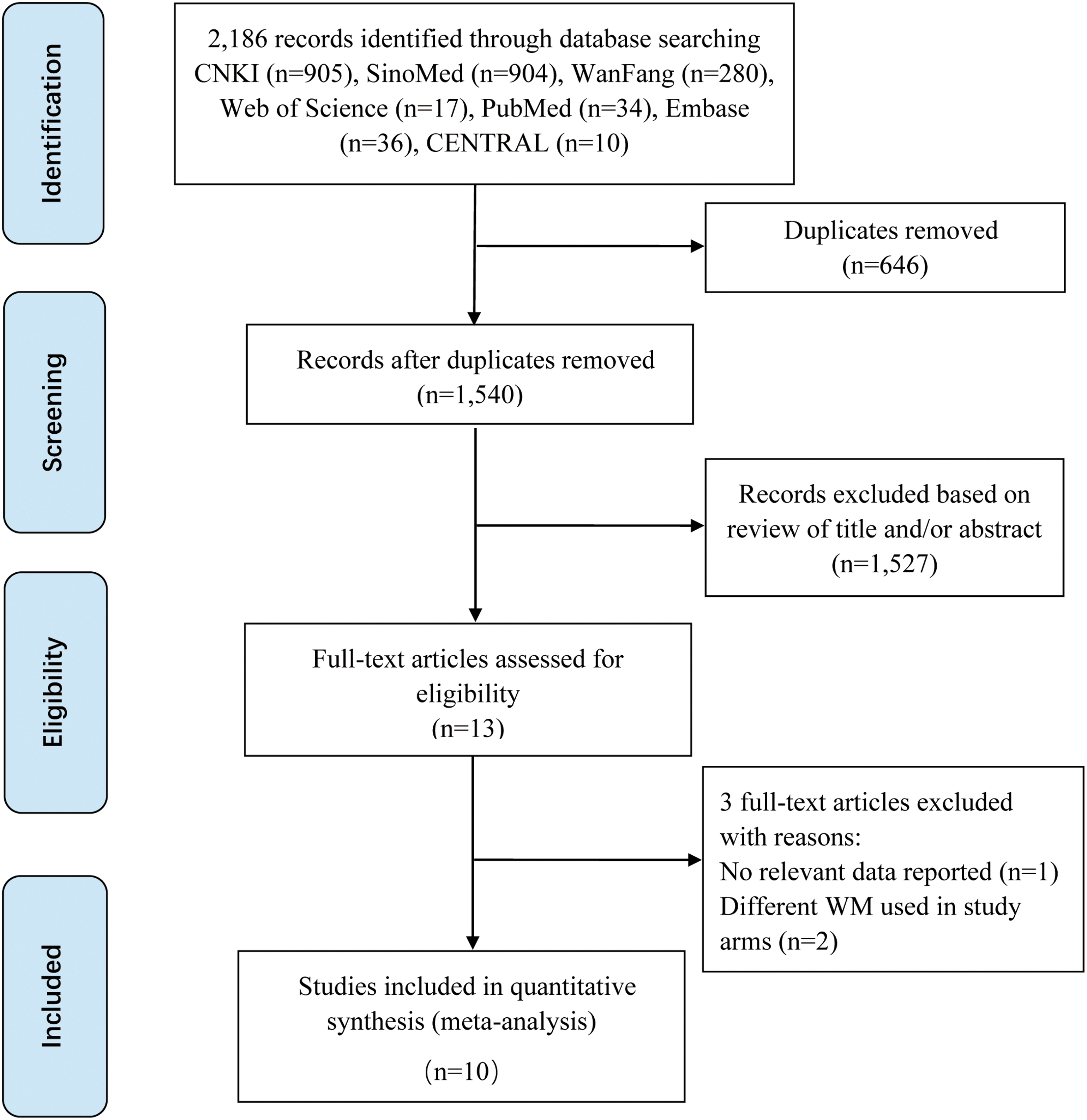
Study flow diagram.
Description of included studies
The 10 eligible studies included in this review were all published in 2020 and conducted in China. All included studies compared TCM+WM with WM alone. Included sample sizes ranged from 57 to 284, with a total of 1,285 COVID-19 patients. The course of treatment ranged from 5 to 14 days. The characteristics of the included studies are shown in Table 1.
Characteristics of 10 Included Randomized-Controlled Trials
Outcome measures include: ① cure rate; ② improvement in chest CT images; ③ lowering body temperature; ④ relieving cough; ⑤ deterioration of condition; ⑥ adverse effects.
CT, computed tomography; I/C, intervention group (TCM+WM group)/control group (WM group); MD, mean difference; M/F, male/female; N/A, not available; RCT, randomized-controlled trial; RR, risk ratio; TCM, Traditional Chinese Medicine; WM, Western medicine therapy (medications for antiviral, anti-infection, oxygen inhalation, symptomatic supportive treatments, and so on).
Four formulations, including granule, capsule, decoction, and oral liquid of TCM, were included in this review. The top 5 ranked Chinese herbs used in the eligible studies of this review were Lianqiao (Fructus Forsythia Suspensae), Jinyinhua (Flos Lonicerae), Shigao (Gypsum Fibrosum), Mahuang (Herba Ephedrae), and Kuxingren (Semen Armeniacae Amarum). Compositions of TCM used in the included studies are presented in Supplementary Appendix Table A2. The WM treatments included in this review were medications taken for antiviral, anti-infection, oxygen inhalation, and symptomatic supportive treatments. Lopinavir, ritonavir, and arbidol were the top 3 common antiviral medicines; quinolone antibacterial agent and cephalosporin were the most common anti-infection medications used in the WM treatments.
Risk of bias
Supplementary Appendix Figure A1 summarizes the risk of bias of the 10 RCTs included in this review. Only eight RCTs 36 –40,43 –45 adequately described the random sequence generation method. Three RCTs 36,37,45 described an appropriate method of allocation concealment. Blinding for patients and work staff was not clearly defined in two studies, 39,45 and was not mentioned in the remaining RCTs. Only two RCTs 36,45 used blinded outcome assessors and only three RCTs 36,37,45 provided details regarding dropouts. Selective outcome reporting was judged as an unclear risk in all the included studies, due to limitations in available information on the study protocol. The risk of other possible biases was considered unclear for one study, on the grounds of having no comparable information at baseline.
Effect of TCM on COVID-19
Cure rate
Of the 10 studies included in this review, 6 studies 37,38,42 –45 presented the cure rate. Compared with WM alone, the combined use of TCM and WM may increase the cure rate (RR 1.15 [95% CI 1.04–1.26]; I 2 = 60%; Fig. 2) in the treatment of COVID-19 with low certainty based on GRADE.

Cure rate in the TCM+WM group versus the WM alone group. TCM, Traditional Chinese Medicine; WM, Western medicine.
Lowering body temperature
Nine studies 36 –42,44 reported results of lowering body temperature. One of these studies 45 showed time to recovery for fever, two studies 38,44 presented score of common TCM clinical symptoms, and six studies 36,37,39 –42 reported number of patients with lowered body temperature after treatment with TCM+WM, compared with WM alone. Time to recovery for fever in the TCM+WM group was significantly shorter (MD −1.00 [95% CI −1.17 to −0.83]). Fever scores were significantly reduced by TCM+WM, 38,44 according to both the 2002 (MD −0.56 [95% CI −0.62 to −0.50]) 31 and 2010 (MD −0.50 [95% CI −0.72 to −0.28]) 30 versions of scoring methods. A meta-analysis of patients with fever disappearance (RR 1.10 [95% CI 0.94–1.29]; I 2 = 85%; Fig. 3) indicated it is unclear whether TCM+WM was superior to WM alone (very low certainty based on GRADE).
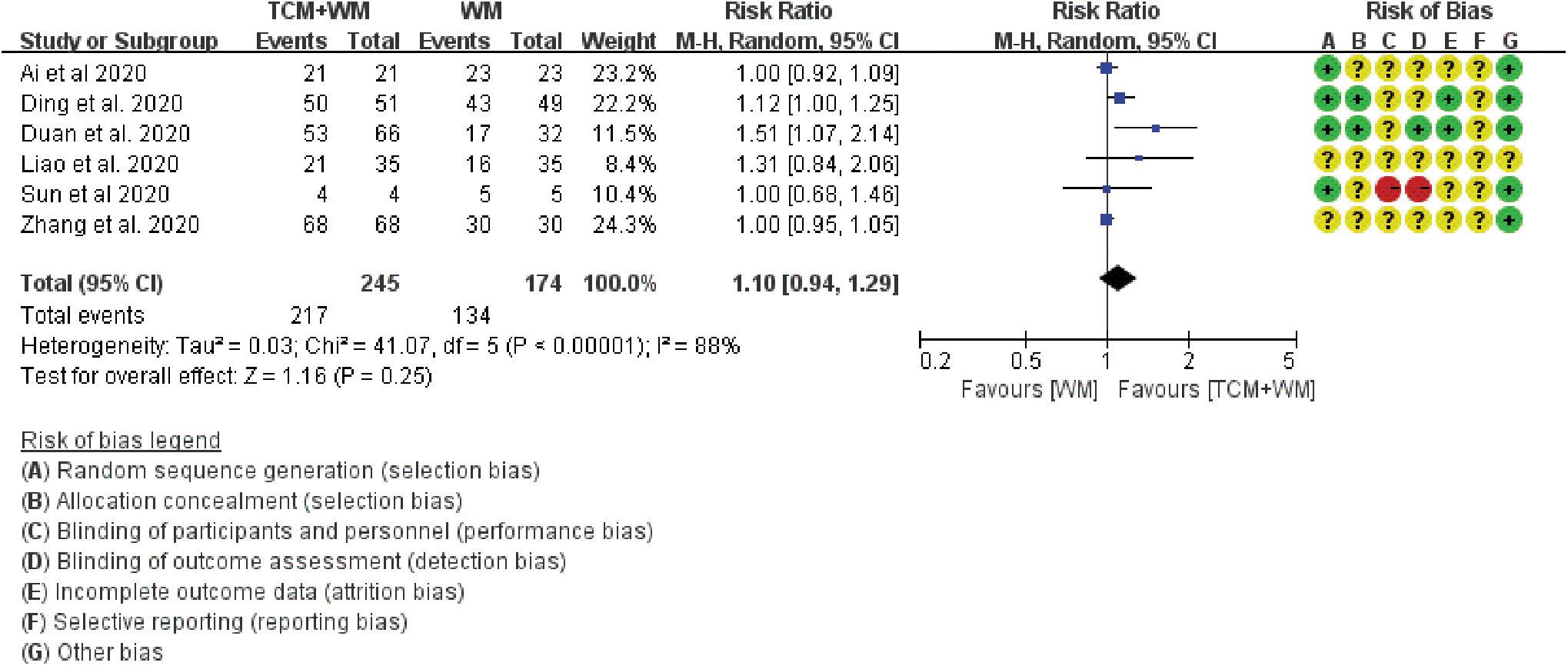
Number of patients with lowered body temperature in the TCM+WM group versus the WM-alone group.
Relieving cough
Nine studies 36 –42,44 evaluated cough relief. In six of these studies, 36,37,39 –42 patients experienced greater relief of cough in the TCM+WM group than in the WM-alone group (moderate certainty based on GRADE) (RR 1.32 [95% CI 1.15–1.52]; I 2 = 0%; Fig. 4). In one study, 45 time to cough relief was shorter with TCM+WM than with WM alone (MD −3.71 [95% CI −4.06 to −3.36]). Two studies 38,44 presented score for cough using different scoring guidelines, showing a beneficial effect of combined therapy on cough (MD −1.17 [95% CI −1.29 to −1.05] and MD −1.03 [95% CI −1.20 to −0.86], respectively).
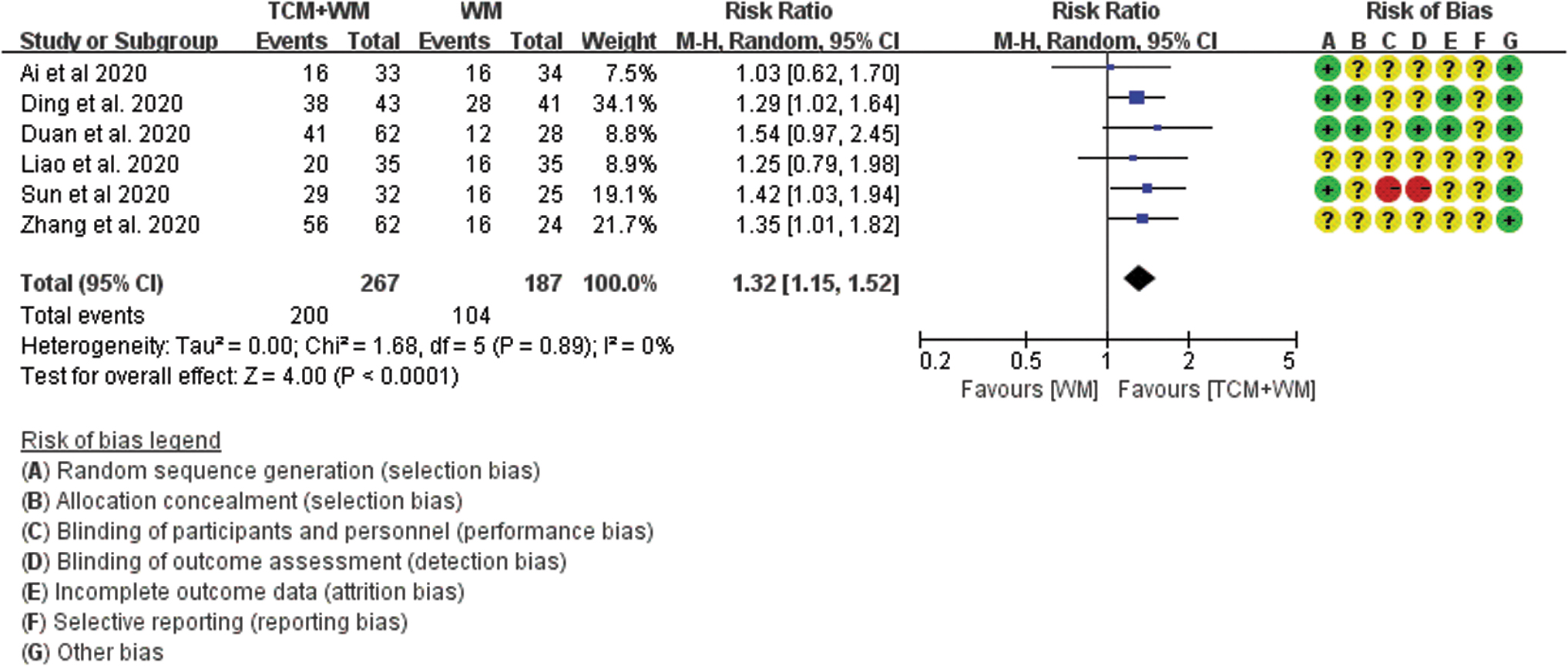
Number of patients with cough relieved in the TCM+WM group versus the WM-alone group.
Improvement in chest CT images
Five studies presented data on improvement of chest CT images. 37,41,42,44,45 Of these, one study 42 showed a decrease in chest imaging scores (MD 1.97 [95% CI 1.34–2.60]), and four studies 37,41,44,45 reported a number of improved chest CT images. A meta-analysis of the number of improvements in chest CT images (RR 1.23 [95% CI 1.11–1.37]; I 2 = 5%; Supplementary Appendix Fig. A2) suggested a probably positive effect of TCM+WM on the resolution of inflammatory infiltrates on chest CT images compared with WM alone (moderate certainty based on GRADE).
Deterioration of condition
Six studies 36,38,39,42 –44 reported on number of cases transitioning from moderate to severe disease. Transition to greater severity in the TCM+WM group appeared to be less than in the WM-alone group (RR 0.58 [95% CI 0.43–0.77]; I 2 = 0%; Supplementary Appendix Fig. A3) (moderate certainty based on GRADE).
Adverse effects
Nine studies 36 –38,40 –45 described the occurrence of adverse reactions, of which three studies 38,40,44 reported no obvious adverse effect, and six studies 36,37,41 –43,45 provided data on adverse effects. There were 108 (25.2%) patients in the TCM+WM group and 104 (29.5%) in the WM-alone group who experienced adverse effects, with abnormal liver function (14.3% vs. 18.1%) and diarrhea (11.4% vs. 8.2%) being the most commonly observed adverse events. The occurrence of any adverse effect was used as a composite outcome for meta-analysis; however, no difference in the rate of occurrence of adverse effects was found between TCM+WM and WM alone (RR 0.81 [95% CI 0.42–1.57]; I 2 = 56%; Supplementary Appendix Fig. A4). The authors are uncertain whether TCM+WM reduced adverse effects compared with WM alone (very low certainty based on GRADE).
Sensitivity analysis
Using a fixed-effects model for meta-analysis, a pooled estimate of the relative rate of lowering body temperature favored the TCM+WM group (RR 1.15 [95% CI 1.03–1.28]; I 2 = 85%). All pooled estimates were consistent when excluding one study at a time. After excluding the trial by Duan et al. 36 when analyzing the occurrence of an adverse effect as an outcome, the overall result was unchanged (RR 0.80 [95% CI 0.64–1.00]; Supplementary Appendix Fig. A5), although heterogeneity was much smaller (p = 0.49, I 2 = 0%).
Subgroup analysis
The authors performed a subgroup analysis to evaluate the influence of severity of disease on cure rate between TCM+WM and WM-alone groups. There was little evidence of heterogeneity among trials in the mild/moderate plus severe/critical case group (RR 2.59 [95% CI 1.30–5.19]; I 2 = 0%; Supplementary Appendix Fig. A6) and mild/moderate group (RR 2.32 [95% CI 1.55–3.46]; I 2 = 0%; Supplementary Appendix Fig. A6), suggesting that severity of disease was the main cause for heterogeneity in cure rate. Moreover, results of subgroup analysis for cure rate were similar to the results of this meta-analysis of all eligible studies.
Certainty of evidence
All observed sample sizes used in the meta-analysis were larger than OIS (Supplementary Appendix Table A3). Using GRADE, the authors rated the evidence for primary review outcomes of improvement in chest CT images, cough relief, and deterioration of disease as “moderate certainty,” cure rate as “low certainty,” and lowering body temperature and adverse effects as “very low certainty.” A summary of the certainty of evidence in this review is presented in Table 2.
Summary OF Quality of the Evidence in This Review
GRADE Working Group grades of evidence. High certainty: the authors are very confident that the true effect lies close to that of the estimate of the effect. Moderate certainty: the authors are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different. Low certainty: the authors' confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect. Very low certainty: the authors have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect.
The risk in the intervention group (and its 95% CI) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
Quality was downgraded due to risk of bias and inconsistency (substantial heterogeneity).
Quality was downgraded due to risk of bias, inconsistency (substantial heterogeneity), and imprecision (the 95% CI includes both no effect).
Quality was downgraded due to risk of bias.
Quality was downgraded due to risk of bias.
Quality was downgraded due to risk of bias.
Quality was downgraded due to risk of bias, inconsistency (substantial heterogeneity), and imprecision (wide CIs and the 95% CI include both no effect).
CI, confidence interval; COVID-19, coronavirus disease 2019; GRADE, grading of recommendation, assessment, development, and evaluation.
Discussion
Main findings
In this study, the authors assessed the effects of TCM combined with WM compared with WM alone in the treatment of COVID-19, with a systematic review of available literature on this topic. Although TCM combined with WM has an uncertain effect on lowering body temperature, and adverse effects compared with WM alone, these findings indicated that TCM combined WM is likely to have beneficial effects on the overall cure rate, chest CT images, symptoms of cough, and disease progression compared with WM alone in the treatment of COVID-19 patients. Since current WM practice is one of providing COVID-19 patients with supportive treatment, TCM is considered an auxiliary treatment in the RCTs included in this review.
Strengths and limitations
To the best of knowledge, this is the first comprehensive systematic review/meta-analysis focusing on both Chinese and English literature of RCTs that assessed the effects of TCM as an auxiliary treatment for COVID-19. By including only RCTs, this review provides a relatively high degree of evidence that TCM could be effective and safe in the treatment of COVID-19. The results of subgroup and sensitivity analyses suggest a high degree of robustness in this study findings.
There are several limitations to this systematic review. First, the quality of included 10 RCTs was not high according to the Cochrane Review Manual. Only two RCTs 36,45 used appropriate blinding methods and none reported adequate blinding of treatment outcomes. Second, subgroup analysis to assess heterogeneity in lowering body temperature was challenging due to lack of information Third, this review only included English and Chinese language articles, which may increase the risk of publication bias. Fourth, as symptom recovery time and length of hospital stay were not reported in included studies, these outcomes could not be assessed. Finally, different herbs/formulae were used in the 10 included studies. As a result, it is difficult to isolate the specific substance(s) that may be the critical determinant(s) of the efficacy of TCM. On the contrary, unlike WM, many TCMs are not targeted to a specific organ or a specific pathogen. Most of the herbs/formulae included in the 10 trials have been extensively used historically for other patient populations, and the safety of these herbs/formulae evaluated in numerous previous clinical studies.
Interpretation
This systematic review summarizes currently available evidence on TCM as an auxiliary treatment for COVID-19, in conjunction with WM. Findings suggest that TCM plus WM could lead to improved outcomes in COVID-19 patients compared with WM alone. These findings are consistent with a previous systematic review that comprised four RCTs and seven case/control studies with a total sample size of 982 patients, which reported that the clinical cure rate RR for TCM+WM compared with WM alone in treating COVID-19 was 1.60 (95% CI 1.18–2.12), suggesting that TCM is useful in the treatment of COVID-19. 46 However, the previous review included case/control studies, which may introduce bias into the meta-analysis.
In the present study, the authors are uncertain whether TCM+WM is effective in lowering the body temperature of COVID-19 patients, compared with WM alone, as the certainty of the evidence has been assessed as very low, which is different from other systematic reviews that included observational studies. 46,47 Previous studies 48,49 suggested that the median antifebrile onset time for TCM was shorter than for WM, although the difference was not statistically significant for recovery time and disappearance rate. Hence, time to fever recovery should be reported in future studies. They were unable to identify the reasons for high heterogeneity in studies on lowering body temperature. Differences in sample sizes, number of treatment courses, and quality of RCTs may influence heterogeneity. It was difficult to conduct informative subgroup analysis to explore heterogeneity from these aspects because of insufficient information. Finally, because repeating meta-analysis of lowering body temperature with a fixed-effects model produced inconsistent results compared with a random-effects model, results on lowering body temperature in this review should be interpreted with caution.
The authors are also uncertain if TCM+WM reduces adverse effects compared with WM alone, because of the very low certainty of the evidence conferred by very serious imprecision (the 95% CI for adverse effects includes both appreciable benefit and appreciable harm) and a serious risk of bias. The studies 36,37,41 –43,45 on adverse effects also demonstrated significant heterogeneity, which was largely attributable to the study by Duan et al. 36 This may be due to the large doses of Jinhua Qinggan granule, which is cold in nature and could easily result in diarrhea, 50 as given in Duan's study. Furthermore, cases in Duan's study had predominantly mild symptoms, while cases from other studies included patients with moderate or severe symptoms. 37,41 –43,45 Excluding Duan's study did substantially reduce heterogeneity, although the overall results remained similar.
COVID-19 can cause a strong immune response and inflammatory storm. 51 In contrast to WM, TCM has an overall multicomponent, multipathway, and multitarget regulatory function, 52 and can protect against COVID-19 injury via anti-inflammatory, antioxidant, and antiapoptotic effects through a holistic treatment approach. 53 TCM can inhibit the replication of COVID-19 and reduce cytokine release from host cells by acting on multiple ribosomal proteins. 54 There is compelling evidence that TCM combined with WM can inhibit and alleviate excessive immune response and eliminate inflammation by regulating immune- and cytokine-related pathways, 55,56 resulting in relief of clinical symptoms of COVID-19. Studies have reported on the chemical composition and pharmacologic mechanisms of Qingfei Paidu decoction (QFPD) and Lianhua Qingwen in treating COVID-19. 57,58
However, adverse effects may be associated with the use of TCM in treatment of COVID-19. Studies have shown that some TCMs contain nephrotoxins and mutagens, 59,60 and the toxicologic features of some TCM treatments remain to be fully understood, raising concerns that TCM may present some risks. In the present review, six studies 36,37,41 –43,45 reported that some cases had diarrhea and vomiting due to intolerance of TCM. These adverse effects, while frequently observed in patients treated by TCM, are not life-threatening and often mild. If TCM can benefit patients with COVID-19, a disease that is often severe or even life-threatening, these low-risk adverse effects may be tolerable by patients.
Clinical implications
Based on the evidence synthesized here, there is moderate certainty in the evidence that the use of TCM combined with WM is likely to improve chest CT images, relieve cough, and reduce deterioration rate compared with WM alone, suggesting that TCM has an auxiliary effect in treating COVID-19. Although the certainty of evidence for fever relief and adverse effects was very low, this does not mean that TCM is ineffective, but rather that the lack of evidence makes it difficult to draw definitive conclusions on these outcomes. It should be noted that no attempt was made in this systematic review to define minimally important differences. What is a small or even trivial effect in one context may be a large effect in another context. 61,62 Given the complexity in TCM formulation, with inherent difficulties to isolate a specific effect on a specific organ or a specific system, and the lack of an effective treatment specifically targeting COVID-19, the authors consider any improvement in clinical outcomes important.
Research implications
Further rigorous RCTs on TCM for the treatment of COVID-19 are needed to provide stronger evidence of the benefits of TCM used in conjunction with WM. To optimize the effect of TCM in the treatment of COVID-19, the design, quality, and reporting of RCTs should be improved, especially with respect to randomization of patients to treatment arms and concealment of the randomization sequence. Although blinding patients for treatment with TCM may be difficult, blinding of health care providers, outcome assessors, and analysts should be feasible. Future studies should consider assessing the effects of TCM on COVID-19 patients with different severity of symptoms, as the effects of treatment may vary with severity. Future studies should examine the effect of specific components of TCM and elucidate the biologic mechanisms underlying the therapeutic effects of TCM in the treatment of COVID-19.
Conclusion
The results of this systematic review suggest that TCM as an auxiliary treatment is likely to help improve the main symptoms of COVID-10, and inhibit disease progression. However, due to the limited number of high-quality studies and the high degree of heterogeneity among currently available studies, a more definitive conclusion on the effects of TCM on lowering body temperature and adverse effects cannot be drawn at this time. Large and rigorous multicenter trials are needed to confirm the efficacy and safety of TCM as an auxiliary treatment for COVID-19.
Footnotes
Authors' Contributions
L.P.Z. and J.W. drafted this review. R.H.X. made substantial contributions to the conception and design of the review. L.P.Z. and J.W. participated in the acquisition of the data, the analysis, and interpretation of the data. R.H.X., S.P., D.K., D.W.C., and S.W.W. revised the article critically for important intellectual content. R.H.X. approved the version of the article to be published.
Ethical Approval
This article is a review article and does not involve a research protocol requiring approval by the relevant institutional review board or ethics committee.
Acknowledgments
The authors thank all the authors and participants of the eligible articles.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported, in part, by grants from the Canadian Institute of Health Research (FND-148438), Clinical Research Startup Program of Southern Medical University by High-level University Construction Funding of Guangdong Provincial Department of Education (LC2019ZD019), and Foshan Special Project of Emergency Science and Technology Response to COVID-19 (2020001000376). D.K. is the Natural Sciences and Engineering Research Council of Canada Chair in Risk Science at the University of Ottawa.
Supplementary Material
Supplementary Appendix Figure S1
Supplementary Appendix Figure S2
Supplementary Appendix Figure S3
Supplementary Appendix Figure S4
Supplementary Appendix Figure S5
Supplementary Appendix Figure S6
Supplementary Appendix SA1
Supplementary Appendix SA2
Supplementary Appendix Table S1
Supplementary Appendix Table S2
Supplementary Appendix Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.