
Abstract
Background:
Fibromyalgia (FMS) is a complex condition that is characterized by various pain syndromes and fatigue, among other symptoms experienced. Current medical treatment of FMS involves both pharmacological and nonpharmacological approaches, but often with ineffective outcomes. Medicinal cannabis has the potential to be a therapeutic option for patients with FMS due to the positive research in chronic pain management. In addition, it has been found to have fewer adverse effects compared with currently available pain medications. This literature review aims at answering whether medicinal cannabis is reported to be safe and effective for the treatment of pain and symptomology experienced by people with FMS.
Methods:
A systematic review was conducted on human trials utilizing cannabis in FMS. MEDLINE, Embase, CINAHL, AMED, Scopus, and Cochrane CENTRAL were used for databases search, and mesh terms were used for cannabis and FMS. The search was limited to studies conducted from 2000 to 2020.
Results:
From the 181 citations identified, 10 studies were included after title, abstract, and full text screening occurred. A total of 1136 of patients (intervention n = 945, control n = 108, crossover n = 83) participated in the 10 studies ranging from 9 to 383 patients (mean = 114, median = 36). Of these studies, there were three randomized controlled trials, six observational studies, and one study that compared the management of chronic pain patients with FMS patients. Cannabis was found to be safe and well tolerated in FMS. The main adverse events identified included feeling “high,” dizziness/vertigo, dry mouth, cough, red eyes, and drowsiness with no serious adverse events reported.
Conclusions:
This literature review identified that medical cannabis may be beneficial for some people with FMS. Further studies are required to confirm its efficacy, what type of cannabis is the most effective form to use, and what assessment tools need to be utilized to understand how to quantify clinical outcomes.
Introduction
Fibromyalgia (FMS)
FMS is a complex condition involving a number of potential risk factors and pathophysiological mechanisms. Multiple genetic polymorphisms affecting pain transmission and processing through the serotoninergic, catecholaminergic, and dopaminergic mechanisms have been found to play an important role in the etiology of FMS. 6 Moreover, environmental factors such as physical and psychological trauma, daily distress, and various infections (e.g., Epstein–Barr virus, Lyme disease, brucellosis, hepatitis C) may trigger FMS in genetically predisposed individuals. 7 –10 Central sensitization and abnormal pain modulation appears to be the main underlying mechanism causing hypersensitivity to painful stimuli and reduced descending pain inhibition. 11 Research suggests that patients with FMS may have impaired pain processing potentially due to alterations in functional connectivity and levels of inhibitory and excitatory neurotransmitter concentrations in the pain-processing regions of the brain. 8
Current medical treatment of FMS involves both pharmacological and nonpharmacological approaches aiming at improving symptoms, function, and quality of life. 12 Nonpharmacological options include exercise, cognitive behavioral therapy, and education. 13 Several pharmacological agents have shown various effectiveness in the management of FMS, such as amitriptyline (tricyclic antidepressant), pregabalin (anticonvulsant), duloxetine, milnacipran (serotonin-noradrenaline reuptake inhibitors), and tramadol (weak opioid with mild serotonin-noradrenaline reuptake inhibition). 14,15 However, the majority of these drugs have been found to provide only modest benefits and are often associated with adverse effects (AEs), which may compromise compliance. 14
Medicinal cannabis is defined as a product made in a Good Manufacturing Practice facility and considered to be of pharmaceutical grade, legal and standardized to delta-9-tetrahydrocannabinol (THC) and cannabidiol (CBD) amounts. 16 This review does not consider any research into other products or compounds acting on the endocannabinoid system (ECS). Medicinal cannabis could be a therapeutic option for FMS patients due to its potential effectiveness for chronic pain management. 16 In addition, it has been found to have fewer AEs compared with currently available pain medications. 17 Current literature has found that medicinal cannabis use has been associated with lower opioid consumption and improved quality of life in patients with chronic pain. 18
There are two types of cannabinoid-containing products on the market, plant-based (cannabis) and isolated compounds. Cannabis spp. of the Cannabaceae family are natural sources of terpenophenolic compounds known as cannabinoids, of which THC and CBD are the most studied. 19 –21 In addition to THC and CBD, plant-based cannabis contains many other cannabinoid and non-cannabinoid molecules such as terpenes. 20,21 The synergistic interplay of the plant compounds, called the entourage effect, has been found to be beneficial. 22 Both plant-derived cannabinoids and isolated compounds have been found to be promising treatment options for general chronic pain management. 20
The ECS is one of the key endogenous systems playing an important role in various physiological functions, including modulation of pain, inflammation, and cognitive and neurological function. 23 Humans and other mammals produce endogenous cannabinoids that are called endocannabinoids. 20 The ECS consists of cannabinoid receptors 1 and 2 (CB1 and CB2) and endogenous cannabinoid receptor ligands (endocannabinoids). CB1 are primarily expressed in the brain and, in lesser amounts, in the peripheral tissues, whereas CB2 are mainly present in immune cells and tissues. 24 THC, the main psychoactive constituent in cannabis, activates CB1 and CB2. It induces central and peripheral neuronal activity and is responsible for analgesic and psychotropic effects of cannabis. 25 CBD, the major nonintoxicating constituent in cannabis, does not bind to these receptors; however, it may potentiate analgesic effects and decrease psychotropic effects of THC and possess anxiolytic, antipsychotic, anti-inflammatory, anti-epileptic, anti-ischemic, and anti-emetic properties. 25,26
It has been hypothesized that cannabinoids may alter pain processing, reduce low-grade inflammation, enable modulation of emotional and cognitive function, and buffer stress in FMS patients. 27 In addition, endocannabinoid deficiency has been theorized as a possible cause for chronic pain conditions, including FMS. 28 The complexity of FMS symptoms should be taken into consideration. Due to the complex pathophysiology and lack of effective treatment options, the potential of engaging the ECS to provide therapeutic effects for the condition is attractive. The objective of this review is to assess current evidence on medicinal cannabis for FMS to evaluate safety and efficacy of its use in the treatment of the disease.
Materials and Methods
Research question: Is medicinal cannabis safe and effective for the treatment of pain and symptomology experienced by people with FMS?
Inclusion criteria
Types of studies
All peer-reviewed original research with or without control groups, including randomized controlled trials (RCTs), non-RCTs, quasi-experiments, before and after studies, observational studies, prospective and retrospective cohort studies, case control studies, and analytical cross-sectional studies, were included if they fulfilled the pre-specified criteria. Systematic reviews and meta-analyses, and studies published before 2000 were excluded.
Registration
Registered with PROSPERO 2020 CRD42020165389.
Types of participants
Participants of any age, with any form of FMS were included.
Types of intervention
Any formulation of cannabis products (plant-based or synthetic) at any dose, by any route, was administered for the relief of FMS symptoms with or without co-medication.
Types of outcome measures
Primary outcomes: - Patient-reported health effects - AEs - Quality of life
Secondary outcomes:
- Patterns of cannabis use: product, route of administration, co-medication, and medication stopped or reduced during cannabis treatment.
Search strategy
The following sources were used to identify relevant studies:
MEDLINE (PubMed)
Embase (Ovid)
CINAHL (EBSCOhost)
AMED (EBSCOhost)
Scopus (Elsevier)
CENTRAL (Cochrane)
Search terms:
MeSH terms: [cannabis]
(cannabis OR hemp OR hemp plant OR marijuana OR ganja OR hashish OR marihuana OR bhang OR marinol OR dronabinol OR nabilone OR cesamet OR dexanabinol OR sativex OR tetrahydrocannabinol)
MeSH terms: [fibromyalgia]
(fibromyalgia OR fibrositis OR fibromyalgi* OR fms)
1 OR 2
3 OR 4
5 AND 6
The searches were limited to studies published from 2000 to 2020. The year 2000 was chosen as the beginning of this review, as very little research regarding cannabis and FMS was found before this date. A gray search was conducted that reviewed the bibliographies of the review articles and randomized trials identified during the search to identify additional peer-reviewed studies. No search strategy was used for nonsynthetic cannabis formulations, nor other cannabinoids or terpenes as clinical trial research for these products and compounds is limited.
Selection of studies
I.K. conducted the search with search results combined and stored them in an Endnote Library. Duplicates were identified and deleted. Studies were then analyzed by screening via titles and then abstracts. Studies that clearly did not satisfy the inclusion criteria were eliminated, and full texts of the remaining studies were obtained. After reading full texts, an agreement was reached between two review authors (I.K., J.S.) on a final selection of studies. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow chart was used to present study selection activities (Fig. 1).

Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram for Medicinal Cannabis and Fibromyalgia literature review.
Data extraction
The data extracted from the studies included specific details about study design, number of participants, interventions and study methods, outcome measures, and results specific to this review objectives. Data were extracted by I.K. and reviewed by J.S. The final selection was reviewed by J.S. and E.T.
Critical appraisal
The review included observational studies and RCTs. The RCTs were evaluated by using the Joanna Briggs Institute (JBI) critical appraisal checklist for RCTs to appraise the methodological qualities of the studies. 29
Results
The initial search identified 182 citations, which included 181 citations from the database search and 1 citation from the gray literature. After title, abstract, and full text screening, a total of 10 studies were eligible and included in this review. See PRISMA diagram in Figure 1 (Refs. 30 –39 ).
Descriptions of studies
The characteristics of included studies are presented in Table 1. The 10 studies included three RCTs 33,35,36 and one small pilot study without controls. 37 All RCTs were double blinded, two of which were crossover trials. 33,35 The remaining six studies were observational, two of which had control groups, 38,39 three were without controls, 31,32,34 and one was a crossover study. 30
Characteristics of Included Studies
CBD, cannabidiol; CC, cannabis consumers; FIQ, fibromyalgia impact questionnaire; FIQR, revised fibromyalgia impact questionnaire; FMS, fibromyalgia; ISI, Insomnia Severity Index; LBP, low back pain; LSEQ, Leeds Sleep Evaluation Questionnaire; MC, medical cannabis; ODI, Oswestry Disability Index; PDI, Pain Disability Index; PROs, patient reported outcomes; PSQI, Pittsburgh Sleep Quality Index; ROA, route of administration; ROM, range of motion; SAT, standardized analgesic therapy; SF-36, Short Form 36 Health Survey; THC, delta-9-tetrahydrocannabinol
Participants
A total number of 1136 of patients (intervention n = 945, control n = 108, crossover n = 83) participated in the 10 studies ranging from 9 to 383 (mean = 114, median = 36). Six studies (number of participants: n = 304) reported premature withdrawals (n = 68, 22%) 30,31,33,35 –37 due to various reasons, including AEs, noncompliance with study protocols, expenses, insufficient therapy effects, and unknown reasons (Table 2).
Adverse Effects and Withdrawals
AE, adverse effects; FMS, fibromyalgia; MC, medical cannabis; SAT, standardized analgesic therapy; THC, delta-9-tetrahydrocannabinol.
Critical analysis
A JBI critical appraisal checklist for RCTs was used to evaluate the methodological quality of three RCTs selected for inclusion. All RCTs met all but 1 of 13 requirements (92.3%) of the critical analysis criteria. The requirement that the studies did not meet asked “Were the treatment groups treated identically other than the intervention of interest.” The three publications were subject to confounders due to potential differences in concomitant medications during the intervention period. All RCTs were found to be randomized, double blinded, appropriately designed, and analyzed, and they had outcomes measured consistently between treatment groups by using reliable methods (Table 3).
Critical Appraisal Results
[1]: answers: yes, no, unclear (?) or NA.
1. Was true randomization used for assignment of participants to treatment groups?
2. Was allocation to treatment groups concealed?
3. Were treatment groups similar at the baseline?
4. Were participants blind to treatment assignment?
5. Were those delivering treatment blind to treatment assignment?
6. Were outcomes assessors blind to treatment assignment?
7. Were treatment groups treated identically other than the intervention of interest?
8. Was follow-up complete and if not, were differences between groups in terms of their follow-up adequately described and analyzed?
9. Were participants analyzed in the groups to which they were randomized?
10. Were outcomes measured in the same way for treatment groups?
11. Were outcomes measured in a reliable way?
12. Was appropriate statistical analysis used?
13. Was the trial design appropriate, and any deviations from the standard RCT design (individual randomization, parallel groups) accounted for in the conduct and analysis of the trial?
NA, not applicable; RCT, randomized controlled trial.
Type of cannabis and route of administration
All studies reported the type of cannabis used and administration methods (Table 1). Six studies evaluated the effects of plant-based cannabis administered by smoking, eating, vaporization/inhalation, and/or oral drops. 30,32,34,35,38,39 Four studies used synthetic forms of THC—oral dronabinol 31,37 and oral nabilone 33,36 —rather than plant-based forms. Dronabinol (also known as Marinol and Syndros) is a trade name for a synthetic form of THC (oral capsules ranging in strength from 2.4 mg to 10 mg) 31,37 ; Nabilone (trademarked under Cesamet™) is also a synthetic cannabinoid that mimics THC (oral capsules of 0.5 mg or 1.0 mg*). 33,36 For prospective studies, one study used plant-based products, 35 whereas the other three used Dronabinol and Nabilone. The study conducted by van de Donk et al., 35 which compared plant-based cannabis with a placebo, evaluated three different products from Bedrocan, a Dutch company producing standardized medicinal cannabis. These included Bedrocan [22% THC (220 mg/g) with <1% CBD], Bediol [6.3% THC (63 m/g) and 8% CBD (80 m/g)], and Bedrolite [9% CBD (90 mg/g) and <1% THC]. 35 These products are all dried, milled, and homogenized flowers from Cannabis sativa, which can be vaporized.
Controls
Nine studies assessed the effects of cannabis treatment in patients with FMS with or without controls. 30,32 –39 One of three RCTs used placebo as a control 33 ; one compared four cannabis varieties, including three varieties with different THC and CBD content, and one placebo variety without any THC or CBD 35 ; and one compared Nabilone with amitriptyline. 36 Two of the six observational studies used non-cannabis users as their control group. 38,39 One observational study was a crossover study comparing standardized analgesic therapy (SAT) consisting of oxycodone hydrochloride and duloxetine with medicinal cannabis therapy. 30 The remaining three observational studies did not have controls. 31,32,34 One study assessed the effects of cannabis treatment on chronic pain in two groups of patients: patients with central neuropathy (n = 32) and patients with FMS (n = 92). 31
Interventions
The dosage and ratio of the intervention is important for identification of outcomes. The study just cited used plants (inflorescence or flower) for the three different ratios for vaporization. The trial procedure was based on a single vapor inhalation, therefore understanding the content of each inhalation is important. One hundred milligrams of Bedrocan, a THC dominant chemotype, contained 22.4 mg THC, <1 mg CBD in one inhalation; 200 mg of Bediol, a CBD and THC chemotype, contained 13.4 mg of THC, 17.8 mg of CBD in one inhalation; and 200 mg of Bedrolite, a high CBD and low THC chemotype, contained 18.4 mg of CBD, <1 mg THC in one inhalation. 35 For the studies assessing Nabilone, the dosages varied from 0.5 mg once daily to 1 mg twice a day over a period of 2 weeks. 33,36 The Dronabinol study dosed patients daily between 2.5 and 15 mg, with weekly increases of 2.5 mg provided no side effects were reported. 37 The observational studies other than the retrospective study that used Dronabinol 31 did not collect information pertaining to cannabis chemovars, company brands nor mentioned the THC:CBD ratio.
Outcome measures of interventions
Pain
All studies reported at least one pain-related outcome by using different assessment tools, including visual analogue scales (VAS), revised FMS impact questionnaire (FIQR), numeric rating scale (NRS), verbal rating scale (VRS), 5-point Likert scale, McGill pain questionnaire, and an anonymous online questionnaire (Table 4). However, only one study found a 30% and 50% reduction in pain 35 ; one study reported a 50% reduction in pain. 37 The IMMPACT article, 40 discussing chronic pain prevention interventions and outcome measures, suggests that all clinical trials focusing on chronic pain should include pain assessment tools that measure presence and severity, as well as pain intensity and physical and emotional functioning.
Assessment Tools and Outcomes
Indicates that they have been validated for FMS.
FIQ, fibromyalgia impact questionnaire; FIQR, revised fibromyalgia impact questionnaire; FMS, fibromyalgia; ISI, Insomnia Severity Index; LSEQ, Leeds Sleep Evaluation Questionnaire; NRS, Numeric Rating Scale; ODI, Oswestry Disability Index; PDI, Pain Disability Index; PGIC, Patient's Global Impression of Change scale. PSQI, Pittsburgh Sleep Quality Index; SF-36, 36-item Short Form Health Survey; VAS, visual analogue scales; VRS, verbal rating scale; Y/N, yes/no.
Observational studies
Fiz et al. 39 used a 100-mm VAS before and at 2 h after cannabis consumption and reported a mean reduction of pain of 37.1 mm (p < 0.001). Habib and Artul 34 used the FIQR and reported pain reduction from a mean 9.39 ± 0.94 (7–10) to 3.88 ± 1.98 (1–7) (p < 0.001). Habib and Avisar 38 used an anonymous online questionnaire to evaluate the effects of cannabis in patients with FMS and found that 94% of cannabis users experienced pain improvement. Sagy et al. 32 used a 0–10 NRS and found that pain intensity reduced from a median 9.0 at baseline to 5.0 at the 6-month follow-up (p < 0.001). Weber et al. 31 used a 6-point VRS and maximum/minimum pain intensity by using an 11-point NRS and reported a reduction in mean pain intensity in FMS patients from 7.99 ± 1.5 at baseline to 4.4 ± 1.5 after the 7-month THC treatment. Yassin et al. 30 assessed FMS low back pain by using a 1–10 VAS and reported a pain reduction from 8.1 ± 1.4 at baseline to 5.3 ± 1.3 after the 3-month treatment and 3.3 ± 2.2 after the 6-month treatment (p < 0.0001).
Experimental studies
In a small pilot study performed by Schley et al., 37 four patients with FMS who completed the study were treated with daily THC over 3 months and experienced significant pain reduction by about 67% (from a mean 8.1 ± 7.0 to 2.8 ± 5.0; p < 0.01), which was evaluated by using a 0–10 VAS. An RCT by Skrabek et al. 33 used a 10-cm VAS to assess the effects of Nabilone on pain in patients with FMS and reported a significant pain reduction at 4 weeks in comparison to baseline (−2.04, p < 0.02).
The RCT conducted by van de Donk et al. 35 assessed spontaneous pain by using an 11-point (0–10) VAS at baseline (before cannabis inhalation) and at 1, 2, and 3 h after single inhalation. It was found that none of the treatments had an effect greater than placebo on spontaneous pain scores or electrical pain responses. The RCT by Ware et al. 36 compared Nabilone with amitriptyline in FMS patients with insomnia, where pain was measured by using the McGill Pain Questionnaire; no differences were reported between Nabilone and amitriptyline treatments for pain (McGill present pain intensity difference = −0.1; 95% confidence interval [CI] = −0.3 to 0.2).
Quality of life and other outcomes
Some studies assessed the effects on quality of life, 30,32,34,36 –39 mental state, 32 –36,38,39 sleep quality, 32,34,36,38,39 and other FMS symptoms, 33,34,38,39 as well as global satisfaction with the treatment 30,36 and psychoactive effects of cannabis. 35
Observational studies
Fiz et al. 39 used the 36-item Short Form Health Survey (SF-36), the FMS impact questionnaire (FIQ), and the Pittsburgh Sleep Quality Index (PSQI). The SF-36 mental health component score was slightly, but significantly, higher in the cannabis group (mean [M] = 29.6 ± standard deviation [SD] = 8.2) than in the nonuser group (M = 24.9 ± SD = 8.9), p < 0.05. The difference in the physical component score was nonsignificant between groups (cannabis group: M = 26.29 ± SD = 6.7; nonuser group: M = 27.34 ± SD = 5.8; p = 0.53). There were no differences in the FIQ (M = 65.5 ± SD = 11.9; M = 65.5 ± SD = 12.8; p = 0.36) nor in the PSQI (M = 14.1 ± SD = 3.2; M = 14.4 ± SD = 3.3; p = 0.73).
Habib and Artul 34 used the FIQR and reported significant improvement of all FIQR parameter scores (p < 0.001). Habib and Avisar 38 conducted an anonymous online questionnaire to evaluate the effects of cannabis on patients' quality of life and FMS-related symptoms. The following results were identified: 93% of participants reported better quality of sleep, 85% reported improvement of depression, 81% reported improved daily activity, 62% reported improvement of anxiety, and 43% reported undertaking sports activity while on cannabis treatment compared with only 32% before the treatment. 38
Sagy et al. 32 used a 5-point Likert scale to assess quality-of-life parameters and an 8-point Likert scale to assess FMS-related symptoms before and after treatment. After 6 months of treatment, 61.9% of participants reported their quality of life to be good or very good compared with 2.7% at baseline (p < 0.001). Some quality-of-life components, including sleep quality, appetite, and sexual activity, significantly improved at 6 months (p < 0.001, 0.02, and 0.03 respectively). Other components such as mobility, dressing, and concentration did not improve, and the quality of daily activities deteriorated at 6 months (p < 0.001). The sleep problems reported by 92.9% of participants at baseline improved in 73.4% and disappeared in 13.2% of participants (p < 0.001). Depression-related symptoms reported by 59.2% of patients at baseline improved in 80.8% of patients (p < 0.001).
Yassin et al. 30 used the Oswestry Disability Index (ODI) (0–100 scale), FIQR (0–100 scale), and the Patient's Global Impression of Change (PGIC) scale. The following results were reported: improvement of FIQR score from 45.3 ± 10.2 at baseline to 68.7 ± 15.6 after the 3-month treatment and 80.5 ± 12.2 after the 6-month treatment (p < 0.0001); improvement of Schober test results from 3.5 ± 1.8 at baseline to 4.2 ± 2.2 after the 3-month treatment and 5.3 ± 1.5 after the 6-month treatment (p < 0.0001); and reduction of ODI from 73.7 ± 11.4 at baseline to 45.9 ± 19.1 after the 3-month treatment and 30.7 ± 13.6 after the 6-month treatment (p < 0.0001). PGIC was significantly higher during medicinal cannabis therapy than during SAT (p < 0.0001). 30
Experimental studies
Schley et al. 37 used the SF-36, Pain Disability Index, and FIQ and they found no significant changes in response to THC medication. Skrabek et al. 33 used FIQ to evaluate FMS-related parameters. FIQ and anxiety scores significantly decreased (−12.07, p < 0.02 and −1.67, p < 0.02, respectively) after 4 weeks of treatment with Nabilone. There were no significant improvements in the placebo group.
The RCT by van de Donk et al. 35 used the Bond and Lader questionnaire and the Bowdle questionnaire. The responses to the Bond and Lader questionnaire indicated mild deterioration in mood observed during Bediol treatment compared with placebo (p = 0.02) and mild deterioration in alertness during Bediol (p = 0.01) and Bedrocan treatment (p = 0.02). Bedrocan and Bediol caused moderate to high responses, on average just below 50% of the maximum possible response, but significantly greater than placebo (p < 0.001). Bedrolite had less intense drug high responses compared with either Bedrocan (p = 0.003) or Bediol (p < 0.001). 35
Ware et al. 36 used the Insomnia Severity Index (ISI) and the Leeds Sleep Evaluation Questionnaire (LSEQ); short-form Profile of Mood States, FIQ, and global satisfaction with the treatment by using a simple yes/no scale. Nabilone was found to have a greater effect on sleep than amitriptyline on the ISI (adjusted difference = −3.25; CI = −5.26 to −1.24). Based on the LSEQ, there was no evidence of superiority of either drug. There were no marked differences in other scales of the LSEQ between the two drugs, although there was a suggestion of Nabilone performing better than amitriptyline for ease (difference = −0.7; CI = −1.4 to 0.02) and speed (difference = −0.7; CI = −1.36 to 0.03) of falling asleep. At the completion of the trial, preference for Nabilone was reported by 41% and for amitriptyline by 32% of participants (difference = 9%; 95% CI = −16% to 32%). 36
Safety
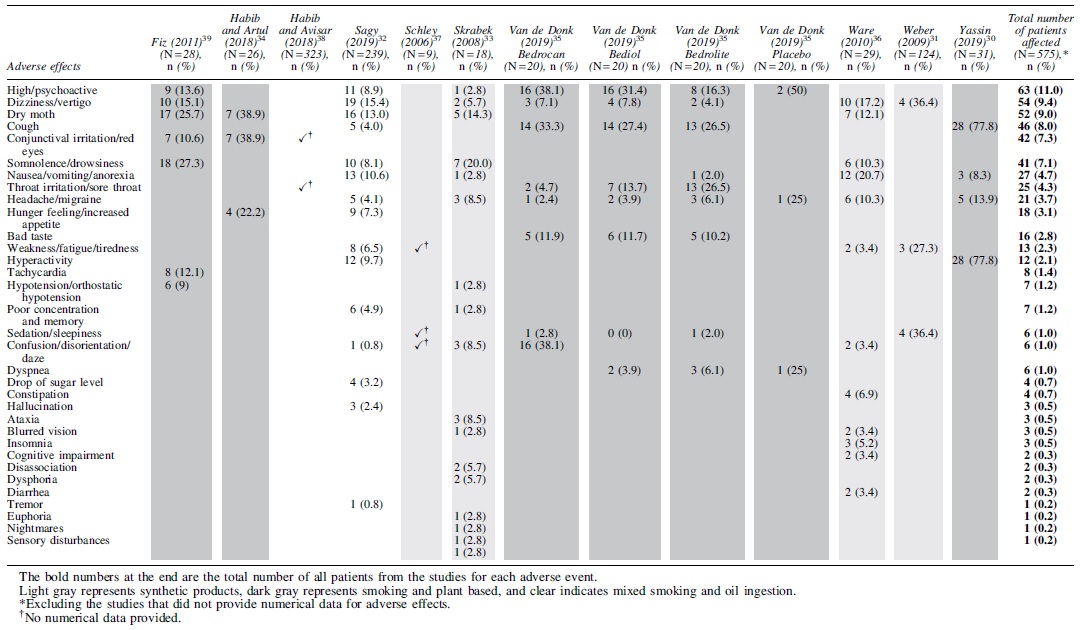
All studies assessed the safety of cannabis use through identification of AEs (Tables 2 and 4). The most frequent AEs of cannabis treatment were feeling “high” (n = 63), dizziness/vertigo (n = 54), dry mouth (n = 52), cough (n = 46), conjunctival irritation/red eyes (n = 42), somnolence/drowsiness (n = 41), nausea/vomiting/anorexia (n = 27), throat irritation/sore throat (n = 25), headache/migraine (n = 21), hunger feeling/increased appetite (n = 18), bad taste (n = 16), weakness/fatigue/tiredness (n = 13), and hyperactivity (n = 12) (Table 5). No serious AEs were reported. One study reported 25 patients (8%) feeling dependent on cannabis. 38
Summary of Adverse Effects
Tolerability
Out of six studies that reported withdrawals (n = 304), 41 participants (13.5%) dropped out due to AEs from cannabis treatment, including drowsiness, dizziness, sedation, daze/disorientation, fatigue/tiredness, nausea, poor coordination, decreased concentration, headache, hyper-alert state, edema, insomnia, and enhanced appetite 30,31,33,35 –37 (Table 2).
Discussion
One of the most important findings from this review is that medicinal cannabis was found to be safe and well tolerated, although due to the diversity of cannabis cultivars and preparations, further research and consideration is required for each cannabis drug/dosage form used in research and clinical settings. The main reported side effects in FMS trials overall include drowsiness, dizziness, sedation, daze/disorientation, fatigue/tiredness, nausea, poor coordination, decreased concentration, headache, hyper-alert state, edema, insomnia, and enhanced appetite, 30,31,33,35 –37 which correlate with the reported outcomes for cannabis trials more generally. 41,42 The main side effects from cannabis products are due to the effects of THC, and these effects are amplified when consumed via methods with quicker absorption such as smoking or vaping compared with oral ingestion. 43 Moreover, the pharmacokinetics and pharmacodynamics differ between inhalation and oral ingestion influencing the onset and duration of desired AEs for each method of administration. 44
Given the greater frequency of side effects associated with inhalation, as identified in this review, some FMS patients may prefer other forms of administration. Oral ingestion is one such option, particularly given that oil-based products can be dosed through incremental titration, thereby possibly reducing the incidence of adverse events and side effects. 45 Two studies in this literature review reported that only 5% (Ref. 38 ) and 20% (Ref. 32 ) of the participants were using oil, whereas a further four studies assessed only oil-based products. 31,33,36,37 Although oil-based products have been reported to commonly produce drowsiness, tiredness, dry mouth, nausea, and confusion, 42 the main side effect of orally administered cannabis oil reported from the studies examined in this literature review was feeling “high” or intoxicated. There are several reasons that people with FMS may respond better to cannabis administered through inhalation rather than oral ingestion. These reasons may include different cluster types of FMS, severity of pain and symptoms, and interindividual variability due to their ECS or their cytochrome P450 enzyme profile. 23 The dose or amount of dried flower used is also important. 46 Accordingly, further research is required to identify the best administration method, form, and dosage for the management of FMS.
The studies included in this review commonly focused on the use and effect of cannabis on the management of FMS-related pain. FMS is a complex disorder involving chronic widespread pain along with other physical and mental issues, resulting in treatment options to date having had limited success. 47 The experience of pain by people with FMS, and the factors contributing to this experience, vary greatly. 47 This may be why the pain scales used in the studies included in this literature review varied. The VAS (n = 5) was the most common pain assessment tool used in the studies assessed. It was reportedly the most sensitive and specific tool for assessing pain in patients with FMS and demonstrated the highest correlation with other pain measures, physical functioning, stiffness, and fatigue. 48 In addition, VAS has an advantage of being a consistent, concise, and quick measure, as well as easy to administer in the clinical setting. 48,49
However, the 5-point Likert scale, FIQ, NRS, VRS, an online questionnaire, and the McGill pain questionnaire were also utilized. The use of different outcome measures presents challenges to researchers seeking to compare results between studies or calculate cumulative results through meta-analysis. However, diverse pain scales may also be appropriate in this specific disease population by enabling researchers to evaluate change in a greater range of symptoms and, in doing so, capture a wider spectrum of intervention effects. Research in other complex conditions such as multiple sclerosis has incorporated different yet complementary pain scales, in addition to quality-of-life measures as the primary outcome, and such an approach may also be suitable for FMS research. 50 Although six studies included in this review used a pain scale and quality-of-life measure, none of these studies examined the effects on pain with changes in quality of life, but they rather reported each measure as two different outcomes. Other previous FMS research has examined the correlation between pain reduction, and both sleep quality and overall quality of life in individuals with FMS, but studied a stretching intervention. 51 Future cannabis clinical research in FMS populations should explore the relationship between the change in an individual's pain levels and their quality of life or level of daily living activity.
It is also worth noting that none of the studies included in this review measured pain expectancy. Previous research involving people who live with chronic pain, including people who have FMS, has found that pain expectancy can undermine the individual's choice of activity and behavior. 52 Similarly, longitudinal and daily diary studies have found that higher pain expectancy can lead to greater pain and disability outcomes. 53,54 With this in mind, pain expectancy can impact a person's FMS outcome, behavior, and mental and emotional health. 55 Pain expectancy also intertwines with quality of life, and an expansion of pain expectancy can be explained by an individual's personality and other multifaceted characteristics. The impact of personality on pain expectancy becomes particularly relevant in FMS given the link between higher levels of neuroticism and FIQR found in individuals with FMS (p = 0.002), symptom severity (p = 0.008), and typically worse mental health—including higher levels of anxiety, depression, and stress—thereby affecting quality of life. 55 In the case of cannabis, there would be further benefits to measuring pain expectancy and personality in clinical trials due to the reported effects of cannabis on mental states such as anxiety, stress, 56 and pain. 33 In addition, it would also be beneficial for clinical trials to note the date of diagnosis and clinical outcomes, as they have been found to have an impact.
From the studies identified in this literature review, only two studies used placebo. The placebo effect has been known to be problematic in pain research with a landmark review of neuropathic pain studies between 1990 and 2013 finding that the placebo effect increased significantly (p = 0.002) whereas drug response decreased on average by 34.7% (Ref. 57 ). In addition, it has been found that the placebo effect can be aggravated when the drug in question has psychoactive properties, for example, antidepressants or cannabis, or have a reputation as being “miraculous” such as the public perception of cannabis. 58 Smoked cannabis studies call into question the reliability of blinding versus placebo in regards to the cognitive effect. 58 One of the reasons for this may be that most inhaled placebo preparations are not completely inert, as they contain terpenes that themselves have biologically active constituents. 59 The placebo effect in FMS populations may be further exacerbated by the duration of the illness. For example, one trial evaluated the placebo response after long-term exposure to FMS pain during a 12-week placebo-controlled RCT on milnacipran. 60 Of the placebo group (n = 37), 22 patients were classified as placebo non-responders and 15 were responders, according to the PGIC scale. The study found an inverse association between the length of time that participants experienced FMS symptoms and a reduction in pressure pain sensitivity among the placebo responders (r = 0.689; p = 0.004) but not in the non-responders (r = −0.348; p = 0.112). This indicates that when recruiting for trials, early FMS interventions from diagnosis may express better outcomes as the endogenous pain regulation may still be harnessed. 60 The degree to which this factor has impacted the results of the studies included in this literature review is unclear, as only three studies 32,34,38 reported the mean duration of FMS since diagnosis.
Insufficient attention has been given to safety issues in the study population of the articles included in this review. A history of psychosis, cardiac comorbidity, liver disease, recurrent falls, addiction problems, pregnancy, and breastfeeding are all well-documented contraindications for cannabis administration. 61 Clinical trials investigating medicinal cannabis need to consider possible long-term safety implications in specific populations such as pregnant women. 62 Pregnant and breastfeeding women are one group in particular that should not be administered cannabis either medicinally or legally. 63 Cannabis has been found to cross the placenta and pass into breastmilk, which can result in fetal and neonatal exposure to this drug. This exposure has been linked to growth restriction, stillbirth, spontaneous preterm birth, and neonatal intensive care unit admission. 63 As women who have FMS could be using cannabis for their symptomology, it is highly advisable that they are educated on the detriments of using cannabis, recreational or medicinal, during pregnancy and breastfeeding. Despite this, pregnant or breastfeeding ladies were not discussed in the studies and surveys identified in this literature review.
In addition, as cannabis use in children other than those with intractable epilepsy has limited research and is generally not recommended, 64 safety research involving children who have been diagnosed with FMS is urgently needed and, until this has occurred, children with FMS should not be prescribed cannabis. In more general adult populations, there is still mixed evidence on long-term safety of cannabis use, which is mostly derived from recreational rather than medicinal use. The cardiovascular, respiratory, cognitive, psychological, and mental long-term impacts of cannabis should be considered; therefore, more additional research is required to compare the long-term effects of oral administration of cannabis oil with smoking and inhalation. 62 The clinical trials included in this review have provided pilot data on safety and basic efficacy for the use of medicinal cannabis for people with FMS; however, three were using oral administration of synthetic cannabis (oil), and one study considered plant-based cannabis administered via inhalation. The different administration methods make comparisons between studies difficult, impacting overall understanding of the safety of cannabis use within an FMS population. Accordingly, additional studies using plant-based oil ingestion or other inhalation studies are required.
The information obtained from this literature review indicates that medicinal cannabis can benefit people with FMS, but many research gaps remain. Future research needs to better describe: the individuals who will most benefit from cannabis use for FMS symptoms; the most effective, tolerable, and acceptable chemovar or product for this population; and the preferred dose and method of administration (oral or inhalation). Despite these gaps, this research provides evidence that oral ingestion of synthetic cannabis may assist with chronic pain management and inhalation of cannabis may assist with rapid-onset pain relief for individuals with FMS.
Limitations
This review included a wide range of experimental and observational studies potentially impacting the heterogeneity of the review cohort. As only three RCTs and six observational studies were included in the review, interpretation and generalizability of results is limited. Of the four clinical trials reviewed, three used oil whereas one compared inhaled variants with dosage forms varying widely. This variability impacts timelines and the size of effect, making it difficult to compare outcomes. In addition, potential studies may have been missed due to the date restriction and search terms used, although gray searches were included, and two authors screened the citations. This review mainly focused on the assessment of pain, quality of life, side effects, and safety of cannabis in FMS patients; hence, some other outcome measures or aspects of these trials may have been missed.
Conclusion
FMS is a complex condition that is characterized by pain and fatigue among other symptoms. This literature review identified that medicinal cannabis may be beneficial for some people with FMS; however, further studies are required to confirm the possible impact of cannabis on pain in this cohort. In addition, it is important to identify what chemovar types, THC to CBD ratios, dosage regimen, or form of administration are appropriate for various symptomology, and what assessment tools are required to quantify and interpret outcomes. Due to the poor treatment options available to people with FMS, further investigations into cannabis for this condition are both warranted and worthwhile.
Footnotes
Acknowledgments
The authors would like to acknowledge the Endeavour College of Natural Health for supporting the student through a summer school research grant. The authors also want to thank Dr. Amie Steel for assisting with the editing of this article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Funding from Endeavour College of Natural Health was given to the student via a summer research position grant.