
Abstract
Objective:
Chronic hand eczema (CHE) is a common inflammatory skin disease with a major psychological and socioeconomic impacts on patients' quality of life (QoL) and work ability. To the best of knowledge, this study is the first randomized-controlled trial conducted to evaluate the effect of paraffin bath therapy in management of hand eczema and its related symptoms.
Design:
This study was a parallel-group, active-control, randomized clinical trial with measures at pretreatment, 6th week, and 12th week of treatment.
Settings:
The study took place at the Outpatient Clinic of Faculty of Physical Therapy, Cairo University, and some licensed rehabilitation centers in Cairo for a 1-year period.
Subjects:
Sixty patients with moderate to severe CHE were randomly assigned into two groups of equal number; the paraffin bath therapy group and the control group.
Interventions:
The paraffin group received paraffin bath therapy for 5 days a week for 12 weeks, in addition to the routine skin care program, while the control group only received the routine skin care program.
Outcome measures:
SCORing Atopic Dermatitis (SCORAD) was used to assess the severity of atopic dermatitis and dermatology life quality index (DLQI) to assess the effect of CHE on quality of patients' life. All measurements were obtained before, at the 6th week, and at the 12th week of treatment.
Results:
Marked improvement in the severity of the disease symptoms was observed, reflected by a highly decrease in objective SCORAD score in the paraffin group over time more than the control group. The percentage of reduction was 28.6% in paraffin group versus 0.41% in control group. Subjective item score (itching and sleepiness) was reduced in the paraffin group more than the control group with a percentage of improvement (47% and 5.5%), respectively. Regarding QoL measure, there were highly positive changes in DLQI in paraffin group more than the control group. The percentage of improvement was 60% in paraffin group and 3.8% in control group.
Conclusions:
Paraffin bath therapy applied for a 12-week duration seems to be effective, both in reducing severity of eczema symptoms and improving QoL in patients with CHE.
Introduction
Hand eczema (HE) is the most common form of inflammatory dermatosis, confined to the hands, with major psychological and socioeconomic impacts on patients' quality of life (QoL). Eczema and dermatitis are used as synonyms. 1,2 Chronic hand eczema (CHE), the most debilitating condition among atopic dermatitis patients, 3 is an eczematous process that lasts for more than 3 months or occurs more than twice a year. The disease is not uniform and varies in severity, depending on etiology and morphology. 4
Hands are the most visible area affected by eczema. HE's chronic nature is attributed to the multifactorial origin of irritants, allergic and endogenous factors acting in concert leading to poor response of the disease to treatment. Eczema is characterized by some primary clinical signs, such as erythema, scaling, fissure, papules, vesicles, hyperkeratosis, and subjective symptoms of itching and pain. 5 –7 Besides the negative impact of CHE on patients' QoL because of the chronic relapsing nature of the disease, 8,9 its painful fissures and blisters prevent manual work, thus causing significant disability and economic loss to both individuals and society. 10 HE is associated with intense use of health care services, high rates of prolonged sick leave, and a major risk of job loss or change. 11 –13 The aforementioned factors, in addition to the poor prognosis of HE, make it an important disease to study from an individual and a social perspective. 14
Traditionally, paraffin bath therapy (PBT) as a type of superficial thermotherapy was proved as an effective treatment for arthritic and inflammatory conditions such as osteoarthritis, rheumatoid arthritis, hand arthritis, carpal tunnel syndrome, stiffness, and multiple sclerosis by improving local blood flow and relieving pain. Paraffin wax is safe to come in contact with the patient due to its low melting point, approximately around 37.5°C. 15 –19
The key factors in treating CHE include the use of emollients as well as complete careful history and avoidance of possible triggers. 20 In the dermocosmetic field, PBT has also been widely used because of its ability to improve skin quality, through its reparative effects on the skin barrier, and it acts as a potent emollient. 21 Moreover, the use PBT on the hands has a very soothing and therapeutic effect. However, the present literature lacks PBT application for CHE; there is a strong need for randomized-controlled trials to study the effect of PBT in CHE, therefore, the purpose of this study was to evaluate the efficacy of PBT on the severity of eczema symptoms and QoL in patients with CHE.
Materials and Methods
Trial design
A randomized, single-blind, active-controlled, parallel-group study was conducted at the Outpatient Clinic of Faculty of Physical Therapy, Cairo University, and some licensed rehabilitation centers in Cairo for a 1-year period. Patients with CHE were recruited for this study via specialized dermatologists' referrals (from various dermatology departments of Cairo University teaching hospitals and some physicians' consultations in dermatology clinics). After a full explanation of the aim and the protocol of the study, each patient accepted to participate in this study signed a written declaration of informed consent before enrollment. All research procedures were in accordance with the Declaration of Helsinki. The study was approved by the Institutional Review Board at the Faculty of Physical Therapy, Cairo University, Egypt (Reference No. P.T. REC/012/002655), and was registered with the
Participants
Sixty patients with moderate to severe CHE were randomized into two groups of equal size: the PBT group and the control group. A complete history of the condition, as well as clinical examination of the appearance, distribution, and the location of dermatitis, was carefully examined by a specialized dermatologist to rule out possible differential diagnoses.
Inclusion and exclusion criteria
Patients who met the following criteria were eligible for entering the study. (1) Age of the patient ranged from 20 to 40 years; (2) time elapsed from the beginning of the disease was more than 3 months according to the Guideline of the German Dermatological Society 19 ; (3) two relapses or more than three consecutive weeks at least with visible signs in the last 3 months; and (4) had a negative patch test or a clinically irrelevant test reaction to rule out allergic contact dermatitis. Patients were excluded if they had (1) active eczematous lesions on other parts of the body; (2) malignant or premalignant skin tumors; (3) allergic contact dermatitis of the hands; (4) infective skin disease that may interfere with the conduct of the study; (5) patients with impaired skin sensory discrimination abilities; and (6) allergies to paraffin or other ingredients.
Sampling and randomization
G-power software (version 3.0.10) was used to estimate sample size. The sample size of 68 participants was more than sufficient to ensure 80% power with an error risk of 5%. Eligible patients (60) were randomly assigned to either of the two groups of equal number: the paraffin group and the control group. Consecutive patients were given consecutive numbers on the list, and a computer-generated randomization list was created accordingly by the department's secretary. The department's secretary concealed the randomization sequence until the end of the trial.
Measurement procedures
Measurements were done by a blind assessor on three occasions: at randomization (T1), at the 6th week (T2), and at the 12th week (T3) of treatment (Fig. 1).
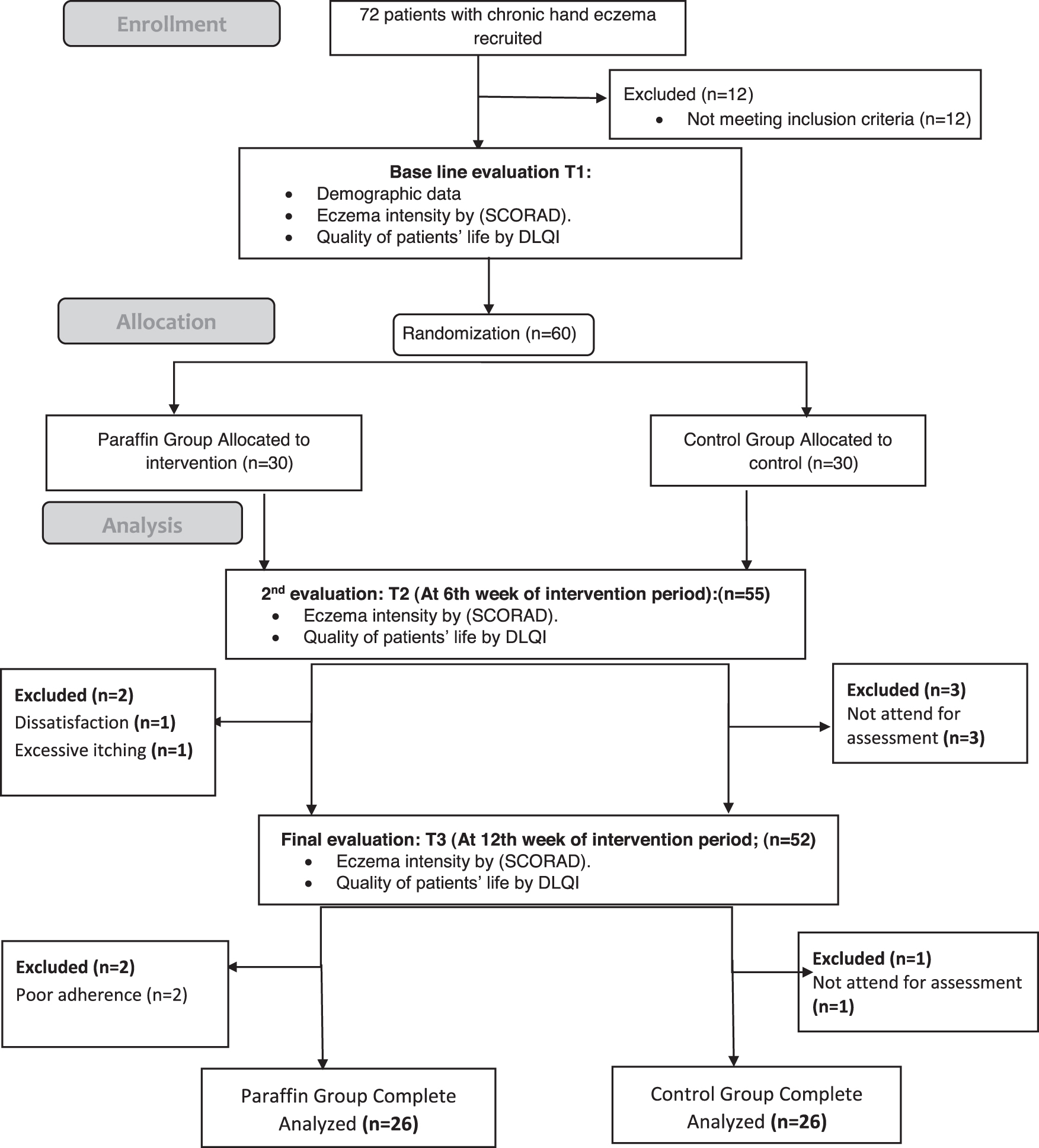
Participating patients and their dropout throughout the study.
Assessment of eczema severity
SCORAD (“SCORing Atopic Dermatitis”) is the most widely used clinical tool for assessing the severity (i.e., extent, intensity) of atopic dermatitis as objectively as possible. 22 It consists of six objective items (erythema, edema/papules, effect of scratching, oozing/crust formation, lichenification, and dryness), and two subjective symptoms (itching and sleeplessness), the maximum score is 103 points. 23 In objective SCORAD, the subjective symptoms (itching and sleeplessness) are not assessed; the total score is 83 points. 24 –26 “Bonus points” for disfiguring lesions or functional limiting lesions received 10 extra points. Objective SCORAD (without subjective measures) is an excellent system for clinical trials. A research assistant assessed each item of severity and extent and then calculated using the SCORAD Calculator (version 0.9.0). 27
Dermatology life quality index
Dermatology life quality index (DLQI) is a simple and self-explanatory questionnaire tool designed for adult patients. The Arabic version of DLQI was used in the current study and it consists of 10 questions describing symptoms, feelings, leisure activities, work or school activities, personal relationships, and treatment. The responses for each question are “not at all,” “a little,” “a lot,” and “very much,” scaled as 0, 1, 2, and 3, respectively. After summing the score of each question, the total score ranges 0 as a minimum score and 30 as a maximum score. Higher scores represent more impairment of QoL. 28 –34
Treatment procedures
Patients were educated about the disease, its causes, and adequate skin care and protection. All patients in both groups received written information about the skin care program and were advised to use emollients. Only patients in the paraffin group received PBT in addition to skin care measures (gloves, lifestyle changes, emollients, and moisturizers), while the control group received skin care measures only. The used emollient types were in two forms, lotions (containing glycerol only) or creams (without lanolin).
Paraffin apparatus
The paraffin apparatus (Para-Therapy, Model PT-18-S-V-INT; Whitehall Manufacturing, CA) was used for melting the wax. The internal wall of the paraffin tank is made of stainless steel and the apparatus has a metallic aluminum cover. The paraffin apparatus has a specific wax heater and thermostat to control temperature (input voltage, 230 V AC; power input, 0.36 KW/1.5 A, 50/60 Hz).
The treatment protocol
Patients in the paraffin group received paraffin wax baths (with dipping and wrapping technique) 5 days a week for 12 weeks. Once prepared, the paraffin wax blocks were placed inside the tank, and the thermostat was set between 35°C and 40°C. Melting of the paraffin took 90–120 min. Patients were instructed to wash and thoroughly dry the hands and to remove any jewelry before the application of paraffin wax; then after adjusting the suitable temperature for each patient, the patient's hands were slowly and completely submerged into the paraffin bath for 3–4 sec and then withdrawn. Patients were instructed to keep fingers in abduction, and avoid moving hand joints or breaking the “glove” of paraffin in between dips.
Immersion of the hands was repeated for five to eight times until a thick layer of paraffin covered each hand, forming a white “glove.” Then hands were kept in sealed plastic bags for 15–20 min before the wax was removed, then squeezed into a ball, stored in an appropriate container/bag, and clearly labeled with the individual patient's details in between the treatments. 35,36
Instructions
All patients were given the following instructions. (1) Avoid alkaline soaps, use conventional soap instead. (2) Wash hands in warm water. (3) Rinse and dry hands after washing. (4) Do not wear rings on fingers at work. (5) Wear clean protective gloves that remain intact while performing “wet” work for a short period. Cotton gloves should be worn underneath if the work lasts more than 10 min. (6) Do not use disinfectants, unless specifically required. (7) Use a lipid-rich moisturizer especially after work and before bedtime. 37
Statistical analysis
Data were described and analyzed for all available patients. Statistical analysis was done through SPSS version 23 (IBM SPSS Statistics, Armonk, NY). Level of significance was p-value <0.05, using two-tailed tests. Continuous variables were summarized as mean ± standard deviation and categoric variables as frequency and percentage (%). The Shapiro–Wilk test was used to detect a normal distribution of data. One-way repeated-measures analysis of variance (ANOVA) was used to detect change of eczema severity (objective SCORAD score) throughout the study duration for all patients, while the Friedman test was to detect the change in subjective item score as well as the impact of the disease on the QoL. Independent t-test was used to compare the differences between both groups for parametric normally distributed data, while the Mann–Whitney test was used to detect differences between both groups for nonparametric data.
Results
Figure 1 presents the flowchart for patients with their dropout throughout the study as recommended by the CONSORT (Consolidated Standards of Reporting Trials) statement. 38 Seventy-two patients were screened for eligibility, and 60 subjects fulfilled the inclusion criteria and were initially randomized into two groups of equal number. During the treatment period, eight patients (13%) dropped out: four in the paraffin group and four in the control group. One patient in the paraffin group withdrew due to development of excessive itching, one patient discontinued as a result of dissatisfaction with paraffin therapy, and two patients reported poor adherence to the treatment. Participants with poor adherence to the program (defined as missing more than three consecutive sessions or more than 20% of all sessions) were excluded from the study. Four patients in the control group did not attend for reassessment. The data of dropout patients were excluded and not used in the statistical analysis. The data were available for 52 patients: control group (n = 26) and paraffin group (n = 26) for the final analysis.
Baseline demographic and clinical characteristics of patients
Table 1 shows the characteristics of the patients completing the study. Both groups were comparable at the time of randomization (T1) regarding the demographic and clinical characteristics. The results showed that both groups bear similar characteristics regarding age, gender, emollient type, duration of disease, baseline objective SCORAD score, baseline subjective items, and baseline DLQI score, as no statistically significant differences between both groups, p-value >0.05.
Baseline Demographic and Clinical Characteristics
p: probability <0.05.
C, cream; DLQI, dermatology life quality index; F, female; L, lotion; M, male; SCORAD, SCORing Atopic Dermatitis; SD, standard deviation.
The magnitude of the effect
A one-way repeated-measures ANOVA was conducted to evaluate if there was a change in objective SCORAD score over time within each group. For the paraffin group, the results of the ANOVA test indicated a significant time effect, Wilks' Lambda = 0.076 F(1.53, 38.47) = 198.122, p < 0.05, follow-up of comparisons indicated that each pairwise difference was significant, p < 0.05, and thus, there was a marked decrease in the objective SCORAD score over time, while in the control group, there was a very small reduction with no statistically significant differences, Wilks' Lambda = 0.869 F(2, 50) = 1.58, p > 0.05. Parametric independent t-test showed a statistically significant difference between both groups at the 6th week and 12th week p < 0.05. The percentage of reduction in the objective SCORAD score in paraffin group was more than the control group at the end of treatment (28.6% vs. 0.41%) (Table 2).
Statistical Analysis of Objective SCORing Atopic Dermatitis and Subjective SCORing Atopic Dermatitis Within Each Group and Between-Group Comparison at Baseline Assessment, and After 6 Weeks and 12 Weeks of Treatment
p: probability <0.05.
Significant.
SCORAD, SCORing Atopic Dermatitis; SD, standard deviation.
A Friedman test was conducted to evaluate if there was a change in subjective item score (itching and sleepiness) over time within each group. The results indicated a significant time effect, p-value <0.05. Wilcoxon comparisons indicated that each pairwise difference was significant, p-value <0.05, and thus, there was a marked decrease in subjective item score over time, while in the control group, there was a very small reduction with no statistically significant difference with the time, p > 0.05. The Mann–Whitney test showed a statistically significant difference between both groups at the 6th week and 12th week of treatment as p < 0.05. The percentage of reduction in subjective item score in the paraffin group was more than the control group at the end of treatment (47% vs. 5.5%) (Table 2).
QoL scores
A Friedman test was conducted to evaluate if there was a change in DLQI score throughout the study duration within each group. In the paraffin group, the results indicated a significant time effect, p-value <0.05. Wilcoxon comparisons indicated that each pairwise difference was significant, p-value <0.05, and thus, there was a significant decrease in DLQI score over time, p-value <0.05, while in control group, no statistically significant difference, p > 0.05. The Mann–Whitney test showed a statistically significant difference at the 6th week and 12th week of treatment between both groups p < 0.05. The percentage of decrease in DLQI score in the paraffin group was more than the control group (60% vs. 3.8%) (Table 3).
Statistical Analysis of Dermatology Life Quality Index: Within Each Group and Between-Group Comparison at Baseline Assessment, and After 6 Weeks and 12 Weeks of Treatment (Dermatology Life Quality Index)
p: probability <0.05.
Significant.
DLQI, dermatology life quality index.
Discussion
HE has psychosocial consequences such as involuntary job rotation or early retirement. 39 Furthermore, QoL has been shown to correlate negatively to the severity of the disease. 9,40 To the best of knowledge, this study is the first single-blinded randomized clinical trial evaluating the effect of PBT on the severity of the disease symptoms and QoL in patients with CHE. According to the results of the current study, statistically significant reductions in the severity of the disease symptoms and a significant improvement in QoL, measured by SCORAD score (objective and subjective items) and DLQI, respectively, were observed in the paraffin group over time with no statistically significant changes in the control group. In addition, statistically significant differences between groups regarding all variables favoring the paraffin group over time.
The significant improvements in these variables in the paraffin group could be attributed to the effect of PBT as one of the therapeutic heating modalities that demonstrate their effectiveness by producing analgesia, changes in local or systemic temperature, improving blood supply, and increased metabolism. 41 –44 In addition, paraffin is a very potent emollient and has the ability to improve skin quality by skin repair. 18,21
In literature, many studies 16,40,42,45 approved the effect of paraffin therapy either alone or with exercise on reduction of pain and tenderness of hand joints by improving blood flow, minimizing muscle spasms and inflammation, and relaxing muscles.
Results of this study are consistent with that of Mir-Bonafé et al. 35 as they reported that paraffin therapy was effective in treating patients with CHE. They used the DermaSat questionnaire to evaluate patient satisfaction after PBT and found that the percentage of efficacy was very good or good in 46% and 54%, respectively. Moreover, the effect of paraffin on QoL in patients with CHE was considered very positive in 30%, positive in 53%, and fair in 15%, without side effects, however, about 51% of patients reported the time-consuming effect of paraffin. The overall satisfaction of patients was very good in 54% and good in 46%. However, a similarity between the current study results and that of Mir-Bonafé et al., still there are some differences in treatment duration, sample size as only 13 patients (5 men and 8 women) were included, ages of the patients, outcome measures, and the absence of blindness and the control group.
Results of the current study are very promising and the strengths of this study were that objective as well as subjective outcome measures were used to evaluate the severity of the disease symptoms and the impact of disease on the QoL. Also, this study had a high level of adherence because only two patients reported poor adherence and one reported dissatisfaction with paraffin therapy; such adherence level may be uncommon in the daily clinical practice of physical therapy. Regarding side effects, no major side effects were reported, only one patient complained of excessive itching.
The current study has some limitations such as small sample size and the long-term effect of PBT was not measured as well as patients' adherence to instructions. Therefore, further research, with a larger sample size, about the long-term effect of adding paraffin therapy for the treatment of CHE, to evaluate the effect of home treatment with paraffin therapy after patient training to reduce the impact of time, considering patients' adherence measurement as well as the comparison between male and female results, may also be required.
Conclusions
On the basis of the current study, it can be concluded that paraffin bath therapy may reduce eczema symptoms and improve QoL in patients with CHE. Paraffin wax therapy may be regarded as an additional effective short-term therapy option for CHE.
Footnotes
Acknowledgments
The authors would like to gratitude all patients participated in this study and The Deanship of Scientific Research at Princess Nourah bint Abdulrahman University for funding this research through the Fast-track Research Funding Program.
Authors' Contributions
I.S.W. and Z.M.I.: Research concept and design; I.S.W. and Z.M.I.: Collection and/or assembly of data; I.S.W. and Z.M.I.: Data analysis and interpretation; I.S.W. and Z.M.I.: Writing the article; I.S.W. and Z.M.I.: Critical revision of the article; I.S.W. and Z.M.I.: Final approval of article. All coauthors have reviewed and approved of the article before submission.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was funded by the Deanship of Scientific Research at Princess Nourah bint Abdulrahman University through the Fast-track Research Funding Program.